Article Text

Abstract
Objective To systematically review the effect of oral intake of bacterial probiotics on 15 variables related to obesity, diabetes and non-alcoholic fatty liver disease.
Design Systematic review and meta-analysis.
Data sources Medline, EMBASE and COCHRANE from 1990 to June 2018.
Eligibility criteria Randomised controlled trials (≥14 days) excluding hypercholesterolaemia, alcoholic liver disease, polycystic ovary syndrome and children <3 years.
Results One hundred and five articles met inclusion criteria, representing 6826 subjects. In overweight but not obese subjects, probiotics induced improvements in: body weight (k=25 trials, d=−0.94 kg mean difference, 95% CI −1.17 to −0.70, I²=0.0%), body mass index (k=32, d=−0.55 kg/m², 95% CI −0.86 to −0.23, I²=91.9%), waist circumference (k=13, d=−1.31 cm, 95% CI −1.79 to −0.83, I²=14.5%), body fat mass (k=11, d=−0.96 kg, 95% CI −1.21 to −0.71, I²=0.0%) and visceral adipose tissue mass (k=5, d=−6.30 cm², 95% CI −9.05 to −3.56, I²=0.0%). In type 2 diabetics, probiotics reduced fasting glucose (k=19, d=−0.66 mmol/L, 95% CI −1.00 to −0.31, I²=27.7%), glycated haemoglobin (k=13, d=−0.28 pp, 95% CI −0.46 to −0.11, I²=54.1%), insulin (k=13, d=−1.66 mU/L, 95% CI −2.70 to −0.61, I²=37.8%) and homeostatic model of insulin resistance (k=10, d=−1.05 pp, 95% CI −1.48 to −0.61, I²=18.2%). In subjects with fatty liver diseases, probiotics reduced alanine (k=12, d=−10.2 U/L, 95% CI −14.3 to −6.0, I²=93.50%) and aspartate aminotransferases (k=10, d=−9.9 U/L, 95% CI −14.1 to -5.8, I²=96.1%). These improvements were mostly observed with bifidobacteria (Bifidobacterium breve, B. longum), Streptococcus salivarius subsp. thermophilus and lactobacilli (Lactobacillus acidophilus, L. casei, L. delbrueckii) containing mixtures and influenced by trials conducted in one country.
Conclusions The intake of probiotics resulted in minor but consistent improvements in several metabolic risk factors in subjects with metabolic diseases.
Trial registration number CRD42016033273.
- obesity
- diabetes
- non-alcoholic fatty liver disease
- probiotics
- bifidobacterium
- lactobacillus
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We underscored food grade bacterial probiotics’ inherent effects, analysed a large panel of variables and performed subgroup explorations analysis to detect a disease stage severity dependence.
We performed, for the first time, subgroup explorations to detect bacterial species contribution.
We integrated both exploratory and secondary outcomes, 43 trials conducted in one country, trials with small sample size, heterogeneous study populations, incomplete information on drug treatment, dietary and physical activity records.
For some trials, parameters necessary for the estimation of effect sizes were unknown and we had to base our calculations on assumptions that could be only in part derived from the data at hand.
Introduction
The high prevalence of obesity, diabetes and non-alcoholic fatty liver disease (NAFLD) is a global health problem resulting in considerable healthcare costs. Lifestyle changes are regarded as cornerstones in the management of these tightly linked disorders that progress over an individual’s lifetime.
The rapid progression of these diseases is linked to changes in a myriad of environmental factors interacting with genetic and epigenetic factors. The gut microbiota is a key player at the interface between environmental changes and host biology. Metabolic traits, such as obesity, diabetes and non-alcoholic steatohepatitis are associated with changes in gut microbiota diversity and composition.1 2 Gut microbiota profile is also associated with specific dietary patterns3 and respond to dietary4 5 and therapeutic interventions.6 However, until recently, causal roles of the gut microbiota in the development and maintenance of chronic metabolic disorders is suggested mainly based on findings in rodents.7
Probiotics are defined as ‘live microorganisms that, when administered in adequate amounts, confer a health benefit on the host’.8 In rodents, numerous studies have shown beneficial effects of probiotics on energy, glucose and lipid metabolism,9 although not consistently.10 In humans, the number of studies with probiotics nearly doubled over the last 2 years. Several meta-analyses evaluated the impact of probiotics on metabolic variables11–17 but explorations to detect a disease stage severity dependence are scarce. Furthermore, no meta-analysis evaluated the contribution of bacteria used in foods that are listed as biological agents under European Food Safety Authority qualified presumption of safety list and none examined the specific contribution of bacterial species.18
We thus conducted a systematic review and meta-analysis aiming to investigate the impact of probiotics on 15 variables related to obesity, diabetes and NAFLD. We investigated multiple outcomes, many of which are inter-related so that concomitant effects would corroborate consistent probiotics effects. We aimed at elucidating whether there is an overall effect of probiotics on metabolic impairments and, if so, under which conditions the effect occurs. These goals were pursued by investigating the following questions: (1) What is the effect of probiotics on different outcomes related to obesity, metabolic syndrome, diabetes and NAFLD? (2) Is there effect heterogeneity by gender? (3) Is there effect heterogeneity in the following study populations: normal weight (NW), overweight (OW), obese (OB), metabolic syndrome, impaired fasting glucose (IFG), type 2 diabetes (T2DM), gestational diabetes, NAFLD? (4) Is there effect heterogeneity by total daily dose, food form and probiotics species (or combination of them)?
Methods
The search strategy, eligibility criteria and outcomes were described a priori (PROSPERO CRD42016033273).
Data sources
We searched PUBMED/MEDLINE, EMBASE and the COCHRANE CENTRAL library for eligible articles published in English, French, German, Spanish or Portuguese between January 1990 and June 2018. We also searched the reference list of the identified papers.
Study selection
We included human intervention studies that fulfilled the following inclusion criteria: (1) randomised controlled trials (parallel or cross-over), (2) published since 1990, (3) treatment duration of at least 14 days (at which some metabolic effect may occur, yet the short duration may reduce a chance to detect an effect), (4) use of probiotics (following genera: Bifidobacterium, Lactobacillus, Lactococcus, Leuconostoc, Oenococcus, Pediococcus, Propionibacterium and Streptococcus) as key independent variables and (5) reported data on at least one difference between baseline and end of intervention related to the metabolic impairment using search terms: obese/-ity, diabetic/-es, weight, metabolic syndrome, glucose intolerant, glucose tolerant, glucose tolerance, glucose intolerance, insulin resistance, insulin sensitivity, impaired fasting glucose, waist circumference, abdominal adiposity, abdominal obesity, central obesity, visceral adipose tissue, visceral fat, visceral adiposity, fat, fatty liver, non-alcoholic fatty liver and irrespective of whether the investigators considered the outcome as primary or secondary criteria (see online supplementary file).
Supplementary file 1
The outcomes were body weight (BW), body mass index (BMI), waist circumference (WC), body fat mass (BFM) (determined using bioelectrical impedance or dual energy X-ray absorptiometry), subcutaneous adipose tissue mass (SAT), visceral adipose tissue mass (VAT), fasting glucose (FG), glycated haemoglobin (HbA1c), insulin (INS), homeostatic model of insulin resistance (HOMA-IR), C-reactive protein (CRP), triglycerides (TG), alanine aminotransferase (ALAT), aspartate aminotransferase (ASAT) and gamma-glutamyl transferase (GGT). We excluded studies that administered probiotics with other functional ingredients with the exception of fermentable fibres at a maximum dose of 1.5 g/day. Fructo-oligosaccharides improve probiotics’ survival in the gastrointestinal system19; however, we assumed that three times a day intake of 0.5 g would be insufficient to exert a significant prebiotic effect. Subjects who had isolated hypercholesterolaemia, alcoholic liver disease, polycystic ovary syndrome and children with an age of <3 years were excluded. Three authors (BG, HK, MMS) independently performed the study selection and any disagreement was resolved on a discussion with a fourth author (JS or JMF).
Data extraction
Two reviewers independently extracted data from the original publications: [author, year of publication, country of origin, design of the trial, experimental intervention (type of bacterial species and, if given, subspecies), dose, food form and duration of intervention, comparator/control, characteristics of the population (descriptive statistics of age, sex and BMI), medication for T2DM, descriptive statistics for each outcome (mean/median, SD/SE, CI, etc before and after the intervention)]. We extracted data and calculated the mean and SE for each outcome and time point using standardised units (see online supplementary file). If provided, we extracted statistics quantifying the absolute change postintervention versus preintervention and/or the results of a hypothesis test investigating the statistical significance of this change.
Risk of bias (quality) assessment
We calculated a quality score based on 10 factors, according to a standardised procedure (PEDro tool based on the Delphi list) and classified studies as high quality (≥8 points), moderate quality (>6 and <8 points) or low quality (≤6 points).
Calculation of effect measures
As effect measures, we considered the mean difference in absolute change from baseline between the probiotics and control groups. For studies with more than two measurements during the follow-up, we calculated the change between the last preintervention measurement and the measurement at the end of the administration period. Missing SE for the difference between interventions for change-from-baseline parameter were estimated using the formula recommended in the Cochrane handbook based on an assumption of the magnitude of correlation among the repeated outcome measurements (intrasubject correlation). Since studies did not explicitly report coefficients of intrasubject correlation, we assumed for all outcomes an intermediate magnitude of intrasubject coefficient of 0.5. We conducted sensitivity analyses to examine the robustness of the meta-analysis results with respect to this assumption by varying the intrasubject correlation within realistic ranges (details see below).
Data synthesis
We calculated summary meta-analysis estimates for the difference between probiotic and control, including 95% CI and p values, by using the random effects method (DerSimonian-Laird estimator20) that allows for heterogeneity in results between studies. There was within publication and within study dependence structure because some authors reported multiple randomised trial results investigating different outcomes in the same study population within the same paper. However, because we aimed to synthesise outcomes separately and as separate research questions, we did not adjust our estimates for this multiplicity.
Assessment of study heterogeneity
We examined probiotic effect heterogeneity by forest plots visualising the study-specific efficacy estimates and 95% CIs as well as a χ2 heterogeneity test. To identify any dose–response relationship pattern, we plotted the study-specific efficacy estimates ordered by the total daily dose of probiotics administered. To explore whether the heterogeneity pattern is related to study-specific variables, we generated stratified forest plots grouping studies by characteristics of the intervention, food form and specific study populations. To quantify the magnitude of heterogeneity, we calculated the between study variance (τ²) and the I² statistic, that is, the percentage of variation in effect estimates attributable to heterogeneity. Further, we applied a hypothesis test for heterogeneity based on the Q χ2 statistic.21 Forest plots were grouped in different levels of heterogeneity based on the I² value: low (I²: 0%–25%), intermediate (I²: 25%–50%), moderate (I²: 50%–75%) and high (I²≥75%).
To investigate the possible source of heterogeneity, we performed sensitivity analysis restricted to studies without children, pregnant woman, subjects undergoing gastric surgery and without only one country, due to a high preponderance of the conducted studies. If feasible, depending on the heterogeneity pattern identified, we calculated the following efficacy estimates in total and for subgroups for each outcome: (1) gender; (2) study population. The treatment and placebo groups were classified as NW: 18.5≥BMI<25 kg/m², OW: 25≥BMI<30 kg/m², OB: BMI≥30 kg/m², IFG: 5.6–6.9 mmol/L, T2DM: FG ≥7.0 mmol/L or HbA1C≥6.5% and NAFLD (biopsy or ultrasound diagnosed). For study population characteristics undescribed in the original publication, we used the mean of treatment group value to assign the study population. In trials with mixed study populations, the study population would contribute to each study population specific meta-analysis. (3) Total daily dose. (4) Food forms categorised as (capsule or powder or sachet or pill) and (yoghourt or fermented milk). (5) Characteristics of probiotics interventions: species and subspecies.
Assessment of publication bias
To visually identify publication bias or other small study effects, we used funnel plots or simple scatterplots of the SE versus the study-specific effect estimates including 95% pseudo confidence limits. Potential small study effects were visualised showing the Egger’s line in the funnel plot, a line resulting from a linear regression of the effect estimates on their SE, weighing by the inverse of the variance of the intervention effect estimate. Further, we calculated a Galbraith’s radial plot showing the effect estimate divided by its SE against the precision of the effect estimate. In addition, for groups with more than 10 studies, we tested for small study effects using Egger’s test and Begg’s rank correlation test.22 23 In case of significant funnel asymmetry, we further examined the potential reasons by stratified funnel plots grouping studies by study characteristics that might relate to study size (eg, quality score, baseline value, population, etc). For outcomes with evidence of residual small study effects that could not be explained by known study-specific characteristics (eg, due to publication bias), we conducted a sensitivity analysis recalculating the summary estimates by a trim and fill algorithm.24
Sensitivity analysis
First, we conducted a sensitivity analysis aimed to assess robustness of results regarding our assumption of intrasubject correlation (r=0.5) used to impute SD of change measures. We varied intrasubject correlations within specific ranges obtained from confidence limits of correlation coefficients that were back calculated from studies that explicitly reported SDs of changes by using an approximation formula from the Cochrane handbook. Second, to evaluate the robustness of results obtained with respect to study quality, specific probiotic species or study populations, we conducted sensitivity analyses by recalculating the meta-analytic summary efficacy estimates excluding trials with low and intermediate quality score levels, or studies including the Bacillus coagulans (former Lactobacillus sporogenes) strain or studies including children, pregnant women or gastric surgery. Finally, we investigated the sensitivity of our results with respect to estimates from studies conducted in one country where we observed a high number of trials with similar design and methods and we recalculated estimates excluding those studies. All statistical hypothesis testing was conducted two-sided (p<0.05). All calculations were conducted using the software STATA (StataCorp. 2013. Stata Statistical Software: Release 15. College Station, Texas, USA: StataCorp LP).
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in the design and implementation of the study. There are no plans to involve patients in dissemination.
Results
We identified 1934 records, from which we selected 986 individual abstracts and 161 potentially relevant articles for full review (figure 1). We identified 105 articles19 25–128 reporting data from 99 different research studies including 111 different randomised comparisons of probiotics versus control (further called randomised clinical trials [RCTs], see online supplementary table 1-2) with the following outcomes: BW (number of RCTs: k=58, n=3422 individuals, median=77.4 kg), BMI (k=68, n=4015, 28.2 kg/m²), WC (k=26, n=1583, 98.8 cm); BFM (k=27, n=1562, 27.8 kg), SAT and VAT (k=5, n=543, 192.4 cm² and 114.7 cm², respectively), FG (k=83, n=5188, 6.1 mmol), HbA1c (k=28, n=1796, 6.3%), INS (k=63, n=3854, 11.0 mU/L), HOMA-IR (k=52, n=3513, 3.2), CRP (k=41, n=2376, 3.6 mg/L), TG (k=74, n=4461, 145.4 mg/dL), ALAT (k=26, n=1466, 38.6 IU/L), ASAT (k=23, n=1340, 36.1 IU/L) and GGT (k=14, n=816, 41.5 IU/L). The median duration of the follow-up was 8 weeks (range: 2–28 weeks), probiotics dose ranged from 107 to 1012 CFU daily, and 43 trials were conducted in one country (Iran). Using a PEDro tool-based quality score evaluated for each research study, 69 (70%) studies showed high quality, 15 (15%) studies showed moderate quality and 15 (15%) studies showed low quality (see online supplementary table 3).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Anthropometric variables and BMI
We first examined probiotic effects in all study populations. We observed a minor but significant mean difference in absolute changes for anthropometric parameters, BW: k=58, d=−0.39 kg (95% CI −0.57 to −0.21; I²=22.6%, median duration of the follow-up 10 weeks), BMI: k=68, d=−0.33 kg/m² (95% CI −0.53 to −0.12; I²=86.3%), WC: k=26, d=−1.01 cm (95% CI −1.55 to −0.48; I²=35.6%), BFM: k=27, d=−0.62 kg (95% CI −0.91 to −0.34; I²=16.3%), VAT: k=5, d=−6.30 cm² (95% CI −9.05 to −3.56; I²=0.0%), and SAT: k=5, d=−4.99 cm² (95% CI −7.55 to −2.44; I²=0.0%) with probiotic administration (figure 2A, see online supplementary figures 1–18). Sensitivity analysis excluding different types of trials showed that the effect estimates were robust with respect to study quality, specific study populations (children, pregnancy, gastric surgery) and conserved even when studies from Iran were excluded (see online supplementary table 4–6, supplementary figures 19–24).

Results of meta-analyses: overall estimates and estimates obtained in specific study populations: (A) anthropometric variables and BMI, (B) glucose homeostasis, (C) liver enzymes. (X-axis) Absolute difference in mean change from baseline (probiotics—control groups): random effects estimate and 95% CI; outcomes (measurement unit): ALAT, alanine aminotransferase; ALL, all studies pooled; ASAT, aspartate aminotransferase; BFM, body fat mass; BMI, body mass index; BW, body weight; FG, fasting glucose; GGT, gamma-glutamyl transferase; HbA1c, glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; IFG, impaired fasting glucose; INS, fasting insulin; NAFLD, non-alcoholic fatty liver disease; NW, normal weight; OB, obese; OW, overweight, T2DM, type 2 diabetes mellitus, WC, waist circumference.
Glucose homeostasis and systemic inflammation
We also found a significant mean difference in absolute changes for parameters related to glucose homeostasis and systemic inflammation: FG: k=83, d=−0.12 mmol (95% CI −0.18 to −0.07; I²=55.4%), HbA1c: k=28, d=−0.14 pp (95% CI −0.22 to −0.06; I²=81.3%), INS: k=63, d=−0.80 mU/L (95% CI −1.08 to −0.52, I²=72.8%), HOMA-IR: k=52, d=−0.27 pp (95% CI −0.41 to −0.12; I²=74.9%) and CRP: k=41, d=−0.48 mg/L (95% CI −0.76 to −0.21; I²=67.1%) with probiotics administration (figure 2B, see online supplementary figures 25-39). Sensitivity analysis showed that effect estimates were robust with respect to study quality and specific study populations (children, pregnancy, gastric surgery). Sensitivity analysis recalculating the meta-analysis estimates excluding all studies conducted in Iran revealed non-significant effect estimates for all these parameters (see online supplementary table 7–9, supplementary figures 40–44).
TG and liver function
We observed a significant change in TG: k=74, d=−5.40 mg/dL (95% CI −9.17 to −1.63; I²=35.9%), ALAT: k=26, d=−4.40 U/L (95% CI −7.58 to −1.22; I²=92.9%) and ASAT: k=23, d=−3.67 U/L (95% CI −7.25 to −0.09; I²=96.8%) as well as a borderline significant trend in GGT: k=14, d=−3.14 U/L (95% CI −6.60 to 0.33; I²=86.9%) with high heterogeneity (figure 2C, see online supplementary figures 45–56). Sensitivity analysis showed that effect estimates were robust with respect to study quality and specific study populations (children, pregnancy, gastric surgery). After excluding the trials from Iran, the effect estimates became non-significant (see online supplementary table 9–10, supplementary figures 57–60).
Subgroup analysis by gender
Only a small fraction of studies reported gender-specific estimates. Thus, the power to identify effect heterogeneity by gender was limited for most outcomes. The only evidence for heterogeneity of treatment effect by gender we observed was for FG, INS and HOMA-IR (effect only observed in women, not shown).
Population subgroup analysis
Subgroup analysis in different populations revealed specific effects for anthropometric variables (see online supplementary table 4–6, supplementary figures 61–71). In OW subjects, we obtained a significant mean difference in probiotics administration compared with placebo for: BW (k=25,d=−0.94 kg, 95% CI −1.17 to −0.70, I²=0.0%), BMI (k=32, d=−0.55 kg/m², 95% CI −0.86 to −0.23, I²=91.9%), WC (k=13, d=−1.31 cm, 95% CI −1.79 to −0.83, I²=26.2%), BFM (k=11, d=−0.96 kg, 95% CI −1.21 to −0.71, I²=0.0%), VAT (k=5, d=−6.30 cm², 95% CI −9.05 to −3.56, I²=0.0%) and SAT (k=5, d=−4.99 cm², 95% CI −7.55 to −2.44, I²=0.0%). In contrast, the effect estimates were smaller and non-significant in OB subjects (figure 2A).
Subgroup analysis in different populations revealed an interesting pattern for glucose homeostasis variables (see online supplementary table 7–8, supplementary figures 72–82). In subjects with impaired fasting glucose, we observed significant effects on HbA1c (k=6 including no trial from Iran, d=−0.15 pp, 95% CI −0.31 to 0.00, I²=89.7%) and INS (k=17 including five trials from Iran, d=−0.77 mU/L, 95% CI −1.01 to −0.52, I²=0.0%) (median duration of the follow-up 10 weeks). In type 2 diabetic subjects, probiotics reduced FG (k=19 including nine trials from Iran, d=−0.66 mmol/L, 95% CI −1.00 to −0.31, I²=27.7%), HbA1c (k=13 including seven trials from Iran, d=−0.28 pp, 95% CI −0.46 to −0.11, I²=54.1%), INS (k=13 including eight trials from Iran, d=−1.66 mU/L, 95% CI −2.70 to −0.61, I²=37.8%) and HOMA-IR (k=10 including six trials from Iran, d=−1.05 pp, 95% CI −1.48 to −0.61, I²=18.2%) (figure 2B). Probiotics induced improvements in INS (k=6 including four trials from Iran, d=−3.17 mU/L, 95% CI −4.88 to −1.46, I²=73 .8%) and HOMA-IR (k=6 including four trials from Iran, d=−0.71 pp, 95% CI −1.05 to −0.36, I²=66.4%) in women with gestational diabetes.
In subjects with fatty liver diseases, probiotics reduced ALAT (k=12 including eight trials from Iran, d=−10.2 U/L, 95% CI −14.3 to −6.0, I²=93.50%), ASAT (k=10 including seven trials from Iran, d=−9.9 U/L, 95% CI −14.1 to −5.8, I²=96.1%) (figure 2C, see online supplementary figures 83–84). Also, BW (k=5, d=−1.83 kg, 95% CI −3.49 to −0.17; I²=0.0%), BMI (k=11, d=−1.21 kg/m², 95% CI −2.18 to −0.24; I²=88.5%) and components of metabolic syndrome WC (k=4, d=−1.81 cm, 95% CI −3.20 to −0.43; I²=0.0%), FG (k=12 including nine trials from Iran, d=−0.30 mmol/L, 95% CI −0.52 to −0.08, I²=68.5%) and TG (k=11 including seven trials from Iran, d=−12.89 mg/dL, 95% CI −21.82 to −3.97; I²=33.2%) were reduced in subjects with fatty liver diseases (see online supplementary table 4,5,7,9). Finally, only four trials reported results in subjects with metabolic syndrome (data not shown).
Dose, food form and species subgroup analysis
Except for BMI, subgroup analysis did not reveal a dose-dependent effect. Subgroup analysis revealed no common or unique food form effect (see online supplementary table 4–10).
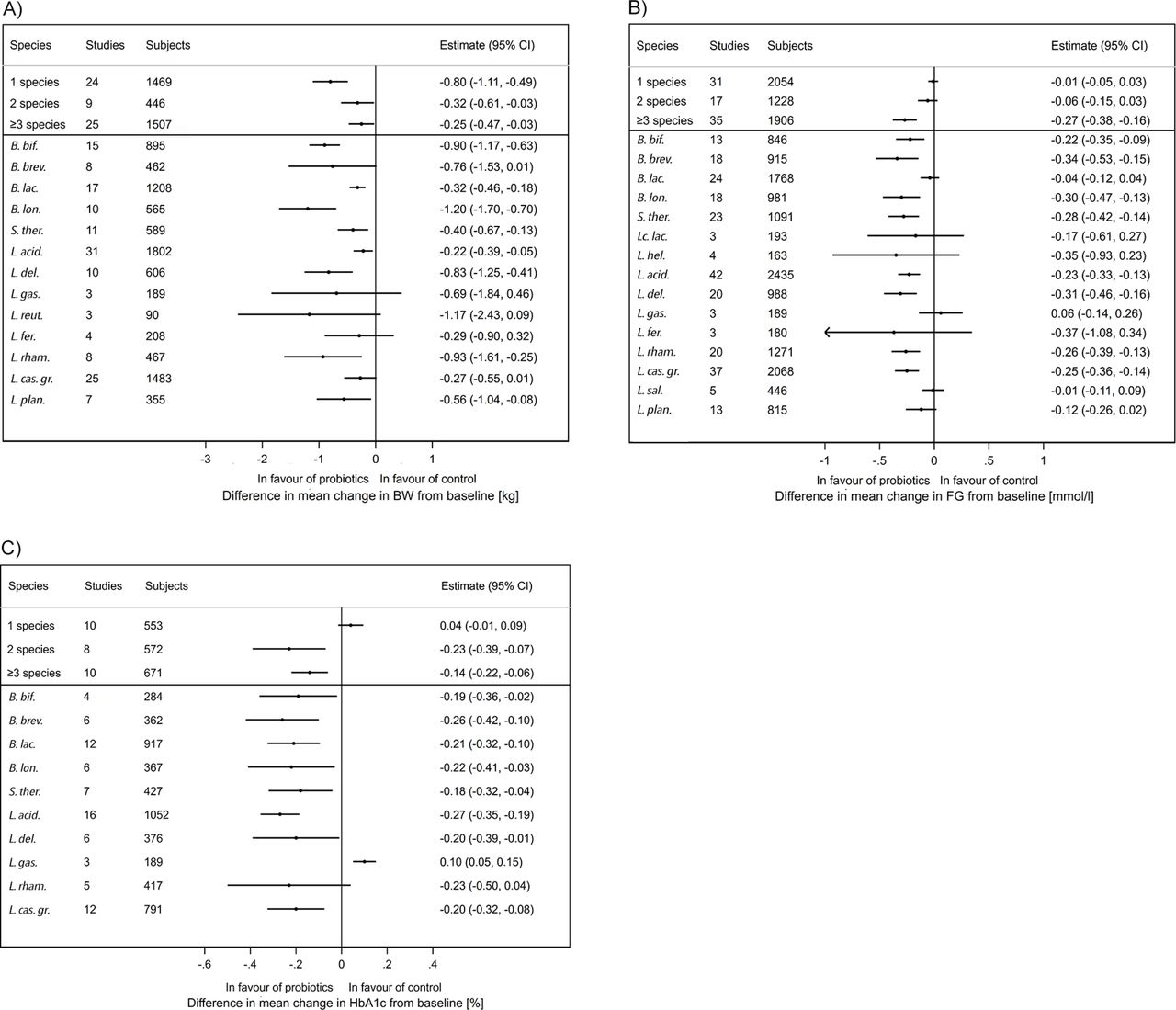
We observed a significant effect with a single bacterial species on all anthropometric variables. In contrast, a subgroup analysis showed that the use of three or more species has significant effects on an increased number of outcomes: BW, BMI, FG, HbA1c, INS, HOMA-IR, TG, ALAT and ASAT (figure 3A-C, see online supplementary table 4–10). Multiple variables BW, BMI, FG, HbA1C, INS, TG, ALAT and ASAT were significantly reduced in interventions with Bifidobacterium breve (trend for BW), B. longum, Streptococcus salivarius subsp. thermophilus, Lactobacillus acidophilus, L. casei group (trend for BW) and L. delbrueckii containing mixtures.
{kind=link}
{kind=link}
{kind=link}
Results of subgroup meta-analyses stratified by probiotics species and total number of different species administered (data shown for at least three trials): (A) body weight (kg), (b) fasting glucose (mmol/L), (C) glycated haemoglobin (%). (X-axis) Absolute difference in mean change from baseline (probiotics group—control group): random effects estimate and 95% CI. B. bif, Bifidobacterium bifidum; B. brev, Bifidobacterium breve; B. lac., Bifidobacterium animalis subsp. lactis; B. lon., Bifidobacterium longum; S. therm., Streptococcus salivarius subsp. thermophilus; Lc. lact, Lactococcus lactis; L. hel., Lactobacillus helveticus; L. acid., Lactobacillus acidophilus; L. del., Lactobacillus delbrueckii; L. gas., Lactobacillus gasseri; L. reut., Lactobacillus reuteri; L. fer., Lactobacillus fermentum; L. rham., Lactobacillus rhamnosus; L. cas. gr., Lactobacillus casei or paracasei; L. sal., Lactobacillus salivarius; L. plan., Lactobacillus plantarum.
Robustness of results regarding assumptions of intra-subject correlation
With the exception of ALAT, ASAT and TG, estimation of intrasubject correlation showed lower 90% CI bounds that were larger than 0.5. Therefore, for the majority of outcomes, the assumption of a correlation coefficient of 0.5 was found to be conservative since an assumed higher correlation coefficient would result in larger and more significant treatment effect values. For ALAT, ASAT and TG, the lower bounds of the 90% CI for the within subject correlation were below 0.5. Sensitivity analysis using these lower bound CI values as estimates for within subject correlation did not alter the conclusions reached for these outcomes.
Discussion
This meta-analysis revealed that probiotics consumption improves anthropometric parameters and BMI with small effect sizes. The effects on glucose homeostasis, systemic inflammation, TG and liver function were as well of small size and influenced by Iranian studies. These effect estimates became non-significant when excluding Iranian trials. This could be due to multiple factors like design, clinical practices, genetics, diets, lifestyle and/or environmental factors the strains tested could favour a response to probiotics in Iran. Finally, this meta-analysis did not explore the contribution of the Iranian studies in different study populations and care should be taken when generalising those findings.
A weight loss of 3% to 5% results in clinically relevant reductions in cardiovascular risk factors and weight loss of 2% to 5% results in modest lowering of HbA1c in OW and OB adults with T2DM.129 We found that probiotics consumption resulted in BW loss in OW individuals (0.94 kg, 1.2%), which is below the clinically meaningful threshold, suggesting that probiotics might be a complement to standard weight loss approaches. In addition to its effects on BW, probiotics consumption decreased BFM and WC, indicating improved body composition and fat distribution. This was corroborated in studies using computer tomography76–79 124 and probiotic interventions reduced both visceral and subcutaneous adipose tissue. In OB subjects, however, the effects of probiotics were non-significant. Obesity is a chronic disease characterised by severe gut microbial dysbiosis and OB subjects may be resistant to probiotics or require long-term administration. The median intervention duration with probiotics was 8 weeks in OW subjects and it remains to be explored whether probiotics could achieve or contribute to a clinically meaningful weight loss as part of a long-term lifestyle intervention.
Probiotics intake improved glucose control in subjects with impaired fasting glucose and T2DM. The HbA1c effect size was doubled in diabetics and INS was proportionally reduced, indicating improved insulin resistance. Probiotics intake reduced BW in subjects with T2DM indicating that BW loss contributes to the better glycaemic control. Overall, the metabolic status of subjects with T2DM improved as indicated by reduced TG and CRP, although additional research in these population is warranted. Finally, in subjects with T2DM, the mean difference in HbA1c with probiotics was −0.28, which is promisingly close to the HbA1c reductions of 0.5–2 pp associated with medical nutrition therapy.130
Probiotic intake reduced liver enzyme activity in subjects with fatty liver disease. These changes occurred with reduced BW and components of metabolic syndrome (WC, FG, TG) yet surprisingly, the surrogate of insulin resistance remained unchanged. This is promising although the number of trials is small (12), the trials were of short duration (≤12 weeks except98 119) and the majority of them were performed in Iran. Additional evaluation of liver pathology using non-invasive assessments and liver biopsy would be needed to support a clinical recommendation.
Previous meta-analyses suggested benefits with multistrain probiotic mixes compared with a single strain. We corroborated that probiotic mixes composed of three or more species resulted in improvements and identified core species: B. breve, B. longum, Streptococcus salivarius subsp. thermophilus, L. acidophilus, L. casei group, L. delbrueckii. Interestingly, yoghourt starter bacteria include L. delbrueckii subsp. bulgaricus and S. thermophilus and this finding is of interest in respect to an inverse association between yoghourt and BW change and the incidence of T2DM.131 132 In diabetics, treatment with metformin and acarbose changes faecal microbiota with an increased abundance of lactobacilli (which belongs to the Firmicutes phyla) and bifidobacteria (Actinobacteria) and these species could potentially contribute to the antidiabetic effect.133–135 The intake of probiotics on top of medication may induce even more pronounced changes in microbiota of the small intestine and this raises the question whether probiotics could become a part of the nutritional strategy in diabetes management.
Different probiotic species and strains may have multiple modes of actions affecting sugar digestion and absorption,136 fat absorption,106 gut barrier function,112 115 137 low-grade inflammation, 39 71 81 99 110 111 116 ,138 bile acid metabolism,97 139 incretin secretion120 and gut microbiota ecosystems19 44 87 115 119 and, in particular, short chain fatty acid production.121 It is reasonable to anticipate that these multiple effects may combine to induce significant effects, particularly in the case of multispecies mixes. However, the exact mechanism behind probiotics’ efficacy is unknown and currently limited to hypotheses. The majority of studies examined in the current analysis poorly described the rationale of the probiotics selected, dosing remained arbitrary and, overall, the approaches were rather empiric. Therefore, further research is warranted to select the probiotics strains not only for their capacity to comply with food grade status, but also for their capacity to survive through gastrointestinal tract (assuming this is required) and affect relevant biological target(s).
Limitations of the study
We integrated both exploratory and secondary outcomes, trials with small sample size, heterogeneous study populations, no or incomplete information on concomitant hypoglycaemic drug treatment and no or incomplete dietary and physical activity records. The heterogeneity of probiotic strains implies a limitation that we aimed to reduce by the subgroup meta-analysis at the species level. Thirty-eight per cent of trials were conducted in Iran and published within the last 6 years. These trials reported very similar designs, sample sizes, methodology, endpoints and results. Exclusion of these trials render the effect of probiotics non-significant for FG, HbA1c, INS, HOMA-IR, CRP, TG, ALAT and ASAT. The influence of these trials on the overall meta-analysis is clear though the precise reason why is difficult to know with certainty. Care is required in interpreting these data in generalising them to subjects outside of Iran. Furthermore, non-published results from studies that did not show significant results could introduce a potential bias. While our diagnostic publication bias analyses indicated evidence for publication bias (both asymmetric funnel plots and Egger’s test) for outcomes FG, HbA1c, INS, ALAT, ASAT and GGT, correction of estimates by imputing non-published studies demonstrated no effect of small study size. While including studies with low methodological quality may influence our analyses, recalculating summary estimates with filtering study quality demonstrated that our results were robust despite potential bias. For some trials, important parameters necessary for the estimation of effect sizes were unknown and we had to base our calculations on assumptions that could be only in part derived from the data at hand. For example, if SD of changes were not explicitly reported, we had to impute these by assuming a value for the intrasubject correlation. A sensitivity analysis varying the correlation assumptions within realistic ranges of correlation showed robustness of results. Even though for some outcomes the true correlation between subjects might be higher, we chose a conservative estimate (r=0.5) aimed at avoiding any overestimation bias of effect sizes and type I error inflation. Finally, we did not adjust our estimates for multiplicity tests.
Significance of the study
This meta-analysis showed that the intake of probiotics resulted in minor improvements of BW and body composition in OW subjects. Probiotics administration may provide improved glucose control and insulin function in type 2 diabetic subjects, and liver enzymes in those with fatty liver disease. These improvements were observed with B. breve, B. longum, Streptococcus salivarius subsp. thermophilus, L. acidophilus, L. casei and L. delbrueckii containing mixtures.
Unanswered questions and future research
This review and meta-analysis brought forth several questions: First, what are the underlying mechanisms? Second, how can multispecies mixes be optimised to induce synergistic effects? Third, can probiotics become part of standard dietary recommendations for obesity, diabetes and non-alcoholic disease management? Finally, with these questions, this study paves the way for clinical studies examining the potential of probiotic mixes as part of a long-term dietary intervention.
Acknowledgments
We thank Murielle Gagneau, Danone Nutricia Research, for her guidance and review of the systematic review and meta-analysis protocol, Agnès Meunier, Danone Nutricia Research, for her initial bibliography screen, Marion Genser, BGStats Consulting for her systematic literature review and data extraction, Quentin Dornic, Danone Nutricia Research and Kevin J Carroll, KJC Statistics Ltd for their statistical review and Timothy Swartz, Institute of Cardiometabolism and Nutrition, for his English editing.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
Footnotes
HK and BG contributed equally.
Contributors Study concept and design: HK, BG, JS, SR, KC. Systematic literature review: BG, HK, JS, MMS, JMF. Data extraction: BG, HK, JS, MMS, JMF. Concept and conduct of statistical analysis: BG. Interpretation of data: HK, BG, MMS, SR, JS, KC. Drafting of the manuscript: HK, BG. Critical revision HK, BG, MMS, JMF, SR, JS, KC. All authors approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Danone Nutricia Research, Palaiseau, France. The work of BGStats Consulting was funded by Danone Research, Palaiseau, France. Danone Research supported collaborative work of the Institute of Cardiometabolism and Nutrition. JS received consultancy fee from Danone Research.
Competing interests HK and JMF are employees of Danone Nutricia Research; BG received funding from Danone Research; JS received consultancy fees from Danone Research, is presently member of the Scientific Advisory Board of Actial SRL and acted as expert for Actial in a court hearing ; KC, MMS and SR have a collaborative agreement with Danone Research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Authors have included all available data in the research through supplementary figures and tables.
Patient consent for publication Not required.