Article Text

Abstract
Objective Serum α-fetoprotein (AFP) is the most commonly used biomarker for screening hepatocellular carcinoma (HCC) but fails to detect about half of the patients. Thus, we investigated if circulating microRNAs (miRNAs) could outperform AFP for HCC detection.
Design A retrospective cohort study.
Setting Two clinical centres in China.
Participants The exploration phase included 96 patients with HCC who received primary curative hepatectomy, and the validation phase included 29 hepatitis B carriers, 57 patients with HCC and 30 healthy controls.
Main outcome measures Expression of miRNAs was measured by real-time quantitative reverse transcription–PCR. Areas under receiver operating characteristic curves were used to determine the feasibility of using serum miRNA concentration as a diagnostic marker for defining HCC. A multivariate logistic regression analysis was used to evaluate performances of combined serum miRNAs.
Results In the exploration phase, miRNA profiling on resected tumour/adjacent non-tumour tissues identified miR-15b, miR-21, miR-130b and miR-183 highly expressed in tumours. These miRNAs were also detectable in culture supernatants of HCC cell lines and in serum samples of patients. Remarkably, these serum miRNAs were markedly reduced after surgery, indicating the tumour-derived source of these circulating miRNAs. In a cross-centre validation study, combined miR-15b and miR-130b demonstrated as a classifier for HCC detection, yielding a receiver operating characteristic curve area of 0.98 (98.2% sensitivity and 91.5% specificity). The detection sensitivity of the classifier in a subgroup of HCCs with low AFP (<20 ng/ml) was 96.7%. The classifier also identified early-stage HCC cases that could not be detected by AFP.
Conclusion The combined miR-15b and miR-130b classifier is a serum biomarker with clinical value for HCC screening.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article Summary
Article focus
More than half of the patients with HCC are not eligible for curative treatments because of the advanced tumour stages at the time of diagnosis.
Serum AFP has long been used as a biomarker for HCC screening, but its sensitivity and accuracy are only modest.
Circulating miRNAs are highly stable in blood and have a potential to become promising cancer biomarkers.
Key messages
This study identifies combined serum miR-15b and miR-130b as a classifier that provides high sensitivity and accuracy for detection of HCC.
The classifier outperformed AFP in discriminating HCC cases from non-cancerous controls. In addition, it identified early-stage HCC cases that could not be detected by AFP.
These findings collectively suggest that the miRNA classifier has clinical value and might be used for HCC screening programme, which could increase chances of patients with HCC for curative treatments.
Strengths and limitations of this study
The proposed classifier has been validated in an independent cohort of serum samples that includes patients with HCC, chronic hepatitis B carriers and healthy controls, suggesting the high positive predictive rate of the circulating miRNA classifier, and could be used as non-invasive biomarkers for HCC.
Other variables may affect the diagnostic accuracy of the classifier, for example, the presence of hepatitis C virus, which is also a risk factor for HCC. The application of the classifier in hepatitis C virus-related HCC is yet to be validated.
Introduction
Hepatocellular carcinoma (HCC) is the most common type of malignancy of liver cancer, with high incidences (>500 000 cases per year) in hepatitis B virus (HBV) endemic regions, including China, Southeast Asia and sub-Sahara Africa.1 2 HCC is also highly malignant and lethal, with an overall 5-year survival rate of 5%–9% from the time of clinical diagnosis. The dismal prognosis is largely caused by late detection of the tumours when standard surgery is not operable, high recurrence rate of the malignancy and resistance to chemotherapy.3 4 Approximately 80% of patients with HCC are untreatable because of advanced tumour stages at presentation; nevertheless, curative hepatectomy can improve the 5-year survival rate to 69% if the tumour is detected earlier, particularly when the tumour is single nodule and smaller than 2 cm.5 6
Diagnosis of HCC is usually based on imaging techniques (abdominal ultrasound, MRI and contrast-enhanced CT scan showing a suspicious liver lesion), elevated serum α-fetoprotein (AFP) or optional biopsy. Advances in MRI and CT scan have greatly improved imaging of focal hypervascular mass consistent with HCC, but these procedures are costly and not readily available in developing countries. Ultrasonography can detect large lesion but fails to detect small tumour, especially in obese patients and those with underlying liver cirrhosis; and the procedures are operator-dependent, varying the diagnostic accuracy. Serum AFP has long been used as a tumour marker for HCC screening—AFP <20 ng/ml is considered as normal and AFP >400 ng/ml as true positive in general. The European Society for Medical Oncology (EMSO) guidelines also recommended that elevation of AFP >400 ng/ml can be used instead of fine-needle cytology for diagnosis, especially in patients with liver cirrhosis.7 Despite that, the sensitivity of AFP is only modest (sensitivity: 39%–65% and specificity: 76%–94%), leaving approximate one-third of the patients with early-stage HCC with small tumours (<3 cm) undiagnosed.8 On the other hand, serum AFP level is elevated in benign liver diseases, such as hepatitis and cirrhosis.9 Thus, there is still pressing need for circulating biomarkers to detect early HCC in at-risk populations (patients with chronic hepatitis and/or liver cirrhosis).
MicroRNAs (miRNAs) are a class of non-coding small RNAs that regulate expression of genes at post-transcriptional level. They are involved in various biological processes, including development, differentiation, signal transduction and carcinogenesis.10 11 The use of miRNA as cancer biomarker is of particular interest because (1) different cancer types have distinct miRNA expression profiles12;(2) cancers could affect miRNA levels in the bloodstream,13 although the exact mechanisms through which the miRNAs are being released extracellularly remain unclear and (3) miRNAs could be detected in blood plasma or serum with high stability.13 14 They are well protected from RNases and remain stable after harsh conditions. To explore the clinical applicability of miRNAs as non-invasive circulating HCC biomarker, we investigated the expression profile of miRNAs in tumour tissues and selected candidate miRNA biomarkers. These biomarkers were evaluated in a set of serum samples from the same patient cohort. Last but not least, we further validated the miRNA biomarkers for detecting HCC in a separate cohort of serum samples from another clinical centre.
Patients and methods
Patients
Figure 1 shows the schematic flow chart for this miRNA biomarker discovery study. We first profiled 220 miRNAs using real-time quantitative PCR (qPCR) on frozen tumour and matched adjacent non-tumour tissues from 96 Chinese patients with HCC who received primary curative hepatectomy at Queen Mary Hospital (Pokfulam, Hong Kong) between 1990 and 2007.15–17 Among this cohort, we identified 15 patients with HCC having sufficient amount of matched serum samples collected before and after surgery to allow us measuring the selected miRNAs levels by qPCR. The preoperative serum samples were collected from 1 to 4 days before surgery, whereas the postoperative serum samples were collected from 8 to 359 days after surgery. The Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster approved this study, and each patient gave his/her written informed consent on the use of the clinical specimens for research.

Schematic flow chart of microRNA (miRNA) biomarker discovery for detecting hepatocellular carcinoma (HCC). This study was divided into three phases: exploration, selection/filtering and cross-centre validation. Two different cohorts of patients were included—one from Hong Kong (n=96) and one from Shanghai (n=116).
For the validation study, we obtained 116 serum samples from Chang Zheng Hospital and Eastern Hepatobiliary Surgery Hospital (Shanghai, China), which included 29 hepatitis B carriers, 57 patients with HCC and 30 healthy controls who underwent routine physical examinations with no underlying liver diseases. The hepatitis B carriers were individuals with positive serum hepatitis B surface antigen for at least 6 months at the time of blood collection, and they had previously shown normal (or minimally raised) levels of liver enzymes and negative for hepatitis B surface antigen. The clinical–pathological characteristics of the participants are summarised in table 1.
Demographic and clinicopathologic parameters of patients from different cohorts
Cell lines
Liver cell lines (MIHA, CL-48, HepG2, Hep3B, PLC/PRF/5 and MHCC-97H) were obtained as previously described.18 19 Cells were grown in Dulbecco's modified Eagle's medium (HyClone, Logan, Utah, USA) supplemented with 10% fetal bovine serum at 37°C in a 5% CO2 incubator. Upon confluence, media were collected and spun at 1200 g for 3 min to remove living cells before RNA extraction.
Samples processing and miRNA extraction
Total RNAs were extracted from frozen liver tissues using TRIzol (Invitrogen, Carlsbad, California, USA) as previously described.15 Blood samples were stored with EDTA, and serum specimens were stored at −80°C until use. Total RNAs from serum samples or cell culture media were extracted using TRIzol LS (Invitrogen). Each of the 500 μl of sera or media was added with 1 ml of TRIzol LS and then added with 200 μl chloroform. One volume of the aqueous layer was precipitated with 1.5 volumes of absolute ethanol, and the mixture was transferred to RNeasy Mini spin column (Qiagen, Hilden, Germany) for purification according to the manufacturer's instructions. Each sample was eluted with 30 μl RNase-free water. The concentrations of RNA extracted from the clinical samples ranged from 3.96 to 41.95 ng/μl.
miRNA quantification by real-time qPCR
miRNAs from tumour and adjacent non-tumour tissues were profiled using custom qPCR assays as described.15 The profiling data are available in Gene Expression Omnibus, under accession number GSE22058.
Expressions of the potential miRNA biomarkers were quantified in serum samples and HCC cell-conditioned media by TaqMan miRNA Assay (Applied Biosystems, Foster City, California, USA). For the total RNA extracted, 10 ng of RNA was subjected to the reverse transcription (RT) reactions using TaqMan miRNA Reverse Transcription Kit (Applied Biosystems), according to the manufacturer's recommendation. The RT products were then diluted by combining 10 μl RT product with 57.8 μl water. qPCR reactions were performed in duplicate, in scaled-down 10 μL reaction volumes containing 5 μl TaqMan 2X Universal PCR Master Mix with No AmpErase UNG (Applied Biosystems), 0.5 μl 20X miRNA-specific TaqMan probe and 5 μl diluted RT product (ie, 1:15 final dilution in the qPCR reaction). The qPCR reactions were run in ABI StepOnePlus real-time PCR system, and data were collected and analysed with StepOne software (Applied Biosystems).
For each of the TaqMan miRNA assays, we determined the limits of linear quantification and PCR efficiency. We prepared a standard calibration curve by a 10-fold dilution of single-stranded DNA oligonucleotides corresponding to the mature miRNA sequences (ranged from 368 to 3.7×1010 copies of RT input). The limits of linear quantification of each of the assays were determined with PCR efficiencies of 100±8% and linearities (Pearson's correlation) >0.99. To ensure the reliability of the data, values that were near or below the limits of the linear quantification were removed and excluded from further analyses. miRNA concentrations were normalised to the total RNA input and expressed as the number of copies per nanogram of RNA.
Statistical analysis
The statistical differences of miRNA levels between tumour and adjacent non-tumour tissues were determined by paired t test with univariate p value at <0.001 and false-discovery rate <0.001. Clustering of the differentially expressed miRNAs was performed with centred correlation and average linkage. The differences of serum miRNAs before and after surgery were studied by Wilcoxon signed-rank test, and p value at <0.05 was considered statistically significant. Logistic regression analysis was performed to analyse various combinations of miRNA markers. The receiver operating characteristic (ROC) curve and the area under the curve (AUC) were used to determine the feasibility of using serum miRNA concentration as a diagnostic marker for defining HCC. The Youden's Index was used to identify the optimal cut-off point.
Results
Candidate miRNAs are highly expressed in AFP-low tumour tissues
To generate a comprehensive set of miRNA expression profiles for HCC, we analysed expressions of 220 miRNAs from 96 pairs of HCC tumour and adjacent non-tumour tissues using real-time qPCR as described.15 Clustering analysis revealed that HCC and non-tumour tissues expressed distinct patterns of miRNAs as shown in the heat map (figure 2A). Furthermore, statistical analysis using paired t test identified that 105 miRNAs were differentially expressed with false-discovery rate <0.001.

(A) Hierarchical clustering (centred correlation and average linkage) over 105 differentially expressed microRNAs (miRNAs). Heat map colours represent the relative miRNA expression as indicated in the colour key. (B) Expressions of the candidate miRNA biomarkers in hepatocellular carcinoma tumour (TU) and adjacent non-tumour (AN) tissues. The tumour tissues were subdivided into three groups according to the serum α-fetoprotein (AFP) levels of the individual patients (AFP <20, between 20–400 and >400 ng/ml). The box plots show the median (horizontal bar), 25th and 75th percentiles and the whiskers of the graph show the largest and smallest values.
Given the marked miRNA alteration in tumour tissues, our next question is whether certain miRNAs could be useful for detecting HCC cases, including those with low serum AFP of <400 ng/ml. We identified the following 14 miRNAs upregulated in the AFP-low HCC subgroup: miR-9, -9*, -15b, -21, -34c, -96, -130b, -183, -188, -196b, -216, -224, -301 and -324-5p. Subsequently, we selected those having high copy number (>100 copies/10 pg input RNA) present in the tumour tissues. Consistently, these six miRNAs (miR-15b, -21, -130b, -183, -224 and -301) were highly expressed in all HCC samples of varying serum AFP levels (figure 2B).
Detection of candidate miRNAs in HCC culture supernatant
Our next selection criterion is whether the miRNAs can be measured or detected in the culture supernatants from a panel of HCC cell lines. We thus assayed by qPCR the above selected miRNAs in culture media conditioned with a panel of HCC cell lines, including HepG2, Hep3B, PLC/PRF/5 and MHCC-97H. Two immortalised human hepatocyte cell lines, CL-48 and MIHA, were included as controls. All the miRNAs could be detected in the culture media, except miR-301 and miR-224, whose concentrations were beyond the detection limits and thus were excluded from further analyses. We found that miR-15b, miR-21, miR-183 and miR-130b had generally higher copy numbers in the medium of HCC cells when compared to CL-48 or MIHA (figure 3).

TaqMan quantitative PCR assay of extracellular levels of four candidate biomarkers, miR-15b, miR-21, miR-130b and miR-183, in culture medium harvested from four hepatocellular carcinoma cell lines (HepG2, Hep3B, PLC/PRF/5 (PLC) and MHCC-97H (97H)) and two immortalised hepatocyte cell lines (CL-48 and MIHA). The assays were repeated at least twice in different samples. The error bars represent mean±SEM.
Detection of miRNAs in serum samples from patients with HCC pre- and post-surgery
To determine if the circulating miRNAs were derived primarily from tumours, we measured their levels in serum samples of 15 selected patients with HCC before and after surgery treatment. In agreement with the tissue data as stated above, miR-224 and miR-301 levels were very low in the sera (data not shown). For the other four miRNAs, there was a trend of reduction of miRNAs levels after surgery. As shown in figure 4, the median copies of miR-130b decreased significantly from 124.8 to 96.2 (p=0.0158) and miR-183 from 153.3 to 95.2 (p=0.0084). We also observed reductions of miR-15b and miR-21 levels after surgery, although the declination was not statistically significant. The median level of miR-15b was reduced from 177.6 to 64.1 (p=0.0637), whereas the median level of miR-21 was decreased from 221 404.4 to 100 140.5 (p=0.0648).

Declination of serum microRNA (miRNA) markers in patients with hepatocellular carcinoma (HCC) after surgery treatment. Changes in serum levels of miR-15b, miR-21, miR-130b and miR-183 in patients with HCC (n=15) before (pre-op) and after (post-op) surgical removal of the tumours. Statistical differences were analysed using Wilcoxon signed-rank test. Table in the lower panel indicates the median level of the individual miRNAs before and after surgery.
Circulating miR-15b and miR-130b classifier defines HCC cases in an independent cohort
We next verified the discriminative power of these miRNAs in identifying HCC cases in an independent cohort of 30 healthy controls, 29 hepatitis B individuals and 57 patients with HCC. The levels of the four miRNAs in these serum samples were measured, and ROC analysis was performed on individual miRNAs. The cut-off of each miRNA was selected with highest Youden's Index. Among the four miRNAs, miR-130b showed the highest AUC of 0.913 (sensitivity of 87.7% and specificity of 81.4%) in separating the non-cancerous controls from those with HCCs, whereas miR-15b gave the highest sensitivity (98.3%), although its specificity (15.3%) was only modest (table 2).
Predictive performance of individual serum miRNAs and miRNA classifier (miR-15b and miR-130b) as biomarkers for detection of HCC
Recognising the limitations of individual tests, we performed multivariate logistic regression analysis on various combinations of the miRNA biomarkers and found that the combined miR-15b and miR-130b gave the best performance. It could be a potential classifier for detecting HCC, and the formula of the classifier is as follow:
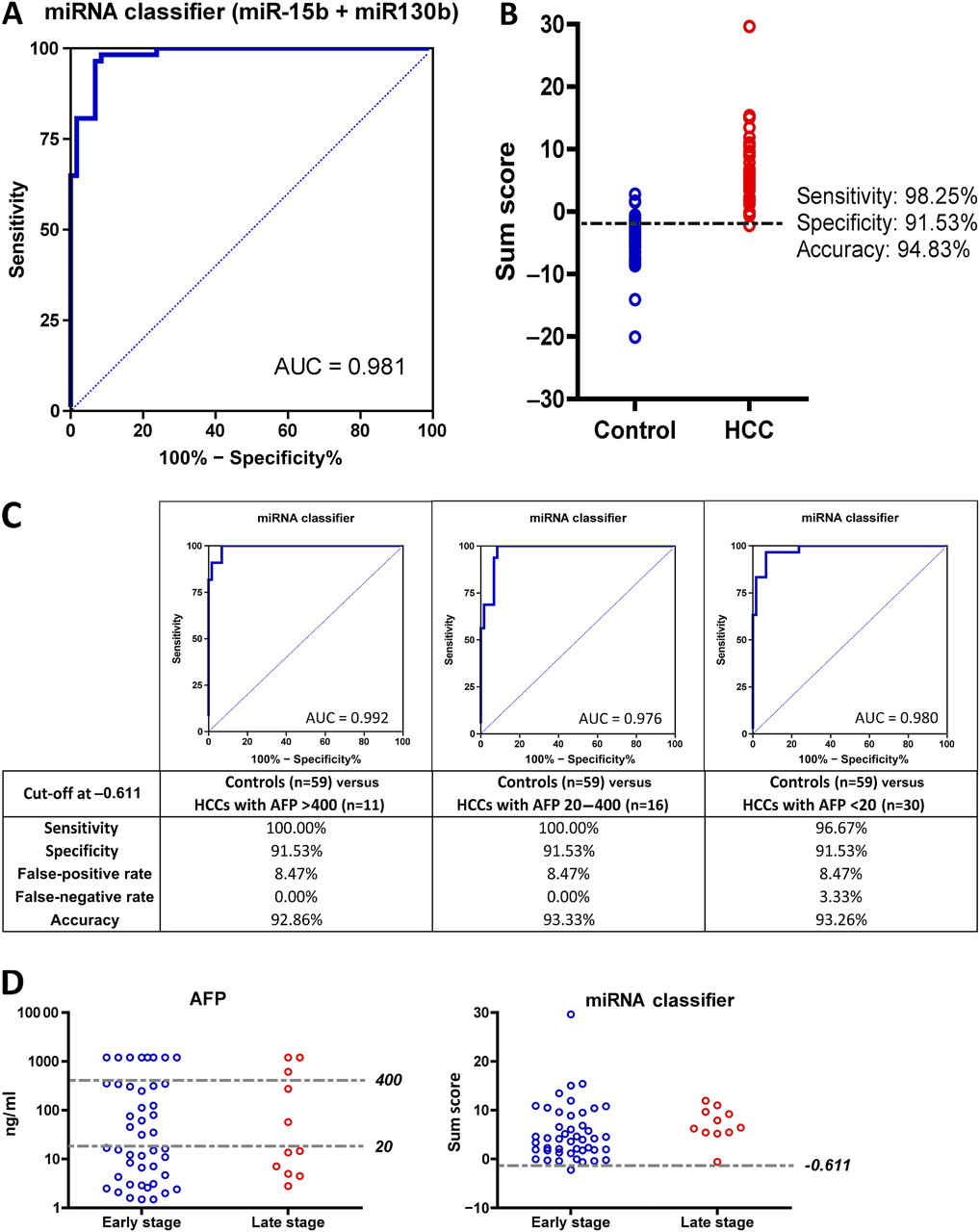
The ROC curve of the classifier has an AUC of 0.981 (figure 5A). A sum score of the classifier at −0.61109 was chosen as a cut-off, as it has the highest Youden's Index of 0.8977. At this cut-off, the classifier has enhanced sensitivity of 98.3% and specificity of 91.5% (figure 5B) when compared to the performance of individual miRNAs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Performance of the miR-15b and miR-130b classifier for detection of hepatocellular carcinoma (HCC) in an independent cohort. (A) Receiver operating characteristic (ROC) curve analysis of the microRNA (miRNA) classifier over patients with HCC and non-cancerous control subjects (healthy and chronic hepatitis B carriers). The miRNA classifier was derived from the logistic regression model that composed of two miRNAs, that are, miR-15b and miR-130b. (B) Dot plots of the sum score of the logistic regression model in non-cancerous control subjects (Control) and patients with HCC (HCC). The sensitivity, specificity and accuracy were calculated based on the cut-off at −0.611 that was determined by the Youden's Index. (C) ROC curve analyses of the miRNA classifier over control subjects (healthy and chronic hepatitis B individuals) and subgroup of patients with HCC with α-fetoprotein (AFP) levels >400, between 20 and 400 or <20 ng/ml. The sensitivity, specificity, false-positive rate, false-negative rate and accuracy at a cut-off of −0.611 were indicated below each ROC graph. (D) AFP and miRNA classifier (miR-15b and miR-130b) were compared in HCC cases between early (I and II) and late (III and IV) stages. The cut-off values were marked by grey lines. AUC, area under the curve.
We next tested if the classifier could successfully differentiate a subset of patients with low serum AFP from non-cancerous controls. Three subgroups were defined: (1) HCCs with AFP >400 ng/ml (n=11) and non-cancerous controls (n=59); (2) HCCs with AFP between 20 and 400 ng/ml (n=16) and non-cancerous controls (n=59); (3) HCCs with AFP <20 ng/ml (n=30) and non-cancerous controls (n=59). We found that the classifier could accurately distinguish subjects with HCC from the controls with high sensitivity and specificity in all cases (figure 5C). For the HCC subgroup with AFP <20 ng/ml, the AUC of the classifier is 0.980, with sensitivity of 96.7% and specificity of 91.5%.
Next, we evaluated the performance of miR-15b and miR-130b classifier in detecting early-stage HCC cases. As shown in figure 5D, the miRNA classifier could accurately identify 97.8% (44 out of 45) HCC cases from both tumour-node-metastasis stages I and II, whereas serum AFP (cut-off level at 20 ng/ml) could only detect 48.9% (22 out of 45) of the same cases. In short, the circulating miR-15b and miR-130b is a classifier that outperforms the serum AFP as tumour marker in detecting HCC.
Discussion
The present study has developed an unprecedented miRNA scoring system able to identify HCC cases that could not be detected by the conventional AFP tumour marker. Our in vitro studies also showed that the extracellular miRNAs are good indicator of the miRNA expression in cancer cells. These finding collectively implicate the potential application of circulating miRNAs as a non-invasive serological biomarker for solid malignancy like HCC.
Our tumour biomarker discovery strategy is divided into three phases: (1) Exploration phase: to identify candidate markers through molecular profiling of miRNAs in matched tumour and adjacent non-tumour tissues samples from patients with HCC (n=96). (2) Selection/filtering phase: to select those miRNAs highly expressed in both tumour tissues as well as in serum samples. In addition, we used preoperative and postoperative serum samples from the same patients with HCC (n=15) to further refine those miRNAs that were likely derived from HCC tumours. After surgical removal of the HCC tumours, serum levels of these miRNAs were significantly reduced. (3) Cross-centre validation phase: to validate the miRNA biomarkers in an independent cohort (n=116), including HCC cases, hepatitis B carriers and non-malignant healthy controls from geographically distant medical centre. Herein, our findings showed that the combined miR-15b and miR-130b is a robust classifier in detecting HCC cases and outperforms AFP as tumour marker with high positive predictive value.
Previous studies have suggested the potential use of circulating miRNAs in the diagnosis of HCC.20 21 The study by Qu et al21 suggested that serum miR-16 could be used as a second-line test when the serum AFP and other markers are at normal levels. However, in our analysis, we did not find miR-16 significantly differentially expressed between tumour and adjacent normal tissues. Another study using Solexa sequencing on pooled serum samples identified miR-375 as a candidate biomarker for HBV-positive HCC, which was further validated by TaqMan miRNA qPCR assays.20 The majority of the HCC cases in our cohort were also HBV-positive, but we did not select miR-375 during our initial screen. This is because the difference was not significant when comparing the HCC tumours of low AFP level with the corresponding normal samples. Nevertheless, we indeed found miR-375 has an important role in regulating YAP oncogenic signalling pathway in HCC.22 Further investigation is under way to evaluate the application of miR-375 for identifying subtype of HCC, for which the Hippo-YAP signaling is aberrantly regulated.
Limited information of miR-15b is available in HCC, and its molecular mechanisms and roles in pathogenesis remain largely unknown. Consistent with the present findings, miR-15b was recently shown to be overexpressed in HCC tumours,23 and it is in a pilot cross-sectional, phase II biomarker study for Barrett's oesophagus progression.24 Recently, miR-15b has been shown to be a direct transcriptional target of E2F and may be involved in preventing replicative stress in response to mitogenic signalling.25 On the other hand, the oncogenic role of miR-130b in hepatocarcinogenesis is prominent and is considered as a cancer stem cell miRNA in HCC. First, it has been shown highly expressed in CD133+ tumour-initiating cells in HCC, and transduction of miR-130b into CD133-negative cells could promote tumourigenesis and induce chemoresistance.26 Second, miR-130b directly targets a well-known tumour suppressor, RUNX3, and regulates expression of pro-apoptotic Bim, thereby enhancing cell viability.27 Despite of these observations, it is still unknown if miR-15b and miR-130b in circulation contribute to HCC development and tumour progression.
Although the miRNA classifier gave a high positive predictive value in our HCC cohort, there are several limitations in this study. First, the classifier has yet to be validated in other ethnic populations, such as Europe and Japan in which hepatitis C virus is the major aetiology of HCC. Second, the post-surgical serum samples were in small sample size and varied at different time points. It would be imperative to test more longitudinal samples in order to justify the specific time or period that the circulating miRNAs return to basal levels.
There are mounting evidences indicating that serum-based miRNAs are useful as non-invasive biomarkers for different cancer types.14 28–32 Today, circulating miRNAs in serum have been reported as potential diagnostic markers for B cell lymphoma,33 leukaemia,34 oesophageal squamous cell carcinoma,35 as well as lung,36 breast,37 colon,38 gastric,39 pancreatic,40 prostate41 and ovarian42 cancers. A handful of studies showed that miRNAs could be released into bloodstream via active secretion from diseased tissues in forms of protein-bound complex43or as membrane-bound vesicles (eg, exosomes).44 Because of the high rate of proliferation and cell lysis in tumours, non-specific passive release could also exist in cancer that contribute to the abundance of miRNAs in the bloodstream. Not only reflecting physiological and pathological changes, these circulating miRNAs could be functional and correlated with tumour progression and clinical outcomes.32 45 46 Most recently, miR-16, -21, -122 and -375 in serum were suggested as potential diagnostic markers for HCC.20 21 47 Nevertheless, their diagnostic performance has not been robustly validated in an independent cohort. Our present findings demonstrate that the circulating miR-15b and miR-130b hold promise as valuable tumour markers for detecting HCC, in which both the early-stage and low-AFP groups were covered with high sensitivity and specificity. Early detection of HCC could save many lives and enhance the quality of life in patients suffering from this lethal malignancy.
References
Footnotes
To cite: Liu AM, Yao T-J, Wang W, et al. Circulating miR-15b and miR-130b in serum as potential markers for detecting hepatocellular carcinoma: a retrospective cohort study. BMJ Open 2012;2:e000825. doi:10.1136/bmjopen-2012-000825
Contributors AML: experimental design, experimental performance, analysis of data and drafting of the manuscript; T-JY: statistical analysis and revision of the manuscript; WW: experimental performance; K-FW: drafting and revision of the manuscript; NPL: revision of the manuscript and material support; STF: acquisition of clinical samples and revision of the manuscript; RTPP: acquisition of clinical samples and study supervision; CG: acquisition of clinical samples and revision of the manuscript; JML: study design, study supervision and revision of the manuscript.
Funding The research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.