Article Text

Abstract
Background Cardiovascular disease (CVD) is responsible for the largest number of discharges against medical advice (AMA). However, there is limited information regarding the reasons for discharges AMA in the CVD setting.
Objective To identify reasons for discharges AMA among patients with CVD.
Design Qualitative study using focus group interviews (FGIs).
Participants A convenience sample of patients with a CVD-related discharge diagnosis who left AMA and providers (physicians, nurses and social workers) whose patients have left AMA.
Primary and secondary outcomes To identify patients' reasons for discharges AMA as identified by patients and providers. To identify strategies to reduce discharges AMA.
Approach FGIs were grouped according to patients, physicians and nurses/social workers. A content analysis was performed independently by three coauthors to identify the nature and range of the participants' viewpoints on the reasons for discharges AMA. The content analysis involved specific categories of reasons as motivated by the Health Belief Model as well as reasons (ie, themes) that emerged from the interview data.
Results 9 patients, 10 physicians and 23 nurses/social workers were recruited for the FGIs. Patients and providers reported the same three reasons for discharges AMA: (1) patient's preference for their own doctor, (2) long wait time and (3) factors outside the hospital. Patients identified an unmet expectation to be involved in setting the treatment plan as a reason to leave AMA. Participants identified improved communication as a solution for reducing discharges AMA.
Conclusions Patients wanted more involvement in their care, exhibited a strong preference for their own primary physician, felt that they spent a long time waiting in the hospital and were motivated to leave AMA by factors outside the hospital. Providers identified similar reasons except the patients' desire for involvement. Additional research is needed to determine the applicability of results in broader patient and provider populations.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Prior studies identifying reasons for discharges AMA have not focused on individuals with CVD while reasons may differ in this population compared with a general inpatient sample or to individuals with a history of substance abuse or mental illness.
-
The study identified patients' reasons for discharge AMA following a hospitalisation due to CVD.
-
Reasons were provided by patients who left AMA and by providers (physicians, nurses and social workers) whose patients have left AMA.
Key messages
-
Reasons for leaving AMA included: (1) patients' preference for their own doctor, (2) long wait time and (3) factors outside the hospital.
-
Patients and providers were mostly aligned in identifying patients' reasons for leaving AMA; however, providers did not identify one reason identified by patients: patients' unmet desire to be more involved in their care.
-
The study highlighted the importance of considering patient and provider perspectives when identifying patients' reasons for leaving AMA, some of which can be addressed via improved patient–provider communication during the hospital stay.
Strengths and limitations of this study
-
Strengths of the study included: (1) a focus on a major disease group, that is, responsible for the largest number of discharges AMA among major disease groups; (2) identified care seeking attitudes and motivations that are nearly impossible to identify without direct interviews; (3) included the perspectives of the stakeholders that would need to be involved in any hospital-based intervention targeting discharges AMA, namely patients, physicians, nurses and social workers; (4) focus group sessions were conducted separately for patients, physicians and nurses/social workers in order to facilitate a candid discussion regarding the reasons for patients to leave AMA.
-
Limitations of the study included: (1) low response rate for patient focus groups; (2) patients who did not participate in the FGIs may have identified additional reasons for a discharge AMA that were not captured in this study; (3) did not recruit homeless individuals, who constitute a subpopulation of individuals who leave AMA.
Introduction
Cardiovascular disease (CVD) is the leading cause of hospitalisations in the USA,1 with an estimated direct and indirect cost of $503.2 billion in 2010.2 In 2006, the number of discharges with heart disease as the first-listed diagnosis was 4.2 million.3 However, a proportion of these CVD discharges were against medical advice (AMA), whereby the patient decides to leave the hospital before the discharge has been authorised by the patient's physician.4 National inpatient data from the Healthcare Cost and Utilisation Project Nationwide Inpatient Sample show that diseases of the circulatory system rank first among major diagnostic categories in terms of the number of discharges AMA.5
Recently, the policy focus regarding cost containment and quality improvement has shifted to hospital readmissions. Medicare Administrative Contractors have recently begun informing hospitals that any readmission occurring within 30 days of an acute stay discharge is subject to review and referral to the quality improvement organisation, with a possible payment denial for the second admission, the initial admission or both.6 President Obama's 2010 budget singled out hospital readmissions as the largest source of waste in the American healthcare system and called for initiatives that would save $26 billion over 10 years.6 Discharges AMA in a CVD sample have been demonstrated to be associated with a higher likelihood of hospital readmission for CVD.7
Discharges AMA associated with CVD as well as readmissions resulting from these discharges AMA could be impacted by targeted interventions designed to reduce discharges AMA. However, the design of effective interventions depends on the identification of reasons for discharges AMA.4 In the clinical setting, identifying the reasons for discharges AMA from both patients' and providers' perspectives provides information that can be used to foster shared decision-making8 around the hospital stay, which, in turn, supports8 the delivery of patient-centred care. Patient centred care is defined as care that ‘is respectful of and responsive to individual patient preferences, needs and values’ and that ensures ‘that patient values guide all clinical decisions’.9 Shared decision-making around the treatment plan, including the hospital discharge time, requires input from both the provider and the patient. Thus, it is important to identify reasons for discharges AMA and from both patients' and providers' perspectives.
Reasons for discharges AMA in a general inpatient population,10 ,11 among patients with asthma12 and among patients with a history of psychiatric conditions, drug or alcohol abuse have been identified.13–15 The reasons identified in a general inpatient population and among patients with asthma include (1) drug addiction, (2) pain management, (3) external obligations, (4) wait time, (5) dissatisfaction with care, (6) teaching hospital setting, (7) communication and (8) feeling better.10–12 Factors associated with discharges AMA also have been identified among patients with mental illness or substance abuse and include: young age, single marital status, male gender, comorbid diagnosis of personality or substance use disorders, pessimistic attitudes towards treatment, disruptive behaviour, history of discharges AMA, sickness or death in the family, financial problems, legal issues, provider's failure to orient patients to hospitalisation and failure to establish a supportive provider–patient relationship.13–15
It is not clear to what extent prior findings would translate to a CVD setting, where decision-making could be considered to be relatively more deliberate compared with the broader population of patients who leave AMA, in which mental illness or substance abuse can be more prevalent and could impact decision-making. In order to develop effective interventions that also target discharges AMA in a CVD setting, the reasons applicable to this specific patient population must first be identified. The objective of this qualitative study was to identify reasons for discharges AMA among patients with a CVD admission from the patient's and provider's perspective.
Methods
Participants
Focus group interviews (FGIs) were conducted to explore why patients left AMA following a CVD-related hospitalisation. A convenience sample of patients hospitalised for CVD who left AMA and healthcare providers who treated patients requiring CVD-related care during their inpatient stay were recruited at three area hospitals in Maryland between April 2009 and July 2009. Two patient FGIs, two physician FGIs and three nurse/social worker FGIs were conducted. Patients, physicians and nurses/social workers were interviewed separately in order to facilitate a more candid discussion and reduce social desirability bias as it applies to patients discussing situations that implicate providers, and providers (eg, physicians) discussing situations that implicate patients or other providers (eg, nurses). The study was approved by the University of Maryland Baltimore Institutional Review Board, the Bon Secours Hospital Institutional Review Board and the MedStar Office of Research Integrity.
Patient inclusion criteria required a discharge AMA between 1 July 2006 and 30 June 2008, with a primary admitting diagnosis of CVD (The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM): 390–459). To reduce the likelihood that patients required detoxification or psychiatric services, patients with a non-primary admitting diagnosis of alcohol abuse (ICD-9: 265.2, 291.1–291.3, 291.5–291.9, 303.0, 303.9, 357.5, 425.5, 535.3, 571.0–571.1, 980.x, V11.3), drug abuse (ICD-9: 292.x, 304.x, 305.2–305.9, V65.42) or psychoses (ICD-9: 293.8, 295.x, 296.04, 296.44, 296.54, 297.x, 298.x) were excluded. In addition, patient discharge records with no home address and invalid phone numbers, as well as non-Maryland residents were excluded.
Participant recruitment to the patient FGI was based on an initial invitation letter sent via mail. The objective was to conduct one patient FGI at each of the three participating hospital sites, with a targeted recruitment of 10 patients per FGI for a total of 30 patients. Until we reached a sufficient number of positive responses (ie, 30 positive responses), a follow-up telephone call was made after 1 week of non-response to the initial invitation letter. Clinical directors at the corresponding hospitals contacted healthcare providers (ie, physicians, nurses and social workers) experienced with patients leaving AMA to inform them about the FGI. A $50 honorarium for each participant was set using the wage-payment model.16
Conducting the focus groups
The methodological framework to develop a topic guide was based on the cognitive constructs (perceived susceptibility to health consequences due to discharges AMA, perceived severity of health consequences due to discharges AMA, benefits and costs of discharges AMA) of the Health Belief Model.17 This topic guide was reviewed by clinicians (ES and MRW), a hospital administrator and a health services researcher trained in qualitative analysis (FGP) and was modified as needed to direct the conversation.
Each FGI lasted approximately 1 h. The provider FGIs were held in a convenient hospital location, and the patient interviews were held at facilities outside the hospitals to minimise patient discomfort, given the interview topic. The same moderator (EO) guided all FGIs. Two research assistants attended each FGI. All participants were informed that the discussion would be audio-recorded and that the transcriptions would be anonymous and confidential. Each participant verbally agreed to these conditions.
Analysis
The recordings were manually transcribed by MZ. Each transcription was subject to an additional review for accuracy by EO and EL. The associated audiotapes were subsequently destroyed. A content analysis was performed in order to identify the nature and range of the participants' attitudes. The content analysis involved the research questions motivating the study (ie, to produce enquiry-driven categories of the reasons for discharges AMA as informed by the application of the Health Belief Model) as well as themes that emerged from interview data (ie, to produce thematic categories). Within the context of patient, physician and nurse/social worker FGIs, a complex thematic analysis18 was conducted through immersion in the interview transcriptions to produce inductively identified emergent themes. The content analysis was performed independently by EO, MZ and EL. They compared and condensed their findings into a final analysis report. The researchers were not necessarily searching for convergence in opinions and were just as interested in identifying dissenting opinions. Key concepts were reported through narrative and the use of participants' quotes. Quotes were selected for their relevance and representativeness of the final selected themes, as identified based on thematic- and enquiry-driven categories. Themes were identified separately for the patient groups, the physician groups and the combined nurse and social worker groups.
Results
A total of 120 patients meeting the inclusion and exclusion criteria were contacted by invitation letter. Twenty-seven envelopes were returned due to invalid address, and 63 patients did not respond to the letter. A total of 30 patients responded either to the invitation letter or to the follow-up telephone call. Nineteen patients were placed in scheduled FGIs, with a final participation count of nine patients: seven men, six African-Americans, with mean age of 56 years. A total of 10 physicians (eight men) and 23 nurses/social workers (two men) were placed in scheduled FGIs consisting of two physician-only groups and three nurse/social worker-only groups.
Reasons for discharges AMA
Figure 1 summarises the reasons for discharges AMA among patients with CVD. Three themes were identified across the three types of FGIs (ie, patient-only, physician-only and nurses/social workers-only).

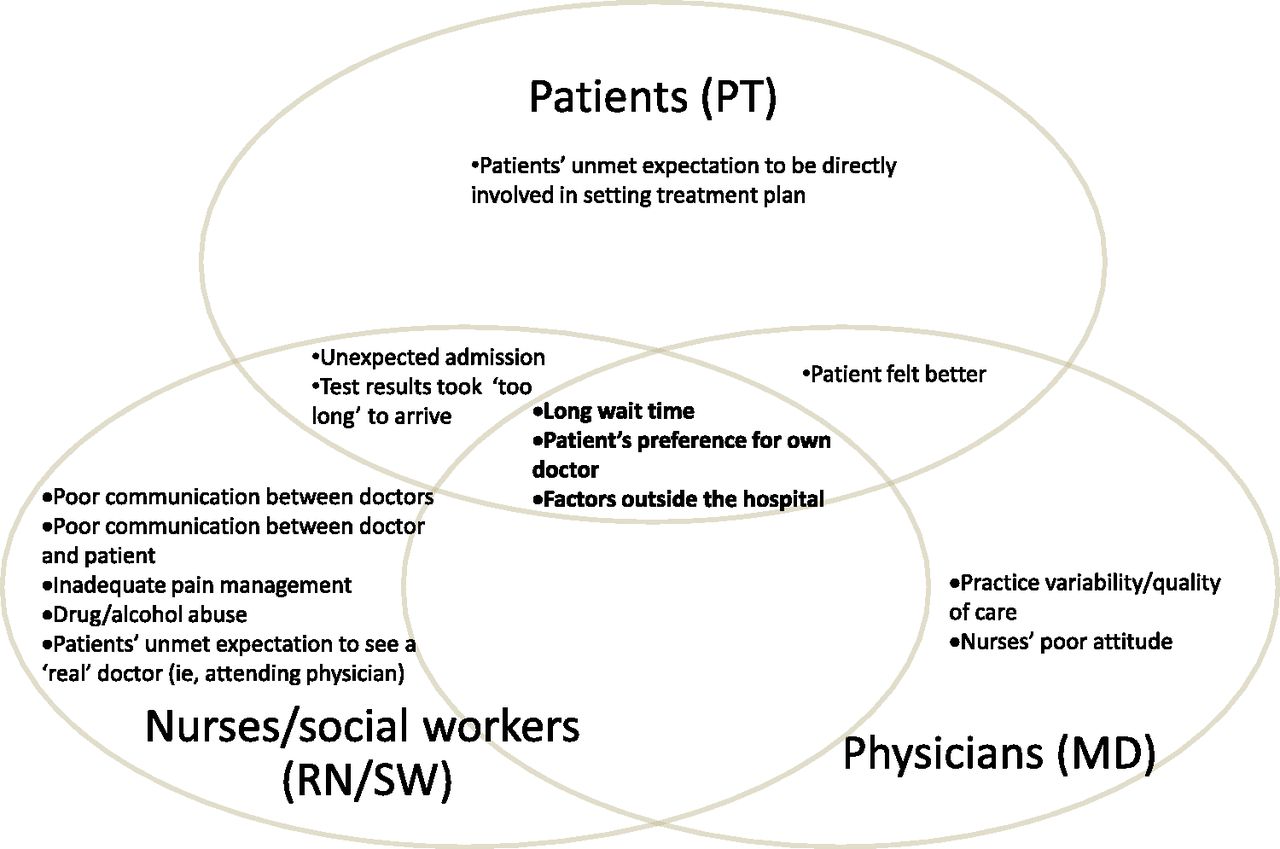{kind=link}
Patient-reported and provider-perceived reasons for discharges against medical advice following a hospitalisation due to cardiovascular disease.
Patient's preference for their own physician/specialist
The patient's lack of access to their own physician or cardiologist during the inpatient stay was identified by patients and providers as a perceived barrier to completing their course of treatment.
Patient (PT): “So he said ‘I'll send you to my heart doctor’, and I said I don't want to go to your heart doctor because I got a specialist myself right in this same hospital. He said ‘I'm not going to discharge you’, and I said… ‘I'm going to go out of here. If that's the way it has to be, I will sign myself out.’ ”
Doctor (MD): “…She had a cardiologist at [Hospital 1], there have been multiple times where the [Emergency Medical Services] brought her [to Hospital 2] because they directed all the ambulance to [Hospital 2],…she was not happy that she was brought to [Hospital 2] in the first place, she had been asking ER [emergency room] doctors to be transferred out to [Hospital 1]. She gave everyone the cardiologist's number, but they were unable to reach the cardiologist. Finally the patient came up to the floor…I explained we tried to call. It was in the middle of the night, so she called her family member and she left AMA.”
Nurse/social worker (RN/SW): “One of the things that I see is that patients frequently have other care systems in place and have come here because their hospital of choice is on red, or they were visiting and admitted here emergently and their home hospital is a medical facility, or their physician is not on staff and won't be following them here, and they have an ongoing relationship with another provider…. and they want to get back to that provider system.”
Long waiting time
Patients and providers identified experiencing a long waiting time as a reason for discharges AMA in the CVD population.
PT: “I laid there for two hours. Nobody came to give me an EKG. It was like they were ignoring me…After I had laid there for about two hours, the pain had stopped,…so I got up and I was leaving.”
MD: “Long wait time in the ER. If we're waiting for a bed to open up, even if they have already been admitted they have already been there for a couple of hours. And then when you go admit them and you do all the work and everything's ready for them to be transferred up to a bed, however the bed is not clean or available and they have to stay in the ER and wait. A lot of patients don't like sitting in the ER waiting for a room to open up as well.”
RN/SW: “You do have patients that have not been seen for 10, 11 h by a doctor.”
“Timeliness I think it's a frustration, as we discussed, length of stay…whether it's having the test ordered, done on the same day, results in a timely manner, so that they're not waiting all day.”
Factors outside the hospital
One barrier to completing the course of treatment identified by both patients and doctors was having ‘something more important to do.’ These activities included taking care of children at home, collecting a pay cheque and paying rent.
PT: “Just one particular time when I signed out, it's because when I came it was the middle of the night, I had to pick up my grandson and I drove myself here and I needed to put my car up so it wouldn't get towed away, and make sure that my grandson was gonna be picked up properly. And I signed myself out, took care of that business, and came back.”
MD: “Some of them get their checks, I think it's on the first day of the month. I'm not sure. So you tend to see on the first day of the month a lot of them are going to leave.”
“I think in the last six to eight months I've seen a lot of more people who are worried about jobs and cannot stay in the hospital because they will lose their jobs.”
RN/SW: “For instance I had a patient who [was admitted for] chest pain….But there is some situation she wants to leave, like she came here at evening time and the doctor wants her to stay here. …She said, ‘My friend told me that he will not stay with my kids, if I don't go home, the social service will come and take my children.’ ”
“Things are not okay at home for them to be in the hospital. So they give it a day or so, and then, ‘I have to get out of here because I have children at home, I have this going on, nobody can pick my children up from school’ or they can't even go to school, so they just can't stay.”
“Actually it's a survival reason for a lot of people. Because they know if they don't pay the rent right now, they're going to get evicted.”
Other reasons
One reason was identified by the patient focus groups but not by the physician or nurse/social worker focus groups. Patients identified an unmet expectation to be involved in decision-making (eg, setting the treatment plan) as a reason to discharge AMA. There were a few reasons identified only by the physician focus groups and not by either patient or nurse/social worker focus groups. These reasons included practice variability and nurses' attitude to patients.
Solutions
Participants were asked to identify strategies and make recommendations for reducing the frequency of discharges AMA. Patients, physicians, nurses and social workers identified a need for improved communication. Patients emphasised that providers should be educated in cultural diversity, interpersonal skills and customer service. Moreover, patients indicated that there should be more truthful and accurate communication from providers regarding the wait time.
Physicians recommended training programmes that would educate providers on what it feels like to be ‘on the patients' side’. They also encouraged thorough communication with patients about their plan of care and the rationale behind the plan, for example, why certain medications are being prescribed or the reasons for fasting before a medical test. They suggested that providers avoid making false promises and provide the patient with documentation regarding the patient's symptoms and plan of care, as a way to keep the patient informed.
Nurses suggested improving the quality of verbal communication in order to better manage patients' expectations provide open dialogue regarding the expected procedures to be performed and minimise making false promises. They also suggested discussing the hospitalisation process and plan of care when the patient is still in the emergency department waiting for a room (as one participant described, “Discharge begins at admission”) and maintain an open line of communication throughout patient's stay. In addition, nurses would like to see a cardiologist providing clinical service in the emergency department in order to address cardiovascular patients' issues earlier on in their hospitalisation process. Finally, nurses recommended that providers establish a relationship with the patient's primary care physician because patients trust their own doctor and might be convinced to stay if the primary physician were in communication with the patient.
Discussion
Several studies have identified reasons for patient discharges AMA based on primary data; however, none were conducted in the CVD setting. Until now, little information has been reported regarding the reasons for a discharge AMA in the CVD setting besides predictive factors consistently found in analyses of secondary data, such as lower socioeconomic status, male sex, younger age, Medicaid or no insurance and substance abuse.19–21 It was unclear to what extent the factors associated with discharges AMA reported in current literature would translate to the CVD setting, where decision-making could be considered to be relatively more deliberate compared with the broader population of patients who leave AMA, in which mental illness or substance abuse would be more prevalent and could impact decision-making. In order to explore reasons for discharges AMA that may arise in the CVD context, we implemented a study focused on patients admitted due to CVD and we expressly excluded individuals with a comorbid condition of mental illness and/or substance abuse. We identified four key issues relevant to the discharge AMA in the CVD setting: (1) patients wanted more involvement in their care; (2) the need to involve the patient's primary care physician or a specialist (eg, cardiologist); (3) obligations outside the hospital setting and (4) long wait time.
Patients were probed to further understand the need for greater involvement in their care. During discussions, patients indicated that they gained knowledge about appropriate care for their CVD condition through repeated exposure to the post-discharge situation. These patients were aware of the implications of their decision to discharge AMA and were willing to take responsibility for their decision. The feeling of ownership was also reflected in their expectations regarding their level of involvement in their care plan: they sought a greater engagement than was offered. The importance of the patient's knowledge base and the patient's broader healthcare institutional context (ie, relationship with specialist provider) in explaining observed discharges AMA requires further study. The study results suggest that patients admitted for CVD conditions and who do not present with mental illness or substance abuse diagnoses may offer different reasons for leaving AMA compared with patient populations that have been the subject of prior studies. A survey of a larger population of patients would be needed to validate these findings.
These descriptions offered by the participants in the patient FGIs are consistent with a healthcare model that regards physicians and other healthcare providers as the content experts, with patients bringing little expertise to the table in terms of managing their illness. However, in the chronic disease setting, a new model of the physician's role has been emerging: people with chronic conditions often manage their condition, and healthcare providers should be consultants supporting them in this role.22 In an American Heart Association (AHA) scientific statement,23 a panel of physicians reviewed the literature on factors that appear to significantly influence patient compliance, such as the patient's knowledge base, historical levels of compliance, the patient's confidence in their ability to follow physician-recommended behaviours, the patient's perception of their health status and the benefits of therapy or behavioural choices, the availability of social support and the complexity of the regimen. The panel recognised that some of those factors were in turn influenced by the patient's relationship and communication with the provider. The AHA guide to primary prevention of CVD24 states, “The physician must commit the time to make a proper assessment and initiate preventive efforts. Patients should be involved in developing an effective plan for change and strategies for altering behavior. A long-term physician-patient relationship is usually needed for successful prevention and modification of risk factors.” In the AHA guidelines for primary prevention of CVD and stroke,25 a panel of physicians summarised, “Primary prevention, by its very nature, requires a lifetime of interactions that virtually define successful provider-patient relationships.” The examples show that successful physician–patient relationship is the key in both preventing and treating CVD.
The translation of these guidelines to the inpatient setting would address many of the gaps in care that were identified during the interviews with patients, physicians and nurses and social workers, namely (1) failure to determine the patient's perception of their health status and of the benefits of remaining in the hospital to complete the stay, (2) failure to involve the patient in developing an effective plan for change and strategies for altering behaviour post-discharge and (3) failure to leverage the successful provider–patient relationships that might already exist between the patient's primary physician or cardiologist. The translation of these guidelines to the inpatient setting also would address four of the eight most important characteristics of high quality and safe care, as identified by patients in a report26 from the Picker Institute (formerly Picker/Commonwealth Program for Patient-Centred Care): respect for the patient's values, preferences and expressed needs; coordinated and integrated care; clear high-quality information and education for the patient and family; continuity, including through care-site transitions.
Evidence from other disease settings supports the utility of leveraging and strengthening patient–provider relationships for creating optimal discharge outcomes. A study investigating racial differences in attitudes regarding CVD prevention and treatment found that the length of relationship between the patient and provider appeared to influence willingness of the patient to accept physician recommendations.27 Patients also want physicians to effectively communicate information to them. A study investigating the physician–patient relationship as a predictor of quality of life of cardiac patients after rehabilitation found that physician's promotion of patient participation has a significant influence on patient's quality of life.28 The quality of patient and provider interactions is critical to the delivery of patient-centred care, which has been shown to improve patient's health outcomes and quality of life.29
Compared with a previous study,10 there was less overlap between patients and physicians with regard to the identified reasons for a discharge AMA. As shown in figure 1, we found areas of overlap and just as many areas of no overlap across the three groups of participants in terms of the reasons for discharges AMA. To the extent that there are gaps between patients and healthcare providers with regard to the perceived reasons for discharges AMA and/or strategies to address discharges AMA, areas of common ground should be identified as the building blocks for developing successful interventions targeting discharges AMA.
The current study has a few limitations. Patients without a documented home address were excluded from the study. With this exclusion, we were unable to recruit homeless individuals, which form a subpopulation of discharges AMA.30 The response rate was fairly low (30 of 93 or 32.3%) and therefore the study sample, based on patient focus groups, should not be considered to be representative of the general population of patients with CVD who discharge AMA. The strength of the focus group methodology lies in the opportunity to explore care seeking attitudes and motivations that are nearly impossible to examine using observational data sets. The patient responses may be subject to non-response bias such that those patients who participated in the FGIs may differ from those who did not participate in the FGIs in terms of the stated reasons for a discharge AMA. While results are not generalisable, the results are novel in that they describe patients' and providers' perspectives on decision-making around discharges AMA among individuals with a CVD-related hospitalisation. The information reported in this study can be used in the design of patient and/or provider surveys, in the design of interventions targeting discharges AMA or in the development of approaches to improve patient–physician, patient–nurse or patient–social worker communication in the inpatient setting.
Conclusions
This study, focused on patients who left AMA after a CVD admission, found that patients wanted more involvement in their own care, voiced a strong preference for their own primary care provider/cardiologist, felt that they spent a long time waiting in the hospital and were motivated to leave the hospital AMA by factors outside the hospital. While some reasons for discharges AMA, such as preference for their own primary provider/cardiologist, long wait time and factors outside the hospital were reported by patients as well as by healthcare providers, other reasons were identified only by the patients. Programmes developed to address discharges AMA should consider the various motivations for discharges AMA across the different disease settings in which discharges AMA occur and, in a first step, build on reasons that have been identified by both patients and healthcare providers. In addition, healthcare providers should continue efforts to understand the patient's goals and objectives regarding their hospital stay, while patients should continue to communicate these goals and objectives to their provider. To this end, reasons for discharges AMA that have been identified only by patients or only by providers deserve due attention since both providers and patients play a critical role in developing and sustaining shared decision-making (and, consequently, shared responsibility) regarding the hospital (length of) stay and discharge outcome.
Acknowledgments
The authors are grateful to Phillip Panzarella, Randolph Whipps and the staff at Franklin Square Hospital, Maryland General Hospital and Bon Secours Hospital. The physician leads at each site were immensely helpful with engaging the appropriate institutional leadership and support personnel, as well as with recruitment. The study would not have been possible without the support and commitment of the physician leads, support staff and focus group participants. We also thank Dr Phillip Panzarella for providing comments on an earlier version of the paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement 1
Footnotes
-
To cite: Onukwugha E, Saunders E, Mullins CD, et al. A qualitative study to identify reasons for discharges against medical advice in the cardiovascular setting. BMJ Open 2012;2:e000902. doi:10.1136/bmjopen-2012-000902
-
Contributors EO was the lead author and is responsible for all aspects of the study. EO, MZ and EL analysed the data. All authors contributed to the study design, interpretation of the results, as well as to the review and editing of the manuscript. All authors approved the submitted manuscript.
-
Funding EO is supported by the National Institutes of Health K12 Career Development Award 1K12RR023250-01.
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the University of Maryland Baltimore Institutional Review Board, the Bon Secours Hospital Institutional Review Board and the MedStar Office of Research Integrity.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional data available.