Article Text

Abstract
Purpose Women who experience gestational diabetes mellitus (GDM) are at exceptionally high-risk of developing type 2 diabetes (T2DM) later in life. However, limited information is available about genetic and environmental factors that are implicated in the progression from GDM to T2DM.
Participants The Diabetes & Women’s Health (DWH) Study applied a hybrid design, which combined new prospective data collection with existing data in two prospective cohorts, the Danish National Birth Cohort (DNBC) and the Nurses’ Health Study II (NHS II). In total, the DWH Study identified 7759 women with a GDM diagnosis from both cohorts; 4457 women participated in the DWH Study data collection, which included two cycles of follow-up from 2012 to 2014 and 2014 to 2016.
Findings to date Progression from GDM to T2DM was high. In the NHS II group, by 2013, 23.1% (n=846/3667) developed T2DM. In the DNBC group, at cycle 1 (2012–2014), the progression rate was even higher: 27.2% (n=215/790) had developed T2DM. Furthermore, we have shown that women who had GDM experienced a significantly greater risk of hypertension and cardiovascular diseases, as well as early stages of glomerular hyperfiltration and renal damage. Moreover, the DWH Study findings have shown that healthful diet and lifestyle factors and weight control were related to a lower risk of T2DM, hypertension and cardiovascular diseases.
Future plans Primary data collection for the DWH Study is complete and investigators are currently investigating interactions of the abovementioned modifiable factors with T2DM genetic susceptibility in determining the risk of progression from GDM to T2DM. Findings from ongoing work will provide further insights for identifying more precise prevention strategies for T2DM and comorbidities in this high-risk population. Future work will examine novel biomarkers of health and disease in this cohort.
- gestational diabetes
- epidemiology
- diabetes in pregnancy
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The Diabetes & Women’s Health Study covered two independent populations in the USA and Denmark, which allows for replication of findings.
Women in both cohorts were followed up for a long time after gestational diabetes index pregnancy, for over 9 years in Denmark and 23 years in the USA, which allowed time for development of type 2 diabetes and comorbidities.
Multiple types of biospecimens and comprehensive data on women’s pregnancy history, diet, lifestyle, anthropometrics, family medical history, participants’ current general health and health in childhood, health of the participants’ male partner and health of the participants’ children were collected.
The study population is relatively homogenous, which is critical for enhancing data collection quality, reducing confounding by socio-economic status and minimising bias due to population stratification in gene-environment interaction studies.
The majority of participants were Caucasians and thus findings may not be generalisable to other racial and ethnic groups.
Introduction
Type 2 diabetes mellitus (T2DM) has become a global epidemic, with over 29 million individuals in the USA and 415 million worldwide affected.1 The health consequences of diabetes are far reaching. By the time T2DM is diagnosed, diabetes-related metabolic abnormalities frequently have begun to damage the heart, kidney and nerves.2 After diagnosis, further complications can result from poor glucose control including cardiovascular disease, blindness and kidney failure.3 T2DM has become the sixth leading cause of disability4 and accounts for almost 4% of all deaths in the USA.5 Hence, prevention and early identification of individuals at high-risk for T2DM are critical.
Gestational diabetes mellitus (GDM) is a common metabolic complication affecting approximately 5%–9% of US pregnancies6 and 2%–25% of pregnancies worldwide, depending on the diagnostic criteria and the race-ethnic background of the population.7 Pregnancy may be considered as a ‘stress test’ that can reveal women at high-risk for developing future cardiometabolic complications through the manifestation of GDM.8 It is estimated that 30%–70% of women with a history of GDM will develop T2DM within 15 years of having GDM.9–11 Even among low-risk women of normal weight, a history of GDM was related to more than a 6-fold increased risk of developing T2DM later in life.12 Thus, women with GDM may offer a unique opportunity to investigate early prevention strategies for T2DM. However, thus far, limited information is available about genetic and environmental factors that are implicated in the progression from GDM to T2DM, which may help to develop more targeted personalised interventions.
To address the above critical data gaps, the Diabetes & Women’s Health (DWH) Study was conducted to investigate the long-term health consequences of GDM and their determinants.13 The primary aim was to identify genomic and environmental determinants underlying the development of T2DM and comorbidities among women with a history of GDM. This study also offers a unique opportunity to investigate the early pathophysiology involved in the progression from GDM to T2DM to understand why some women develop T2DM and comorbidities and others do not.13 The DWH Study includes two cycles of new prospective data collected from women with a history of GDM in both the USA and Denmark.
Cohort description
Study overview
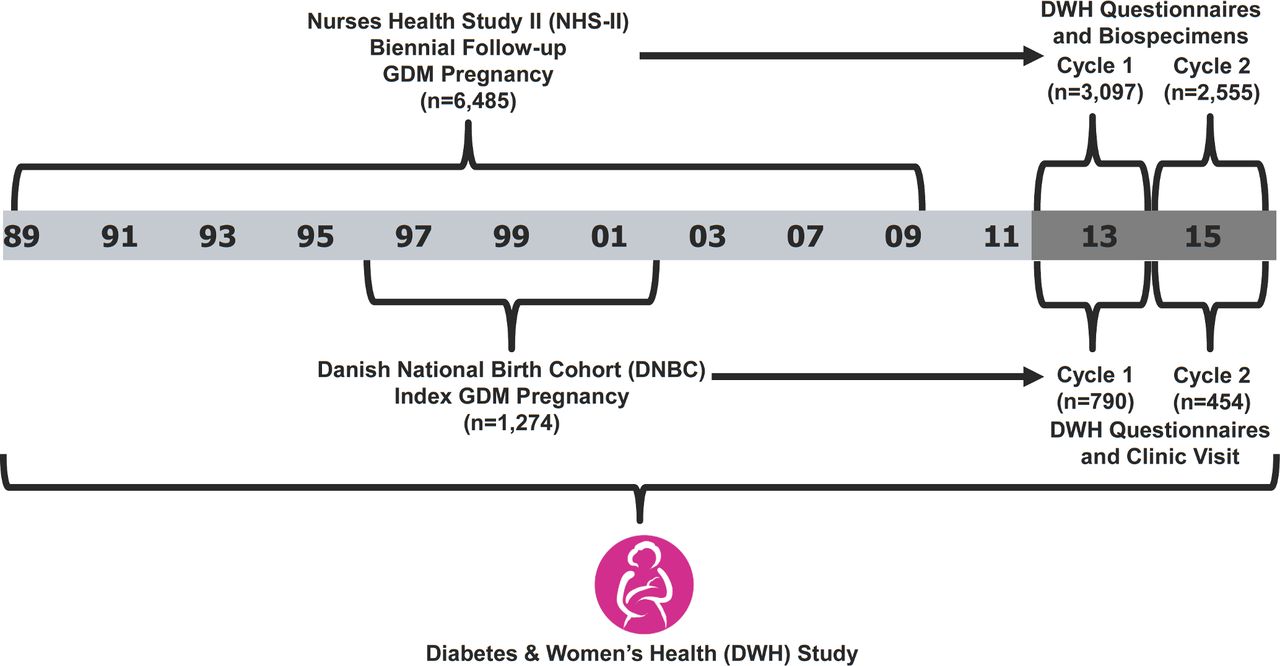
The DWH Study applied a hybrid design which combined new prospective data collection with existing data in two ongoing cohorts, the Danish National Birth Cohort (DNBC) and the Nurses’ Health Study II (NHS II). The source population of the DWH Study included 7759 women with a GDM diagnosis from both cohorts. New prospective data collection of the DWH Study included two cycles of follow-up; cycle 1 data were collected from 2012 to 2014 and cycle 2 data were collected from 2014 to 2016. A schematic of the DWH Study follow-up in the context of the original data collections that took place for the NHS II and DNBC is shown in figure 1. Whenever possible, efforts were made to harmonise the data collected in the two cohorts. For example, comparable questionnaires were administered and the same biospecimen collection and processing materials were used and standardised protocols were used for the biospecimen processing.
{kind=link}
Schematic of data collection in the Diabetes & Women’s Health (DWH) Study. The DWH Study applied a hybrid design by combining new prospective data collection across two follow-up DWH cycles (2012–2016) with existing data longitudinally collected in the Nurses Health Study II (NHS II) and the Danish National Birth Cohort (DNBC) among women with gestational diabetes (GDM).
Study population
Nurses’ Health Study II
The eligible source population of the DWH Study from NHS II was women who developed GDM at any time through 2009 and were alive in 2011 (n=6485). The NHS II is an ongoing prospective US cohort study, which in 1989 enrolled 116 430 female-registered nurses free of cancer and 25–42 years of age.14 Every 2 years NHS II participants complete questionnaires updating their health status and lifestyle factors. Women with GDM in NHS II were identified through the main biennial NHS II questionnaires up to 2001 or the 2009 pregnancy questionnaire, which inquired about the physician’s diagnoses of GDM and other conditions in all previous pregnancies. Self-reported GDM among NHS II participants was previously validated using medical records with confirmation among 94% of cases.15
Women from NHS II with an email address on file were invited to participate in the DWH Study; follow-up emails and phone calls were provided to non-responders. Women could choose to complete the questionnaire via a secure website or request a scannable paper form. Women who did not respond via email, or those for whom no email address was available, were sent a paper questionnaire. In total 3667 (56.6%) women participated in at least one data collection cycle; specifically, cycle 1 and 2 included 3097 and 2555 women, respectively. Baseline characteristics of the enrolled sample at the NHS II enrolment in 1989 are shown in table 1. Characteristics of women who participated in the DWH Study were largely comparable with the eligible sample (online supplementary table 1).
Supplementary file 1
Baseline characteristics of women enrolled in the Diabetes & Women’s Health Study: The Nurses’ Health Study II site (baseline in 1989) (n=3667)
In cycle 1, NHS II participants were asked to complete a questionnaire and provide biospecimens. In cycle 2, women who did not enrol in cycle 1 were re-contacted and asked to complete a shorter questionnaire and, if desired, provide biospecimens. Women who enrolled in cycle 1 and re-enrolled in cycle 2 were provided a new questionnaire and asked to also provide biospecimens.
Danish National Birth Cohort
The eligible source population for the DWH Study from the DNBC was women who developed GDM during any of their pregnancies recorded in the DNBC and for whom medical record review confirmed that they did not have prepregnancy diabetes (n=1274). The DNBC is a prospective cohort study which enrolled 91 827 pregnant Danish women between 1996 and 2002.16 DNBC participants completed questionnaires throughout pregnancy and post partum. Details on identification of GDM in DNBC have been previously described.17 Briefly, women with GDM were identified either through the Danish National Patient Register or through DNBC telephone interviews at 30 weeks of gestation or 6 months post partum. Validation using hospital records revealed a high sensitivity (96%) for GDM diagnosis, but a low positive predictive value (59%).17 For that reason, women were classified into two GDM categories: verified or suspected. The suspected GDM group included women who met the criteria for GDM based on the interview or self-report or from the register, but medical record confirmation was not available. Sensitivity analyses can leverage this distinction to examine for differences across these two groups, which may be a possible indicator of GDM severity.
Women who did not respond to the DWH Study invitation letter within 2 weeks were contacted via telephone. Women who did not wish to complete a clinical exam were invited to complete the study questionnaire online. A total of 790 women agreed to participate in cycle 1 of the DWH Study; the majority completed a clinic visit (n=607; 76.8%). Cycle 2 included 454 women, all of whom had participated in cycle 1; the majority completed a clinic visit (n=371; 81.7%).
Baseline characteristics of the enrolled sample at the DNBC index pregnancy are shown in table 2. Characteristics of women who participated in DWH Study were largely comparable with the eligible sample (online supplementary table 2).
Baseline characteristics of women enrolled in the Diabetes & Women’s Health Study: The Danish National Birth Cohort (DNBC) site (1996–2002) (n=790)
Patient and public involvement
Neither the study participants nor the public were involved in setting the research questions or the outcome measures, study design, recruitment or conduct of the study. There are no plans to involve patients in dissemination.
Data collection and measures
Historical data
DWH data from the historical data collections of the NHS II (biennial questionnaires) and DNBC will be combined with the new data collected in the DWH Study. Historical data from NHS II and DNBC relevant to the DWH Study aims are listed in online supplementary appendix 1.
New prospective data
Questionnaire data
Collection of new data at the DWH Study follow-up through study questionnaires (online or paper) included the following domains: pregnancy history, first GDM pregnancy, diet, lifestyle, anthropometrics, family medical history, participants’ current general health and health in childhood, health of the participants’ male partner and health of the participants’ children. Details of the domains at each cycle are available in online supplementary appendix 2. Data quality assurance was performed on online questionnaires by using normal ranges on all numeric fields and implementing logic checks establishing parent-child relationships between questions and on scanned paper questionnaire by performing manual visual inspection of the original form and implementing data cleaning rules, which followed the logic checks based on parent-child relationships between questions and biologically plausible values.
Clinical examination and biospecimens
Biospecimen collection for study participants from NHS II was conducted via a mailed kit. Detailed and standardised instructions for drawing blood samples after fasting for 8–10 hours at home, at work or by a phlebotomist was included in the kit. In cycle 1, blood (total 25 mL including PAXgene tubes for RNA), first morning urine and toenails were collected. Two types of biospecimen collection kits were used in cycle 2. Women who returned biospecimens in cycle 1 were sent a full kit for the collection of blood (20 mL), first morning urine and fasting saliva. Women who only returned questionnaires in cycle 1, but no biospecimens, were sent an abbreviated kit for the collection of dried blood spots, first morning urine and fasting saliva. Samples were shipped overnight to a central laboratory where blood was processed according to standardised procedures and temporarily stored at −80℃ until shipment to the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) repository for permanent storage at −80℃. When necessary, biospecimens available from historical collection of the NHS II may be used as well.
The DWH Study follow-up clinical exam for participants from the DNBC consisted of biospecimen collection, oral glucose tolerance test (OGTT), anthropometric measurements (height, weight, waist and hip), measures of blood pressure and resting heart rate and a dual-energy X-ray absorptiometry scan for body composition and bone mineral density. The first blood draw at the clinical exam (total 41 mL including PAXgene tubes for RNA) was an 8–10 hour fasting draw after which women drank a 75 g glucose solution for an OGTT. The second blood draw (12 mL) was completed after 120 min. The samples were processed according to standardised procedures in the clinic or analysed for the OGTT and complete blood count. Women provided the first morning urine sample. Additionally, toenails were collected in cycle 1 and fasting saliva in cycle 2. Biospecimens were temporarily stored at −80℃ until shipment to the NICHD repository for permanent storage at −80℃.
Findings to date
Progression from gestational diabetes to type 2 diabetes and comorbidities
In this high-risk population, the progression rate to T2DM was high. Among GDM women in NHS II who participated the DWH Study new data collection, by 2013, 846 of 3667 women (23.1%) had developed T2DM (table 3). In the DNBC group, at cycle 1 (2012–2014), 215 of 790 women (27.2%) had developed T2DM (table 4); in the subset of women with medically verified GDM, 170 of 487 (34.9%) had developed T2DM. A small number of women from the DNBC developed type 1 diabetes after GDM (n=22, 2.8%), which is consistent with the high risk for late development of type 1 diabetes mellitus in the Danish population.11 18 We have also extended our research beyond T2DM where we have observed that the NHS II participants of the DWH Study also had an increased risk of hypertension and cardiovascular diseases as well as T2DM.19 20 Furthermore, among Danish participants GDM was a risk factor for early stages of glomerular hyperfiltration and renal damage.21 Future work will include other comorbidities such as autoimmune disorders, obstructive sleep apnea and liver function and fat.
Characteristics of women at cycle 1 (2012–2014) of the Diabetes & Women’s Health Study: The Nurses’ Health Study II (NHS II) site (n=3667)
Characteristics of women at cycle 1 (2012–2014) of the Diabetes & Women’s Health Study: The Danish National Birth Cohort site (n=790)
Risk factors for the progression from gestational diabetes to type 2 diabetes and comorbidities
DWH Study findings published to date have shown that healthful diet and lifestyle factors and weight control are related to lower risk progression from GDM to T2DM, hypertension and cardiovascular diseases. Specifically, analyses among the NHS II participants of the DWH Study have examined major risk factors such as healthful dietary patterns, improvement in physical activity and weight control and their association with T2DM12 22–25 and hypertension,26 among women with a history of GDM. For example, adherence to a Dietary Approaches to Stop Hypertension) or alternate Healthy Eating Index dietary pattern was associated with a 15%–35% lower risk of developing T2DM among women with a history of GDM.22 Similar findings were also observed for these dietary patterns and risk of hypertension.26 On the other hand, a low-carbohydrate dietary pattern, with high protein and fat intake mainly from animal-source foods, was associated with a 40% higher T2DM risk.24 Increasing physical activity was associated with a lower risk for T2DM.23 These findings on diet and physical activity were independent of body mass index , suggesting these factors may contribute to T2DM beyond effects on body weight, which is a strong risk factor for the development of T2DM.12 However, weight control appears to be the most effective way to reduce T2DM risk among women with GDM as women with obesity at baseline who gained ≥5 kg after having GDM had a 43-times higher risk of developing T2DM compared with women with normal weight at baseline and who gained <5 kg after having GDM.12 Taken together, these findings suggest an encouraging and hopeful message to women with a history of GDM. Although they are at exceptionally high risk for T2DM and hypertension, promoting a healthful diet and active lifestyle and maintaining a healthy weight may substantially lower their risk. These findings encourage future intervention studies on promoting healthful diet, lifestyle and weight to prevent T2DM and comorbidities among these women at high risk. Nonetheless, it should be noted that effective prevention will require screening women at high risk to implement these lifestyle changes, but studies have shown that postpartum screening for T2DM is low even among women with a history of GDM.27
The DWH Study investigators are currently investigating interactions of the above mentioned modifiable factors with T2DM genetic susceptibility in determining the risk of progression from GDM to T2DM and are developing a risk prediction model for T2DM among these high-risk women. Findings from ongoing work will provide further insights in identifying more precise prevention strategies for T2DM and comorbidities in this high-risk population.
Strengths and limitations
One of the unique features of the DWH Study is the availability of detailed longitudinal follow-up data over many years after index pregnancy complicated by GDM. This study combined data from before and/or during the GDM pregnancy with long-term follow-up, which included questionnaire data, biospecimen collections and clinical exams (Danish site). Moreover, for eligible women whose biospecimen is not available from the new collection in the DWH Study, their biospecimen from the historical collection may be available for addressing DWH Study questions. Furthermore, the study covered two independent populations which allows for replication of findings. It is also important to consider the differences in the underlying populations between the NHS II women in the USA and the DNBC women in Denmark. Although the GDM screening and diagnosis criteria differed between the two groups, identification of GDM events in both cohorts (based on medical records review) was demonstrated to be valid.15 17 Furthermore, women in both cohorts were followed up for a long time after the index pregnancy, with over 9 years in Denmark and 23 years in the USA, which allowed time for development of T2DM and comorbidities.
A limitation of the DWH Study, because the majority of participants were Caucasians, is that the findings may not be generalisable to other racial and ethnic groups. However, the relative homogeneity of the study population is critical for enhancing data collection quality, reducing confounding by socio-economic status and minimising bias due to population stratification in gene-environment interaction studies. Second, universal screening of GDM was not applied in Denmark during the years in which data for the DNBC were collected and the DNBC population had a relatively higher socio-economic status than Danish women as a whole; thus, the prevalence of GDM is lower than reported in other European countries. Last, the diagnosis criteria and screening strategy differed between the two cohorts. However, identification of GDM events in both cohorts was demonstrated to be valid (based on medical records review).15 17 Regardless of the exact criteria, diagnosis of GDM indicates these women had a degree of glucose intolerance during pregnancy, and as such, represent a high-risk population for T2DM and comorbidities later in their lives. It should also be noted that, currently, there is no consensus on optimal GDM diagnosis criteria worldwide. Inclusion of two independent populations in the study offers a unique opportunity of replicating/confirming findings from one population in the other. Whenever applicable, we will also pool findings from the two populations based on a meta-analysis approach.
References
Footnotes
Contributors CZ conceived of the study. CZ contributed to the conception of the research questions and funding application. CZ, EHY, WB, KB, AL, JLM, SFO, REG-L, SS, AV, LGG, SH, AJG, SHL, CMM, JEC and FBH contributed to the conception of the protocol. SNH and CZ drafted the manuscript. REG-L, SS, AV, LGG, SH, AJG, SHL, CMM, JEC and FBH assisted with data collection. All authors provided comments on the manuscript draft and agreed on the final submitted version.
Funding The Diabetes & Women’s Health Study was supported by the Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development at the National Institutes of Health [contract numbers: HHSN275201000020C HHSN275201500003C, HHSN275201300026I, HHSN275201100002I]. The Nurses’ Health Study II cohort is supported by the National Institutes of Health [grant number UM1 CA176726]. The Danish National Birth Cohort is supported by the March of Dimes Birth Defects Foundation [6-FY-96-0240, 6- FY97-0553, 6-FY97-0521, 6-FY00-407]; Innovation Fund Denmark [grant number 09-067124, ‘Centre for Fetal Programming’]; Danish Council for Independent Research [grant number 9601842 and 22-03- 0536]; the Health Foundation [11/263-96]; and the Heart Foundation [96-2-4-83-22450].
Competing interests AV is employed by AstraZeneca; all other authors declare no competing interests.
Ethics approval All women provided written informed consent. The Danish National Birth Cohort component was approved by the Regional Scientific Ethical Committee of the Capital Region of Denmark (record no. H- 4-2013-129). The Nurses’ Health Study II component study protocols were approved by the institutional review boards of Brigham and Women’s Hospital, the Harvard T.H. Chan School of Public Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data, along with a set of guidelines for researchers applying for the data, will be posted to a data-sharing site: NICHD/Division of Intramural Population Health Research (DIPHR) Biospecimen Repository Access and Data Sharing (BRADS) (https://brads.nichd.nih.gov). All requests for data must include a short protocol with a specific research question and a plan for analysis. The DWH Study governance will be followed and individuals using DWH Study data must agree to all data use and sharing procedures at each of the relevant institutions participating in the DWH Study.
Collaborators The DWH study team welcomes collaboration. Newly collected DWH Study data will be made accessible in documented repositories and electronic archives after completion of the studies’ analytic phase. The data, along with a set of guidelines for researchers applying for the data, will be posted to a data-sharing site: NICHD/Division of Intramural Population Health Research (DIPHR) Biospecimen Repository Access and Data Sharing (BRADS) (https://brads.nichd.nih.gov). All requests for data must include a short protocol with a specific research question and a plan for analysis. The DWH Study governance will be followed and individuals using DWH Study data must agree to all data use and sharing procedures at each of the relevant institutions participating in the DWH Study.
Patient consent for publication Obtained.