Article Text

Abstract
Objectives To compare necrotising enterocolitis (NEC) prevention practices and NEC associated factors between units from eight countries of the International Network for Evaluation of Outcomes of Neonates, and to assess their association with surgical NEC rates.
Design Prospective unit-level survey combined with retrospective cohort study.
Setting Neonatal intensive care units in Australia/New Zealand, Canada, Finland, Israel, Spain, Sweden, Switzerland and Tuscany (Italy).
Patients Extremely preterm infants born between 240 to 286 weeks’ gestation, with birth weights<1500 g, and admitted between 2014–2015.
Exposures NEC prevention practices (probiotics, feeding, donor milk) using responses of an on-line pre-piloted questionnaire containing 10 questions and factors associated with NEC in literature (antenatal steroids, c-section, indomethacin treated patent ductus arteriosus and sepsis) using cohort data.
Outcome measures Surgical NEC rates and death following NEC using cohort data.
Results The survey response rate was 91% (153 units). Both probiotic provision and donor milk availability varied between 0%–100% among networks whereas feeding initiation and advancement rates were similar in most networks. The 9792 infants included in the cohort study to link survey results and cohort outcomes, revealed similar baseline characteristics but considerable differences in factors associated with NEC between networks. 397 (4.1%) neonates underwent NEC surgery, ranging from 2.4%–8.4% between networks. Standardised ratios for surgical NEC were lower for Australia/New Zealand, higher for Spain, and comparable for the remaining six networks.
Conclusions The variation in implementation of NEC prevention practices and in factors associated with NEC in literature could not be associated with the variation in surgical NEC incidence. This corroborates the current lack of consensus surrounding the use of preventive strategies for NEC and emphasises the need for research.
- neonatology
- paediatric gastroenterology
- perinatology
- paediatrics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We report on a large, multinational patient database and high survey response rate, enabling a snapshot of contemporary necrotising enterocolitis outcome and practices.
Survey was completed by a single representative at each site rather than all practitioners, whereas responses were based on neonatal intensive care unit policies rather than personal opinion.
As individual patient data for NEC prevention were not available, we applied a pragmatic approach linking unit level survey data on prevention with patient level cohort data on outcome and risk factors to report on a possible association between NEC prevention and outcome.
When linking survey with cohort study data we have assumed that all neonates within a unit were treated equally, which is an assumption and needs confirmation but is acceptable for generating a hypothesis.
Introduction
Necrotising enterocolitis (NEC) remains a potentially devastating complication with variable treatment success rates. In the USA and Canada, NEC affects approximately 7% of babies weighing between 500–1500 g with approximately 20%–30% of mortality rate.1 A recent systematic review revealed similar or lower incidence rates for Japan (1.6%), Italy (3%), Korea (6.4%) and Spain (6.9%) for infants born <1500 g.2 In a study from the National Institute of Child Health and Human Development (NICHD) of extremely preterm infants born between 2000–2011, NEC related deaths rose from 23% to 30%, whereas overall mortality declined.3 In survivors, NEC and surgery for NEC have been associated with increased risk of adverse neurodevelopmental outcome at 2 years of age.4–6 The financial impact of NEC is estimated at US$1 billion per year in the USA alone.7
NEC is considered a multifactorial disease that results in profound inflammation and intestinal injury.7 8 Research in preventive measures is progressing but a unanimously accepted approach is yet to be identified. Probiotics supplementation reduced rates of NEC in multiple studies; however, results of two large randomised clinical trials are contradictory with no consensus on which probiotic may effectively prevent NEC.9 10 Donor milk and exclusive human milk diets are also proposed as preventive measures, however, the evidence for NEC reduction is tentative at best.11 12 Early initiation and rapid advancement of feeds have not been shown to cause harm, but standard practice in many units has not changed due to fear of NEC.13
In this context, our objective was to investigate what the uptake of preventative approaches at various units was and whether different approaches to prevention and different incidences of factors associated with NEC in literature were associated also with variations in the incidence of surgical NEC in the participating eight high-income countries.
Methods
Study design, questionnaire and population
In this mixed methods study, we used a survey to determine unit level NEC prevention practices in each country, and a retrospective patient cohort to obtain patient level NEC associated factors and rates for surgical NEC and mortality following NEC.
Survey (unit level data)
In 2016, an online pre-piloted, anonymous questionnaire was sent to the directors of 168 tertiary neonatal intensive care units (NICUs) from eight collaborating networks: Australia/New Zealand Neonatal Network, Canadian Neonatal Network, Finish Medical Birth Register, Israel Neonatal Network, Spanish Neonatal Network, Swedish Neonatal Quality Register (SNQ), Swiss Neonatal Network and the Tuscany Neonatal Network in Italy. The questionnaire contained questions about treatment practices relating to extremely preterm infants under 29 weeks’ gestation. The methodology for this survey was as published previously.14 Reminders were sent twice (at a monthly interval) to units that did not respond. The survey was first sent in August 2016 and was closed in December 2016. Responders were instructed to answer all questions based on their practices in the year 2015. One response per unit (usually the director) was collected. The 10 questions relevant to NEC comprised four domains, including probiotic usage (five questions), start and advancement of enteral feeding (three questions), donor-milk availability and donor-milk handling (two questions). The survey was distributed in English and is provided as a supplementary file (see online supplement 1).
Supplemental material
Cohort study (patient level data)
Patient data collected from infants born between 240 to 286 weeks’ gestation, weighing <1500 g and admitted to same neonatal units between 1 January 2014 and 31 December 2015 were compared between the eight participating countries. Extremely preterm infants of <24 weeks’ gestation were excluded from the current study, as admission to care and care provision to such infants varies considerably among the eight collaborating countries. Infants with major congenital anomalies and those born outside any of the participating hospitals and admitted after 1 week of age were excluded, as these infants may not have received all described preventive measures.
All networks have obtained ethical/regulatory approval or its equivalent from their local granting agencies to allow for de-identified data to be collated and sent to the International Network for Evaluation of Outcomes of Neonates (iNeo) Coordinating Centre. Overall coordination of the project is also approved by the Research Ethics Board at the Mount Sinai Hospital, Toronto, Ontario Canada for the development, compilation, hosting and management of the iNeo dataset at the MiCare Research Centre (12–0336-E). Privacy and confidentiality of patient data is of prime importance to the iNeo collaboration and data handling is in accordance with the Privacy Commissioner’s guidelines.
Covariate definitions
Gestational age (GA) was determined by the best estimate based on early prenatal ultrasound, last menstrual period, or physical examination of infants at birth, in that order. Birth weight z scores were calculated relative to population-specific and sex-specific birth weight for GA references selected by each network as most appropriate for the comparison. Antenatal steroid use was defined as any administration before birth, regardless of the time interval, patent ductus arteriosus (PDA) by clinical or echocardiographic diagnosis and sepsis by clear clinical evidence of infection as well as at least one relevant positive result from blood or cerebral fluid cultures.
Outcomes and measures
A lack of consensus on defining NEC among the eight participating countries led us to use surgical NEC as primary outcome. Surgical NEC was defined as laparotomy, laparoscopy, bowel resection, or intraperitoneal drain placement for NEC or suspected NEC. Indication to operate was pneumoperitoneum or clinical deterioration despite maximal medical therapy.15–17 Using surgical NEC as primary outcome also allows exclusion of potential cases of spontaneous intestinal perforations (SIP) as they can be identified reliably only at surgery, unless the surgery was limited to peritoneal drainage. Mortality following NEC was defined as death after receiving a diagnosis of NEC stage 2 or above, according to Bell’s criteria,18 and was analysed to ensure that the comparison of surgical NEC among countries was not biased by a high proportion of potential surgical NEC cases missing due to higher NEC death rates. As Sweden does not collect NEC data according to Bell's criteria, its mortality following NEC may be somewhat lower than reported.
Statistical analysis
Unit level analyses
Unit level survey responses were reported using descriptive statistics and reported as percentages or displayed graphically.
Mixed level analyses
Unit level data for preventative approaches of probiotic usage, early feeding and donor milk availability were analysed for their association with patient level data of surgical NEC. A multi-level logistic regression model was developed with surgical NEC as dependent variable, and unit-level practices (probiotics, early feeding and donor milk use) and individual patient level data (GA, male sex, multiple births and birth-weight z-score) as independent variables. Adjusted ORs and 95% CI were calculated. This analysis was not possible for Australia/New Zealand and Spain, as permission for linking survey information and patient data were not available. No model could be developed for networks where all units provided any of the prophylactic approach to all or to none of their patients. Generalised estimation equation was used to account for auto-correlation within units.
Patient level analyses
Patient level data were used to calculate variations in baseline characteristics, factors associated with NEC in literature, surgical NEC rates and mortality following NEC for participating networks. Standardised ratios (SRs) for participating networks were calculated as the observed number of infants who received NEC surgery divided by the number of infants expected to receive NEC surgery, based on the sum of predicted probabilities from a multivariable adjusted logistic regression model using data from all other countries in the study. Adjustment was made for the same parameters as for the ORs. Standardised ratio (SR) estimates were graphically displayed. As the SR estimates are calculated in relation to all other countries combined, it is not directly comparable between contributors. Data management and statistical analyses were performed at the iNeo Coordinating Centre in Toronto, Canada using SAS V.9.2 (SAS Institute).
Patient and public involvement
This study used de-identified data. Patients or public were not involved in the development of the research question, the outcome measures or the study design. The results of this study will be disseminated to the public via the iNeo-website (www.ineonetwork.org) and to the parent groups of the individual networks.
Results
Unit level analyses of survey
Probiotics
Out of a total of 168 network units, 153 (91%) responded to the online survey (table 1). Probiotic provision for infants born <29 weeks’ gestation ranged from 0% of units in Israel and Sweden to 100% of units in Finland. Among units providing probiotics, initiation of therapy ranged from 0 to 3 days of age in most units. Lactobacillus and/or Bifidobacterium were the preferred probiotic species; however, other species were provided as well (see online supplement 2). In most units in Australia/New Zealand, Finland and Tuscany, probiotic supplementation was continued in cases of culture positive sepsis, whereas most units in Switzerland stopped providing probiotics.
Supplemental material
Results of survey of NEC prevention practices and unit-level linked outcome analyses
Enteral feeding
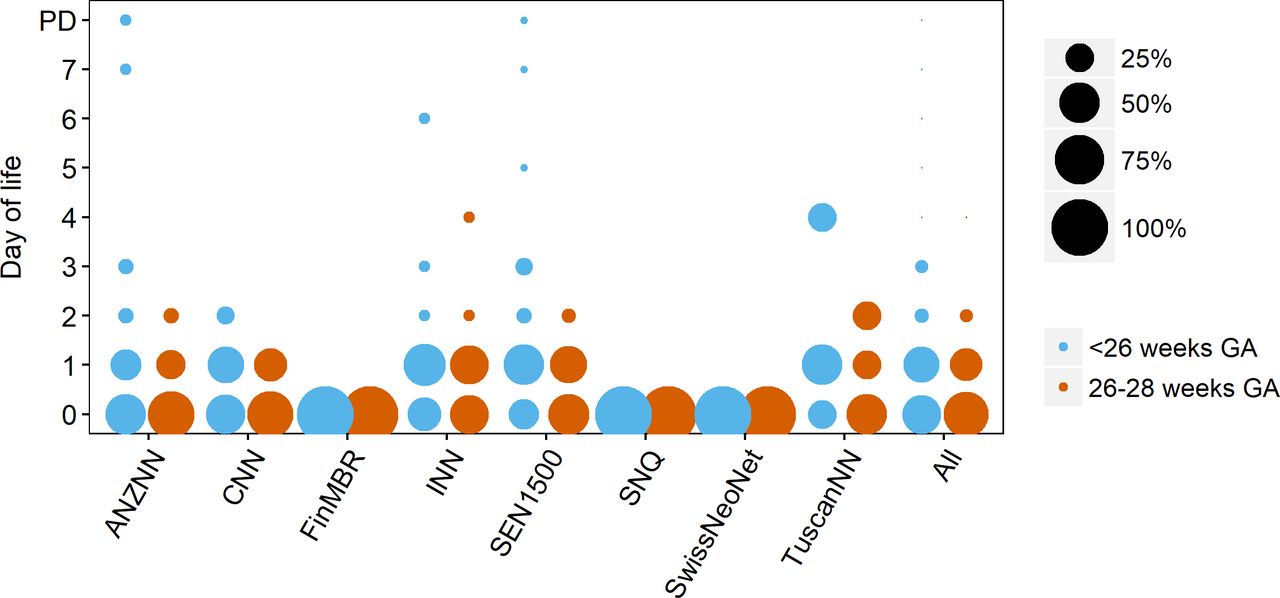
Table 1 summarises enteral feeding initiation and advancement practices for infants <26 weeks’ gestation and between 26–28 weeks’ gestation. Figure 1 summarises feeding initiation in both age groups. The majority of units began enteral feeding on first or second day of life. In Finland, Sweden and Switzerland, all units reported initiating feeding on first day of life. There was some variation in daily rates of advancement between and within all networks, with a majority of units advancing at rates between 10 to 25 mL/kg/day. No overall preference in enteral feeding volume was seen in infants who received milk fortifier, with a range in administration varying between 70–120 mL/kg/day.

Routine start of enteral feeding for extremely preterm infants. Bubble chart displaying routine start of enteral feeding for network infants<26 weeks’ gestation and 26–28 weeks’ gestation. Circle size corresponds to proportion of units per network with routine start of enteral feeding at any given day. ANZNN, Australian and New Zealand neonatal network; CNN, Canadian Neonatal Network; FinMBR, Finnish medical birth register; GA, gestational age; INN, Israel Neonatal Network; PD, physician dependent; SEN1500, Spanish neonatal network; SNQ, Swedish Neonatal Quality Register; SwissNeoNet, Swiss neonatal network; TuscanNN, Tuscan neonatal network.
Donor Milk
Donor milk availability ranged between 0% of units in Israel to 100% of units in Finland, Sweden and Tuscany. A majority of units in Spain, Switzerland and Tuscany had initiation criteria at <32 weeks’ gestation or <1501 g weight, whereas in Sweden most units provided donor milk at <34 weeks’ gestation. No uniform stopping criteria for donor milk use were applied by most units, except for Tuscany where the majority of units stopped at 1800 g. Units in Finland and Spain used variable criteria other than age or weight for starting and stopping donor milk provision.
Mixed level analyses of surveyed practices and surgical NEC
Probiotics: We could only compare units in Canada which showed no difference in surgical NEC with probiotics and Switzerland which showed lower odds with probiotics (table 1). The adjusted OR combining all units from the six networks allowing linkage between unit survey and cohort study revealed no significant association of probiotics provision with surgical NEC (0.84, 95% CI 0.61 to 1.16).
Early initiation of feeding: Data from Canada, Israel and Tuscany were available for comparative analyses (table 1). Except for neonates of 26–28 weeks’ GA in Tuscany there was no difference in odds of surgical NEC in group who were initiated feeds on day of birth compared with units which started feeds later. The adjusted OR combining all units providing enteral feeding on day 0 revealed no significant association to surgical NEC (1.16, 95% CI 0.83 to 1.63).
Donor milk: Data from Canada and Switzerland were available for comparative analyses. There was no difference in odds of surgical NEC between units which provided donor milk compared with those units which did not provide donor milk. The adjusted OR combining all units also revealed no association (table 1).
Patient level analyses of cohort study
A total of 9792 infants were included in the analysis. The baseline characteristics in table 2 reveal a small variation among networks in their overall mean GA (range 26.3–26.5 weeks), mean birth weight z-score (−0.22 to +0.18), SGA-ratios (8.8%–12.8%) and male sex distribution (51.5%–55.3%). There was considerable variation between networks among factors associated with NEC in literature: receipt of antenatal steroids ranged from 82.9% in Israel to 97.3% in Finland, caesarean section ranged from 60.0% in Canada to 82.7% in Switzerland, PDA treated with indomethacin ranged from 0% in countries exclusively administering ibuprofen or paracetamol to treat PDA (Spain, Sweden, Tuscany) to 39.6% in Switzerland and sepsis ranged from 14.6% in Switzerland to 46.2% in Spain.
Baseline characteristics, factors associated with NEC in literature and outcomes in neonates 240–286 weeks’ gestation between 2014–2015 (patient level data)
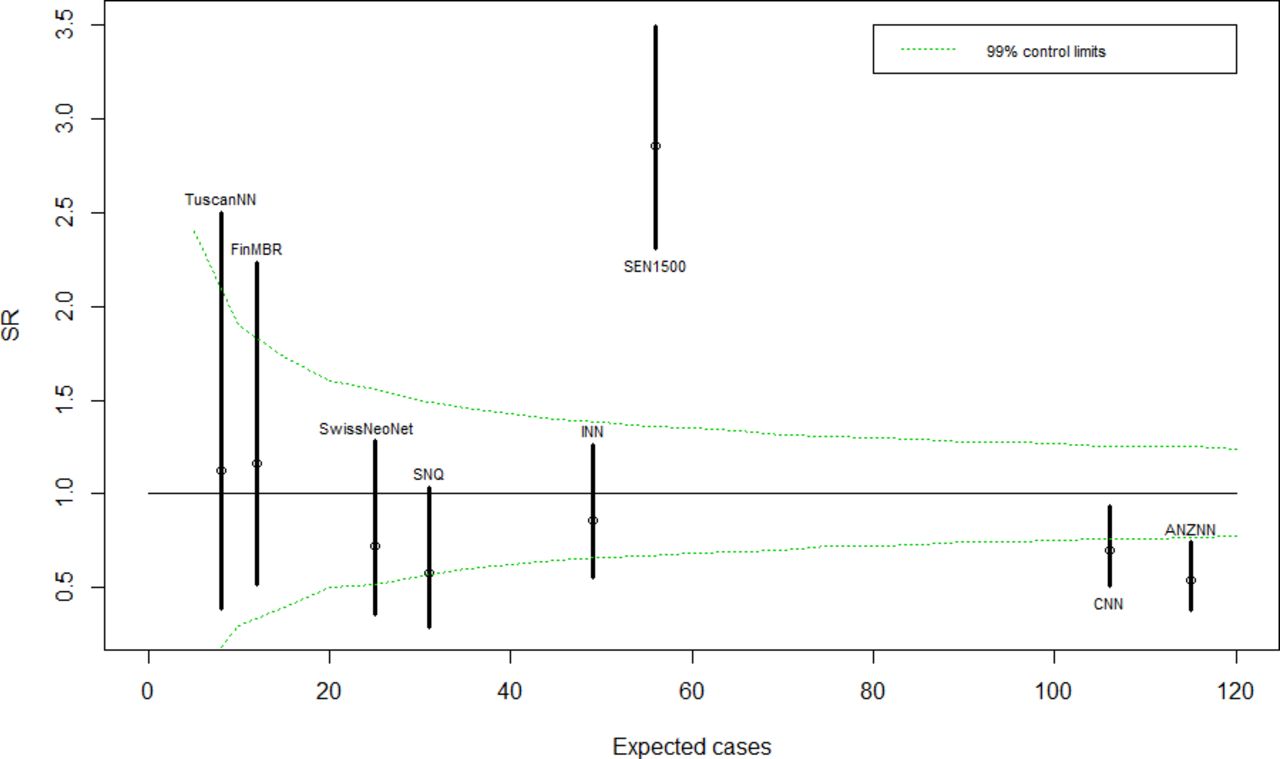
Overall, average surgical NEC incidence rate in all countries combined was 4.1%, (ranging from 2.4% in Australia and New Zealand and 8.4% in Spain) whereas death following NEC diagnosis occurred in 2.4% of all infants (ranging from 1.4% in Sweden to 3.3% in Spain) (table 2, figure 2). As none of the countries had higher rates of mortality following NEC in relation to their surgical NEC incidence rate, we ruled out the possibility that the surgical NEC incidence rate of any country is under-reported due to death before surgery can take place. Australia/New Zealand had lowest adjusted standardised ratios for surgical NEC whereas Spain had the highest standardised ratio among participating networks (figure 3).

Necrotising enterocolitis surgery prevalence rate and 95% CI by network for 2014–2015. ANZNN, Australian and New Zealand neonatal network; CNN, Canadian Neonatal Network; FinMBR, Finnish medical birth register; INN, Israel Neonatal Network; NEC, necrotising enterocolitis; SEN1500, Spanish neonatal network; SNQ, Swedish Neonatal Quality Register; SwissNeoNet, Swiss neonatal network; TuscanNN, Tuscan neonatal network.

{kind=link}
{kind=link}
{kind=link}
Standardised ratios for surgically treated necrotising enterocolitis from 2014 to 2015. Standardised ratios were adjusted for: gestational age, male sex, multiple birth and birth-weight z-score. abbreviations: ANZNN, Australian and New Zealand neonatal network; CNN, Canadian Neonatal Network; FinMBR, Finnish medical birth register; INN, Israel Neonatal Network; SEN1500, Spanish neonatal network; SNQ, Swedish Neonatal Quality Register; SwissNeoNet, Swiss neonatal network; SR, standardised ratio; TuscanNN, Tuscan neonatal network.
Discussion
In this large multi-centre, multi-national, mixed methods study linking unit level survey and retrospective patient level cohort data, we identified that, on a unit level, NEC preventive practices of using probiotics or donor milk varied from 0%–100% between networks, whereas feeding start age and advancement had minor variation between the units of each network. In mixed level analyses, probiotics were associated with reduced odds of surgical NEC in Switzerland and early feeding was associated with reduced odds of surgical NEC in Tuscany for neonates of 26–28 weeks’ gestation. Donor milk provision was not associated with surgical NEC. Patient level analyses revealed that 1 in every 25 admitted infants at 24–28 weeks’ gestation received surgical intervention for NEC with some variation between networks in incidence and NEC associated mortality. Standardised ratios for surgical NEC were lower in Australia/New Zealand, higher in Spain and comparable for the remaining six networks.
Multiple meta-analyses of randomised studies have shown that probiotics are associated with reduced rates of NEC and sepsis.19 20 However, a lack of consensus regarding the strain(s), dose and duration and timing of use has prevented many units from adopting it as a strategy. Moreover, the long-term effects on immune function and metabolism following replacement of a maternally derived intestinal microbiome with a dominant exogenous bacterial species is not known.21 The wide variation in units that participated in this study regarding their use, strains, start and stop time and the lack of association with surgical NEC rate may be due to the very high-risk population, different strains and the fact that this study involves the entire population at unit-level rather than a select population enrolled in randomised trial. The difference in results between systematic reviews and this study could be due to pooling of inhomogeneous studies into meta-analyses as concerns raised by several investigators indicate. Further pragmatic studies from multiple countries are needed.
There is evidence that implementing evidence-based standardised feeding guidelines reduces the incidence of NEC.8 Although such guidelines are not uniform, they have generally incorporated an early minimal enteral nutrition phase during which 10–20 mL/kg/d of enteral nutrition is provided without increase, followed by daily advancement based on continued tolerance. Older practices withheld feedings for days to weeks after birth in an attempt to avoid an assumed association of NEC with the start of enteral feeding.22 The majority of units among the eight participating countries initiate early feeding with rapid rates of advancement, with few units continuing to favour the slower approach. We found no association between feeding start and surgical NEC. This may be due to the very small number of units which delay feeds.
Although using donor milk in lieu of formula feedings has led to reduced NEC rates in recent studies, it is unclear whether donor milk itself protected against NEC or whether the avoidance of formula acted as a protective factor.8 We identified a large variation between networks regarding availability and provision of donor milk and varying preferences for initiation and stopping criteria. At unit level analyses, there was no association between donor milk and surgical NEC. One explanation may be that units without donor milk available may actually have a more active programme to help mothers provide breast milk.
Recent publications, several of them population-based, report NEC rates for very low birth weight infants (VLBW, 500–1500 g) in the range of 2%–12%.15 23–28 In a previous review, variations in rates across different NICHD centres and periods ranged from 1%–22% of VLBW infants between 1987–2000.29 Reported mortality of infants with NEC continues to remain high at approximately 15%–30%.15 30 Incidences of surgical intervention are less often reported but usually occur in 30%–50% of patients acquiring NEC.15 16 28 31 Considering these rates, the proportions of surgical NEC and death following NEC diagnosis in the current study are within the middle to upper range of previously published values, as expected given the lower GA range (240–286) of our study versus previously reported VLBW references. They correlate well with the NEC rates reported for infants<28 weeks GA in a recent review.2
The risk of acquiring NEC is inversely proportional to GA.8 16 31–34 Fetal growth restriction and male sex may be additional risk factors.27 31 In our study, GA and birth weight z-score were comparable and therefore they did not explain outcome variation between networks. Given the association between NEC and antenatal steroid administration,23 31 35 caesarean section,34 36 37 sepsis6 16 38 and PDA treated with indomethacin,36 39 40 we expected surgical NEC incidence to be affected by the variation of these factors between networks. However, there was no association in networks with up to 10% lower proportions of antenatal steroid use (Sweden, Israel), up to 17% lower proportions of vaginal delivery (Switzerland), and up to twice as many indomethacin-treated PDA patients (Switzerland). The only association observed was for the two networks with the highest proportions of surgical NEC (Tuscany, Spain), which also had the highest proportions of sepsis. This is noteworthy as it is known that sepsis and NEC can occur concurrently. But it is at times very difficult to differentiate which complication occurred first. It is possible that sepsis triggered the inflammatory response and may have led to ischaemia and on the other hand ischaemic bowel with increased permeability allowed translocation of bacteria from intestine into the blood stream.4 24 Our result highlights the need for increased efforts for prevention of infection in general for improved outcome of preterm neonates.
The lack of consensus on defining NEC has led to variable definitions in research databases and clinical trials.41 This challenge is reflected in the participating eight networks as well, where most networks used Bell's stage 2 as the defining threshold, while one network included ‘mild’ or ‘initial’ cases, corresponding to Bell’s stage 1.18 The current study therefore included iNeo networks collecting data on surgical NEC based on laparotomy or drainage, according to the accepted indication to operate in cases of pneumoperitoneum or clinical deterioration despite maximal medical therapy.15–17 Nevertheless, variation in threshold to operate in NEC may exist and contribute to variations in surgical NEC. The study is further restricted to infants<29 weeks’ gestation whose risk of acquiring NEC is enhanced and who are more likely to have a common pathogenesis.33 34 41
The current study is strengthened by the large, multinational patient database and high survey response rate, enabling a snapshot of contemporary outcome and practices. However, not all reporting networks are population based.42 Moreover, the survey was completed by a single representative at each site rather than all practitioners, but responses were based on NICU policies rather than personal opinion. We would have liked the analyses of individual per patient practices as this would have been the most ideal pragmatic scenario; however, in our database these items are not collected. Thus, in linking survey with cohort study we have assumed that all neonates within a unit were treated equally, which is an assumption and needs confirmation. However, it is acceptable for generating a hypothesis. Also, NEC-related mortality was based on Bell stage 2 even though the networks were not certain on whether all units reported NEC as of stage 2 only and did not by mistake also report on NEC stage I in some cases which are assumed to be exceptions. This uncertainty however led to our decision not to evaluate NEC stage 2 as primary outcome but instead revert to the more robust outcome of NEC surgery as primary outcome. The networks were however confident, that the reported NEC-related mortality predominantly based on Bell's stage 2 was accurate enough to rule out a large survival bias. Another limitation could arise if NEC surgery is limited to peritoneal drainage in a patient because without laparotomy, a differentiation between NEC and SIP cannot be made. In the context of this study, this is relevant as probiotic treatment would not be expected to influence SIP and a high SIP contamination could therefore bias the study results concerning probiotics. We however believe the effect of this bias to be small as the number of neonates with NEC exclusively managed by peritoneal drainage is usually small as primary peritoneal drainage is usually a temporising measure followed by definitive surgery or death prior to further surgery. Among the remaining cases exclusively treated by peritoneal drainage, there is no evidence to suggest that they would be predominantly cases of SIP.
In conclusion, the variation in NEC preventive practices between eight regionally defined networks of high-income nations was high for probiotic use and donor milk use, but less so for feeding practices. Despite large variabilities in factors known to influence NEC outcome, there was no significant relationship between the NEC preventive practice usage by units and surgical NEC rates. Overall, one in 25 extremely preterm neonates received NEC surgery. The standardised ratios for NEC surgery were significantly lower in Australia/New Zealand and significantly higher in Spain. Our results identify several areas of urgent research need and generates several hypotheses for studies aimed at improving outcome of this devastating disease. It also provides a platform for evaluating practices using a construct of comparative effectiveness research whereby pragmatic evaluation of two or more strategies can be conducted under the umbrella of a registry-based pragmatic clinical trial.43 44
Acknowledgments
The authors gratefully acknowledge all investigators and data abstractors of the networks participating in the iNeo consortium for their diligent work. We thank Iris Kulbatski, PhD and Sarah Hutchinson, PhD from the Maternal-Infant Care Research Centre (MiCare) in Toronto, Ontario, Canada, for editorial support for this manuscript and other MiCare staff for organisational and statistical support. We also acknowledge other networks which contributed to the survey but did not have information on patient outcomes available: the Neonatal Research Network Japan and the Illinois Neonatal Network.
References
Footnotes
Collaborators ANZNN (Australia and New Zealand Neonatal Network): Ross Haslam* Chair of the Executive Committee; Flinders Medical Centre, SA: Peter Marshall. Gold Coast University Hospital, QLD: Peter Schmidt. Gosford District Hospital, NSW: Adam Buckmaster*. John Hunter Children’s Hospital, NSW: Paul Craven, Koert de Waal*. King Edward Memorial and Princess Margaret Hospitals, WA: Karen Simmer, Andy Gill*, Jane Pillow*. Liverpool Hospital, NSW: Jacqueline Stack. Mater Mothers' Hospital, QLD: Lucy Cooke. Mercy Hospital for Women, VIC: Dan Casalaz, Jim Holberton*. Monash Medical Centre, VIC: Charles Barfield. Nepean Hospital, NSW: Lyn Downe, Vijay Shingde. Newborn Emergency Transport Service (VIC): Michael Stewart. NSW Pregnancy and Newborn Services Network: Barbara Bajuk*. NSW Newborn & Paediatric Emergency Transport Service: Andrew Berry. Royal Children's Hospital, VIC: Rod Hunt. Royal Darwin Hospital, NT: Charles Kilburn. Royal Hobart Hospital, Tasmania: Tony De Paoli. Royal Hospital for Women, NSW: Kei Lui*. Royal North Shore Hospital, NSW: Mary Paradisis. Royal Prince Alfred Hospital, NSW: Ingrid Rieger, Shelley Reid*. Royal Brisbane and Women's Hospital, QLD: David Cartwright, Pieter Koorts. Royal Women's Hospital, VIC: Carl Kuschel, Lex Doyle. Sydney Children's Hospital, NSW: Andrew Numa. The Canberra Hospital, ACT: Hazel Carlisle. The Children's Hospital at Westmead, NSW: Nadia Badawi, Robert Halliday. The Townsville Hospital, QLD: Guan Koh*. Western Australia Neonatal Transport Service: Steven Resnick. Westmead Hospital, NSW: Melissa Luig. Women's & Children's Hospital, SA: Chad Andersen. National Perinatal Epidemiology and Statistics Unit, University of New South Wales: Georgina Chambers*. New Zealand: Christchurch Women's Hospital: Adrienne Lynn, Brian Darlow. Dunedin Hospital: Roland Broadbent*. Middlemore Hospital: Lindsay Mildenhall. Auckland City Hospital: Mariam Buksh, Malcolm Battin. North Shore and Waitakere Hospitals: Jutta van den Boom*. Waikato Hospital: David Bourchier, Lee Carpenter*. Wellington Women's Hospital: Vaughan Richardson. Singapore: KK Women's and Children's Hospital, Singapore: Victor Samuel Rajadurai*. * denotes the ANZNN Executive Committee.
CNN (Canadian Neonatal Network): Prakesh S Shah, MD, MSc (Director, Canadian Neonatal Network and site investigator), Mount Sinai Hospital, Toronto, Ontario; Adele Harrison, MD, MBChB, Victoria General Hospital, Victoria, British Columbia; Anne Synnes, MDCM, MHSC, and Joseph Ting, MD, B.C. Women’s Hospital and Health Centre, Vancouver, British Columbia; Zenon Cieslak, MD, Royal Columbian Hospital, New Westminster, British Columbia; Rebecca Sherlock, MD, Surrey Memorial Hospital, Surrey, British Columbia; Wendy Yee, MD, Foothills Medical Centre, Calgary, Alberta; Khalid Aziz, MBBS, MA, MEd, and Jennifer Toye, MD, Royal Alexandra Hospital, Edmonton, Alberta; Carlos Fajardo, MD, Alberta Children’s Hospital, Calgary, Alberta; Zarin Kalapesi, MD, Regina General Hospital, Regina, Saskatchewan; Koravangattu Sankaran, MD, MBBS, and Sibasis Daspal, MD, Royal University Hospital, Saskatoon, Saskatchewan; Mary Seshia, MBChB, Winnipeg Health Sciences Centre, Winnipeg, Manitoba; Ruben Alvaro, MD, St. Boniface General Hospital, Winnipeg, Manitoba; Amit Mukerji, MD, Hamilton Health Sciences Centre, Hamilton, Ontario; Orlando Da Silva, MD, MSc, London Health Sciences Centre, London, Ontario; Chuks Nwaesei, MD, Windsor Regional Hospital, Windsor, Ontario; Kyong-Soon Lee, MD, MSc, Hospital for Sick Children, Toronto, Ontario; Michael Dunn, MD, Sunnybrook Health Sciences Centre, Toronto, Ontario; Brigitte Lemyre, MD, Children’s Hospital of Eastern Ontario and Ottawa General Hospital, Ottawa, Ontario; Kimberly Dow, MD, Kingston General Hospital, Kingston, Ontario; Ermelinda Pelausa, MD, Jewish General Hospital, Montréal, Québec; Keith Barrington, MBChB, Hôpital Sainte-Justine, Montréal, Québec; Christine Drolet, MD, and Bruno Piedboeuf, MD, Centre Hospitalier Universitaire de Québec, Sainte Foy Québec; Martine Claveau, MSc, LLM, NNP, and Marc Beltempo, MD, McGill University Health Centre, Montréal, Québec; Valerie Bertelle, MD, and Edith Masse, MD, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Québec; Roderick Canning, MD, Moncton Hospital, Moncton, New Brunswick; Hala Makary, MD, Dr. Everett Chalmers Hospital, Fredericton, New Brunswick; Cecil Ojah, MBBS, and Luis Monterrosa, MD, Saint John Regional Hospital, Saint John, New Brunswick; Akhil Deshpandey, MBBS, MRCPI, Janeway Children’s Health and Rehabilitation Centre, St. John’s, Newfoundland; Jehier Afifi, MB BCh, MSc, IWK Health Centre, Halifax, Nova Scotia; Andrzej Kajetanowicz, MD, Cape Breton Regional Hospital, Sydney, Nova Scotia; Shoo K Lee, MBBS, PhD (Chairman, Canadian Neonatal Network), Mount Sinai Hospital, Toronto, Ontario. FinMBR (Finnish Medical Birth Register): Sture Andersson, MD, Helsinki University Hospital, Helsinki; Liisa Lehtonen, MD, Turku University Hospital, Turku; Outi Tammela, MD, Tampere University Hospital, Tampere; Ulla Sankilampi, MD, Kuopio University Hospital, Kuopio; Timo Saarela, MD, Oulu University Hospital, Oulu. INN (Israel Neonatal Network): Eli Heymann, MD, Assaf Harofeh Medical Center, Tzrifin; Shmuel Zangen, MD, Barzilai Medical Center, Ashkelon; Tatyana Smolkin, MD, Baruch Padeh Medical Center, Poriya; Francis Mimouni, MD, Bikur Cholim Hospital, Jerusalem; David Bader, MD, Bnai Zion Medical Center, Haifa; Avi Rothschild, MD, Carmel Medical Center, Haifa; Zipora Strauss, Chaim Sheba Medical Center, Ramat Gan; Clari Felszer, MD, Emek Medical Center, Afula; Hussam Omari, MD, French Saint Vincent de Paul Hospital, Nazareth; Smadar Even Tov-Friedman, MD, Hadassah University Hospital-Ein Karem, Jerusalem; Benjamin Bar-Oz, MD, Hadassah University Hospital-Har Hazofim, Jerusalem; Michael Feldman, MD, Hillel Yaffe Medical Center, Hadera; Nizar Saad, MD, Holy Family (Italian) Hospital, Nazareth; Orna Flidel-Rimon, MD, Kaplan Medical Center, Rehovot; Meir Weisbrod, MD, Laniado Hospital, Netanya; Daniel Lubin, MD, Mayanei Hayeshua Medical Center, Bnei Brak; Ita Litmanovitz, MD, Meir Medical Center, Kfar Saba; Amir Kugelman, MD, Rambam Medical Center; Eric Shinwell, MD, Rivka Ziv Medical Center, Safed; Gil Klinger, MD, Schneider Children’s Medical Center of Israel, Rabin Medical Center (Beilinson Campus), Petah Tikva; Yousif Nijim, MD, Scottish (EMMS) Hospital, Nazareth; Alona Bin-Nun, MD, Shaare-Zedek Medical Center, Jerusalem; Agneta Golan, MD, Soroka Medical Center, Beersheba; Dror Mandel, MD, Sourasky Medical Center, Tel Aviv; Vered Fleisher-Sheffer, MD,Western Galilee Medical Center, Nahariya; David Kohelet, MD, Wolfson Medical Center, Holon; Lev Bakhrakh, MD, Yoseftal Hospital, Eilat. SEN1500 (Spanish Neonatal Network): Alejandro Avila-Alvarez, MD, and José Luis Fernandez-Trisac, MD, Complexo Hospitalario Universitario De A Coruña, A Coruña; Mª Luz Couce Pico, MD, and María José Fernández Seara, MD, Hospital Clínico Universitario de Santiago, Santiago de Compostela; Andrés Martínez Gutiérrez, MD, Complejo Hospitalario Albacete, Albacete; Carolina Vizcaíno, MD, Hospital General Universitario de Elche, Alicante; Miriam Salvador Iglesias, MD, and Honorio Sánchez Zaplana, MD, Hospital General Universitario de Alicante, Alicante; Belén Fernández Colomer, MD, and José Enrique García López, MD, Hospital Universitario Central de Asturias, Oviedo, Asturias; Rafael García Mozo, MD, and M. Teresa González Martínez, MD, Hospital Universitario de Cabueñes, Gijón, Asturias; Mª Dolores Muro Sebastián, MD, and Marta Balart Carbonell, MD, Clínica Corachán, Barcelona, Barcelona; Joan Badia Barnusell, MD, and Mònica Domingo Puiggròs, MD, Corporacio Parc Taulí, Sabadell, Barcelona; Josep Figueras Aloy, MD, and Francesc Botet Mussons, MD, Hospital Clínic de Barcelona, Barcelona; Israel Anquela Sanz, MD, Hospitalario De Granollers, Granollers; Gemma Ginovart Galiana, MD, H. De La Santa Creu I Sant Pau, Barcelona; W. Coroleu, MD, Hospital Universitari Germans Trias I Pujol, Badalona; Martin Iriondo, MD, Hospital Sant Joan de Déu Barcelona, Esplugues de Llobregat, Barcelona; Laura Castells Vilella, MD, Hospital General de Cataluña, Barcelona; Roser Porta, MD, Institute Dexeus, Barcelona; Xavier Demestre, MD, and Silvia Martínez Nadal, MD, Scias-Hospital Barcelona, Barcelona; Cristina de Frutos Martínez, MD, Hospital Universitario de Burgos, Burgos; María Jesús López Cuesta, MD, H. San Pedro de Alcántara, Cáceres; Dolores Esquivel Mora, MD, and Joaquín Ortiz Tardío, MD, Hospital Jerez, Cádiz; Isabel Benavente, MD, and Almudena Alonso, MD, Hospital Universitario Puerta Del Mar, Cádiz; Ramón Aguilera Olmos, MD, Hospital General de Castellón, Castellón; Miguel A. García Cabezas, MD, and Mª Dolores Martínez Jiménez, MD, Hospital General Universitario de Ciudad Real, Ciudad Real; Mª Pilar Jaraba Caballero, MD, and Mª Dolores Ordoñez Díaz, MD, Hospital Universitario Reina Sofía, Córdoba; Alberto Trujillo Fagundo, MD, and Lluis Mayol Canals, MD, Hospital Universitari de Girona Dr. Josep Trueta, Girona; Fermín García-Muñoz Rodrigo, MD, and Lourdes Urquía Martí, MD, H.M.I. Las Palmas, Las Palmas, Gran Canaria; María Fernanda Moreno Galdo, MD, and José Antonio Hurtado Suazo, MD, Hospital Universitario Virgen De Las Nieves, Granada; Eduardo Narbona López, and José Uberos Fernández, MD, Hospital Universitario San Cecilio, Granada; Miguel A Cortajarena Altuna, MD, and Oihana Muga Zuriarrain Hospital, MD, Donostia, Gipuzkoa; David Mora Navarro, MD, Hospital Juan Ramón Jiménez, Huelva, Huelva; María Teresa Domínguez, MD, Hospital Costa De La Luz, Huelva; Mª Yolanda Ruiz del Prado, MD, and Inés Esteban Díez, MD, Hospital San Pedro, Logroño, La Rioja; María Teresa Palau Benavides, MD, and Santiago Lapeña, MD, Hospital de León, León, León; Teresa Prada, MD, Hospital del Bierzo, Ponferrada, León; Eduard Soler Mir, MD, Hospital Arnau De Vilanova, Lleida; Araceli Corredera Sánchez, MD, Enrique Criado Vega, MD, Náyade del Prado, MD, and Cristina Fernández, MD, Hospital Clínico San Carlos, Madrid; Lucía Cabanillas Vilaplana, MD, and Irene Cuadrado Pérez, MD, Hospital Universitario De Getafe, Madrid; Luisa López Gómez, MD, Hospital De La Zarzuela, Madrid; Laura Domingo Comeche, MD, Hospital Universitario de Fuenlabrada, Fuenlabrada, Madrid; Isabel Llana Martín, MD, Hospital Madrid-Torrelodones, Madrid, Madrid; Carmen González Armengod, MD, and Carmen Muñoz Labián, MD, Hospital Universitario Puerta De Hierro, Majadahonda, Madrid; Mª José Santos Muñoz, MD, Hospital Severo Ochoa, Leganés, Madrid; Dorotea Blanco Bravo, MD, and Vicente Pérez, MD, Hospital Gregorio Marañón, Madrid; Mª Dolores Elorza Fernández, MD, Celia Díaz González, MD, and Susana Ares Segura, MD, H.U. La Paz, Madrid; Manuela López Azorín, MD, Hospital Universitario Quirónsalud Madrid, Madrid; Ana Belén Jimenez MD, Hospital Universitario Fundación Jiménez Díaz, Madrid; Tomás Sánchez-Tamayo, MD, and Elías Tapia Moreno, MD, Hospital Carlos Haya, Málaga; María González, MD, and José Enrique Sánchez Martínez, MD, Hospital Parque San Antonio De Málaga, Málaga; José María Lloreda García, MD, Hospital Universitario Santa Lucia De Cartagena, Murcia; Concepción Goñi Orayen, MD, Hospital Virgen Del Camino De Pamplona, Pamplona, Navarra; Javier Vilas González, MD, Complexo Hospitalario Pontevedra, Pontevedra; María Suárez Albo, MD, and Eva González Colmenero, MD, Hospital Xeral De Vigo, Pontevedra; Elena Pilar Gutiérrez González, MD, and Beatriz Vacas del Arco, MD, Hospital Universitario de Salamanca, Salamanca; Josefina Márquez Fernández, MD, and Laura Acosta Gordillo, MD, Hospital Valme, Sevilla; Mercedes Granero Asensio, MD, Hospital Virgen De La Macarena, Sevilla; Carmen Macías Díaz, MD, Hospital Universitario Virgen Del Rocío, Sevilla; Mar Albújar, MD, Hospital Universitari de Tarragona Joan XXIII, Tarragona; Pedro Fuster Jorge. MD, Hospital Universitario De Canarias, San Cristóbal de La Laguna, Santa Cruz de Tenerife; Sabina Romero, MD, and Mónica Rivero Falero, MD, Hospital Universitario Nuestra Señora De Candelaria, Santa Cruz de Tenerife; Ana Belén Escobar Izquierdo, Hospital Virgen De La Salud, Toledo; Javier Estañ Capell, MD, Hospital Clinico Universitario De Valencia, Valencia; Mª Isabel Izquierdo Macián, MD, Hospital Universitari La Fe, Valencia; Mª Mar Montejo Vicente, MD, and Raquel Izquierdo Caballero, MD, Hospital Universitario Río Hortega, Valladolid; Mª Mercedes Martínez, MD, and Aintzane Euba, MD, Hospital de Txagorritxu, Vitoria-Gasteiz; Amaya Rodríguez Serna, MD, and Juan María López de Heredia Goya, MD, Hospital de Cruces, Baracaldo; Alberto Pérez Legorburu, MD, and Ana Gutiérrez Amorós, MD, Hospital Universitario de Basurto, Bilbao; Víctor Manuel Marugán Isabel, MD, and Natalio Hernández González, MD, Hospital Virgen De La Concha - Complejo Asistencial De Zamora, Zamora; Segundo Rite Gracia, MD, Hospital Miguel Servet, Zaragoza; Mª Purificación Ventura Faci, MD, and Mª Pilar Samper Villagrasa, MD, Hospital Clínico Universitario Lozano Blesa, Zaragoza. SNQ (Swedish Neonatal Quality Register): Jiri Kofron, MD, Södra Älvsborgs Sjukhus, Borås; Katarina Strand Brodd, MD, Mälarsjukhuset, Eskilstuna; Andreas Odlind, MD, Falu Lasarett, Falun; Lars Alberg, MD, Gällivare Sjukhus, Gällivare; Sofia Arwehed, MD, Gävle Sjukhus, Gävle; Ola Hafström, MD, SU/Östra, Göteborg; Anna Kasemo, MD, Länssjukhuset, Halmstad; Karin Nederman, MD, Helsingborgs Lasarett, Helsingborg; Lars Åhman, MD, Hudiksvalls Sjukhus, Hudiksvall; Fredrik Ingemarsson, MD, Länssjukhuset Ryhov, Jönköping; Henrik Petersson, MD, Länssjukhuset, Kalmar; Pernilla Thurn, MD, Blekingesjukhuset, Karlskrona; Eva Albinsson, MD, Centralsjukhuset, Karlstad; Bo Selander, MD, Centralsjukhuset, Kristianstad; Thomas Abrahamsson, MD, Universitetssjukhuset, Linköping; Ingela Heimdahl, MD, Sunderby sjukhus, Luleå; Kristbjorg Sveinsdottir, MD, Skånes Universitetssjukhus, Malmö/Lund; Erik Wejryd, MD, Vrinnevisjukhuset, Norrköping; Anna Hedlund, MD, Skellefteå Lasarett, Skellefteå; Maria Katarina Söderberg, MD, Kärnsjukhuset Skaraborg, Skövde; Boubou Hallberg, MD, Karolinska Sjukhuset, Stockholm; Thomas Brune, MD, Södersjuhuset, Stockholm; Jens Bäckström, MD, Länssjukhuset, Sundsvall; Johan Robinson, MD*, Norra Älvsborgs Länssjukhus, Trollhättan; Aijaz Farooqi, MD, Norrlands Universitetssjukhus, Umeå; Erik Normann, MD, Akademiska Barnsjukhuset, Uppsala; Magnus Fredriksson, MD, Visby Lasarett, Visby; Anders Palm, MD, Västerviks Sjukhus, Västervik; Urban Rosenqvist, MD, Centrallasarettet, Västerås; Bengt Walde, MD, Centrallasarettet, Växjö; Cecilia Hagman, MD, Lasarettet, Ystad; Andreas Ohlin, MD, Universitetssjukhuset, Örebro; Rein Florell, MD, Örnsköldsviks Sjukhus, Örnsköldsvik; Agneta Smedsaas-Löfvenberg, MD, Östersunds Sjukhus, Östersund. *(To honor Dr. Robinson's work, this paper is published posthumously under his name.). SwissNeoNet (Switzerland Neonatal Network): Philipp Meyer, MD, and Claudia Anderegg, MD, Cantonal Hospital, Children's Clinic, Aarau; Sven Schulzke, MD, University Children's Hospital, Basel; Mathias Nelle, MD, University Hospital, Berne; Bendicht Wagner, MD, University Hospital, Berne; Thomas Riedel, MD, Children's Hospital, Chur; Grégoire Kaczala, MD, Cantonal Hospital, Fribourg; Riccardo E. Pfister, MD, University Hospital (HUG), Geneva; Jean-François Tolsa, MD, and Matthias Roth, MD, University Hospital (CHUV), Lausanne; Martin Stocker, MD, Children's Hospital, Lucerne; Bernhard Laubscher, MD, Cantonal Hospital, Neuchatel; Andreas Malzacher, MD, Cantonal Hospital, St. Gallen; John P. Micallef, MD, Children's Hospital, St. Gallen; Lukas Hegi, MD, Cantonal Hospital, Winterthur; Dirk Bassler, MD, and Romaine Arlettaz, MD, University Hospital (USZ), Zurich; Vera Bernet, MD, University Children's Hospital, Zurich. Tuscan NN (TIN Toscane on-line Network, Italy): Carlo Dani, MD, Careggi University Hospital, Florence, Italy; Patrizio Fiorini, MD, Anna Meyer Children’s University Hospital, Florence, Italy; Paolo Ghirri, MD, University Hospital of Pisa, Pisa, Italy; Barbara Tomasini, MD, University Hospital of Siena, Siena, Italy; Franca Rusconi, MD, Anna Meyer Children’s University Hospital and Regional Health Agency, Florence, Italy.
Contributors MA, DB and PSS conceptualised and designed the study and interpreted the data and wrote first draft and prepared final draft. JY performed the statistical evaluations. MA drafted the first manuscript. BAD, KL, BR, SH, MN, SKL, KKH, LL, LSF, MV, MM and MB critically reviewed the study protocol. All authors reviewed, discussed and approved the final manuscript as submitted and agree to be accountable for all aspects of the work. Author Access to Data: PSS and JY had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis.
Funding Funding for iNeo has been provided by a Canadian Institutes of Health Research Chair in Reproductive and Child Health Services and Policy Research (APR-126340) held by PSS. The Australian and New Zealand Neonatal Network is predominantly funded by membership contributions from participating centres. The Canadian Neonatal Network is supported by a team grant from the Canadian Institutes of Health Research (CTP 87518), the Ontario Ministry of Health and individual participating centres. The Finnish Medical Birth Register is governmentally funded and kept by the National Institute for Health and Welfare (THL). The Israel Neonatal Network very low birth weight infant database is partially funded by the Israel Center for Disease Control and the Ministry of Health. The Neonatal Research Network of Japan is partly funded by a Health Labour Sciences Research Grant from the Ministry of Health, Labour and Welfare of Japan. SEN1500 is supported by funds from the Spanish Neonatal Society (SENeo). The Swedish Neonatal Quality Register is funded by the Swedish Government (Ministry of Health and Social Affairs) and the body of regional health care providers (County Councils). SwissNeoNet is partially funded by participating units in the form of membership fees. Tuscany Neonatal Network is funded by the Tuscany Region. The United Kingdom Neonatal Collaborative receives no core funding.
Competing interests MA receives a salary as network coordinator for the Swiss Neonatal Network.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.