Article Text

Abstract
Objective A recent study and comprehensive literature review has indicated that mining could be protective against prostate cancer. This indication has been explored further here by analysing prostate cancer mortality in the German ‘Wismut’ uranium miner cohort, which has detailed information on the number of days worked underground.
Design An historical cohort study of 58 987 male mine workers with retrospective follow-up before 1999 and prospective follow-up since 1999.
Setting and participants Uranium mine workers employed during the period 1970–1990 in the regions of Saxony and Thuringia, Germany, contributing 1.42 million person-years of follow-up ending in 2003.
Outcome measure Simple standardised mortality ratio (SMR) analyses were applied to assess differences between the national and cohort prostate cancer mortality rates and complemented by refined analyses done entirely within the cohort. The internal comparisons applied Poisson regression excess relative prostate cancer mortality risk model with background stratification by age and calendar year and a whole range of possible explanatory covariables that included days worked underground and years worked at high physical activity with γ radiation treated as a confounder.
Results The analysis is based on miner data for 263 prostate cancer deaths. The overall SMR was 0.85 (95% CI 0.75 to 0.95). A linear excess relative risk model with the number of years worked at high physical activity and the number of days worked underground as explanatory covariables provided a statistically significant fit when compared with the background model (p=0.039). Results (with 95% CIs) for the excess relative risk per day worked underground indicated a statistically significant (p=0.0096) small protective effect of −5.59 (−9.81 to −1.36) ×10−5.
Conclusion Evidence is provided from the German Wismut cohort in support of a protective effect from working underground on prostate cancer mortality risk.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Prostate cancer mortality in the Wismut cohort of German uranium miners in relation to time spent working underground and the time worked at high physical activity.
Key messages
Evidence is provided from the German Wismut cohort in support of a protective effect from working underground on prostate cancer mortality risk.
Strengths and limitations of this study
The Wismut study is currently the largest Uranium miner cohort.
There is detailed information on the time spent working underground and on other relevant occupational covariables.
However, there is no information on whether the shifts worked were early, late or at night.
Introduction
Prostate cancer is the second most common cancer diagnosed among men (after lung cancer) and is the sixth most common cause of cancer death among men worldwide.1 In the European Union in 2006, prostate cancer was the most common form of incident cancer and the third most common form of cancer death in men (see table 3 of Ferlay et al2). Prostate cancer incidence in Germany has also become the most common form of incident cancer disease in men. It is notable that the prostate cancer mortality rates were approximately constant in the former eastern German Democratic Republic (GDR) between 1960 and 1980 but rose during the same time by 50% in West Germany.3
Prostate cancer is, in general, a slow-growing tumour with a long latency and an uncertain aetiology. The prevalence of latent microscopic prostate tumours has been shown to be quite high in older people in most populations, that is, at least 50% in men over the age of 70.4 Although there are only a few established risk factors for prostate cancer, such as age, race and a family history of prostate cancer,5 there are also several mooted detrimental and protective associations.
The possible detrimental associations include early baldness,6 shift work,7 arsenic exposures,8 diesel fume exposure9 and oestrogen exposures.10 Some evidence exists for radiation-related prostatic detrimental effects from studies on patients after diagnostic radiation procedures,11 occupationally exposed British nuclear workers,12 military and civil pilots and flight attendants,13 and persons exposed by the Chernobyl accident.14 There was little evidence of a prostate cancer risk radiation dose–response in the Japanese A-bomb survivors.15 A recent meta-analysis of 24 cohort studies has concluded that an association of smoking with prostate cancer incidence and mortality exists.16
The possible protective associations include high sexual and/or androgenic levels,17 ultraviolet and/or vitamin D,18 high physical activity (PA)19—although some inconsistent results are observed for PA—and melatonin.20–23 For a cohort of US male health professionals, Giovannucci et al24 reported that for fatal prostate cancer, a recent smoking history, taller height, higher body mass index, family history and high intakes of total energy, calcium and α-linolenic acid were associated with a statistically significant increased risk, but higher vigorous PA level was associated with lower risk.
A recent Australian population-based case–control study and literature review25 has indicated that mining could be protective against prostate cancer. Girschik et al25 concluded that the relationship between mining and prostate cancer could possibly be connected to levels of either PA or changes in melatonin production caused by periods working underground and that these relationships deserve further investigation. Differential risk could not be reported in Girschik et al25 because all but one of the studies reviewed did not report on working periods underground and overground. The main purpose of the present paper is to explore these indications further by analysing prostate cancer mortality risk in a cohort of male mine workers involved in uranium extraction at the former Wismut company in East Germany applying both external (national male rates for the former GDR) and internal backgrounds. New covariables for occupational PA and time spent underground have been specially created for this investigation. Simple standardised mortality ratio (SMR) analyses are complemented by refined analyses done entirely within the cohort.
The German ‘Wismut’ uranium mine workers' cohort has currently been followed up from 1 January 1946 to 31 December 2003, with almost 2 million person-years of observation and has already been described in detail.26 It is currently the largest miners cohort study and several analyses of the detrimental health effects data pertaining to the 58 987 male former employees have recently been published.27–33
There are several occupational risk factors for detrimental health effects, relevant to the cohort members, particularly with respect to lung cancer, including exposure to radon, γ radiation, long-lived radionuclides,34 fine dust, arsenic dust and quartz dust,35 asbestos36 and diesel exposure. However, exposure covariables for the latter two quantities are not available in the cohort data. Previous analyses have shown that the mortality from prostate cancer in this cohort (1960–2006) is notably lower than in the comparison population of the former GDR (SMR=0.88, 95% CI 0.78 to 1.0027). The total absorbed dose to the prostate has not yet been calculated. However, since the absorbed dose to non-respiratory track organs is dominated by external γ radiation and the contributions of radon progeny, radon gas and particularly long-lived radionuclides are expected to be only a few per cent,37 only the γ radiation is explicitly considered here, as a potential confounder. The effective γ doses have been converted into prostate organ dose via voxel model dose conversion factors.38
Materials and methods
Cohort definition, time periods and mortality follow-up
Full details of the cohort have already been given.28 30 Every cohort member contributes to the number of person-years starting 180 days after the date of first employment and ending at the earliest of date of loss to follow-up, date of death or end of follow-up (31 December 2003). Due to the relatively high Percentage of Missing Causes of Death (PMCD) of 37.25% and the systematic variation of PMCD with calendar time from 1946 to 1969, the analyses here are based on the subset of Wismut miner cohort data covering the period 1970–2003 for which the PMCD is 3.56%. Consequently, no corrections for missing causes of death have been made. This difference in PMCD is due to the late start of data collection for this cohort on 1 January 1999, linked with the fact that death certificates were rarely kept by the authorities for more than 30 years.
National rates for the former GDR covering the same calendar year range are applied for the external comparisons. Former disease codes of the comparison external background rates for the GDR were re-coded via earlier ICD revisions to the 10th ICD code,39 which was applied throughout. This recoding process was complicated by several revisions to ICD codes during the period of data coverage and German reunification. Population prostate cancer rates are not available just for the relevant mining region of Thuringia and Saxony. Consequently, the external rates applied here cover the total area of the former GDR (including East Berlin) during the time period 1970–1997; in contrast, from 1998, the rates pertain to the former GDR states and the whole of Berlin. The codes used here in the various time periods are as follows: 1970–1978 ICD 8, code number 185; 1979 ICD 8, code number 179–189 for the urogenital system; 1980–1997 ICD 9, code number 185; 1998–2003 ICD 10, code number C61, all for prostate cancer.
Analysis
The Poisson regression methods applied here require the tabulation of the individual data into grouped data records, as described below and in previous analyses.30–32 This is because the input data for Poisson regression needs to consist of records containing the number of prostate cancer cases, the number of person-years and the mean values of the possible explanatory covariables. Poisson regression is a likelihood-based method for the quantitative analysis of such records or ‘event-time tables’,40 whereby the rates to be modelled are computed as the ratios of prostate cancer cases to person-years for each record in the input data set. Descriptions of the background rates (ie, the spontaneous rates) were necessary to assess the excess risks, whereby such descriptions can either be based on models derived directly from the cohort data (internal comparisons) or from data on the GDR population rates (external comparisons).
Quantitative risk evaluation methods were based on the simple SMR model, where the SMR is the ratio of the observed number of prostate cancer deaths in the cohort to the number of prostate cancer deaths expected in the comparison population (see Breslow and Day, p65–68).40 It is possible that an increased or decreased overall SMR could be a result of either an occupational or lifestyle exposure effect in the data. This can be tested directly by considering the simple SMR model with an exposure response to various possible explanatory covariables, for external and internal comparisons. In the case of the SMR model for external comparisons with an exposure response, a background SMR is computed (ie, the overall ratio of the observed background number of prostate cancer deaths in the cohort to the number of prostate cancer deaths expected in the comparison population) with an additional SMR that is linearly dependent on the covariable of interest.
The more refined analysis entirely within the cohort (internal comparisons) applied Poisson regression excess relative prostate cancer mortality risk model with background rate stratification by age and calendar year and a whole range of possible explanatory covariables: age (a), year (y), γ prostate dose (g), years at medium PA (mpa), years at high PA (hpa), days worked underground (u) and time since either first or last underground shift (t).
Data tabulations
Tabulations of person-years at risk and cancer deaths were created with the DATAB module of the EPICURE software41 for the whole cohort data (1946–2003), so that the covariables of interest could be accumulated from the beginning of the cohort. The period of interest here was then selected to be 1970–2003 during the data analysis and model fitting procedures. Cross-classifications were made by attained age, a, in 16 categories (<15, 15 to <20, 20 to <25, …, 85+ years); individual calendar year, y, in 58 categories, and cumulative γ prostate doses, with a 5-year lag-time (eight categories: 0, >0 to <50, 50 to <100, 100 to <150, 150 to <200, 200 to <300, 300 to <400, 400+ mGy). For the current analysis, new covariables for occupational PA and time spent underground have been specially created. Exact shift information relating to daily underground and overground activities in each calendar year was used. The number of days worked underground in any one calendar year was then accumulated over calendar years of employment in eight categories (0, >0 to <1000, 1000 to <2000, 2000 to <3000, 3000 to <4000, 4000 to <5000, 5000 to <6000, 6000+ days). For the PA categories, information on the job type in each calendar year was extracted from the Wismut records. Each of the several hundred job types had already been classified into three levels of PA corresponding to different breathing rates for the purpose of organ dose calculations, for example, job types hewer, metal worker and lorry driver were classified as high, medium and low PA, respectively. The number of years worked in each of the high and medium PA classes were then accumulated over calendar years of employment, each in eight categories (0, >0 to <5, 5 to <10, 10 to <15, 15 to <20, 20 to <25, 25 to <30, 30+ years). Choice of units (years or days) reflects the quality of the information available in the mining records.
Standardised mortality ratios
Mortality rates observed in the cohort were compared with the GDR external rates. The first stage of the SMR analysis for prostate cancer has been done as described previously for extra-pulmonary cancers28 with some extensions that allow a comparison of internal (miner cohort) and external (former GDR) background (spontaneous) rates. Justifications for the generally preferable internal comparison (done entirely within the cohort), connected with differences in the maturity of the smoking epidemic between the cohort and the GDR, have recently been given.32 The simplest SMR model relates the rates in the population of interest (the miner cohort) to a multiple of the rates from the external population (the former GDR).
If λ*(a, y) denotes the external rates as a function of age and calendar year and λ(a, y) denotes the observed rates in the miners cohort, then the SMR model can be written as
However, it is also possible to fit a RR model
Refined ERR models with background stratification by age and calendar year were employed—if r(a, y, g, mpa, hpa, u, t) is the prostate cancer mortality rate and r0 (a, y) = r (a,y,0,0,0,0,0) is the background disease rate for non-exposed individuals, g =0, mpa =0 … etc then
The γ prostate dose, years at medium PA, years at high PA and days worked underground were each included:
Maximum likelihood with the AMFIT module of the EPICURE software41 was used for estimation of the SMR and ERR fit parameters associated with equations 1–5 above. CIs were computed at the 95% level and the Wald type CIs are given since, although very similar intervals were found with the profile likelihood-based CIs, some of the lower limits could not be numerically calculated with the latter method.
Results
Of the total 58 987 cohort members in the complete follow-up period between 1946 and 2003, 55 435 members were included in the follow-up from 1970, specifically considered in the risk analysis presented here. In total, 20 920 persons were deceased (of which 1560 died before 1970), 35 294 were alive and 2773 were lost to follow-up (of which 1992 were lost before 1970). There were 263 prostate cancer deaths observed during 1.42 million person-years of observation between 1970 and 2003. The cumulative numbers of observed and expected prostate cancer deaths in this period are shown in figure 1A,B as a function of calendar year from 1970 and age attained from 40 years. The absolute number of prostate cancers occurring reaches a maximum in the category 75–80 years of age, due to the age distribution in the cohort, and increases steadily from 1970–2003 and the cumulative number of prostate cancers increases as a function of age attained and calendar year.

(A) The cumulative number of prostate cancer deaths observed in the Wismut cohort and expected from former German Democratic Republic (GDR) rates as a function of calendar year. (B) The cumulative number of prostate cancer deaths observed in the Wismut cohort and expected from GDR rates as a function of age attained.
The mean values (and ranges) of age attained, mean number of days worked underground and mean number of years worked at high PA are 47 (14–103) years, 1649 (0–10 704) days and 3.5 (0–44) years, respectively. Table 1 gives the category-specific values for the number of prostate cancer deaths and person-years, for the number of years worked at high PA and days spent underground categories of mine workers.
Category means and ranges for the number of days worked underground and the number of years worked at high physical activity (PA)
SMR results (comparison of cohort rates with external rates)
The total number of deaths from prostate cancer (1970–2003) observed (O) was significantly lower (p<0.001) than expected (E) from national rates (equation 1). The SMR value with 95% CIs is 0.85 (0.75 to 0.95). Quantitative differences between GDR external rates and internal cohort rates can be assessed directly from a categorical SMR analysis in categories of attained age and calendar year. Some statistically significantly low categorical SMR values were found mainly in the age group 65–75 and in the calendar period from 1991 to 1995 (results not shown). The overall SMR with 95% CIs when recomputed by two categories of below and above mean time spent underground (1649 days) becomes 0.92 (0.76 to 1.07) and 0.79 (0.65 to 0.92), respectively. The SMR recomputed by two categories of below and above mean time worked at high PA (3.52 years) becomes 0.82 (0.69 to 0.94) and 0.91 (0.73 to 1.10), respectively.
Simple ERR parametric cohort risk models (comparison of cohort rates with external rates)
Cumulative exposure effects for various covariables in terms of ERR per unit exposure and 95% CIs are given in the first results column of table 2 (equation 2). The ERR per day worked underground, relative to the external GDR rates, is −4.44 (−7.11 to −1.76) ×10−5 and was found to be the statistically strongest exposure effect (p=0.001), that is, decreased for the number of days worked underground relative to the external rates. A similar value of −3.3 (−7.2 to 0.06) ×10−5 relative to the internal controls was found (table 2, third results column), although of reduced statistical significance (p=0.097). This latter result is connected with a background SMR of 0.93 (0.78 to 1.08) (table 2, second results column). The SMR model did not converge (NC) for the γ prostate dose relative to the external background rates. A statistically significant (p=0.03) decreased ERR/Gy for prostate γ doses, relative to the internal background of −1.27 (−2.4 to −0.14), was also found (table 2, third results column).
Results of fitting the models
Refined ERR parametric cohort risk models
The statistical significance of ERR/Gy for prostate γ doses reported with the simple analysis was not confirmed by the refined analysis (ERR/Gy=−1.18 (−2.4 to 0.02), see table 2, fourth results column) (equations 3–5). Although the coefficient for γ dose was of borderline statistical significance in the univariate model, the forward selection did not keep the γ prostate dose in the multivariate model. A preferred model by forward selection of the covariables γ prostate dose, g; years at medium PA, mpa; years at high PA, hpa, and days worked underground, u, taken linearly one or two at a time was found to be the model that included both hpa and u (table 3). This model had a reduction in deviance with respect to the stratified background model of 6.5 (p=0.04) by the likelihood ratio test. This model provided the results in the last column of table 2 (with 95% CIs) for the ERR per day worked underground, which indicates a statistically significant (p=0.01) small decreased effect of −5.59 (−9.81 to −1.36) ×10−5, and for the ERR per year worked at high PA, which indicates a statistically significant (p=0.04) small detrimental effect of 0.021 (0.001 to 0.040). The clinical significance of the results can be assessed by obtaining the number of deaths from prostate cancer prevented in this cohort from working underground, obtained from the fitted background and fitted excess number of cases in the preferred model. Depending on whether the slightly increased risk from high PA is accounted for or not, this number is either 14 or 22 prostate cancer deaths, respectively.
Results of applying model selection techniques with the likelihood ratio test for variable selection
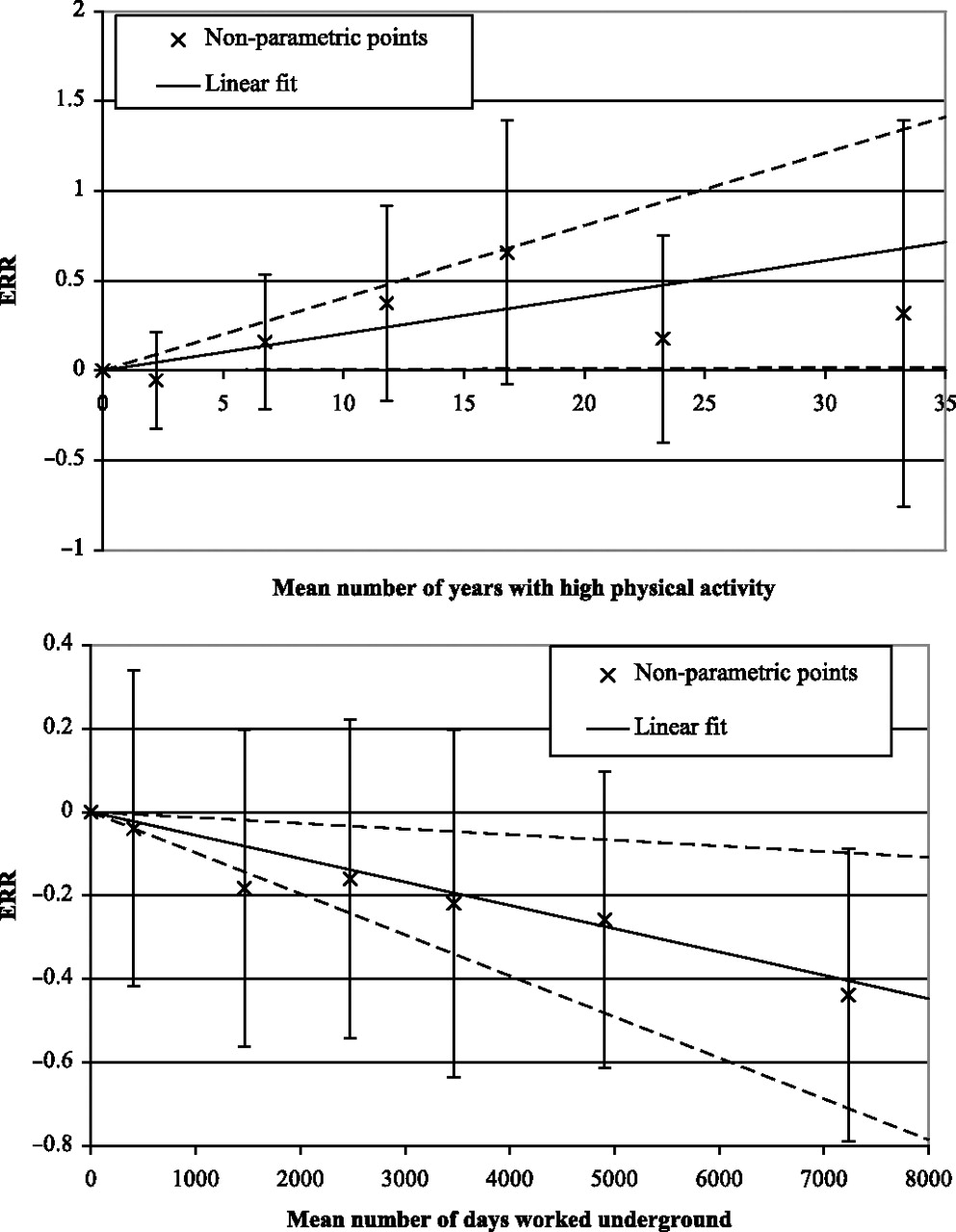
Models that included just hpa or just u did not result in statistically significant risks (table 2, fourth results column) or lead to statistically significant model improvement (table 3). No evidence for an interaction between hpa and u was indicated by including a cross term in the preferred model (p>0.5). Testing of the quadratic or parabolic forms for hpa and u or testing risk effect modification by attained age (table 3) or time since first or last underground shift (results not shown) did not lead to statistically significant model improvement. The dose–response forms for the preferred model and the adjusted non-parametric risks with 95% CIs are shown in figure 2. It was not possible to confirm this result by backwards selection since the models with all six main covariables failed to converge.

{kind=link}
{kind=link}
The upper panel shows the excess relative risk (ERR) and 95% CI as a function of mean number of years with high physical activity (PA) and corresponds to the risk given in the last column of table 2. The non-parametric points with 95% CI are adjusted for mean number of days worked underground. The lower panel shows the ERR and 95% CI as a function of mean number of days worked underground and corresponds to the risk given in the last column of table 2. The non-parametric points with 95% CI are adjusted for mean number of years with high PA.
Discussion
The Wismut cohort is one of the largest single occupational cohorts and one of only a few cohorts with detailed information on the number of shifts worked underground. Although the number of shifts was documented, it is not known if these were early morning, daytime or night shifts. A substantial proportion (25%) of person-years are contributed by mine workers who did not work underground, which generally ensures the stability of analyses based on internal rates. The ERR per unit of various exposures have been modelled relative to the internal rates and relative to the external rates for the general population of the former GDR.
A statistically significant (p=0.001) negative response for the ERR per day worked underground, when modelled in relation to the general population of the former GDR, is reported here. There are some indications of unit exposure responses of the ERR which are decreased for γ prostate dose (p=0.03 and 0.055 for the simple and refined models, respectively) with respect to the internal rates. Rather than being decreased, the γ dose is a possible proxy variables for the number of days worked underground since there are moderate degrees of correlations between these covariables (ρ=0.68 for the correlation between time-dependent cumulative γ prostate doses and the number of days worked underground, see also table 1). Indication that the γ dose may be acting as a proxy was tested here directly by the creation of new categories of mine workers, with numbers of years worked at high or medium PA and the number of days worked underground and the application of model selection techniques.
The assumption is made in this paper that radon and long-lived radionuclides make only minor contributions to the total prostate dose. Previous analyses have shown that the ERR per 100 WLM of radon exposure, based on internal Poisson models, was not elevated for prostate cancer (ERR/100 WLM =0.000, 95% CI, −0.024 to 0.024).31 None of the radiation covariables (ie, γ prostate dose but also including long-lived radionuclides and radon), when tested by inclusion singularly as linear risks in refined internal Poisson regression models, resulted in a deviance drop of more than three with respect to the background model which was stratified on age attained and calendar year.
A linear ERR model with the number of years worked at high PA and the number of days worked underground as explanatory covariables provided a statistically significant fit when compared with the background model (p=0.039). Results (with 95% CI) for the ERR per day worked underground indicated a statistically significant (p=0.01) small decreased effect at −5.59 (−9.81 to −1.36) ×10−5 and for the ERR per year worked at high PA, a statistically significant (p=0.04) small detrimental effect at 0.021 (0.001 to 0.040). This main result provides new evidence in support of the decreased effect of working underground which is manifested with respect to the internal and the external rates.
The number of days worked underground is connected with a particular hypothesis for reduced prostate cancer rates, for example, melatonin production rates (as described in detail in Girschik et al25 and references therein). In summary, melatonin has been shown to have anti-cancer properties acting through several mechanisms.20–23 The production of melatonin in the pineal gland is regulated by the natural diurnal light-level cycle, with suppressed production during the day, which is restored at night. Underground miners on day shifts would have a reduced exposure to visible light leading to an extended melatonin production period.
The relation between PA and prostate cancer risk was classified as ‘probable’ with respect to decreased risk, by the IARC in 2002,42 but no definite mechanisms have been identified for a relation between PA and prostate cancer. Several plausible mechanisms have been postulated which include modulation of testosterone and vitamin D levels by PA, a link between physical inactivity and overweight/obesity and a beneficial modulation of immune function through exercise (see Lee et al43 for a review). A recent systematic review and meta-analysis44 considered 13 studies with occupational PA, considered to be ‘higher quality’ studies and reported that nine studies gave a decreased risk, one study an increased risk and three studies reported no association. Two other studies have reported increased risks: Hosseini et al45 found that intensity of occupational PA was associated with increased prostate cancer risk and Zeegers et al46 reported an increased risk for obese men (body mass index over 30) who were physically active for more than 1 h/day and in men with high background energy intake.
A statistically significant increase in risk with increasing high PA is observed here, in contrast to the IARC classification and the majority of other studies. It is important to note that the variable PA here measures only part of the total PA and could be prone to misclassification. The PA variable is limited to the work period at the Wismut company (the mean duration of work at the company, 14 years) and no leisure time activities could be considered. The classification is simply based on job type without consideration of possible changes in PA in a specific job over time, for example, due to improved technical ‘labour-saving’ equipment. PA could also be an indicator of socioeconomic status because the jobs with low PA are more likely to be associated with higher education.
Another possible source of bias in the results based on external comparisons that should be considered is the selection bias known as the healthy worker effect. However, this effect, which can generally lead to occupational cohorts presenting mortality risks less than the general population, is not indicated since the risks are similar with respect to internal and external backgrounds. The occurrence of this form of bias could also be tested here by considering all solid cancer minus the sites that have already been linked to the main mine radiation exposure, that is, radon (lung, larynx, tongue, mouth and pharynx). For this group of cancers, the SMR with 95% CI is 1.01 (0.97 to 1.04) also indicating that the healthy worker effect is not having a significant influence on the prostate cancer results in this cohort.
A further source of bias, possibly affecting the decrease in risk with increasing duration of working underground based on internal comparisons, could be the healthy worker survivor effect. Unhealthy workers may move from working underground to working at the surface. Consequently, the duration of working underground may be higher in the healthy group compared with the unhealthy group, leading to artificially decreased effects in relation to duration of working underground. However, this effect has been tested for by fitting the preferred model, which included both the number of days worked underground and number of years worked at high PA, to the subgroup of all solid cancers minus the sites that have already been linked to the main mine radiation exposure (lung, larynx, tongue, mouth and pharynx) and minus prostate. No significant trends were found (p>0.5 for the linear trend of ERR with respect to the number of days worked underground and p=0.11 for the linear trend of ERR with number of years worked at high PA) indicating that the healthy worker survivor effect is not directly biasing the results for prostate cancer.
Although there is no general consensus as to whether radiation exposure is associated with prostate cancer risk,47 an x-ray procedure risk doubling dose of about 20 mGy for prostate cancer incidence has been reported.11 The magnitudes and ranges of the γ prostate doses in the Wismut study (with the prostate cancer mortality cases having a range up to 444 mGy and the cohort person-year weighted mean γ prostate dose of 34 mGy) should be large enough to find such an increased risk at the 20 mSv level, given the similar relative biological effect of x-rays and γ rays. However, a γ risk, at this 20 mSv level, has not been found in the Wismut cohort data for prostate cancer mortality.
Yang et al8 reported that SMRs for prostate cancer declined gradually in an SW coastal district of Taiwan after the arsenic-contaminated artesian well drinking water supply was improved to a tap-water system. Since arsenic dust exposures are also available for the Wismut miners,35 an arsenic covariable could be added to the preferred model for PA and time worked underground described above in a subsidiary analysis, but this only resulted in a deviance drop of 1.2 and a p value of 0.33 for the associated arsenic risk coefficient and did not confound the main risks from the preferred model.
An examination of the effects of smoking on the risk of prostate cancer mortality, as indicated in Huncharek et al,16 could not be carried out for the Wismut cohort due to only a very limited amount of information on smoking being available.29
Although there were 264 prostate cancer deaths in the whole cohort, only one occurred before 1970, that is, during the period with a higher percentage of missing causes of death. This is consistent with prostate cancer generally being a type of cancer that occurs predominantly in old age coupled with the observation that—due to miners entering and leaving the cohort at various points in time during the follow-up period—the cohort aged, on average, at half the rate of any individual, that is, in 1960 and 2003, the mean ages of cohort members were 35 and 57 years, respectively. Consequently, it is very important to continue work on extending the current follow-up period.
Conclusions
This work has extended the evidence in support of a decreased, possibly protective, effect for prostate cancer mortality from working underground provided in25 and could be interpreted as support for ‘The Melatonin Hypothesis’. A linear internal excess RR model with the number of years worked at high PA and the number of days worked underground as explanatory covariables provided a statistically significant fit when compared with the background model (p=0.039). Results (with 95% CI) for the ERR per day worked underground indicated a statistically significant (p=0.0096) small decreased, possibly protective, effect at −5.59 (−9.81 to −1.36) ×10−5. It is this main result that provides the new evidence in support of the protective effect of working underground which is also manifested with respect to the external rates. Additional computations made to examine the influence of biases due to the γ doses, the healthy worker selection effect and the healthy worker survivor effect indicate that the results are unbiased in these respects, but the effects of such biases cannot be entirely excluded.
Acknowledgments
The authors thank the German Federation of Institutions for Statutory Accident Insurance and Prevention (DGUV) and the Miners' Occupational Compensation Board (Bergbau Berufsgenossenschaft) for their continuous support over many years. The fieldwork for the follow-up was conducted by I+G Gesundheitsforschung and Mediveritas GmbH. Their commitment helped to achieve the low percentage of lost to follow-up. We also thank the members of the Wismut Working Group of the German Radiation Protection Commission for their continued advice. Thanks are also to Dr Nina Petoussi-Henss for providing the γ dose factor for converting effective dose to organ dose. We would also like to thank Professor Donald A. Pierce for useful discussions and three reviewers for comments and suggestions that lead to an improved paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement 1
- Data supplement 2 - Online table 1
Footnotes
To cite: Walsh L, Dufey F, Tschense A, et al. Prostate cancer mortality risk in relation to working underground in the Wismut cohort study of German uranium miners, 1970–2003. BMJ Open 2012;2:e001002. doi:10.1136/bmjopen-2012-001002
Contributors The first author conceived the idea for the publication, did the risk analysis and wrote the first draft of the paper. The coauthors prepared the data for analysis and contributed to all discussions and subsequent drafts of the paper.
Funding EU Alpha-Risk project and the Federal Ministry of Education and Research (BMBF), Germany (Competence Network Radiation Research).
Competing interests None.
Ethics approval The German Federal Commissioner for Data Protection and Freedom of Information has issued a special approval for this research, which constitutes an exemption from the necessity to obtain human subjects approvals.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Wismut epidemiological data can be made available to interested scientists through an application procedure to the German Federal Office of Radiation Protection (BfS) (please see the BfS website at http://www.bfs.de and look at the ‘Wismut’ section, http://www.bfs.de/en/bfs/forschung/Wismut/Wismut_cohort_proposals.html).