Article Text

Abstract
Introduction Osteoarthritis (OA) of the knee is characterised by knee pain, disability and degenerative changes, and places a burden on societies all over the world. Exercise therapy is an often-used modality, but there is little evidence of what type of exercise dose is the most effective, indicating a need for controlled studies of the effect of different dosages. Thus, the aim of the study described in this protocol is to evaluate the effects of high-dose versus low-dose medical exercise therapy (MET) in patients with knee OA.
Methods and analysis This is a multicentre prospective randomised two-arm trial with blinded assessment and data analysis. We are planning to include 200 patients aged 45–85 years with symptomatic (pain and decreased functioning) and X-ray verified diagnosis of knee OA. Those eligible for participation will be randomly allocated to either high-dose (n=100) or low-dose (n=100) MET. All patients receive three supervised treatments each week for 12 weeks, giving a total of 36 MET sessions. The high-dose group exercises for 70–90 min compared with 20–30 min for the low-dose group. The high-dose group exercises for a longer time, and receives a greater number of exercises with more repetitions and sets. Background and outcome variables are recorded at inclusion, and outcome measures are collected after every sixth treatment, at the end of treatment, and at 6-month and 12-month follow-ups. Primary outcome is self-rated knee functioning and pain using the Knee Injury and Osteoarthritis Outcome Score (KOOS). The primary end point is at the end of treatment after 3 months, and secondary end points are at 6 months and 12 months after the end of treatment.
Ethics and dissemination This project has been approved by the Regional Research Ethics Committees in Stockholm, Sweden, and in Norway. Our results will be submitted to peer-reviewed journals and presented at national and international conferences.
Trial registration number NCT02024126; Pre-results.
- knee
- musculoskeletal disorders
- pain management
- clinical trials
- rehabilitation medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, this is the first multicentre study, with a biopsychosocial view of pain, prospectively comparing the effectiveness of two defined doses of pain-free or close to pain-free exercise therapies in patients with symptomatic knee osteoarthritis.
The proposed project includes a relatively large sample where outcomes are evaluated both during the 12-week intervention period, at the end of treatment, and at 6 months and 12 months, respectively.
The overall project uses both subjective and objective data, and includes analyses of cost- effectiveness and early predictors for a follow-up clinical outcome.
Even though the different components of the exercise programmes are well described, one limitation could be possible confounders related to the exercise dose given.
Background
Osteoarthritis (OA) is the most common form of arthritis and is a major health problem worldwide, causing illness and disability.1 2 The burden to society caused by knee OA is substantial.3 The knee joint is most frequently affected, which commonly results in chronic joint pain, knee stiffness, decreased functioning, reduced quality of life (QoL) and sick leave.4 The associated costs of OA are estimated to range between 1% and 2.5% of the gross national product as calculated in six industrialised countries (Sweden, Australia, Canada, France, UK and USA).5
Traditionally, knee OA has been defined as a pathological condition characterised by focal areas of loss of articular cartilage within the synovial joints, associated with hypertrophy of the bone (osteophytes and subchondral bone sclerosis) and thickening of the capsule.6 The mechanisms of knee OA-related pain are, however complex,7 particularly in chronic pain conditions where pain experience is nowadays believed to be more a result of changes in the nervous system than in tissue structures,8 that is, peripheral and central sensitisation.9 This may partly explain why there are poor correlations between structural degenerative changes of the knee, and pain and functioning.10 11
In a systematic review, it was concluded that there exists high-level evidence that land-based therapeutic exercise provides short-term effects on pain relief, and that there is a moderate quality evidence regarding improvement in physical functioning among patients with knee OA.12 Despite this, several questions remain unanswered, particularly regarding dose, intensity and duration of the exercise therapy applied.13 These unanswered questions may be one of the reasons why we see a large variation in treatment effects observed across studies making it difficult to conclude what is the optimal dose when delivering exercise therapy.12 13 The exercises vary from neuromuscular exercise,14 knee joint stabilisation exercises,15 strengthening exercises16 and endurance exercises.17 These forms of exercise therapy do not necessarily take into consideration the theories of local and central sensitisation, thus opening up avenues for exercise therapies where the goal is modulation of pain, decreasing local and central sensitisations. The knowledge that pain and swelling inhibits motor output, decreases range of motion (ROM) and changes coordination,18 and that a strengthening exercise programme can cause adverse effects,19 questions the use of strengthening exercises. In their review,19 Liu et al concluded that out of 121 trials, 53 had no comments about adverse events, 25 reported no adverse events and 43 reported adverse events. The majority of the adverse events from the strength training were muscle strain and joint pain, while more adverse events were reported when performing high-intensity strength training. In this context there is increasing evidence20 that exercise therapy should focus more on treating pain-related knee OA such as peripheral and central sensitisation8 and pain-related bodily and psychological changes21 from a biopsychosocial perspective22 23 rather than an impairment like muscle strength. This view is supported by research showing that pain-related fear is more disabling than pain itself.24 To break the vicious circle of long-term knee pain, we believe it is important to see beyond the knee,8 beyond an impairment such as muscle strength,25 using a biopsychosocial sensitisation model of pain.23
Medical exercise therapy
Medical exercise therapy (MET) focuses on applying optimal dose of exercise, that is, combining global aerobic exercises with semiglobal and local joint exercises, where the goal is to apply 70–90 min of active dynamic exercise therapy.26–35 Using the principle of self-paced exercises36 the patient is to perform more than a 1000 pain-free or close to pain-free repetitions per MET session.26–35 Even though the optimal dose goal of MET is high, the treatment usually starts with a low dose lasting 15–20 min mirroring the ability of the patient within a biopsychosocial context,22 23 starting with an acceptable baseline where the patient manages the exercise therapy.23 26
Global exercise activates the whole body exercising the trunk as well as upper and lower extremities; semiglobal exercise activates muscles, joints and other structures in the extremity; and local exercise activates one joint and the muscles acting on it. Sessions of global exercises are performed several times during one treatment occasion, where the goal is to substantially increase the heart rate activating the endocrine and pain modulating systems of the body, that is, the descending pain-inhibiting system, achieving cortical and spinal inhibition of nociceptive input. Semiglobal and local exercises are performed for the same purpose, however, they are performed in sets of three where each set consists of 30 repetitions. Local exercise can also be performed continuously for 3–5 min as one set, for example, deloaded knee extension, see figure 1.

The principle of deloading, performing local knee exercise.
To achieve a high volume of pain-free or close to pain-free repetitions, the principle of deloading is applied where the weight stack from a pulley apparatus is used to deload a part of the body or the whole body, resulting in less joint forces in the knee joint, see figure 1.
The theoretical basis for the principle of deloading is that the weight from the pulley deloads the weight of the lower leg with a decrease in the compressive forces between bony and cartilaginous structures. Deloading also results in decreased pulling and loading of muscles, tendons and other soft tissues, decreasing sensitisation including mechanical/loading allodynia, making it possible to exercise pain-free or close to pain-free.
MET has been evaluated in several clinical trials, and has been shown to be effective, both in the short term and the long term, in patients with long-term low back pain with or without sciatica,37 subacromial pain33–35 and long-term anterior knee pain.27 28 In these latter studies, an exercise dose lasting 70–90 min has been more favourable than an exercise dose lasting 20–30 min. In a narrative review, Lorås et al, 2015,23 included four Randomised Controlled Trials (RCTs) on the effectiveness of high-dose MET, concluding that high-dose MET was positive and promising. However, to be able to draw any firm conclusions about the efficacy in patients with knee OA, rigorous trials are needed on the effect of MET in this major patient group.38
Effect trials of cost-effectiveness are also needed as they are presently lacking in the scientific literature, and the present project has the potential to fill this knowledge gap. It is also important to point out that no exercise protocol is suited to all patients, and as knowledge of early predictors of poor treatment outcomes obtained from longitudinal data is sparse, the development of patient-customised treatments is hindered.39 According to the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) as well as a recent review,40 prediction studies are needed to be able to better individualise the treatment and match the most promising treatment option to a certain patient profile in order to maximise treatment outcomes and minimise costs. Therefore, we plan to conduct a RCT post hoc prediction study to gain insights into which patient characteristics predict treatment outcome and which patients benefit more or less from exercise treatments.
In this trial, the rationale for comparing high-dose MET (70–90 min) versus low-dose MET (20–30 min) is that high-dose MET should be more effective through an increased activation of the pain modulation systems, like the descending pain inhibiting system.41 The evidence is that exercise-induced hypoalgesia is obtained through higher and more intensive exercise doses of 70% of heart rate reserve (HRR), activating the pain modulating systems and decreasing the sensation of pain.42 However, it has also been shown that an exercise intensity of 50% of HRR is capable of producing an analgesic effect in healthy adults,43 with similar exercise intensities used in both high-dose and low-dose MET. This could have important implications for the use of exercise in the management of pain, particularly in deconditioned individuals (eg, older adults with OA of the knee). In 2008 it was shown for the first time that an endurance activity lasting 2 hours resulted in the production of endogenous neuropeptides (endorphins), creating chemical reactions in brain areas involved in cognitive function and pain modulation, primarily in the prefrontal cortices, insula and the limbic system.44 The rationale is that high-dose MET exercising for 70–90 min may result in an increased production of endogenous neuropeptides in the spinal cord, the brain stem and in the brain, compared with a lower dose MET exercising 20–30 min. The hypothesis is that this should result in less pain and improved functioning in favour of the high-dose MET therapy.
Aim of the study
The aim of this project is to prospectively evaluate short-term and long-term effects of high-dose MET compared with low-dose MET in patients with X-ray verified knee OA regarding pain, functioning and cost-effectiveness. A further aim is to conduct a post hoc analysis on early prognostic factors that predict short-term and long-term follow-up outcomes, by targeting patients’ early status and patients' adherence to the intervention. The long-term goal is to further develop and implement updated knowledge into knee OA rehabilitation to meet the challenge of tomorrow’s patients with knee OA pain.
This study seeks to answer the following research questions:
What is the effect of high-dose MET compared with a low-dose exercise therapy (low-dose MET) with respect to self-rated pain, functional limitations, health-related QoL, depression and anxiety?
What is the effect of high-dose MET compared with low-dose MET on objective performance measures such as physical functioning of a 20-metre walk, sit to stand and single knee bends, and pain threshold as determined by a PainMatcher instrument (Cefar Medical AB, Lund, Sweden)?
What is the cost-effectiveness of MET in patients with knee OA with respect to costs against potential effects (incremental cost-effectiveness ratio, ICER), and cost per quality-adjusted life year (QALY)?
Which patient characteristics (demographic or disease-related) predict long-term treatment outcomes with a focus on pain, functional limitation and health-related QoL? What important interaction effects between patient characteristics and exercise dose may predict treatment outcomes?
Material and methods
Study design
This is a phase 3 superiority trial of high-dose versus low-dose MET. The trial is blinded regarding outcome assessment and analyses. It is a two-arm multicentre trial of a 12-week exercise intervention with a 12-month follow-up. Measurements will be taken at baseline and during the treatment at 2 weeks (6 treatments), 4 weeks (12 treatments), 6 weeks (18 treatments), 8 weeks (24 treatments), 10 weeks (30 treatments), 12 weeks (36 treatments), which is the end of the treatment, and at follow-ups at 26 weeks and 52 weeks after the end of the treatment. Primary end point is at the end of the treatment. Secondary end points are at the 26-week and 52-week follow-ups. The study will conform to Consolidated Standards of Reporting Trials guidelines for reporting parallel, randomised trials45 (see figure 2).
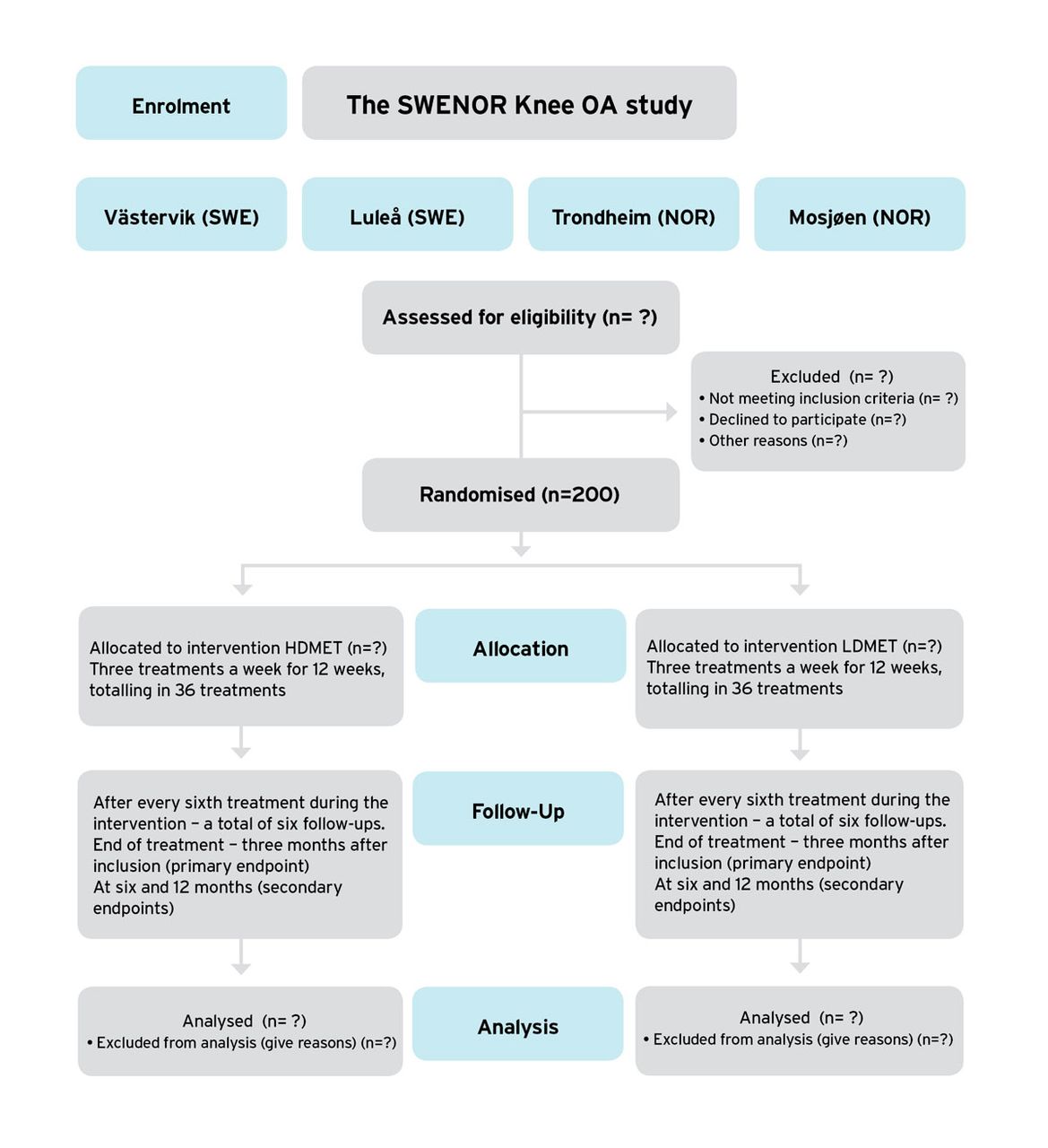
Flow chart of the design and run of the study. HDMET, high-dose MET; LDMET, low-dose MET; MET, medical exercise therapy; OA, osteoarthritis.
Participants
We are planning to include 200 patients with a diagnosis of symptomatic and radiographic knee OA who will be recruited from primary and secondary healthcare settings in Luleå and Västervik in Sweden, and in Trondheim and Mosjøen in Norway, named the SWENOR Knee OA Study.
Inclusion criteria
Subjects aged 45–85 years, living in the defined geographical areas (Västervik and Luleå municipalities in Sweden, and Trondheim and Mosjøen in Norway), who have had a diagnosis of symptomatic and radiographic verified OA grade I–III according to Kellgren and Lawrence,46 47 with at least 3 months pain duration and decreased functioning. The patient is willing to participate in a 12-week intervention period with three sessions each week.
Exclusion criteria
Physiotherapy or other conservative therapy during the previous 3 months or a history of major knee trauma such as knee fractures or ligament ruptures. Inflammatory joint disease, hip symptoms more aggravating than the knee symptoms, scheduled to have knee replacement surgery within 6 months, and comorbidities not allowing exercise such as cardiovascular, respiratory, systemic or metabolic conditions limiting exercise tolerance.
Procedure
Before the intervention starts, regular visits will be made to each intervention site by the first author (TAT), informing and communicating to the local research team the aims and run of the study. Detailed descriptions of the different stages of the study from recruitment, treatment and follow-up assessments, after the end of the intervention period, will be instructed and discussed. Physiotherapists in charge of the objective clinical testing (two in Västervik, one in Luleå, two in Trondheim and two in Mosjøen), otherwise not involved in the treatment, will be educated theoretically and practically on how these tests should be performed. The physiotherapists delivering the exercise intervention (two in Västervik, one in Luleå, two in Trondheim and two in Mosjøen) will, in addition, have structured theoretical and practical sessions on how to apply and grade the exercise therapies. A study nurse at each intervention place is in charge of randomisation, questionnaires, and the scheduling of patients for treatments and assessments. Each of the four intervention centres has a local administration officer.
A data security monitoring plan is conducted by the current investigator monitoring the present pragmatic trial. TAT will visit the four centres from the planning phase of the trial, during the treatment phase and during the follow-up phase in order to monitor that the protocol is followed. Adverse and serious adverse events (SAEs) are reported to the ethics committee.
Recruitment will be achieved through referrals from medical doctors (MDs) in primary and secondary healthcare clinics. The local investigator at each study centre will contact MDs and send written information about the study. The first screening is performed by a MD and a second screening is performed by one of the treating physiotherapists. Both the MD and the physiotherapist guarantee the radiographic inclusion criteria.
Patients will receive oral and written information about the study, and after signing an informed consent form obtained by the local administration officer, they will be assessed for eligibility by physiotherapists at each intervention centre. Participants initially fill out questionnaires for baseline data and perform the physical performance tests. Each patient is then randomised, as described below, to either high-dose or low-dose MET.
Data collection and management
Data from the questionnaires will be depersonalised at each intervention centre by the local research assistant. In order to transfer data from Norway to Sweden, a data transfer agreement (DTA) between Norges Teknisk-Naturvitenskapelige Universitet/Norwegian University of Science and Technology and Karolinska Institutet, has been set up. The questionnaires from the Swedish centres are posted to Karolinska Institutet where data are registered on digital sheets. In Norway, questionnaires from Mosjøen are posted to Trondheim where all questionnaires from the two Norwegian centres are registered on sheets and delivered to Karolinska Institutet according to DTA; Tom Arild Torstensen, Björn Äng and Wilhelmus Grooten are in charge of the data synthesis and analysis.
Postrecruitment retention and compliance strategies
Our experiences of MET as an experimental intervention (HØ and TAT)26–35 leads to the following retention and compliance strategies to be applied in this study:
An independent study nurse at each intervention centre will always be available to answer questions when patients are filling out the questionnaires. This is important to avoid any unnecessary misunderstandings regarding the content of the questionnaire and to make sure that patients understand that all information will be depersonalised.
During the interventions, the treating physiotherapist is present for the entire duration of the exercise in the exercise room answering questions from patients and re-grading the exercises according to changes in patients’ exercise status and knee OA symptoms. Participants are not informed about the hypothesis of the study.
At inclusion and at the end of the 12-week intervention period the patient is informed by the local administration nurse about the 6-month and 12-month follow-ups.
During the postintervention follow-ups, the patient will be contacted 3 weeks prior to the assessment and informed when to come to the intervention site for the planned post-treatment evaluation.
During the intervention period, the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the eight different VAS are assessed after every sixth treatment meaning after 2, 4, 6, 8, 10 and 12 weeks giving a total of six assessments. The purpose of such repeated measurements is to obtain a reasonable measurement accuracy of both functioning status and pain during the 12-week intervention period. The primary end point will be completion of the intervention after 36 treatments, which will take an average of 12 weeks. This is to obtain evaluation of effects on organised exercise therapy related with its direct implementation, while further follow-ups evaluate its retention effects. At this point primary and secondary outcomes are assessed.
Randomisation procedure
In this individual randomised trial, a stratified allocation by age and intervention centre is used, using a computerised programme, where the goal is to get an equal number of patients between the ages of 45 years and 64 years, and 65 years and 85 years at each of the four intervention centres. The randomisation key is concealed at each intervention place and kept locked by a research assistant not involved with the assessment or interventions.
Blinding procedures
The physiotherapists conducting the physical performance tests are blinded to an allocation group and the study participants are instructed by the treating physiotherapists not to reveal details of their intervention during testing. The principal investigator (BOÄ), the assistant principal investigator (TAT) and the research assistants are also blinded to groups when entering data in the data sheets, that is, they do not know which patient has received high-dose or low-dose MET. The group key will be opened after the analyses have been finalised and the results have been written in a manuscript (using interventions A and B until results have been written).
Interventions
All participants receive an MET intervention, where they are treated in groups of four or five in sessions lasting 20–90 min. During the sessions, the participants are supervised by an experienced physiotherapist in an outpatient clinic. All participants are treated three times a week for 12 weeks, thus giving a total of 36 treatments. Each patient in the group has an individualised exercise programme tailored to their specific clinical symptoms and functional level. As the treatment proceeds, exercises are adapted according to changes in symptoms and functioning. The pain experience when exercising should not exceed a 3 on a 0 to 10 scale, where 0 is no pain and 10 is the worst imaginable pain.34 Specially designed exercise equipment consisting of different forms of pulleys, exercise benches, dumbbells and barbells is used to grade and dose the exercises to be pain-free or close to pain-free, with the purpose of mitigating peripheral and central sensitisation while exercising.23 The differences between groups regarding exercise dose is outlined in table 1.
Differences between the high-dose and low-dose medical exercise therapies (METs) regarding number of exercises, sets and repetitions. Difference in time, performing global exercises and total time duration for each treatment
The grading of the exercises, including baseline settings, is based on the initial clinical assessment by the treating physiotherapist. From the patients’ past and present histories and clinical physical assessment, information is gained about the level of pain and possible sensitisation (local versus central sensitisation), range of motion and tolerance for weight bearing within the available active range of motion (AROM) of the knee. This information is used for baseline setting of the exercises where the physiotherapist chooses a starting position (SP), a AROM, and a weight resistance (WR) believed to match the patient’s ability to perform three sets of 30 repetitions (high-dose MET) and two sets of 10 repetitions (low-dose MET), pain-free or close to pain-free. Then there is a test of each exercise where the physiotherapist asks the patient to do as many repetitions as the patient can manage. When the patient reaches 10 repetitions the test is stopped and the patient has to evaluate if the WR, SP or AROM is appropriate to reach a total of 40 repetitions. Any of the above mentioned variables (WR, SP, AROM) can now be changed to reach 40 repetitions, making it possible to perform 30 repetitions in sets of three with a 30-second to 60-second pause between each. The same test procedure is used for the low-dose group where the goal is a test of 15 repetitions making it possible to do two sets of 10 repetitions. At baseline setting, there is a continuous evaluation in the exercise room where the physiotherapist and the patient are communicating working towards an optimal exercise dose for each exercise, as is usually done in clinical practice.23
It should also be possible for the patient to perform the exercise comfortably within the preferred active range of motion, AROM. For example, if a part of AROM in the knee joint is painful, the patient starts to exercise within the pain-free or close to pain-free AROM. As the treatment proceeds, AROM is adjusted, making the patient exercise in a larger and more functional AROM. If it is not possible to grade the exercise pain-free or close to pain-free, the patient is allowed to exercise with pain. When exercising with pain it is important that the pain experience does not cause any anxiety or fear. The pain has to be experienced as meaningful for improvement.48 If the exercise therapy results in an acute increase in pain, the pain should have returned to baseline before the next treatment session commences. If pain does not go back to the prior level, exercises are reassessed, with the most comfortable exercise performed several times, preferably deloaded knee extension and stationary cycling.
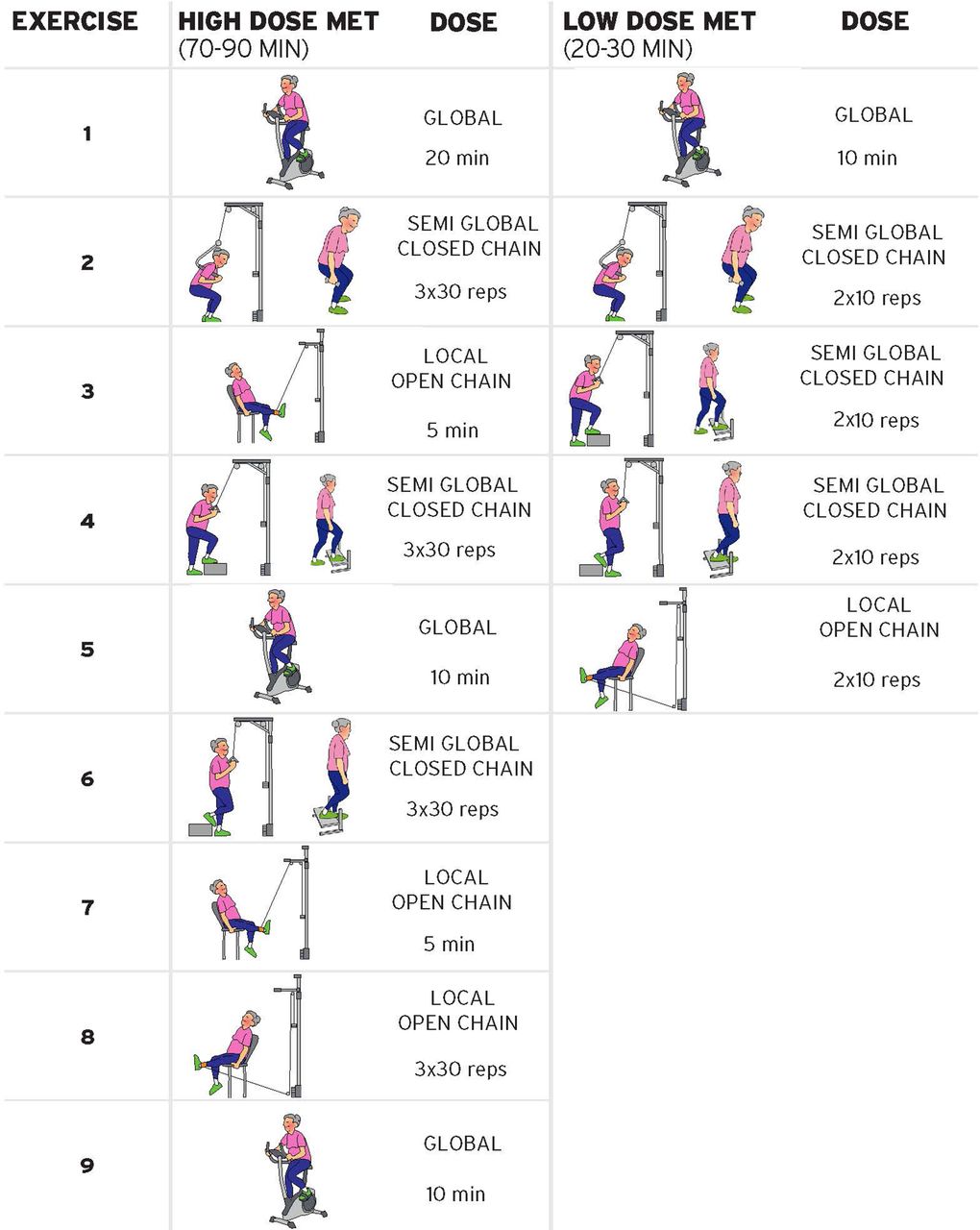
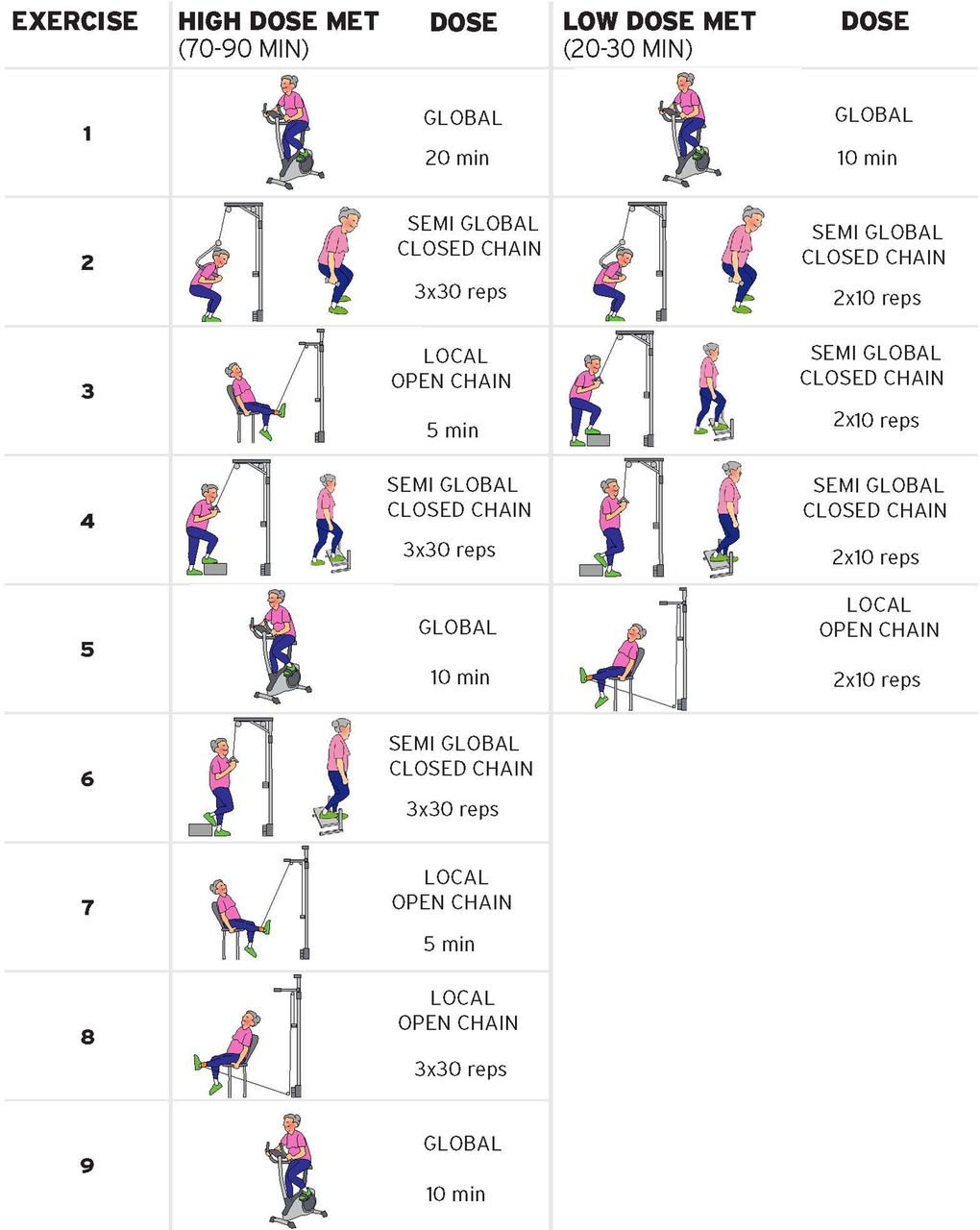
The group of four to five patients also contains patients with other diagnoses, who are not participating in this study, making the delivery of the MET intervention pragmatically similar to a real life situation. To be able to monitor the exercise dose, the treating physiotherapists follow a structured progression plan of the exercises, and fill in a treatment log for each patient at each treatment, (see online supplementary appendix 1—progression plan for high-dose MET, and online supplementary appendix 2—progression plan for low-dose MET). The log contains information about the number of exercises, duration of each global exercise, number of repetitions, and sets and weight resistance applied for semiglobal and local exercises. Consent to publish the photographs in the online supplementary appendices has been obtained from the person pictured. Figure 3 shows the main exercises from the two different exercise interventions compared in this planned randomised trial, high-dose MET versus low-dose MET.
Supplementary file 1
Supplementary file 2
{kind=link}
{kind=link}
{kind=link}
The two different exercise interventions compared in this randomised trial, high-dose MET (HDMET) and low-dose MET (LDMET). MET, medical exercise therapy; OA, osteoarthritis.
To be able to reach a high number of repetitions despite ongoing pain, the principle of deloading is applied, facilitating a high number of repetitions that are nearly or entirely pain-free (see figure 1). For the high-dose MET, the deloaded knee extension is performed twice during a treatment, each time for 5 min. This exercise and the cycling in the middle of each treatment session is a form of restitution, making it easier to both perform the deloaded closed-chain exercises and endure the high-dose MET. Later, as the patient improves and can tolerate increased loading, the exercises are adapted to be more functional, using closed-chain exercises without deloading the body weight.
To further increase the exercise dose for the high-dose MET group, patients perform one home exercise—the seated deloaded knee extension with a yellow tube theraband. The exercise is similar to exercise number 3 (see figure 1). They perform this home exercise once every day, where the dose is three lots of 3 min with a 30-second to 60-second pause between each set. The treating physiotherapists make sure that the patients are compliant in doing their home exercise. Patients in the low-dose MET receive no home exercise.
Baseline data
The following data will be obtained by questionnaire; gender, age, height, weight, physical activity and exercise levels, living arrangement, education level, employment status, possible medication, comorbidities, smoking habits, sleeping habits, pain and function of the knee, catastrophising thoughts, fear avoidance beliefs, level of anxiety and depression, life satisfaction and QoL, and beliefs about exercise. A schematic presentation of the outcome measures recorded at baseline and at the follow-ups is presented in table 2. Each assessment, which involves filling out questionnaires, will take approximately 1 hour. The objective testing of the knee and the testing with the PainMatcher apparatus takes approximately 30 min and will occur the following day.
Study measures to be collected
Primary outcome measures
In accordance with international consensus regarding the core set of outcome measures for clinical trials in OA,49 self-rated functioning and pain scoring (KOOS)50–53 are used as primary outcome measures. KOOS consists of five subscales; pain, other symptoms, functioning in daily living, functioning in sport and recreation (sport/rec) and knee-related QoL. Standardised answer options are given (five Likert boxes) and each question is assigned a score from 0 to 4. A normalised score (100 indicating no symptoms and 0 indicating extreme symptoms) is calculated for each subscale. For the purpose of an RCT, KOOS subscale scores can be aggregated and averaged as the primary outcome. We are planning to use KOOS at several time points; at baseline, and during the intervention period until the final follow-up at 52 weeks (see table 2).
Secondary outcome measures
As a secondary outcome measure, there are eight different pain measurements using a 100 mm Visual Analogue Scale (VAS),54 with terminal descriptors of ‘no pain’ and ‘worst pain’ asking about how painful the knee is, (1) today and (2) on average during the last week, related to the following four different life situations; (1) how painful is your knee, (2) how painful is your knee when loading your knee (eg, walking or standing), (3) how painful is your knee when not loading your knee (eg, sitting, lying), (4) how painful is your knee at night when you are sleeping (eg, knee pain that disturbs your sleep). Data on health related QoL are collected using the EuroQol (EQ 5-D Questionnaire)55 and the Short Form Health Survey (SF-36 Questionnaire).56 These questionnaires will also be used to perform a health economic evaluation of the exercise interventions. Psychological factors such as anxiety and depression, catastrophising and fear-avoidance beliefs are believed to both predict outcome of an intervention57 as well as influence the level of pain in patients with knee OA experience.58 In this study, anxiety and depression are rated using the Hospital Anxiety and Depression Scale (HAD),59 catastrophising is rated using the Pain Catastrophising Scale (PCS)60 and fear avoidance beliefs61 are rated using the Tampa Scale of Kinesiophobia (TSK),62 (table 2). Life satisfaction is assessed using the Life Satisfaction Questionnaire by Fugl-Meyer (LISAT).63 Beliefs and attitudes towards exercise are rated using the Self-Efficacy for Exercise Scale (SEE)64 and the patient’s expectations of performing physical activity are rated using the Outcome Expectancy for Exercise (OEE) Scale.65 PainMatcher apparatus66 is used to record sensory level, pain level and pain tolerance level. It works by pressing the thumb and first finger against a button on each side of the handheld PainMatcher apparatus; an electrode under each button activates an electrical current. As long as the pressure is kept against the buttons, the electrical current will slowly increase where the first sensation of the current is a measurement of sensory threshold. As the pressure is maintained, the electrical current slowly increases, and the sensation will turn into a pain sensation (pain threshold). Keeping the pressure on the buttons, the painful electrical current increases, and pain tolerance is recorded, that is, the measure of how painful an electrical current the patient can endure. Performance tests include the 20-metre walk test,67 first at a self-selected pace and then at maximum pace, the 30-second maximum number of chair to standing tests68 and the 30-seconds maximum number of repeated unilateral knee bends.67 69 Other measurements, logged by the supervising therapist, are recordings of compliance of the exercise treatments during the 12-week intervention also including a recording of exercise dose (weights, sets, repetitions and treatment time) at each treatment occasion. Over the whole project period, from inclusion to end of the 52-week follow-up, any adverse effects are to be noted and reported.
Statistical analysis
In the statistical analyses of both primary and secondary outcomes, the principle of intention to treat will be used, comparing high-dose MET with low-dose MET. Within-group and intergroup statistical testing will be carried out using the general linear model where an α level of 0.05 will be used where appropriate. Significance of main or interaction effects will be explored using follow-up post hoc tests. Effect size Cohen’s d will aid clinical interpretation of the magnitude of treatment effect, where effect-size values below 0.2 will be considered small, 0.5 medium and 0.8 large. The primary end point is at the end of the 12-week intervention period and potential baseline differences will be considered by adding additional baseline variables as covariates to the statistical models. Potential floor or ceiling effects will be computed and considered in our analyses. Because participants of both interventions of both intervention groups are treated together with other patients in the MET groups, the treatment credibility and outcome expectations (OEE) will be evaluated as a potential covariate or confounder for treatment effects.
Analysis of cost-effectiveness will be performed using ICER, in order to provide a single measure for weighing costs against benefits of healthcare interventions. Cost per QALY,70 using data from EQ-5D and SF-36, will be added. In the predictive analyses, multivariable logistic regressions (eg, Generalised Estimating Equation (GEE)) will be used to estimate the association between potential predictors and outcomes. A purposeful selection procedure is planned resulting in a final model that contains only significant independent variables, identified confounders and interactions. All final models will be examined for goodness of fit and accuracy according to established methods.
Sample size
The power calculation was based on proportions that can document a minimal clinical important change. The primary outcome, KOOS is a numerical scale ranging from 0 (maximal problem) to 100 (no problem). A change of 10 points is evaluated as a clinically interesting change.51 The hypothesis is that 40% of the patients receiving high-dose MET and 20% of the patients receiving low-dose MET will obtain a 10-point improvement after end of treatment at the 3-month follow-up. The power calculation showed that 82 patients are needed in each arm to reach 80% between-group power. With a hypothetical dropout of the study of 20% the total sample is 82×2×1.2=197 patients. We plan to include 200 patients giving each exercise intervention group a total of 100 participants.
Ethics and dissemination
The guidelines from the Helsinki declaration will be followed and the protocol has been approved by the Regional Ethics Review Board in Stockholm. Some relevant ethical considerations related to this study are mentioned below.
The infliction of pain
An often overlooked ethical issue is the infliction of pain when instructing patients to exercise.19 Knee OA is commonly a painful condition and it is questionable if it is ethical to push patients through the painful exercise regimens included in the approach that today is recommended for treating knee OA. A worst-case scenario for this type of treatment is pushing the patient into endurance behaviour that in itself may result in long-term pain.71 However, in this study, the focus on grading the exercises pain-free or close to pain-free,to some extent, resolves this problem.
The problem of large exercise dosage
Asking patients to exercise for 70–90 min three times a week for 12 weeks may be ethically questionable. However, such doses of exercise therapy have been shown to be effective in patients with depression72 and there is an argument today that both exercise dose and exercise intensity should be increased for patients suffering from heart disease and a metabolic syndrome, respectively.73 The high compliance with a relatively extensive exercise programme is possible because patients with chronic (or progressed) conditions commonly prioritise rehabilitation to maintain (or improve) good functioning. Thus, there is a need to investigate if a similar high dose of exercise therapy is effective for patients with knee OA. It is also of high relevance to study whether a less time-consuming exercise programme, such as the low-dose MET in the present study, results in similar effects including effects on costs.
Discussion
We believe one important strength of this study is the use of self-paced exercises, grading the exercises pain-free or close to pain-free.36 Research has shown that when patients are asked to self-select their exercise intensity, they choose an intensity that results in a positive affective response making them more motivated to do the exercise. This seems to be the case for both, populations without pain74 and patients suffering from a painful condition.75 The use of a self-paced approach, exercising pain-free or close to pain-free may—we believe—decrease the probability of patients dropping out of the study due to adverse effects such as uncomfortable painful experiences,36 75 which minimises possible nocebo effects,76 and breaks the vicious circle of knee pain.23
To decrease negative affective experiences from exercising, MET applies the principle of deloading, where the application of different types of exercise equipment deloads some of the body weight or the weight of the lower extremity. This is also the case for aquatic exercise therapy where the buoyancy of the water decreases compressive forces on the knee joint. However, aquatic exercises do not seem to be superior to land-based exercises,77 making a call for further research into dose-response effects from exercise therapy.
In an extensive review by Pedersen and Saltin,78 it was concluded that there is evidence for prescribing exercise as a therapy for 26 different chronic diseases. In addition, there is increasing evidence that a higher dose of exercise is more effective than a lower dose in patients with long-term subacromial pain34 and long-term anterior knee pain,27 patients with depression72 and patients with a metabolic syndrome.73 A high dose of exercise has a greater effect on heart function79 and a greater positive impact on mood states and QoL80 in patients with heart failure.
In terms of knee OA, however, the evidence level of exercise dose is poor.12 13 22 78 81 82 In a recent systematic review13 only five studies that compared high-intensity versus low-intensity physical activity were included. Of these five studies, there is only one study17 that is in any way similar to this planned study. The study17 compared high-intensity versus low-intensity cycle ergometry in older adults with knee OA. Both groups cycled for 25 min three times a week for 10 weeks. The high-dose high-intensity group cycled with an intensity of 70% of HRR and the low-dose low-intensity group with an intensity of 40% of HRR. After the end of the intervention period both groups had improved significantly on all outcome measures but there were no differences between groups. Juhl et al 82 argue that an optimal exercise programme for knee OA should focus on improving quadriceps strength and aerobic capacity, as well as improving performance in the lower extremities. Exercise programmes should be supervised and carried out three times a week. They also argue that there is a great need to further investigate the effects of differing exercise doses and that the interventions in such studies are described in detail with regard to intensity, length of programme, total number of supervised sessions, duration of individual supervised sessions and number of sessions per week.
To our knowledge, this study is the first to investigate, in a controlled manner, if an exercise dose lasting 70–90 min is superior in terms of improvements in functioning and pain to a lower dose of exercise therapy lasting 20–30 min in patients with knee OA.
Acknowledgments
The authors thank the following colleagues: Monitoring the study: The following colleagues are monitoring the study at respective intervention centres; In Västervik, Nisse Wallberg PT, in Luleå Mikael Sjöström PT, in Trondheim Håvard Østerås MSc PT and in Mosjøen Morten A Romslo PT. Assessment and treatment of patients: in Mosjøen (Norway), Morten Andre Romslo PT (MSc) and Iselind Thoresen PT, in Trondheim (Norway) Lasse Haugerud PT and Håvard Østerås MSc PT, in Luleå (Sweden) Mikael Sjöström PT, and in Västervik (Sweden) Nisse Wallberg PT and Thomas Aupers PT. Objective functional testing: In Mosjøen (Norway) Stine Krogh Dagsvik PT and Marte Nystad Glad PT, in Trondheim (Norway) Maria Sommervold PT and Lisa Lid PT, in Luleå (Sweden) Peter Wallström PT and in Västervik (Sweden) Erik Sjöstedt PT and Fanny Ek Nordén PT. Local study nurse handling questionnaires and in charge of the randomisation procedure locally and informing patients about follow-up assessments: In Mosjøen (Norway) Elin Slänsby and Lena Aufles, in Trondheim (Norway) Beate Iversen, in Luleå (Sweden) Katarina Söderholm, and in Västervik (Sweden) Marita Johansson.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
Footnotes
Contributors TAT, WJAG, HØ, AH, KH-R and BOÄ, have all actively participated in the planning and design of the study as well as the writing of this manuscript describing the research protocol of the study. Principle investigator in Sweden is BOÄ and in Norway HØ. TAT is the assistant principle investigator for the study.
Funding This work is supported by the Swedish Rheumatology Association and Karolinska Institutet funds, which cover a part of the economical resources. None of the funders have had any influence in developing the protocol or any other part of the study; their role has been strictly financial.
Competing interests TAT teaches courses and conducts seminars in medical exercise therapy.
Patient consent Obtained.
Ethics approval This study has been approved in Sweden by the Regional Research Ethics Committee, Stockholm ref no 2013-04-26 (2013/350-31/1) and in Norway by the Regional Committees for Medical and Health Research Ethics no 2014-06-25 (2014/1167-32).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This manuscript is describing the protocol of the study, hence we do not have any data to share.
Collaborators Nisse Wallberg, Mikael Sjöström, Håvard Østerås, Morten A Romslo, Iselind Thoresen, Lasse Haugerud, Thomas Aupers, Stine Krogh Dagsvik, Marte Nystad Glad, Maria Sommervold, Lisa Lid, Peter Wallström, Erik Sjöstedt, Fanny Ek Nordén, Elin Slänsby, Lena Aufles, Beate Iversen, Katarina Söderholm, Marita Johansson.