Article Text

Abstract
Objectives To evaluate effectiveness of a structured one-to-one behaviour change programme on weight loss in obese and overweight individuals.
Design Randomised controlled trial.
Setting 23 general practices in Camden, London.
Participants 381 adults with body mass index ≥25 kg/m2 randomly assigned to intervention (n=191) or control (n=190) group.
Interventions A structured one-to-one programme, delivered over 14 visits during 12 months by trained advisors in three primary care centres compared with usual care in general practice.
Outcome measures Changes in weight, per cent body fat, waist circumference, blood pressure and heart rate between baseline and 12 months.
Results 217/381 (57.0%) participants were assessed at 12 months: missing values were imputed. The difference in mean weight change between the intervention and control groups was not statistically significant (0.70 kg (0.67 to 2.17, p=0.35)), although a higher proportion of the intervention group (32.7%) than the control group (20.4%) lost 5% or more of their baseline weight (OR: 1.80 (1.02 to 3.18, p=0.04)). The intervention group achieved a lower mean heart rate (mean difference 3.68 beats per minute (0.31 to 7.04, p=0.03)) than the control group. Participants in the intervention group reported higher satisfaction and more positive experiences of their care compared with the control group.
Conclusions Although there is no significant difference in mean weight loss between the intervention and control groups, trained non-specialist advisors can deliver a structured programme and achieve clinically beneficial weight loss in some patients in primary care. The intervention group also reported a higher level of satisfaction with the support received. Primary care interventions are unlikely to be sufficient to tackle the obesity epidemic and effective population-wide measures are also necessary.
Clinical trial registration number Trial registrationClincaltrials.gov NCT00891943.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Evaluated structured one-to-one weight management programme.
Delivery by trained non-specialists.
Primary care setting.
Key messages
Clinically important level of weight loss achieved by higher proportion of participants in the intervention (33%) compared with the control group (20%).
Intervention group reported higher level of satisfaction with support received.
Primary care interventions are unlikely to be sufficient to tackle the obesity epidemic.
Strengths and limitations of this study
Relatively low threshold of body mass index ≥25 for inclusion, with few exclusions, so wide applicability of findings.
High loss to follow-up (43%), although similar to other studies in the area; used multiple imputation to counter any biases.
Introduction
Overweight and obesity are major public health problems,1 representing the fifth leading cause of death in the world2 and an increasing global challenge.3 Obesity has severe impacts on health, increasing the risk of type 2 diabetes, hypertension, some cancers, heart and liver disease.1 4 5 The Foresight Report6 estimated the National Health Service costs attributable to obesity in 2007 as £4.2 billion. In 2010, 68% of men and 58% of women in England were overweight or obese (body mass index (BMI) ≥25 kg/m2).7
Obesity is a chronic condition requiring lifelong management as weight loss is often regained.8 9 Achieving changes in behaviour is challenging,10 largely due to an inability to maintain healthy eating and physical activity behaviours.11 Modest weight loss (3%–9%) can prevent type 2 diabetes, improve fasting plasma glucose, blood pressure and lipids, and reduce antihypertensive medication.12–16 Most overweight patients would like help with weight management from their general practices,17 weight loss is feasible in the short term (3–12 months)18 19 and estimated to be cost saving to the NHS,20 although few recall receiving weight control advice from a health professional.21
The aim of this study was to develop and evaluate the efficacy of an intervention programme with 12-month follow-up, for an ethnically diverse overweight/obese population recruited from general practices in a pragmatic randomised controlled trial (RCT) following the Medical Research Council framework for complex interventions.22 To our knowledge, there are currently no other published RCTs of one-to-one lifestyle interventions delivered in UK general practice to overweight/obese patients without comorbidities.
Methods
Aims
The aims of the study were to assess, by means of a pragmatic parallel group RCT, the effects on anthropometric measures, health-related parameters and the sense of well-being of offering individualised weight management advice in primary care to overweight/obese people who wished to lose weight and to identify the key factors influencing the outcome of the intervention.
The primary outcome was the difference between the control and intervention groups in changes in body weight, and the secondary outcomes were differences in waist circumference, per cent body fat, blood pressure and heart rate from baseline to 12 months.
Interventions
The intervention combined evidence-based components recognised as essential for behaviour change and successful weight loss23—healthier eating, increased physical activity incorporated into patients' everyday lifestyles, tailored goal setting, keeping food and activity diaries, self-monitoring, positive reinforcement, coping with lapses and high-risk situations and long-term support—derived from theoretical frameworks underpinning health promotion that have an emphasis on long-term changes in habits. This includes, for example, social cognitive theory,24 which addresses diet and activity-related social support, outcome expectations, self-efficacy and self-regulation as well as diet and physical activity monitoring to assess changes over time and goal setting.25 It also emphasised SMART (Specific, Measurable, Attainable, Relevant, Timely) goal setting, the relationship between goals and satisfaction and the achievement of goals and rewards, and systems thinking,26 which focuses on environmental changes and stresses long-term changes in routines. The programme also incorporated NICE guidance on management of overweight and obesity27 as well as evidence-based principles of behaviour modification,23 adherence to treatment28 and results from our pilot study (figure 1).18 Six CAMWEL advisors were recruited from various occupational backgrounds including healthcare, in line with the NHS health trainers initiative.35 The advisors received initial training over 2 days and further meetings with the research team every 3–4 months. Training of advisors included briefing on the obesity epidemic; food and physical activity behaviours associated with excess weight; principles of best practice and behaviour change strategies; evidence for what has been shown to work in weight loss management programmes; the use of motivational interviewing methods, counselling techniques and cognitive–behavioural therapy methods to provide tailored support for behaviour change; together with details of the study design and role play. All advisors were given a copy of the National Obesity Forum CD-Rom ‘Managing Obesity in Primary Care’. Participants were invited to attend 30 min sessions with the advisor every fortnight for the first 12 weeks, every 3 weeks for 12 weeks and finally monthly for the next 12 weeks, making a total of 14 sessions. A script and schedule of topics for discussion were provided to the advisors for each session. The topics included personally agreed weight loss goals, eating and physical activity goals, exploration of motivations for losing weight, personal cues to reduce unhealthy eating and sedentary behaviour, support from family and friends, triggers associated with habits and routines, long-term benefits of small changes and the importance of scheduling and time management. A commercially available weight management software package (http://www.perfect-diet-tracker.com) was used to record and monitor participant progress and keep notes of each session by the advisors. The advisors were provided with access to a book giving the calorie content of foods available in the UK,33 a kit including 100-calorie portions of various food items and Adams Food and Alcohol Portion Pots (http://www.adamsportionpot.com). The intervention participants were given pedometers and handouts associated with each session, including a tailored motivational booklet to encourage increased levels of physical activity and a book of walks in the local area specially prepared for the study (appendix 1). Further details are available from the corresponding author (KN).

CAMWEL intervention framework.
There is no current comparator ‘gold standard’ treatment programme available for weight management in general practice. In this pragmatic trial of a complex intervention, we assess the benefit of the intervention compared with routine clinical practice. We provided a copy of the Quick reference NICE clinical guideline on Obesity to all participating general practitioners (GPs)27 and asked control participants to contact their general practice to receive usual weight management care provided by the practice, which could include referral to a dietitian (http://www.camden.nhs.uk/adult-weight-management-service.htm), exercise on referral, the ‘Shape-Up’ programme (http://camden.gov.uk/ccm/navigation/leisure/sport-and-physical-activity/get-active-and-healthy/lose-weight/), prescription of weight loss medication, weight loss surgery or no further treatment.
All participants were given the British Heart Foundation booklet: “So you want to lose weight … for good.”36
Recruitment
All general practices in Camden were visited and invited to participate in the trial. Participants were recruited between July 2009 and January 2010 from 23 of 39 NHS Camden general practices. The London Borough of Camden has areas of relative affluence alongside areas of relative deprivation, with approximately 35% of the population living in areas classified as some of the most deprived in England.37 Education levels are also disparate, with 47% of people in employment being educated to degree level or above, while 17% of working age people have no qualifications.38 Camden has an ethnically diverse population, with 27% belonging to minority ethnic groups.38
Several recruitment approaches were used. Primarily, participating practices wrote to a sample of patients with BMI ≥25 kg/m2; GPs and practice nurses were provided with referral ‘prescription’ pads with a tear-off slip to be given to the patient with contact details of the trial office; and posters and flyers were placed in practice waiting areas and local pharmacies. During the final 6 weeks of the recruitment period, three practices supplemented recruitment by sending text messages to potentially eligible patients using their electronic record (EMIS) and messaging (iPLATO) systems. All practices were reimbursed for time spent on recruitment.
Baseline measurements
Potential participants were screened by telephone for eligibility (MH, EH, TP). Inclusion criteria were: age 18 years and above, BMI ≥25 kg/m2, attending a participating practice and willing to attend visits with a CAMWEL advisor over 12 months. Exclusion criteria were pregnancy or lactation, diagnosis of renal failure, use of a pacemaker, recent diagnosis of cancer or participation in another weight management study. Following GP consent, participants were scheduled for screening appointments with a researcher (MH) at one of three practices. The study was explained and the participant invited to give informed written consent and to complete the baseline questionnaire. Height (without shoes) was measured to the nearest 0.1 cm using a stadiometer. Weight (in light clothing) was measured using the Tanita (BC 420 MA) scales. The scales also reported per cent body fat, basal metabolic rate and metabolic age (age expected for a given value of basal metabolic rate). Waist was measured midway between the iliac crest and the costal margin to the nearest 0.1 cm. Blood pressure and heart rate were measured using a digital automatic monitor (Omron Model M10-IT), with the average of three readings recorded where possible. The printout from the Tanita scales, including weight, BMI and metabolic age, was given to all participants.
Outcomes
All participants were invited for follow-up at 6 and 12 months. A letter was sent 3 weeks prior to the due date, followed by a telephone call to arrange the appointment. Three attempts were made to contact each participant. Measurements taken at baseline were repeated and participants were asked to complete a questionnaire. A £30 voucher was provided for their time to all participants who completed each follow-up appointment.
The self-completed questionnaires included the following validated measures: EuroQol Visual Analogue Scale, Obesity and Weight Loss Quality-of-Life,39 Hospital Anxiety and Depression Scale,40 Rosenberg measure of self-esteem,41 Duke-UNC Functional Social Support Questionnaire,42 Three-Factor Eating Questionnaire-1843 and physical activity (RPAQ),44 as well as socio-demographic information. Deprivation was ascertained using the Index of Multiple Deprivation based on the participant's home address postcode.45
In addition, at follow-up, we used the Patient Assessment of Care for Chronic Conditions46 47 to assess the participants' views on the care they received from the advisors and the GP practice on helping them lose weight. A brief series of statements was used to assess participants' confidence in their ability to manage their weight on a scale of 1 (disagree strongly) to 4 (agree strongly). Further questions asked about the type of help received from the GP practice regarding weight loss, changes made in behaviours related to weight management and experience of study participation. Participants in the intervention group also completed an additional section to ascertain how helpful they found the sessions and materials provided as part of the CAMWEL programme.
Randomisation
Participants were randomly allocated (allocation ratio 1:1) to the control or intervention group (TP, EH, AS), using a computer-generated randomisation application written in VBA for MS Access (TP). The Taves method of minimisation48 was used to ensure the groups were balanced for general practice, gender, age group (≤50/>50 years), BMI category (≤30/>30 kg/m2), diagnosis of diabetes (yes/no) and taking antipsychotic medication or not.
Blinding
The study was single blinded with members of the study team assessing baseline and follow-up measurements blinded to group assignment.
Sample size
In our pilot study, participants had a mean weight of 98.1 kg (SD 17.3 kg) at baseline.18 Since a loss of 5%–10% of body weight in obese adults is associated with significant reductions in the risk of obesity comorbidities, we considered a difference in weight between groups of 7% at 12-month follow-up to be clinically important. For the sample size calculation, we wished to detect a mean weight difference of 6.9 kg at 12 months between the two groups with two-sided statistical significance of 1%, power at 90% and the correlation coefficient between baseline and follow-up values conservatively set at 0.7. We thus calculated a total sample size of 228 (114 per group). Assuming a loss to follow-up at 12 months of 40%,49 it was estimated that 380 participants would be required.
Statistical methods
Comparisons between groups for continuous variables were performed using two-sample t tests and regression methods, adjusting for the baseline value of the variable. χ2 tests and logistic regression were used for categorical variables. Changes were calculated as value at follow-up minus baseline value. Primary analyses were conducted on an intention-to-treat basis, using multiple imputation (MI) to account for missing data at follow-up. Exclusion of subjects with missing data is inefficient and can lead to biased results if those dropped are atypical in some respect50 and MI can both increase efficiency and reduce bias in such settings.51 52 Missingness in this study is dominated by attrition, but there are also some intermediate missing outcome values and missing baseline values (although not for weight) so the ‘Fully Conditional Specification’ form of MI has been used.53 For each outcome, the full set of imputation variables comprised the outcomes at each of the three occasions, together with a set of baseline variables selected for their non-negligible association with missingness or weight loss. For all outcomes, the following baseline variables were included: age, weight, per cent body fat, BMI, fat mass, metabolic age, deprivation status and employment status as well as totals from the Obesity and Weight Loss Quality-of-Life, EuroQol Visual Analogue Scale, Hospital Anxiety and Depression Scale anxiety, Three-Factor Eating Questionnaire emotional eating and RPAQ scales. The imputation procedure was carried out separately for the two groups (intervention and control), and the resulting multiply imputed data sets were combined for the final MI analysis. A total of 200 imputations were used to stabilise the results and to ensure negligible loss of power.50 Analyses using only data on participants who completed 12-month follow-up were also conducted.
Exploratory analyses (not using MI) were conducted excluding subjects who had bariatric surgery or were prescribed weight loss medication during the course of the trial. We also examined whether the degree of weight loss was associated with baseline characteristics or with changes in health or quality-of-life measures. Analyses were performed using STATA V.11.
Ethical approval
The study was approved by the London School of Hygiene & Tropical Medicine Ethics Committee, the Camden and Islington Community Research Ethics Committee (reference number 09/H0722/22) and the North Central London Research Consortium.
Results
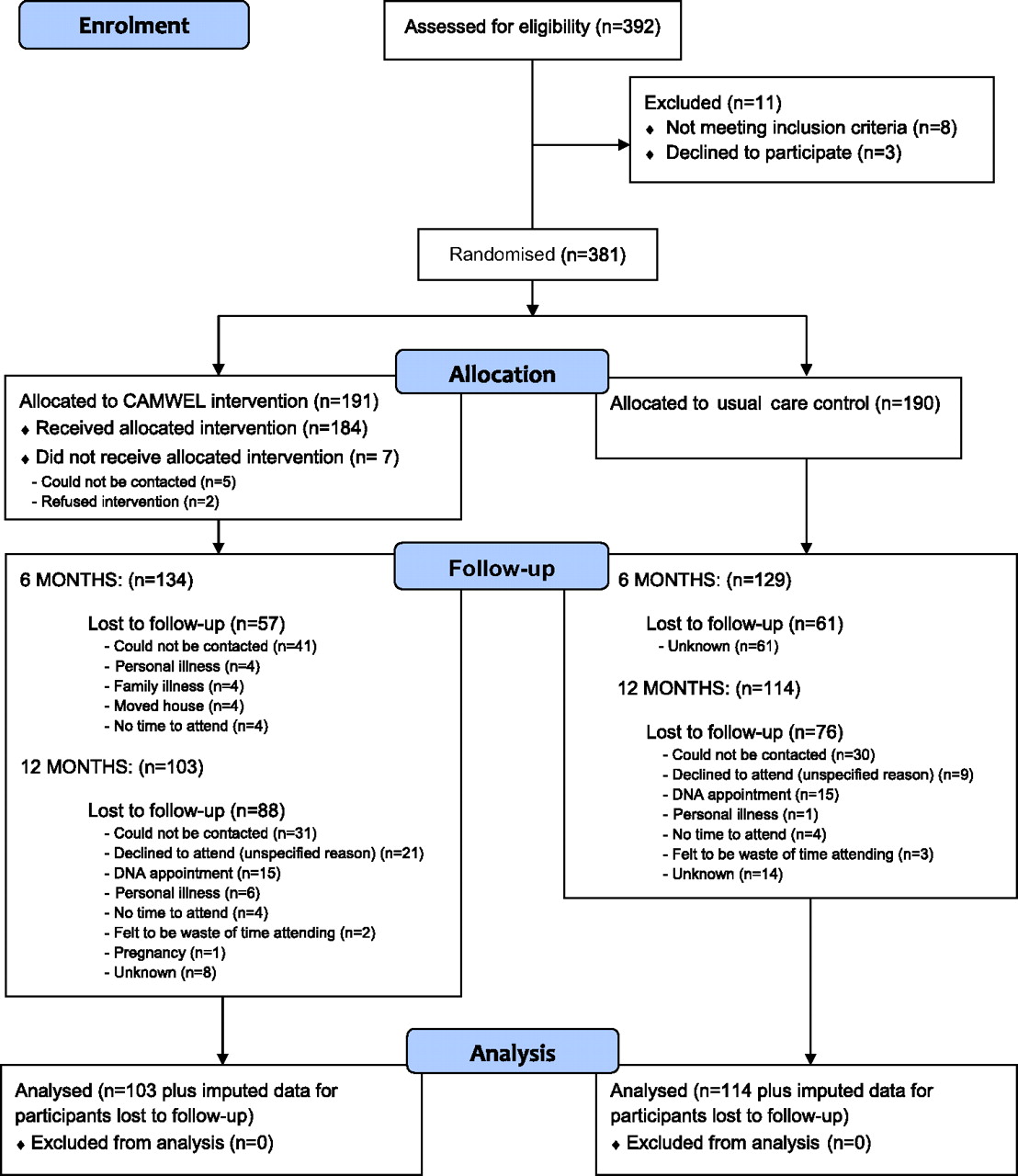
Participants were followed up at 6 months between January 2010 and July 2010 and at 12 months between July 2010 and January 2011. Participant flow through the trial is shown in figure 2.
{kind=link}
{kind=link}
Flow of participants through the trial.
Baseline characteristics
We recruited 381 participants with a median age of 48.5 (IQR 37.5–60.4), weighing 60.1–152.2 kg, with waist circumference of 76–147 cm. The majority (72%) were women, 12% (47/381) had diagnosed diabetes, 1.3% (5/381) were on antipsychotic medication, 60% were in employment, 47% were university graduates and 73% described their ethnicity as Caucasian (table 1). Participants wanted to lose an average of 18 kg (SD =12.4), representing 16.7% of their baseline weight. There were no significant differences between groups for any of these variables.
Baseline characteristics of participants wishing to lose weight allocated to usual care (control) or to the CAMWEL programme (intervention)
Response rates
Measurements were obtained for 69% (n=263) of the sample at 6 months and 57% (n=217) at 12 months. There were no significant differences in follow-up rate at 12 months by randomisation group (60.0% control, 53.9% intervention, p=0.23), but those followed up tended to be older, have lower BMI, fat mass and per cent body fat, and were less likely to be from a deprived area than those not followed up (table 2).
Comparison of baseline characteristics of participants followed up at 12 months and those lost to follow-up (mean (SE) unless otherwise stated)
Primary outcome
Based on the intention-to-treat analysis using imputed missing values (table 3), at 12-month follow-up, structured support resulted in a mean difference in weight loss between the two groups of −0.70 (−2.71 to 0.76) kg. A higher proportion of participants lost 5% or more of their baseline weight in the intervention (32.7%, 95% CI 24.9% to 40.5%) when compared with the usual care (20.4%, 95% CI 13.3% to 27.5%) group (OR 1.80 (1.02 to 3.18, p=0.04).
Changes in outcomes at 6 and 12 months and treatment differences between participants wishing to lose weight allocated to a structured one-to-one weight loss programme (intervention) or to usual care (control)
Secondary outcomes
The intervention programme was also associated with weak evidence of beneficial trends in waist circumference, per cent body fat and per cent weight change. Heart rate was reduced by 3.7 (0.3 to 7.0, p=0.03) beats per minute in the intervention group compared with the control group.
Based on data for participants who completed the 12-month follow-up (table 3), a higher proportion (one in three compared to one in five) in the intervention group had lost at least 5% of their initial weight (difference 14.7% (3.0 to 26.4, p=0.01)) and experienced a greater average reduction in waist circumference (difference 1.88 cm (0.01 to 3.76, p=0.05)) compared with those in the control group. Weak evidence of reductions in weight, per cent body fat, BMI, blood pressure and heart rate were observed in the intervention group compared with the control group. The absolute risk reduction for losing 5% baseline weight was 14.7% (3.0 to 26.4), and the number needed to treat was 6.8 (3.8 to 33.2). A higher proportion of those in the intervention group (84%, 21/25) who had lost ≥5% at 6 months had managed to keep this level of weight loss at 12 months compared with those in the control group (61.5%, 8/13). We were unable to identify characteristics of the subgroup of participants more likely to lose 5% of their baseline weight.
No evidence of differences was found between the two groups on any of the psychological or quality-of-life measures.
Trial participation
Participants in the intervention group were more satisfied than those in the control group with the level of weight loss achieved and they found participation in the trial and feedback of physical measurements helpful (table 4). The intervention group also reported receiving more patient-centred care than those in the control group as measured by the Patient Assessment of Care for Chronic Conditions scales (table 5). Detailed analysis of the interviews and focus groups with a subset of the participants will be reported elsewhere.
Participant satisfaction with care received by allocation group at 12 months
Participant assessment of care received by allocation group at 12 months
The intervention programme
The majority of participants (38/56, 67.9%) reported that a regular meeting with the advisor was the most helpful aspect of the programme and the least helpful was the use of handouts in improving eating habits (17/56, 30.3%). The majority (84%) said they would choose to continue to meet an advisor beyond the 12 months of the current study, with most (73%) preferring to see the advisor at least every 4 weeks.
Behaviours associated with losing 5% or more of baseline weight
Participants who lost 5% or more of their baseline weight were more likely to state that they had reduced their fat and sugar intake in the previous 6 months than those who did not; there was no evidence of increasing levels of physical activity between the groups (table 6). They also reported that attending regular meetings with a non-judgemental advisor, discussion on portion sizes and use of the pedometer were particularly useful and that they would continue to monitor food intake to maintain their weight.
Reported changes* in eating and activity habits by participants who lost 5% or more of baseline weight compared with those who did not
Exploratory analysis
Thirty-eight participants were known to have been prescribed drugs for weight loss or to have undergone weight loss surgery during the trial period. Of these, 27 were followed up at 12 months (12 control: mean weight change −2.44 kg (−7.15 to 2.27); 15 intervention: mean weight change −3.51 kg (−6.95 to −0.08)). The difference between groups was 1.07 kg (−4.32 to 6.46, p=0.69). In analysis excluding these participants, those in the intervention group showed significantly greater reductions in weight (1.72 kg (0.29 to 3.14, p=0.02)), waist circumference (2.52 cm (0.32 to 4.72, p=0.03)), BMI (0.63 kg/m2 (0.11 to 1.14, p=0.02)) and per cent baseline weight loss (1.94% (0.32 to 3.56, p=0.02)) when compared with the control group at 12 months. In addition, a higher proportion of participants in the advisor group lost ≥5% of their baseline weight when compared with the control group (OR 2.68 (1.13 to 5.70, p=0.03)).
The number of sessions attended was available for 87 participants of whom 40 (46%) attended more than 70% (10/14) of the available sessions. Half (50%) of the participants attending more than 70% of the programme lost 5% or more of their baseline weight compared with a quarter (23%) who attended fewer sessions (difference 26.5%, 95% CI 6.9 to 46.3, p=0.01).
Discussion
Principal findings
The structured one-to-one weight loss programme delivered by non-specialists in general practice did not achieve the pre-specified difference in average weight loss of 7%. However, it did result in a higher proportion of the participants losing 5% or more of their baseline weight compared with those randomised to usual care, which is considered a clinically important outcome in similar trials. This suggests that people likely to benefit from such a programme are a subset of the total study population but we were unable to identify particular characteristics that would permit identification of a receptive group in advance. There was some evidence that the intervention group experienced greater reductions in mean weight, waist circumference and % body weight than the control group. While the overall effects on weight loss are modest, they are not unimportant.
Strengths and weaknesses of the study
The key strengths of the CAMWEL programme are its wide applicability to overweight and obese people from diverse backgrounds as there were few exclusions, feasibility of its delivery in primary care by non-specialist trained advisors and a patient-centred approach to making sustainable changes to diet and physical activity easily incorporated into peoples' daily lives.
Limitations include the slow initial recruitment, although this improved over time, particularly with mobile phone text message use.54 Loss to follow-up was high (43%), although similar to that of other weight loss studies in the UK.55–58 The response rate in the DESMOND diabetes management trial19 was substantially higher (91%), perhaps because participants were recently diagnosed diabetics and therefore highly motivated. High attrition in RCTs of weight loss is well recognised,59 with a recent review reporting losses to follow-up of 30%–60%.49
We used MI for missing values to counter any biases due to loss to follow-up as high level of attrition involves considerable uncertainty about outcomes for participants lost to follow-up. We included patients with BMI ≥25 as NICE recommends treatment at this level, although this relatively low threshold and broad inclusion criteria may have diluted the results in terms of average weight loss thus needing a larger sample to detect significant differences.
Participants in the control group were advised to contact their general practice to receive the usual care provided for weight loss. We provided all GPs with NICE guidelines on obesity and participants with the British Heart Foundation booklet on weight loss as well as feedback on the measurements taken at 6 months. This provision of support could be one reason why participants in the control group also lost weight over the period of the trial resulting in greater similarity of changes in the two groups, which would represent bias if the GPs altered their usual care by virtue of trial participation. Outcomes of RCTs may be influenced by participants' treatment preference60 and research assessment procedures61 triggering behaviour change and contributing to the weight loss seen in the control group.
Behaviour change interventions tend to be complex with multiple components and it is difficult to assess the effectiveness of different components. This was a pragmatic trial reflecting the likely performance of the programme as delivered in practice. While the fidelity of the delivery of the intervention could be examined in more detail, we have shown that patient assessment of the structured support by trained advisors is significantly better than usual care.
Cost-effectiveness analyses are required to inform decision making about the value of attaining these outcomes and will be reported in a separate paper.
Putting the study in context
Seven studies of weight change conducted in UK general practice have been published (see table 7). With the exception of a trial in newly diagnosed diabetics, RCTs provided no strong evidence of differences in weight loss between the intervention and control groups, except for those using a commercial provider (Weight Watchers). Our trial achieved results at least comparable with the more targeted interventions based in general practice.
Studies on weight loss conducted in general practice in the UK with 12-month follow-up
Implications
We have demonstrated that one-to-one structured support by a trained advisor in general practice can help people wishing to lose weight change their behaviour sufficiently leading to a clinically important loss in weight. While 1 year may be too short a time to see all the benefits of a weight management intervention, the majority of participants found the Camwel programme helpful suggesting that they will continue to accrue benefit as they implement the behaviour change techniques learned during the study. Understanding how the intervention worked and why it worked just for some participants as well as its cost-effectiveness are important and we will explore these in our subsequent research. The importance of our results lies in their generalisability. Our results, together with those from other researchers, suggest that individual approaches in general practice can achieve modest benefits for the National Health Service. However, primary care interventions are unlikely to be sufficient to address the obesity epidemic and effective population-wide policy measures are needed as well, including increasing energy expenditure through active travel64 and reducing dietary intake.
Acknowledgments
We thank the study participants; the GPs and practice managers at the participating practices (Abbey Medical Centre, Ampthill Square Medical Centre, Belsize Priory Medical Practice, The Bloomsbury Surgery, Brondesbury Medical Centre, Brunswick Medical Centre, Camden Road Surgery, Chomley Gardens Surgery, Fortune Green Road Surgery, Gower Place Practice, Gower Street Practice, Grays Inn Medical Centre, Hampstead Group Practice, James Wigg Group Practice, Kings Cross Road Practice, Museum Practice, Park End Surgery, Parliament Hill Surgery, Prince of Wales Group Practice, Swiss Cottage Surgery, Regents Park Practice); members of the advisory board (Chris Bonell, Phil Edwards, Susan Jebb, David Simpson and Paul Wilkinson); the advisors (Rosalind Bose, Gloria Ferenando, Gillian Lampert, Tim Whelan, Gina Williams, Diana Villamil); as well as Nick Cavill for helping to write the motivational physical activity handbook, Jim McCambridge for help with training advisors and commenting on the manuscript, Kate Lees for help with dietary aspects, Katie Williams (NHS Camden), Suzanne Taylor for data entry, David Taylor for assistance with database management, Ray Bird for audio-visual assistance, Laura Doubleday and Sarah Milton for helping with follow-up of participants, and Adams Portion Pots (Adams Insight Consulting, http://www.adamsportionpot.com) and NHS Camden for their support of this study.
Appendix 1 The structure of the CAMWEL intervention programme
| Session number | Week | Topic materials | Handouts | |
| 1 | 0 | Getting started: establish working relationship and good rapport with participant; elicit personal reasons for losing weight, build commitment to program and introduce lifestyle changes approach. BHF ‘So you want to lose weight’ booklet | Sequence of topics | Behaviour change diary |
| Appointment card | Food diary | |||
| Benefits of healthy habits | Activity diary | |||
| Recording your routines | ||||
| Deciding to change | ||||
| 2 | 2 | Changing habits: review progress, explain importance of changing habits permanently and introduce the five steps to solving problems. | Problem solving | (Behaviour change diary) |
| Build a better recipe | (Food diary) | |||
| Just one more step | (Activity diary) | |||
| 3 | 4 | Healthy eating: review progress, explain importance of regular meals, portion sizes, keeping a record and discuss making easy food swaps. (Adam portion pots; 100 kcal portion size food box) | FSA Eat Well booklet | (Activity diary) |
| Rate your plate | ||||
| Easy food swaps | ||||
| Healthy drinks | ||||
| Food labels card | ||||
| 4 | 6 | Let's get active: review progress, explain importance of activity guidelines and discuss ways of incorporating physical activity into participant's lifestyle. | Being active | Steps chart |
| Your guide to walking in Camden | ||||
| Cut the fat and sugar | Printed weight graph | |||
| Camden outdoor gyms | (Rate your plate) | |||
| 5 | 8 | Taking charge of your environment: review progress, explain importance of cues and discuss ways of changing the environment to make losing weight the ‘easy’ option. | Your environment | (Rate your plate) |
| Goals and rewards | (Steps chart) | |||
| Eat well on the cheap | Printed weight graph | |||
| 6 | 10 | Eating when out and about: review progress, explain keys to making healthy choices when out and about and discuss alcohol if appropriate. | Healthy choices | (Rate your plate) |
| Alcohol and your diet | (Steps chart) | |||
| Eating when out and about | ||||
| 7 | 12 | Tip the calorie balance: review progress at 3-month stage of programme; explain energy balance equation, importance of healthy eating, being active, social support and action planning. | Tipping the calorie balance | (Steps chart) |
| Individual printed weight graph | (Rate your plate) | |||
| 8 | 15 | Positive thinking: review progress and introduce ways to stop negative thoughts and ‘talk back’ with positive ones. | Positive thinking | (Food diary) |
| Camden Walk4Life maps | (Activity diary) | |||
| (Steps chart) | ||||
| (Rate your plate) | ||||
| (Behaviour change diary) | ||||
| 9 | 18 | Getting off the slippery slope: review progress, identify reasons for slips and ways of getting back on course. | Slippery slope | |
| Camden Walk4Life maps | ||||
| BHF ‘Healthy meals, Healthy Heart’ or ‘Food should be fun and healthy’ menus | ||||
| Individual printed weight graph | ||||
| 10 | 21 | Social eating: review progress, discuss social settings where it may be difficult to stay in control of eating healthily and ways to overcome this and enjoy healthy social eating. | Social eating | |
| Individual printed weight graph | ||||
| 11 | 27 | Staying on course: review progress, identify successful changes made and identify situations where participant not in control and discuss ways of overcoming barriers. | Staying on course | (Rate your plate) |
| Healthy snacking | (Food diary) | |||
| 100 Calorie portions | (Steps chart) | |||
| Meal plans—Indian/minimum cooking | ||||
| Individual printed weight graph | (Activity diary) | |||
| 12 | 31 | Staying active: review progress; discuss additional changes made and how further activity can be added into lifestyle. | Staying active | (Activity diary) |
| Individual printed weight graph | (Steps chart) | |||
| 13 | 35 | Managing stress: review progress; discuss how stress affects weight and ways to manage stress. | Day-to-day stress | (Activity diary) |
| Individual printed weight graph | (Steps chart) | |||
| (Rate your plate) | ||||
| (Food diary) | ||||
| 14 | 47 | Reshaping habits: review progress since start of programme; discuss ways of continuing to lose/maintain changes in the long term. | Reshaping habits | (Rate your plate) |
| Cancer Research UK's Ten top tips | (Food diary) | |||
| Camden architecture & walking guide | (Steps chart) | |||
| Travel Camden: Camden walking map | (Activity diary) | |||
| Belsize walk; Jubilee Walk | ||||
| Individual printed weight graph | ||||
| Certificate of achievement | ||||
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
All authors, external and internal, had full access to all the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
To cite: Nanchahal K, Power T, Holdsworth E, et al. A pragmatic randomised controlled trial in primary care of the Camden weight loss (CAMWEL) programme. BMJ Open 2012;2:e000793. doi:10.1136/bmjopen-2011-000793
Contributors KN, JLT, NT, DH, AK, SE and AH contributed to conception and design. MH, JLT, KN, EH, AS and UG contributed to acquisition of data, KN, TP, EH, MK and AH contributed to analysis and interpretation of data, and KN drafted the article. KN, JLT and AH revised it critically for important intellectual content. All authors contributed to the final approval of the version to be published.
Funding This work was supported by Camden Primary Care Trust (NHS Camden). The funding source had no role in the design or conduct of the study; collection, management, analysis or interpretation of the data and preparation, review or approval of the manuscript.
Competing interests All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that KN, TP, EH, MH, AS, UG and JLT had salary support from NHS Camden for the submitted work. AK was Director of Public Health at Camden Primary Care Trust between 2004 and 2009. The views expressed here are personal, and no financial support was received for the other authors' involvement in the CAMWEL Trial. No authors have had a relationship with companies that might have an interest in the submitted work in the previous 3 years nor do their spouses, partners or children have financial relationships that may be relevant to the submitted work. DH is on the scientific advisory board for LighterLife and no other authors have non-financial interests that may be relevant to the submitted work.
Ethics approval Ethics approval was provided by the London School of Hygiene & Tropical Medicine Ethics Committee, the Camden and Islington Community Research Ethics Committee (reference number 09/H0722/22) and the North Central London Research Consortium.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.