Article Text

Abstract
Introduction Autoimmune and autoinflammatory diseases (AIDs) represent a socioeconomic burden as the second cause of chronic illness in Western countries. In this context, the TRANSIMMUNOM clinical protocol is designed to revisit the nosology of AIDs by combining basic, clinical and information sciences. Based on classical and systems biology analyses, it aims to uncover important phenotypes that cut across diagnostic groups so as to discover biomarkers and identify novel therapeutic targets.
Methods and analysis TRANSIMMUNOM is an observational clinical protocol that aims to cross-phenotype a set of 19 AIDs, six related control diseases and healthy volunteers . We assembled a multidisciplinary cohort management team tasked with (1) selecting informative biological (routine and omics type) and clinical parameters to be captured, (2) standardising the sample collection and shipment circuit, (3) selecting omics technologies and benchmarking omics data providers, (4) designing and implementing a multidisease electronic case report form and an omics database and (5) implementing supervised and unsupervised data analyses.
Ethics and dissemination The study was approved by the institutional review board of Pitié-Salpêtrière Hospital (ethics committee Ile-De-France 48–15) and done in accordance with the Declaration of Helsinki and good clinical practice. Written informed consent is obtained from all participants before enrolment in the study. TRANSIMMUNOM’s project website provides information about the protocol (https://www.transimmunom.fr/en/) including experimental set-up and tool developments. Results will be disseminated during annual scientific committees appraising the project progresses and at national and international scientific conferences.
Discussion Systems biology approaches are increasingly implemented in human pathophysiology research. The TRANSIMMUNOM study applies such approach to the pathophysiology of AIDs. We believe that this translational systems immunology approach has the potential to provide breakthrough discoveries for better understanding and treatment of AIDs.
Trial registration number NCT02466217; Pre-results.
- autoimmunity
- inflammation
- multidisciplinarity
- data integration
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study is conducted by a specialised ‘Clinical Investigation Centre in Biotherapy and Immunology’ with extensive experience in clinical immunology research, allowing standardisation of the procedure.
A multidisciplinary cohort management team, with specialists from medical and research specialties as well as from biostatistics and bioinformatics has been gathered allowing a robust study design.
The design integrates more than 800 clinical and biomedical information covering 19 autoimmune and autoinflammatory diseases and six related control diseases assembled in a multidisease harmonised case report form (part 11 compliant), a crucial effort for multidisease cross-analysis.
Production of a large collection of multiomics data from 1000 patient blood and faeces samples following standardised procedures that (1) are analysed through a system immunology approach together with clinical and biomedical data and (2) will benefit to the community once publicly available.
One limitation is that TRANSIMMUNOM patients are currently sampled only once, with the goal of portraying their immune status; however, the resampling of patients at later time points is possible and could be planned according to specific scientific questions that would arise from the study or from the literature.
Introduction
Autoimmune and autoinflammatory diseases (AIDs) are the second highest cause of chronic illness in the Western world.1 Reducing their morbidity is a major public health challenge. Historically, the classification of AIDs was founded first on clinical symptoms. With the development of biomedical technologies, immune markers were then progressively included in the description of AIDs. As examples, specific autoantibodies help to define systemic lupus erythematosus (SLE), type 1 diabetes (T1D), rheumatoid arthritis (RA), mixed cryoglobulinaemia, antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis and some types of myositis. Similarly, histological parameters such as inflammatory cell infiltrate help to refine the diagnosis of the different types of systemic vasculitis, such as Takayasu arteritis, giant cell arteritis and ANCA-associated vasculitis. Finally, genetic markers such as human leucocyte antigen (HLA)-B27 and MEFV gene mutations are associated with spondyloarthritis (SpA) and of familial Mediterranean fever (FMF), respectively.
Importantly, recent progress in molecular understanding of AIDs showed that there are not two distinct categories of diseases. Instead, AIDs form a continuum (the AIDC) of diseases with various proportions of inflammatory and autoimmune manifestations.2–4 Indeed, several cytokines are similarly modulated in different AIDs, such as interleukin (IL)-1 in FMF, uveitis and RA or IL-6 in RA and inflammatory bowel disease (IBD), IL-17 and IL-13 in SpA and tumour necrosis factor (TNF)-α in RA, SpA and IBD,5 and the therapeutic inhibition of these cytokines has been successful in different AIDs.6 Shared genetic association between diseases also helps define this continuum. Many yet unknown molecular and cellular mechanisms and/or alterations may be shared as well. Embracing immune system homeostasis at a multiscale level should be heuristic. It should help characterise commonalities and differences between different AIDs and find important phenotypes that cut across diagnostic groups, likewise providing biomarkers and novel therapeutic targets for these patients.
This complex type of multiscale study can be addressed through a systems biology approach. One example of the potential of systems biology in immunology was the study of the immune response induced by the yellow fever vaccine.7 The strategy involved proteomics, transcriptomics and bioinformatics. Using this approach, the authors identified gene expression signatures that could predict the humoral immune response to the yellow fever vaccine. Similarly, several international projects, such as the Human Immunology Project consortium8 funded by National Institute of Health and the Health Human Project emanating from the Milieu Intérieur Consortium,9 have already revealed the power of multiparametric systems immunology studies.10
We designed and launched an observational the Translational phenomics in immunopathology and inflammation: from cross phenotyping to biotherapy clinical protocol (TRANSIMMUNOM), designed to re-examine the nosology of a selection of AIDs using a multiparametric systems immunology experimental design. To that purpose, we selected 19 AIDs and six related control diseases for which multiparametric cross-analysis will be applied to clinical, biological, immunological and microbiome data between patients and in comparison with healthy volunteers (HV).
TRANSIMMUNOM was established as a multidisciplinary consortium including representatives of (1) clinical care (including medical doctors, medical technologists and nurses from the different specialties), (2) research activities (including immunologists, microbiologists, computational biologists and computer scientists) and (3) regulatory aspects of clinical trials (clinical trial methodologists and clinical research associates). This endeavour has made possible the inclusion of patients with different diseases and followed up in different clinical departments and the completeness and standardisation of data collection and integration. TRANSIMMUNOM is funded by the French Research Agency (ANR) as a Laboratory of Excellence (LabEx).
Study aim
The main goal of TRANSIMMUNOM is to revisit the nosology of multiple AIDs belonging to the AIDC in order (1) to discover and validate biomarkers and novel therapeutic targets and (2) to evaluate biotherapies based on this knowledge. To this end, we propose to cross-phenotype a set of 19 AIDs through a systems immunology approach. The primary evaluation criterion is the significance of new gene expression levels, pathways and signatures involved when comparing the clinical phenotypes of different AIDs. The secondary evaluation criterion is the identification of new biomarkers and/or therapeutic targets by system biology approach. More details on primary and secondary outcome measures can be found on https://clinicaltrials.gov/ct2/show/NCT02466217.
The implementation of the study can be summarised in three steps (figure 1), from design (Step 1) to implementation (Step 2) and data analysis (Step 3).
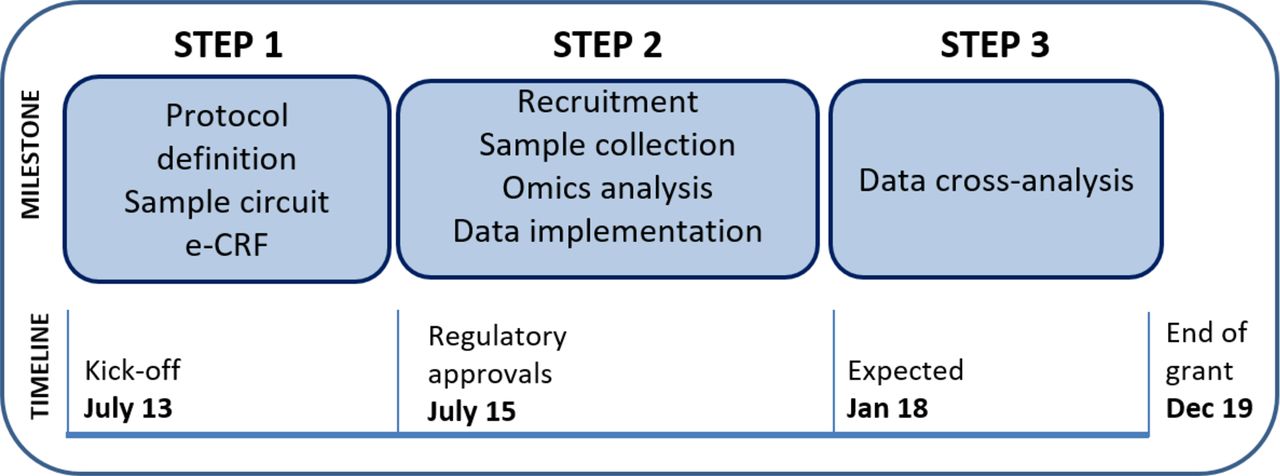
TRANSIMMUNOM overview of the study. The figure represents the implementation of the study summarised in three steps. Step 1: protocol definition, sample circuit, electronic case report form (e-CRF); Step 2: recruitment, sample collection, omics analysis and data implementation and Step 3: data cross-analysis. The three steps are shown chronologically following the timeline of the study.
Methods and analysis
Study design and set-up
The multiple AIDs selected call for multiple medical specialties and together with the systems immunology approach to be implemented; this made the endeavour necessarily multidisciplinary. Therefore, to design the study, we assembled a multidisciplinary cohort management team (CMT) (figure 2), including a clinical expert consortium (CEC) from seven specialties, nurses, biologists, clinical trial methodologists, immunologists, computer scientists and bioinformaticians. We (1) selected the list of 19 AIDs representative of the AIDC and six related control diseases and included HV, (2) established the study protocol, (3) set up a uniform and controlled sample collection and shipment circuit and (4) designed and implemented a multidisease electronic case report form (e-CRF) and a multiomics database. Control diseases were selected as to contrast with the pathophysiology of the autoimmune and inflammatory diseases under study. They were chosen as having overlapping clinical manifestations but different pathophysiological mechanisms: (1) diseases with mainly an inflammatory versus an autoimmune driver (T2D vs T1D; osteoarthritis vs RA), (2) different genetic mutations (TNF-Tumor Necrosis Factor) Receptor Associated Periodic Fever - Cryopyrin-Associated Periodic Syndromes (TRAPS-CAPS) vs FMF), (3) genetic disease versus autoimmune disease of a given tissue (muscular dystrophy vs myositis) and (4) autoimmune disease that may arise as primary or secondary to other pathologies (primary antiphospholipid syndrome (APLS) vs SLE).

TRANSIMMUNOM multidisciplinary cohort management team (CMT). The figure represents the staff involved in the CMT grouped by major discipline (biologists (purple), clinicians (blue), bioinformaticians/statisticians/computer scientists (green)) and their respective role in the implementation of the different aspect of the study (ellipse). Tasks are described following disciplinary colour code described above.
The study has been designed as a multidisease observational protocol of up to 1000 patients suffering from the list of selected diseases (see below). Patients are recruited and blood and faecal samples are collected once, at the time of a clinical evaluation.
Patients are recruited in the departments of Diabetology, Ophthalmology, Internal Medicine and Clinical Immunology at the Pitié-Salpêtrière Hospital, Rheumatology and Gastroenterology at the Saint-Antoine Hospital (Paris) and Internal Medicine at the Tenon Hospital. They are then screened and included by one of the two recruiting centres: Rheumatology at the Saint-Antoine Hospital and the Clinical Investigation Centre of Paris Est. A standard circuit for sample collection and shipment has been established and shared by the two recruiting centres. HV are selected based on internal records.
The study was done in accordance with the Declaration of Helsinki and good clinical practice. Written informed consent is obtained from all participants before enrolment in the study.
Study population
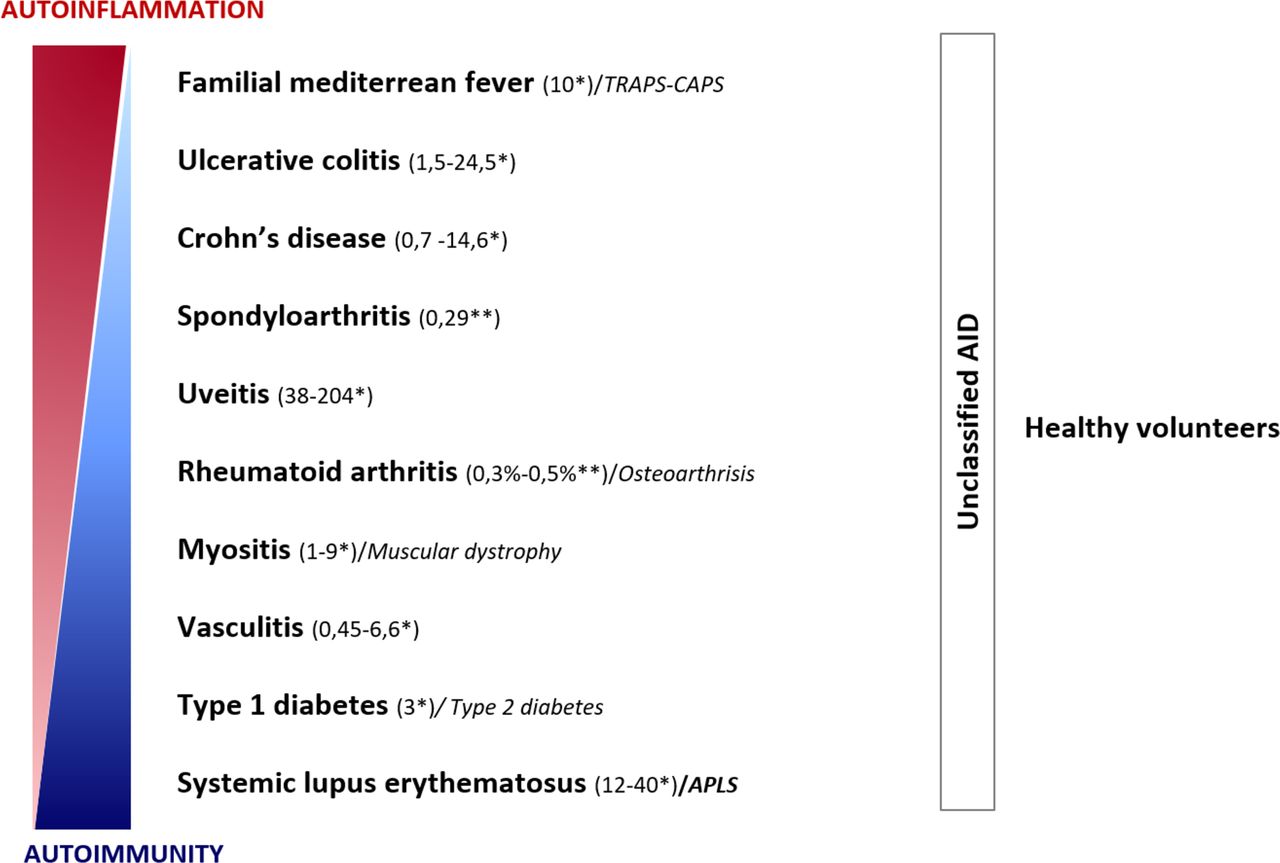
The TRANSIMMUNOM participants comprise three groups: selected AIDs, control diseases and HV. The diseases were selected based on (1) their prevalence (rare and common) and (2) the degree of autoimmune and inflammatory components of the disease so as to cover the entire spectrum of the AIDC. Selected diseases are: FMF, ulcerative colitis (UC), Crohn’s disease (CD), SpA, uveitis, myositis (in particular, polymyositis, dermatomyositis, inclusion-body myositis, necrotising and antisynthetase-related myositis), vasculitis ANCA-related (Churg-Strauss disease and granulomatosis with polyangiitis (GWP)), vasculitis non-ANCA-related (such as Behçet’s disease, cryoglobulinaemia, and Takayasu’s disease), RA, T1D, SLE and unclassified AIDs. We also included control diseases such as TRAPS-CAPS for FMF, APLS for SLE, osteoarthritis for RA, muscular dystrophy for myositis and T2D for T1D. Finally, HV were also included, stratified by age in four groups (18–30, 31–40, 41–50 and over 50 years old) and matched by sex in each group (figure 3). To be in line with the human diseases, we chose to recruit patients with heterogeneous clinical profiles and with various therapies (ie, immunosuppressive therapy, biotherapy or patient with no treatment). Diverse profiles are likely to enrich the cross-evaluation potential of our analysis and allow us to identify new molecular signatures and provide new hypotheses on underlying networks.
{kind=link}
{kind=link}
{kind=link}
TRANSIMMUNOM participant chart. This chart describes the TRANSIMMUNOM group of participants with respect to the autoinflammatory disease (AID) continuum. The TRANSIMMUNOM group is composed of patients affected by either one of the 10 AID families displayed in the chart or a control disease or an unclassified AID, as well from healthy volunteers (HV). Colour gradient bars represent the contribution of autoimmunity (blue) and autoinflammation (red) across the continuum. Each AID family is positioned along these gradients according to current knowledge, together with its respective prevalence (in parentheses) per 100 000 individuals in European Union (*) or per 60 million individuals in France (**) and, when applicable, the associated control diseases (italic). Unclassified AIDs appear across the continuum as the autoimmune/autoinflammatory processes proportions remained to be determined. HV are part of the TRANSIMMUNOM participants. Altogether the group is composed of 19 AIDs, including familial mediterranean fever, ulcerative colitis, Crohn’s disease, spondyloarthritis, rheumatoid arthritis, type 1 diabetes, systemic lupus erythematosus, polymyositis, dermatomyositis, inclusion-body myositis and antisynthetase-related myositis (grouped into myositis), Churg-Strauss disease and granulomatosis with polyangiitis (vasculitis antineutrophil cytoplasmic antibodies (ANCA) related) and Behçet’s disease, cryoglobulinaemia and Takayasu (vasculitis non-ANCA-related) (grouped into vasculitis family); six control diseases, including TRAPS/CAPS, osteoarthrosis, muscular dystrophy, type 2 diabetes and antiphospholipid antibody syndrome (APLS) (adapted from McGonagle and Mc Dermott2).
Inclusion and exclusion criteria
Participants must be over 18 years old, either diagnosed with one selected AID in the last 8 years or with one of the control disease or a healthy subject and covered by the French healthcare system. A participant is excluded if he/she is undergoing cancer chemotherapy, presents contraindications to donating blood (according to the guidelines of WHO11), is pregnant, is affected by a chronic lifelong viral infection unrelated to the disease or had an infectious event within the previous month. Informed consent is obtained from participants at the time of the inclusion visit. The study was approved by the regulatory authorities in June 2015. We aimed to include approximately 1000 patients. As an intermediary goal, we aim to include approximately 100 healthy controls, 300 patients with T1D and T2D and 200 patients with any of the selected AIDs, control diseases or unclassified diseases.
Sample and data collection
For each participant, an anonymised subject unification (ASU) number was generated based on hospital patient number (NIP) and French healthcare registration number (INSEE). ASU is a simple four-letter code one-way encrypted to guarantee safe anonymisation.
We collect 135 mL of blood for routine lab measurements and for multiomics assays. Patients are provided with a standardised kit (Metagenopolis, INRA, France) that allows easy collection of faecal samples and maintenance of their integrity during shipment before microbiota metagenomics studies.12
In a 1-day visit (lasting about 2.5 hour), we collect all samples and all clinical and biological data, which are stored in an in-house secure e-CRF (table 1). Common clinical data include demographic data, educational level, lifestyle, personal and family medical history, current and previous treatment, ECG and quality of life questionnaires. In addition, we collect disease-specific data, such as diagnostic criteria, specific activity score and clinical status and evaluation. The diagnostic criteria CRFs are used to record international validated criteria specific to each disease and features of unclassified AIDs. Specific activity scores were selected based on international guidelines: Auto-Inflammatory Diseases Activity Index for FMF,13 simplified Mayo score for UC,14 Harvey-Bradshaw Index for Crohn’s disease,15 Bath Ankylosing Spondylitis Disease Activity Index for SpA,16 Birmingham Vasculitis Activity Score for Churg-Strauss disease, cryoglobulinaemia and GWP,17 vasculitis disease activity of National Institutes of Health for Takayasu’s disease,18 Disease Activity Score-28 for RA,19 insulin dose-adjusted HbA1c for T1D20 and the Systemic Lupus Erythematosus Disease Activity Index for SLE.19 21 Immediately after collection, samples are shipped following standardised operating procedures to (1) dedicated routine laboratories for routine biology assays at the Pitié-Salpêtrière and Saint-Antoine Hospitals, (2) the Biotherapy Department for cell immunophenotyping and sorting as well as for serum cytokine analysis, (3) the Genetics Laboratory at the Trousseau Hospital for RNA and DNA extraction prior to transcriptomic and HLA analysis, respectively, and (4) the MGP laboratory for microbiome studies. The samples are processed the same day according to specific protocols.
TRANSIMMUNOM data description and management
Data integration and storage
The CMT selected, organised and standardised 865 clinical data and routine lab data on an e-CRF and integrated them using OpenClinica, a Code of Federal Regulations (CFR) 21—part 11 compliant electronic data capture tool.22
Once samples are collected and treated by the different laboratories, several million omics data are generated by using selected technologies and facilities and stored in a dedicated secure database, including deep-immunophenotyping data (circulating leucocyte subpopulations identified by flow cytometry, as an extension of our standardised method for regulatory T cell monitoring23), proteomic, transcriptomic, T cell receptor repertoire and microbiome data. All the information is centralised on secured servers hosted by the investigator laboratory.
Data analysis strategy
Since TRANSIMMUNOM protocol is an open study, we will start analysing data progressively in order to first validate the methodologies selected (pilot study) and second to ensure sample quality and data robustness. Classical statistical analyses and modelling as well as integrative analyses will be used to identify potential biomarkers of disease as well as new therapeutic targets. As a general design, the analysis approach consist in (1) performing quality control on all the data collected using dedicated tools and solutions publicly available (including clinical data through a thorough eCRF monitoring and validation); (2) implementing supervised and classical statistical methods mastered in the team,24 25 we will analyse parameter modulation (such as protein or gene expression level for cytokines and transcriptome, mean fluorescence intensity or percentage for immunophenotyping, diversity for microbiome and T cell receptor repertoire); (3) in parallel, we will implement unsupervised modelling methods publicly available or developed in the laboratory24 26–33 in order to identify more complex or hidden parameter modulations within each type of data sets, such as signature discovery29 32 34 and finally (4) once we will have complete multiparametric data sets for each subject, we will perform integrated analysis using methods relying on Regularised Generalised Canonical Correlation Analysis and variations,35–39 dedicated to the analysis of structured data sets with the aim of deciphering their relationships. Lastly, biomarkers can be discovered without full knowledge of their biological meaning. This is well exemplified in cancer where resistance or sensitivity to chemotherapy can be predicted using biomarkers without understanding the underlying mechanisms. We will thus complete our pragmatic search for biomarkers by more supervised cognitive studies by collating results from our investigations with results in the literature.
These different analysis will be applied (1) between patients (regardless of the disease) and HV, (2) between patients (disease per disease) and HV and (3) between patients diagnosed with different diseases; including gender and age as a variable for stratification of the samples.
Patient and public involvement
Patients and public were not involved in the definition of the research question or the outcome measures nor the design of the study. There are no plans to disseminate the results of the research to study participants.
Discussion
AIDs encompass a large panel of complex diseases with multifactorial aetiology. Recent molecular evidences suggest that some of these diseases share genetic and immune components,2–6 which has been a real breakthrough in the field. Indeed, most AIDs are diagnosed based on specific criteria related to symptoms and signs, which are usually subdivided into organ specific or systemic. However, it is known that many patients suffering from one AID (organ specific or systemic) may with time develop other symptoms and signs relating to a different organ, sometimes leading to the diagnosis of a second AID. Therefore, understanding the commonalities and specificities of AIDs at a molecular and cellular level appears to be essential if we are to propose better tolerated and more effective treatments for patients with AIDs. We describe here a multidisciplinary approach applied to the design, implementation and analysis of a trans-AIDs observational protocol.
Based on translational medicine, a CMT designed an innovative protocol that allowed the inclusion of patients currently followed up in different clinical departments and ensured the completeness and standardisation of data collection and integration. The centralisation of the omics analysis and the standardisation of the technics (flow cytometry panel, molecular biology) provided a uniformity of results. The CMT, including the CEC, recruited researchers from different fields to select, design and integrate state-of-the-art standards in clinical medicine, medical biology measurements and science. All the data collected were finally integrated in an e-CRF (database) so as to share information between all the CMT members.
Compared with other systems immunology projects focusing mainly on biological aspects, TRANSIMMUNOM (1) also collects a large list of clinical data that have been coded so as to allow a cross-analysis between clinical and biological data; (2) analyses patients with different AIDs, control diseases and in HV and (3) investigates cross-talk between the immune system and gut microbiota, as there is robust evidence that the microbiota influences the immune system and vice versa.40–44 TRANSIMMUNOM has the potential to provide fundamental knowledge about the pathophysiology of AIDs and to redefine their nosology. Indeed, we and others already showed the power of systems immunology to better understand biological processes associated with autoimmune and AID.24 26 28 30 45–49 Systems immunology is now seen as the future for new biomarkers and therapeutic target discovery, validated in oncoimmunology.50–52 With the advance of high-throughput data modelling and integrative analyses, it has been already shown that blood can be used to follow and even predict biological process undergoing in distant tissue.34 46 53–55 We have no doubt that with the unprecedented endeavour and deep clinical and immune profiling to be achieved in TRANSIMMUNOM, we will contribute to identify new disease biomarkers and possibly new therapeutic targets.
Ethics and dissemination
The study was approved by the institutional review board of Pitié-Salpêtrière Hospital (ethics committee Ile-De-France 48–15) and done in accordance with the Declaration of Helsinki and good clinical practice. Written informed consent are obtained from all participants before enrolment in the study.
TRANSIMMUNOM’s project website provides information about the protocol (https://www.transimmunom.fr/en/) including experimental set-up, tool developments and publications. Results will be disseminated through annual scientific committees appraising the project progresses, national and international scientific conferences, peer-reviewed journals, as well as through electronic, social, broadcast and print media. Medical school and Science University student will also be informed through lectures.
Protocol status
Step 1 is completed. We are currently at Step 2. Recruitment started in July 2015 and is expected to include 1000 patients by December 2018. A pilot study on the first 96 samples has been set up and both clinical and omics data are currently being analysed. The protocol version currently in use is V.4.0 dated 19 May 2017.
Acknowledgments
All the authors thank the patients for having accepted to enter in this clinical protocol. We thank all the staff members involved in TRANSIMMUNOM protocol: Florence Levenez and Mylène Robinet of INRA for their involvement in microbiota collection and analyses; Camille Louvrier and Fawaz Awad for DNA and RNA extraction in the Genetics Laboratory at the Trousseau Hospital; Michelle Barbie, Cornelia Degbe, Nathalie Fery, Sylvain Porrot, Anne-Laure Raveu and Alexandra Roux for the management of immunological samples in the Biotherapy Department; Adela Mekouo-Tagne and Olivia Tran for the monitoring and the regulatory aspects of the study; Anne-Marie Chenier, Eric Dasque, Edith Guilloux, Françoise Jouhannet, Celine Kocher, Laurence Koehl, Martine Lebot from Pitié-Salpêtrière CIC and the nurses of the Rheumatology Department of the Saint Antoine Hospital for management of the participants.
References
Footnotes
RL and EM-F contributed equally.
Contributors DK initiated and obtained the funding for the TRANSIMMUNOM project as a Laboratory of Excellence from the French National Research Agency (ANR). RL, EM-F and DK wrote the manuscript with input from all the authors. SA, FB, PC, DS, AS and DK designed the TRANSIMMUNOM project. RL, FB, OB, BB, PC, GG, AH, DS, JS, PS and DK designed the study protocol. RL, CA, CR, FT, ID, SH and EM-F designed the e-CRF. EM-F, AS, MR and DK with input from FP, WC, ND and HS designed the scientific research approach. CJ provides the autoantibody assays and rationale for the selection of assays. RL, CR, ChA, JS and J-ES are in charge of patient recruitment. EV and CB were in charge of the regulatory aspects and EV led the monitoring of the study.
Funding Assistance Publique-Hôpitaux de Paris. TRANSIMMUNOM (LabEx), n° ANR-11-IDEX-0004-02.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics committee Ile De France 48-15.
Provenance and peer review Not commissioned; externally peer reviewed.