Article Text

Abstract
Objectives Real-life data on response to Botulinum toxin A (BoNT-A) in cervical dystonia (CD) are sparse. An expert group of neurologists was convened with the overall aim of developing a definition of treatment response, which could be applied in a non-interventional study of BoNT-A-treated subjects with CD.
Design International, multicentre, prospective, observational study of a single injection cycle of BoNT-A as part of normal clinical practice.
Setting 38 centres across Australia, Belgium, Czech Republic, France, Germany, The Netherlands, Portugal, Russia and the UK.
Participants 404 adult subjects with idiopathic CD. Most subjects were women, aged 41–60 years and had previously received BoNT-A.
Outcome measures Patients were classified as responders if they met all the following four criteria: magnitude of effect (≥25% improvement Toronto Western Spasmodic Torticollis Rating Scale), duration of effect (≥12-week interval between the BoNT-A injection day and subject-reported waning of treatment effect), tolerability (absence of severe related adverse event) and subject's positive Clinical Global Improvement (CGI).
Results High rates of response were observed for magnitude of effect (73.6%), tolerability (97.5%) and subject's clinical global improvement (69.8%). The subjective duration of effect criterion was achieved by 49.3% of subjects; 28.6% of subjects achieved the responder definition. Factors most strongly associated with response were age (<40 years; OR 3.9, p<0.05) and absence of baseline head tremor (OR 1.5; not significant).
Conclusions Three of four criteria were met by most patients. The proposed multidimensional definition of response appears to be practical for routine practice. Unrealistically high patient expectation and subjectivity may influence the perception of a quick waning of effect, but highlights that this aspect may be a hurdle to response in some patients.
Clinical registration number (NCT00833196; ClinicalTrials.gov).
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Development and application of a novel multimodal definition of treatment response in a non-interventional study of patients with CD administered BoNT-A in routine clinical practice.
Key messages
Magnitude of effect, subject satisfaction and safety profile are appropriate measures of BoNT-A response in patients with CD.
A multidimensional definition of response enables comprehensive evaluation of treatment response that is not achievable with a single measurement criterion.
Strengths and limitations of this study
This is a large-scale study of CD patient demographics and BoNT-A response in a real-life clinical setting.
The subjective nature of self-reported waning of treatment effect is potentially vulnerable to bias as a result of high patient expectation, which constrains its use as part of the challenging multidimensional definition of response.
Introduction
Cervical dystonia (CD) is the most common of the focal dystonias,1 with a prevalence of 89 per million in parts of the US (Rochester, Minnesota).2 Any muscle in the neck may be abnormally contracted in CD. Sets of contracted muscles can be found in isolation but are most commonly found in combination.3 The majority of cases (∼66%) present with rotational torticollis and laterocollis.4 Classification of CD is based on the primary (idiopathic) or secondary aetiology (eg, dystonia because of a brain tumour).5
Botulinum toxin A (BoNT-A) is a neurotoxin that is isolated and purified from Clostridium botulinum type A bacteria and has gained increasing acceptance as a first-line treatment option for CD.6 There is a substantial body of evidence from clinical studies to support the use of BoNT-A in patients with CD.5 ,7–9 There are currently three major commercially available preparations of Type A toxins: abobotulinumtoxinA (Dysport®, Ipsen, Boulogne-Billancourt, France), onabotulinumtoxinA (Botox®, Allergan Incorporated, Irvine, CA, USA) and incobotulinumtoxinA (Xeomin®, Merz Pharmaceuticals GmBH, Frankfurt, Germany), which differ in their potency; thus, the units of each preparation are not directly interchangeable. BoNT-B has also gained acceptance in the treatment of patients with CD resistant to treatment with BoNT-A.10
The administration of BoNT-A in practice does not reflect the standardised methods adopted in clinical studies because injection schemes are individually determined by the physician. Moreover, BoNT-A administration protocols for CD are not standardised to the subtypes of the condition (ie, predominant and secondary components for head and neck deviations). Although the efficacy and safety of BoNT-A is widely accepted according to robust and well-designed clinical trials, these studies assessed efficacy using mainly Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) or Tsui scale in highly selected patients, which may not relate to real-life practice with individualised patients.
In clinical practice, assessment of BoNT-A effectiveness is multidimensional and cannot be limited to TWSTRS or Tsui scale only, but data on efficacy and safety of BoNT-A in real-world settings are lacking. There is, therefore, a clinical need to pragmatically describe the management of CD subtypes innovatively, taking into account several dimensions of interest for physicians, such as patient's satisfaction, and to establish a robust definition of response to BoNT-A treatment in the real-life management of patients with CD. A meeting of experienced neurologists from France, Germany, Italy, Russia, Spain, Thailand and the UK was convened in 2008, with a view to reaching a consensus on a definition of treatment response, a definition currently lacking in the clinical management of patients with CD receiving BoNT-A. The expert group identified the most relevant predominant and secondary components for head and neck deviations and concurred in proposing a new multidimensional definition of response, which was based on combined aspects of efficacy and tolerability and assessment of global improvement. We present, herein, findings from the application of this novel definition of treatment response in a non-interventional study of subjects with CD who were administered BoNT-A. In this study, the primary objective was to estimate the responder rate following one BoNT-A injection cycle administered via routine practice. Prognostic factors for response were evaluated as an additional exploratory analysis.
Subjects and methods
Study design
This was an international, multicentre, observational, prospective, longitudinal study. Informed consent was obtained prior to subject enrolment and prior to any data collection. Independent Ethics Committee/Institutional Review Board approval in each country was obtained prior to study initiation.
Study population
This study enrolled subjects ≥18 years old, suffering from idiopathic CD with a TWSTRS severity score ≥159 and a ≥12-week interval between the last injection (BoNT-A or BoNT-B) and the first study visit.
To create a homogeneous population for study, subjects with secondary CD were excluded from the study, as were subjects with contraindications of BoNT-A treatment.
Study treatment
The decision to prescribe a BoNT-A preparation was taken prior to, and independently from, the decision to enrol the subject in the study. In order to avoid bias in the recruitment of subjects, physicians were not allowed to choose their subjects but were asked to include consecutive subjects during BoNT-A consultations.
The prescribing of BoNT-A was made in accordance with routine clinical practice and investigators were free to choose: the targeted muscles from the clinically indicated neck muscles; BoNT-A preparation; and injected dose number of points and volume per point. Subjects received a single injection cycle as part of normal clinical practice. Concomitant therapy was permitted throughout the study.
Study assessments
Subjects were assessed during their usual centre visits at the inclusion visit (visit 1; week 0), follow-up visit (visit 2; 3–6 weeks after injection) and end-of-study visit (visit 3; 12–16 weeks after injection). Efficacy assessments encompassed clinical assessment, assessment of CD using the TWSTRS total score (recorded at all visits)11, assessment of tremor using the Tsui Tremor subscale (recorded at all visits)12, assessment of Clinical Global Improvement (CGI) by both investigator and subject (recorded at visit 2) and CD Impact Profile-58 (CDIP-58) (recorded at visits 1 and 2).13 The CDIP-58 comprises a 16-item health-related quality of life (HRQoL) questionnaire encompassing domains relating to head and neck symptoms experienced by the subject, impact on usual daily activities, physical activities, sleep, social activities and emotions/psychosocial functioning. Scores for items within domains were summarised into eight subscale scores, each ranging from 0 to 100 (higher scores indicate worse health).
The primary end point of this study was the percentage of responders after one BoNT-A injection cycle. Response was defined using the ambitious hypothesis for a multidimensional definition of response developed by experienced neurologists, whereby subjects were classified as a responder if they met all the following criteria: (1) magnitude of effect: ≥25% improvement on TWSTRS severity scale at visit 2 (peak effect) or visit 3 (if visit 2 was not performed), compared with visit 1, as reported by Truong et al9; (2) duration of effect: ≥12-week interval between the BoNT-A study injection day and the day the subject reports a clinically relevant waning of treatment effect, justifying a reinjection cycle as reported by Ranoux et al14; (3) good tolerance: no treatment-related severe adverse event (AE) reported during the study and (4) improvement in subject-rated CGI score at visit 2 and visit 3 (equal to either +2 (much improved) or +3 (very much improved)).
Secondary efficacy outcomes included improvements in TWSTRS total and Severity, Disability and Pain subscale scores, tremor (as measured by Tsui score) and CDIP-58.
Only AEs considered by the investigator to be related to study drug were collected during this study, which is in line with current clinical practice. Investigators were asked to report, to the safety department of the BoNT-A manufacturer, any adverse drug reactions using the usual process for such reactions. More specifically on visits 2 and 3, investigators were also requested to document the occurrence and intensity (severe or not) of dysphonia, dysphagia, neck muscle weakness and other.
Study size
The sample size was determined based on both the primary and exploratory objectives (prognostic factors for response). Considering an anticipated rate of responder of 50%, using an estimate for this proportion with a precision of 5%, the required sample size was determined to be 385 subjects (assuming a two-sided 95% CI). When considering the objective related to the detection of prognostic factors (assuming α=5%, power=80%), in order to ensure the ability to detect OR ≥2 and a probability to be exposed to any given level of a prognostic factor larger or equal to 1/3 (=imbalance), the required sample size is 366 subjects. Thus, in order to ensure 385 evaluable subjects, 400 subjects were included in this study.
Statistical analyses
The safety population consisted of all subjects who received one BoNT-A injection, whereas the efficacy population comprised all subjects in the treated population for whom there were data for each of the four underlying variables for response. The responder analysis was performed using the efficacy population, and all secondary end points were assessed using the safety population.
The primary end point was summarised overall, and by each of the four criteria, as the percentage of responders as a point estimate and its associated 95% CI. Responder subgroup analyses were also performed to investigate response based on the following criteria: predominant component of head/neck rotation, BoNT-A preparations, duration of CD, previous BoNT-A use, dystonia localisation (head/neck, trunk, limbs), presence of tremor based on the Tsui scale, use of electromyography and use of concomitant therapies at baseline.
As an exploratory analysis, a stepwise multivariate logistic regression analysis was performed on the efficacy population to assess prognostic factors for response using subgroup variables, as well as additional demographic and disease characteristics variables. ORs with 95% CI estimated by the logistic model were calculated using the primary criteria; a lower 95% CI bound >1 indicated a significantly increased chance of being a responder.
No estimations were made for missing data, and there was no controlling for confounding factors.
Results
Subject population
Between 19 February 2009 and 12 February 2010, 404 subjects from 38 centres in nine countries (Australia, Belgium, Czech Republic, France, Germany, The Netherlands, Portugal, Russia and the UK) were enrolled and followed in this study. A total of 379 subjects (93.8%) completed the study. The most common reason for not completing the study was loss to follow-up (3.2%; n=13); no subjects discontinued due to lack of efficacy. The safety population included all subjects treated with BoNT-A (n=404), whereas the efficacy population included all subjects treated with BoNT-A for whom data were available for each of the four criteria for the primary end point (n=367).
Baseline demographic and disease characteristics are shown in table 1. The majority of subjects were women (64.9%), aged 41–60 years (52.5%) and had suffered from CD for >1 year (90.9%). Nearly all the subjects had sporadic CD (94.8%), and focal dystonia predominated (91.6%). In the few cases of segmental/multifocal dystonias, the upper limb was the most frequently impaired segment. The most common predominant component of CD was rotation (72.8%), followed by laterocollis (14.1%). The majority of subjects had secondary components (83.9%).
Subject demographics and CD characteristics (safety population)
Treatment history
Most subjects had previously received a BoNT-A injection (84.9%). A minority of patients had prior history of treatment with BoNT-B (5.7%). Of the safety population, more than half of subjects (n=215; 53.2%) had previously received benzodiazepines for the treatment of CD and approximately one-third (29.7%) continued to receive these agents after BoNT-A treatment. Prior physical therapy was reported in 49.8% of subjects, but only 14.6% of subjects were receiving physical therapy at the inclusion visit. Analgesics had been previously taken by 40.8% of subjects, with 18.3% of subjects receiving analgesics at the inclusion visit.
Injection schemes
Physicians prescribed three BoNT-A preparations: Dysport (n=279, 69%), Botox (n=113, 28%) and Xeomin (n=12, 3%), independently from study enrolment, as per local clinical practice at the centre. Subjects received Dysport and Botox at median doses of 500 and 160 units, respectively. Overall, 90% of patients received <1000 U of Dysport and 300 U of Botox. In total, the median number of injected muscles was four, of which, the most frequently injected muscles in both the Dysport and Botox groups were the splenius capitis, sternocleidomastoid and trapezius. For Xeomin, the median dose was 200 units, although small patient numbers make results difficult to interpret. Investigators used electromyography during administration of at least one muscle in 185 subjects (46.0%).
Efficacy
Responder analysis
The percentage of subjects meeting the response criteria, as well as each of the individual response criteria, is shown in figure 1. Three criteria out of four were achieved in the majority of patients, as shown by 97.5%, 73.6% and 69.8% of subjects achieving the criterion of magnitude of effect, tolerance (absence of severe related AEs) and subject's CGI, respectively. A total of 49.3% of subjects achieved response based on the duration of effect criterion (≥12 weeks between inclusion and subject-rated waning of treatment effect). Overall, 28.6% (95% CI 24.0% to 33.5%) of subjects were classified as responders to treatment. Evaluation of response by TWSTRS, tolerance and CGI improvement alone (ie, exclusion of duration of effect) established 58.3% (95% CI 53.1% to 63.4%) of subjects as responders.

Responder analysis. AEs, adverse events; CGI, Clinical Global Improvement; TWSTRS, Toronto Western Spasmodic Torticollis Rating Scale.
Responder subgroup analysis
Analysis of the response criteria by subgroup is shown in figure 2 and showed that there were variations in response, albeit these results were not statistically significant. Data revealed that more subjects responded among subgroups presenting with laterocollis (41.7% vs 26.7% with rotation), without baseline tremor (33.2% vs 23.7% with tremor), and those not receiving concomitant medication at baseline (35.1% vs 22.8% receiving baseline concomitant medications).

Subgroup analyses of responders (efficacy population). BoNT-A, Botulinum toxin A; CD, cervical dystonia; EMG, electromyography.
Prognostic factors associated with response
The multivariate logistic regression showed that the most strongly associated factor to response was age (<40 years; OR 3.9, p<0.05). Additional trends with a lower magnitude of association were observed (data not shown).
Secondary efficacy outcomes
Secondary efficacy outcomes are shown in table 2. Subjects reported a notable improvement in TWSTRS total score and subscale scores over the course of treatment, as indicated by the percentage change in scores at each visit. Sixty-six of the 181 subjects (36.5%) with baseline tremor no longer presented with tremor at visit 2. HRQoL improved following BoNT-A treatment, as demonstrated by decreases in all eight subscores of the CDIP-58 at visit 2.
Efficacy outcomes
Safety and tolerability
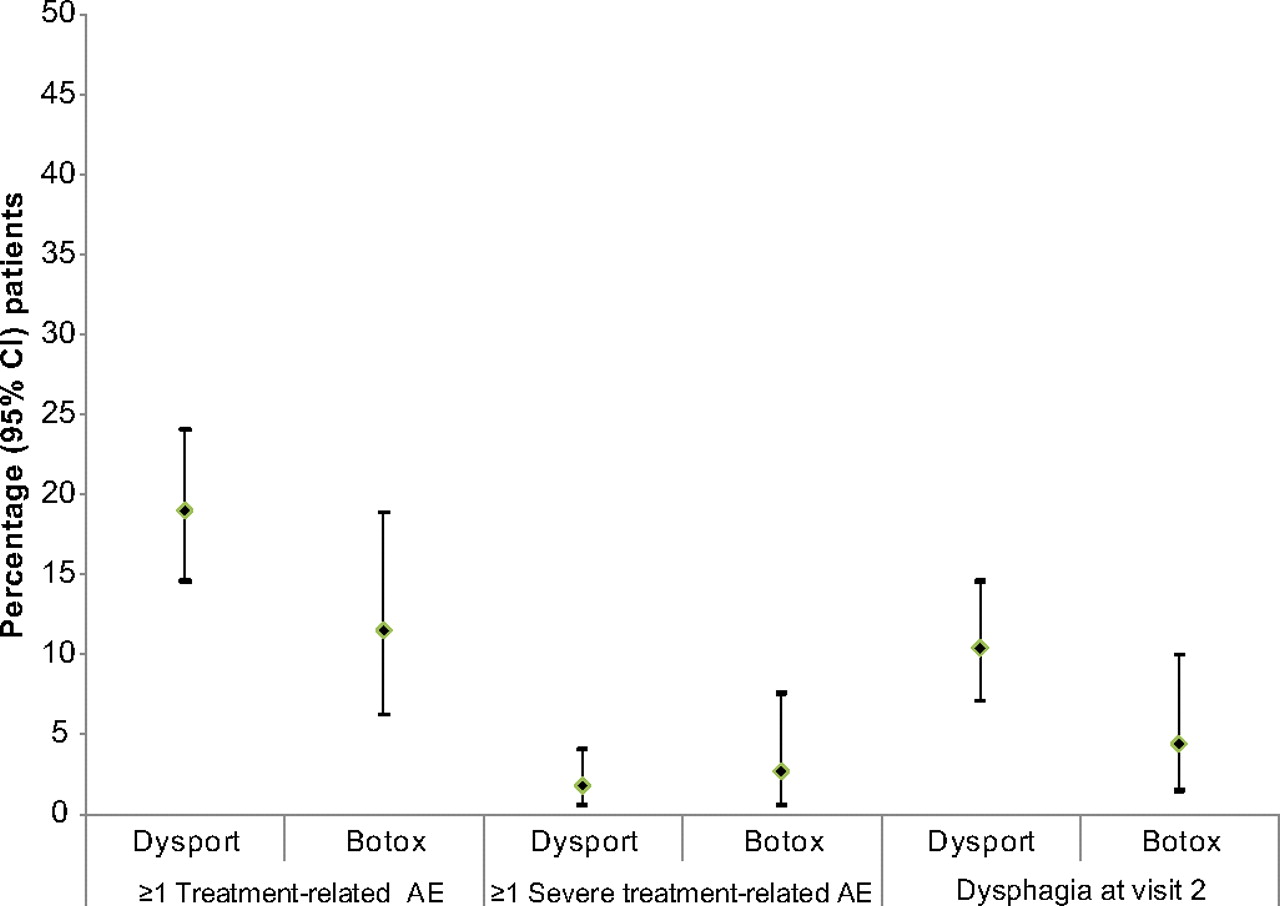
A total of 88 treatment-related AEs were reported during the study. Overall, 68 subjects (16.8%) experienced at least one treatment-related AE. Of the observed AEs, dysphagia was the most commonly reported (9.2%). Overall, 10 treatment-related AEs were considered to be severe, with neck muscle weakness (n=4) being observed as the most common AE at this grade of severity. The incidence of AEs (severe and not severe) and dysphagia did not statistically differ between BoNT-A preparations (figure 3).

{kind=link}
{kind=link}
{kind=link}
Occurrence of AEs with frequently used BoNT-A preparation. AEs, adverse events; BoNT-A, Botulinum toxin A.
Discussion
In this non-interventional study of subjects with CD in routine practice, the majority of subjects were middle-aged women. These demographic data were in accordance with a typical population of subjects with CD.15 TWSTRS and CDIP-58 scores at baseline reflected a population with moderate to severe CD severity.
Real-life data on response to BoNT-A in CD are relatively sparse,16–18 and studies evaluating multidimensional definitions of response, in particular, are lacking. Therefore, the primary objective of this study was to estimate the rate of response following one BoNT-A injection cycle in real-life practice using a challenging multidimensional definition developed by an expert group of neurologists. To our knowledge, this is the first such non-interventional study to apply a consensus-based multimodal definition of response to a large real-world population of patients with CD treated with BoNT-A. In the interpretation of our findings, it should be borne in mind that clinical studies have commonly utilised a single or co-primary end point.19 ,20 Thus, the requirement to achieve four primary end points within the multidimensional response definition proposed in this study represented a significant challenge. Notably, this ambitious definition for response was achieved by almost one-third (approximately 30%) of the 404 subjects who participated in this study. Although the magnitude of effect and subject satisfaction were both high and the number of treatment-related severe AEs was very low, the number of subjects with a duration of effect ≥12 weeks was relatively low. This is in contrast to published observations that suggest that patients experience a duration of effect (mean or total) beyond 12 weeks, as shown in controlled trials of Dysport and Botox.6 ,9 Considering three primary endpoints, that is with the exclusion of the duration of effect criterion, approximately 60% of patients achieved response. In the clinical experience of the expert group of neurologists, the level of response achieved with three or four co-primary end points is highly encouraging. Therefore, our novel findings indicate that measurements for the magnitude of effect, subject satisfaction and safety profile according to routine practice demonstrate good clinical response to BoNT-A in subjects suffering from CD. However, duration of effect, such as defined in the study, may require further confirmation due to its subjective nature. Waning of effect is a gradual process and therefore assessment for duration of effect based on serial subject's CGI measurements (rather than depending on the patient reporting on waning of effect on a single specific date) may have been more appropriate. Regardless of these considerations, unrealistically high patient expectations and subjectivity may influence the perception of quick waning of effect. This highlights that, for some patients, this aspect is seen as a hurdle to response.
The subgroup analyses suggest that laterocollis as a predominant component, the absence of baseline tremor and absence of concomitant medication are factors that may be associated with higher response rates. Even if these data were not statistically significant, they provide a good starting point for further evaluation. In particular, it would be interesting to establish whether the use of concomitant medication at baseline reflects a greater disease severity (as assessed with TWSTRS scores) or more co-morbidities associated with CD (eg, anxiety, depression) that could interfere with the therapeutic effect of BoNT-A. With relevance to the former, data from this study suggest that the duration of CD (≤10 years vs >10 years) did not markedly influence the distribution of concomitant therapies (data not shown).
Efficacy findings confirm the value of BoNT-A as a treatment for CD symptoms. Notable improvements in mean TWSTRS scores were observed, as was improvement in tremor. It is recognised that HRQoL is compromised in CD, especially among women.20 In this analysis of a largely female population, the decrease in subscores of the CDIP-58 (a more sensitive measure of clinical change than other frequently used HRQoL instruments13) is consistent with previous reports in confirming the positive impact of BoNT-A on HRQoL when administered as a therapy for CD.21 ,22
BoNT-A was generally well tolerated in this study, with few reported severe AEs. In general, treatment-emergent side effects were consistent with the known safety profile of this treatment.6 As observed in previous reports, the most common side effect of BoNT-A treatment was dysphagia.6 ,20 Overall, this study highlights that no new safety concerns were raised with BoNT-A when used in routine clinical practice. For any given treatment, an acceptable level of tolerance is required to ensure continued treatment and subject compliance, hence, the inclusion of tolerance as a response criterion. In total, 97.5% of subjects met the response criterion of no severe treatment-related AEs. It may be speculated that the presence of treatment-emergent side effects such as dysphagia could exert a negative impact on objective and subjective assessments of symptom improvement and ultimately response, but observed response rates of 73.6% (magnitude of effect) and 69.8% (subject's CGI) in this study would suggest otherwise.
Inherent to studies of this design (non-interventional), the lack of randomisation, as well as the absence of a control group, means that confirmatory conclusions cannot be drawn. Moreover, the a priori defined duration of effect criteria was based on subject assessment of the waning of treatment effect. Thus, the subjective nature of this assessment has potential for bias resulting from patients' unrealistically high expectations from treatment, a hypothesis supported by the observation of maintained improvements in TWSTRS scores even at visit 3.
Conclusions
This study reveals the CD subject demographics and BoNT-A response in a real-life clinical setting. Using a novel multimodal definition of response, this large-scale study showed that the magnitude of effect, subject satisfaction and safety profile were well met, and it was also felt that these were appropriate measures to assess BoNT-A response in CD subjects. This study also indicates possible predictive factors for BoNT-A in subjects with CD, but further research is required to confirm these in the prognosis of CD.
Acknowledgments
The authors would like to acknowledge the editorial assistance of Ogilvy Healthworld. Funding was provided by Ipsen. The authors would also like to thank members of the INTEREST IN CD study group, who were: Australia: Dr A Hughes, Dr K Kotschet, Dr D Williams, Dr V Fung; Belgium: Dr M van Zandijcke, Dr P Santens, Dr W van Landegem, Dr V Delvaux; Czech Rep: Dr E Ehler, Dr R Jech, Dr P Otruba, Dr M Bareš; France: Dr M Simonetta-Moreau, Dr S Soulayrol, Dr P M Burbaud, Dr A Kreisler, Dr C Vial, Dr M Borg, Dr S Sangla, Dr N Patte-Karsenti; Germany: Dr E Fleischer, Dr M Müngersdorf, Dr I Weimar, Dr R Pfister, Dr B Mohammadi, Dr I Nastos; The Netherlands: Dr Laboyrie, Dr Douma; Portugal: Dr M J Rosas, Dr J Ferreira, Dr M Castelo Branco; Russia: Dr S Timerbaeva, Dr D Khasanova, Dr L Korenko, Dr G Belskaya; UK: Dr P Moore, Dr M Kellet, Dr P Misra, Dr T Harrower.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
Footnotes
Previous publications: (1) Poster presentation, ‘An International, Observational Study To Define Factors Influencing Response to Botulinum Toxin Type A (BoNT-A) in Subjects with Idiopathic Cervical Dystonia: Methodology and Baseline Clinical Data’ at the 63rd Annual Meeting of the American Academy of Neurology, Honolulu, Hawaii, 9–16 April 2011. Abstract number P04.224. (2) Poster presentation, ‘An international observational study to define in real-life practice response to Botulinum toxin type A (BoNT-A) injection in subjects with idiopathic cervical dystonia’ at The MDS 15th International Congress of Parkinson's Disease and Movement Disorders, Toronto, ON, Canada, 5–9 June 2011. Abstract number 662. (3) Poster presentation, ‘An international, observational study to identify in real-life practice prognostic factors for response to Botulinum toxin type A injection in subjects with cervical dystonia’ at the 15th Congress of the European Federation of Neurological Societies, Budapest, Hungary, 10–13 September 2011. Abstract number P1497. (4) Poster presentation, ‘An international, observational study to define in real life practice response to Botulinum toxin type A (BoNT-A) injection in subjects with idiopathic cervical dystonia’ at the 7th International Conference on Basic and Therapeutic Aspects of Botulinum and Tetanus Toxins—Toxins 2011, Santa Fe, USA, 2–5 October 2011.
To cite: Misra VP, Ehler E, Zakine B, et al. Factors influencing response to Botulinum toxin type A in patients with idiopathic cervical dystonia: results from an international observational study. BMJ Open 2012;2:e000881. doi:10.1136/bmjopen-2012-000881
Contributors VPM was involved in the concept and design, provision of study materials or patients, collection and assembly of data, data analysis and interpretation, manuscript review and critique, and final approval of manuscript. EE was involved in the provision of study materials or patients, collection and assembly of data, manuscript review and critique, and final approval of the manuscript. BZ was involved in the concept and design, data analysis and interpretation, manuscript writing, manuscript review and critique, and final approval of the manuscript. PM was involved in the concept and design, data analysis and interpretation, manuscript writing, manuscript review and critique, and final approval of the manuscript. MS-M was involved in the concept and design, provision of study materials or patients, manuscript review and critique, and final approval of the manuscript.
Funding This study was supported by Ipsen Pharma; BZ and PM were involved in the design of the study and the subsequent preparation of this manuscript (writing and review).
Competing interests VPM: Consultancies: Ad hoc consultant to Ipsen Pharma and Syntaxin Ltd. Advisory Boards: Attended Ipsen Pharma Medical Advisory Boards. Contracts: Contracts with Ipsen Pharma and Syntaxin Ltd related to ad hoc Consultancies/Advisory boards. EE: Grants: IGA Ministry of Health, Czech Republic. BZ and PM: Employment: Ipsen. MS-M: Consultancies: Ipsen. Employment: Hôpitaux de Toulouse and Paul Sabatier University.
Ethics approval The ethics approval was provided by Independent Ethics Committee/Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Correction