Article Text

Abstract
Introduction Improving accessible, acceptable recovery-oriented service provision for people with bipolar disorder (BD) is an important priority. Mindfulness and acceptance-based cognitive and behavioural therapies (or ‘third -wave’ CBT) may prove fruitful due to the considerable overlap between these approaches and key features of personal recovery. Groups also confer therapeutic benefits consistent with personal recovery and may improve recovery-oriented service provision by adding another modality for accessing support. The primary objective of this trial is to explore the feasibility and acceptability of a new recovery-focused group therapy (RfGT) intervention for adults with BD. This is the first published feasibility assessment of a time-limited RfGTrecovery-focused group therapy intervention for BD.
Methods/ analysis This protocol describes an open feasibility study, utilising a pre-treatment design versus post- treatment design and nested qualitative evaluation. Participants will be recruited from the Central Coast region of New South Wales, Australia, from primary care providers, specialist mental health services, non-government organisations and via self-referral. The primary outcomes are feasibility and acceptability as indexed by recruitment, retention, intervention adherence, adverse events (if any) and detailed consumer feedback. Clinical outcomes and process measures will be assessed to inform future research. Primary outcome data will utiliseuse descriptive statistics (eg, summarizingsummarising recruitment, demographics, attendance, attrition and intervention adherence). Secondary outcomes will be assessed using repeated-measures analysis of covariance across all time points (including change, effect size and variability).
Ethics and dissemination Ethical approval has been granted by the Northern Sydney Local Health District HREChuman research ethics committee (HREC) (HREC/16/HAWKE/69) and The University of Newcastle HREC (H-2016–0107). The Ffindings will be used to improve the intervention per user needs and preferences, and inform what amendments and/or information are required before a follow-on trial would be possible. This study contributes to a growing body of innovative, recovery-oriented innovations of psychological treatments for adults with BD.
Trial registration number ACTRN12616000887471; Pre-results.
- bipolar disorder
- recovery
- group therapy
- psychological intervention
- third wave cbt
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study involves a relatively small number of participants from a limited geographic region and is being conducted with no comparison group and a limited follow-up period.
Although group therapy can be of benefit for adults with experience of bipolar disorder, several logistical challenges may interfere with recruitment to and conduct of the group.
The proposed intervention is theory driven, incorporates evidence-based principles and strategies and will be developed to reflect expert opinion from consumers, clinicians and researchers.
Intervention duration and setting have also been selected to reflect the central pathway for accessing community-based psychological treatment in Australia, thereby minimising the gap between research and ‘real-world’ practice.
Innovation in the psychological treatment of BD is an important priority and there is a need for improved access to recovery-focused interventions; the findings from the current study will contribute to both.
Background and rationale
The concept of recovery is central to the delivery and evaluation of services for mental health and alcohol and other drugs1 2. Although recovery is personal, common themes include hope, understanding, empowerment and living a meaningful, satisfying life.3–5 Accordingly, recovery extends beyond traditional clinical definitions which focus on reduced symptomatology, hospitalisation and medication compliance.4 5 There is a corresponding need for evidence-based psychosocial treatment approaches to better reflect this evolution in service provision. Recent recovery-focused innovations for bipolar disorder (BD) include individual recovery-focused cognitive and behavioural therapy6; ‘Living with Bipolar’ (a web-based self-management intervention7) and online, recovery-focused, bipolar individual therapy.8 Preliminary findings support the feasibility, acceptability and potential effectiveness of these recovery-focused interventions.6 8 9
Drawing from preliminary findings of the potential benefit in BD10 11 and severe mental illness more broadly,12 we are particularly interested in the application of mindfulness and acceptance-based cognitive and behavioural therapies (or ‘third-wave’ CBT) to treatment innovation in BD (see ref 13 for a review of these approaches). ‘Third-wave’ approaches integrate acceptance and mindfulness with CBT.14 Importantly, there is clear concordance between elements of personal recovery (eg, awareness, understanding, empowerment and valued living) and key targets of ‘third-wave’ approaches, including (a) improved awareness of the experience of and reaction to internal events (thoughts, feelings, memories, urges and/or bodily sensations), (b) developing a less reactive and more considered stance towards internal events and (c) living life in a chosen and personally meaningful way.13 14 Moreover, as BD is typically characterised by comorbid conditions (most commonly anxiety and/or substance misuse15), the transdiagnostic processes targeted by ‘third-wave’ approaches may prove a particularly fruitful avenue for improving recovery outcomes for people with lived experience of BD.
Group-based interventions confer a range of clinical benefits consistent with recovery-oriented service provision (eg, universality, belonging, shared understanding, giving and receiving emotional support, hope and modelling16). Recent protocols lend preliminary support to the utility of mindfulness and acceptance informed groups (eg, refs 17 18). However, in contrast to principles of recovery-focused care, published protocols have not been developed in collaboration with service users, detailed qualitative feedback has not been sought and assessment of personal recovery outcomes has yet to be undertaken. Accordingly, an important opportunity exists to improve recovery-focused service delivery.
Research question
What is the feasibility and acceptability of a recovery-focused group therapy (RfGT) intervention for adults with BD?
Objectives
Primary objectives
To provide preliminary evidence regarding the feasibility and acceptability of delivering and evaluating a RfGT intervention for adults with BD. Specifically, to:
Investigate
Whether clinicians will refer adults with BD into a RfGT intervention.
Whether adults with BD will self-refer into a RfGT intervention.
Whether adults with BD are willing to participate in feasibility (and follow-on) research evaluations of the RfGT intervention.
Retention to the study (including screening, baseline, intervention and follow-up) and reasons for ineligibility, withdrawal and/or non-attendance.
Explore the acceptability of the RfGT intervention as indexed by
Number of sessions attended and level of engagement.
Detailed participant feedback to explore their experience of and satisfaction with the RfGT intervention.
Number and type of adverse events (AEs) (if any).
Explore the feasibility and acceptability of data collection methods (including the number, frequency, duration, content and delivery method of study assessments).
Secondary objectives
Secondary objectives will inform the design of future research and include exploring:
The feasibility of recruiting participants with BD who also have experience of anxiety and substance-related comorbidities.
What ‘treatment as usual’ is likely to consist of and potential similarities/differences to the RfGT intervention.
The most appropriate primary outcome measure—informed by a combination of detailed participant feedback, feasibility data and effect size estimates.
Potential mechanisms of change—to understand the processes that may underlie the impact of the RfGT intervention.
In accordance with the guidelines for developing and evaluating complex interventions,19 the current feasibility study represents vital preparatory work designed to maximise the success of any large-scale follow-on evaluation by
Producing an intervention that is acceptable to service users.
Identifying barriers and facilitators to effective recruitment, retention and data collection.
Informing estimates of recruitment, retention, engagement, adherence and effect size of the intervention across a range of outcome variables.
No prespecified criteria will be set for determining feasibility of a follow-on evaluation. Rather, our decision-making process will be informed by published guidelines for systematically appraising and responding to feasibility data (the A process for Decision-making after Pilot and feasibility Trials (ADePT) Framework20). Specifically, barriers to a large-scale evaluation will be explored, including what amendments and/or information would be needed to improve the success of a follow-on evaluation and the (im)practicality of addressing these. This information will be used to determine whether a main study is (a) not feasible, (b) feasible pending modifications to study protocol or (c) feasible as is.
Trial design
An open feasibility study using a pretreatment design versus post-treatment design and nested qualitative evaluation.
Methods
Participants, interventions and outcomes
Eligibility
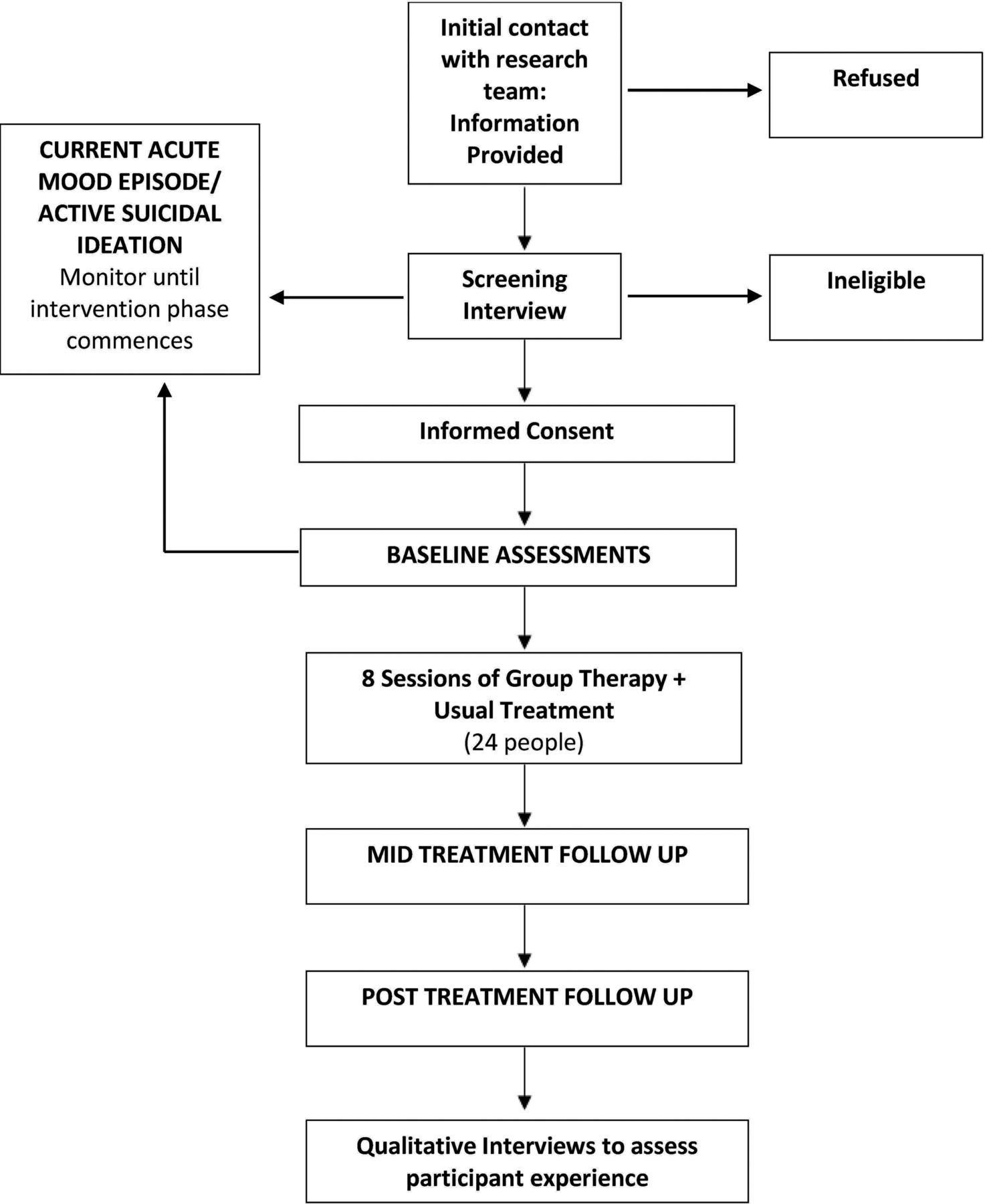
Potential participants will undergo a brief screening assessment (over the phone, Skype or in person, as per participant preference) to ensure that all inclusion and no exclusion criteria are met. Should a participant be deemed ineligible due to a current acute mood episode, if there is sufficient time left in the recruitment period, the potential participant will be offered the option of being recontacted by the research team to reassess mood stability (figure 1).

{kind=link}
Participant timeline.
Inclusion criteria
Aged 18–65.
Meeting Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-V) criteria for BD (BD-I, BD-II, Cyclothymia, Other (Un)Specified).
Able to comprehend English at a level sufficient to complete self-report instruments and clinical interview.
Willing to have RfGT sessions audio recorded.
Exclusion criteria
Current acute mood episode (as per DSM-V criteria for mania or depression).
Current suicidal ideation with intent (as per clinical judgement following discussion with the potential participant and the research team).
Unable or unwilling to provide informed consent.
Participants will not be excluded due to concurrent treatment (pharmacological or non-pharmacological). Information regarding any concurrent treatment will be collected at baseline and each follow-up occasion.
Sample size
Based on clinical and research experience, we expect that 20 participants will allow us to reliably inform our aim of evaluating the feasibility and acceptability of delivering and evaluating a RfGT intervention. Allowing for attrition of approximately 20% (eg, ref 21), the recruitment target is set at 24. This sample will afford the opportunity to deliver two to three sets of closed intervention groups. Group size (ie, 8–12 participants per therapy group) has been chosen to reflect ‘real-world’ practice by mirroring the maximum group size subsidised by the Australian government (n=10). The proposed sample size is comparable with published feasibility trials of psychological interventions in BD8 and above the recommended acceptable floor (n=10 per study arm) for feasibility studies.22
Recruitment
Potential participants for the proposed RfGT intervention will be sourced from across the Central Coast, New South Wales. The Central Coast is predominantly urban region and contains approximately 1.5% of the Australian population. Recruitment sources will include:
The R.E.A.D. Clinic, Erina, New South Wales.
Other inpatient, residential, community, outpatient and clinical health organisations, including private, public and not for profit mental health, drug and alcohol and general health services (eg, general practitioners, psychiatrists, community mental health teams, community health centres, not for profit organisations, residential rehabilitation and inpatient units) located within the borders of the Central Coast Local Health District.
Advertisements (eg, online, local media, flyer/pamphlets and study website).
A member of the research team will contact the principals, directors, case managers and/or other relevant staff contacts of the above organisations, with information about the study. Should they wish their organisation to cooperate with the study, staff members will be asked to provide written information to individual members whom they deem to be an appropriate candidate for the proposed study. If that member or client is interested in participating, based on the information provided, he or she will then voluntarily contact the research team. Alternatively, should the potential participant wish to be contacted directly by a member of the research team, they may choose to complete a ‘consent to contact’ form. At this point, it is made clear that people are only consenting to the research team contacting them to discuss the possibility of participating in the study as opposed to consenting to participate in the study itself. To maximise participant access, the study will also be advertised online, in local media and via posters and leaflets distributed across willing organisations. Interested participants will then able to voluntarily contact the research team to obtain further information.
Enrolment
Individuals who fulfil the requirements of the screening interview will be invited to attend an appointment to conduct the baseline assessment (figure 1). To enhance engagement, baseline assessments will be conducted by the lead facilitator (clinical psychologist, AKB). Following completion of the baseline assessment, the chief investigator will assign consecutively eligible participants with a unique alphanumeric code. Participants will then be offered a brief orientation/overview of the programme and invited to complete a value-based task in preparation for the first group.
Participant reimbursement
Consistent with Australian guidelines for acknowledging the time and value of consumer participation,23 participants will be offered modest reimbursement (for any time, travel and inconvenience associated with participation in study assessments) of up to a total of $40 (or equivalent in gift cards) for the baseline assessment ($20), mid-therapy ($10) and post-therapy ($10) assessments. They will also receive eight sessions of fee-free, consumer-driven, evidence-informed RfGT.
Study intervention
Development
The RfGT intervention will be developed through collaboration between clinicians, consumers and researchers. It will be an iterative process guided by (a) principles and strategies adopted by ‘third-wave’ psychosocial approaches (including mindfulness-based cognitive therapy24; mindfulness-based relapse prevention25; acceptance and commitment therapy26; dialectical behaviour therapy27; compassion-focused therapy28 and acceptance-based behavioural therapy for generalised anxiety disorder29), (b) clinical practice guidelines and published evidence regarding effective and essential components of psychological support for BD and common comorbidities (including anxiety and substance misuse) and (c) expert opinion from consumers, clinicians and researchers. Consumer feedback on the importance, relevance, content and format of the proposed RfGT intervention will be explored through a series of focus groups.
Description
The RfGT intervention will be delivered in addition to any usual treatment (pharmacological and/or psychological). The RfGT intervention will use a combination of group discussion, guided discovery, in-session mindfulness practice and homework activities. To ensure that the intervention is collaborative and respectful of client autonomy, personal choice and responsibility over behaviour change, a motivational interviewing framework will guide the delivery of all sessions.
Intervention content will be selected to support the following treatment objectives:
Increase awareness of personally held values
Strengthen awareness of what group members are already doing that is consistent with these values and support them to continue and/or expand these actions (as needed) and
Increase awareness of how group members typically respond to strong internal events (thoughts, feelings and/or physical sensations), explore the short-term and long-term costs and benefits and (as needed) explore potential opportunities for change.
Our first two aims are informed by the importance of personally meaningful change in recovery-focused service provision.4 There is a long-standing appreciation of the relationship between valued action and personal well-being within person-centred therapeutic approaches.30 Valued action refers to living life in a chosen and meaningful way, guided by what truly matters to the individual (ie, what they want to stand for, how they want to be with themselves, others and the world31). Over recent years, this seemingly intuitive link between valued action and well-being (indexed by vitality, mental health and functional outcomes) has been empirically validated32. Moreover, increasing evidence has demonstrated a positive relationship between valued action and functioning following psychological treatment for adults with experience of trauma33; long-standing symptoms of panic disorder34 and schizophrenia, anorexia, borderline personality disorder or BD.35 Lack of values clarity (uncertainty about personally held values) and lack of awareness (difficulty noticing actions that are consistent with personally held values) represent two key factors that can undermine valued action.31 Accordingly, as per our first two treatment objectives, these represent key targets of the RfGT intervention.
The third treatment objective of the RfGT intervention is guided by reinforcement sensitivity theory.36 37 Briefly, three interconnected systems have been implicated in emotion regulation. The behavioural activation system (BAS) motivates us to seek out rewarding and/or desirable experiences and work towards goals. Conversely, the behavioural inhibition system (BIS) helps to protect us from unpleasant and/or undesirable experiences by motivating us to withdraw and/or avoid. Finally, the fight/flight/ freeze system works in concert with the BIS to help protect us from threat. Although our understanding of the exact nature and function of emotion regulation systems continues to evolve, altered BIS/BAS sensitivity has been implicated in risk of depressive and (hypo)manic episodes38 39 and also progression to BD among at-risk individuals.40 Of note, these systems have also been linked to common comorbid conditions, including problematic substance use (altered BIS/BAS sensitivity41) and anxiety (altered BIS/fight/flight/freeze sensitivity42).
Guided by the reinforcement sensitivity theory,36 37 we seek to use group discussion and guided discovery to explore and normalise any identified vulnerability towards actions driven by urges to withdraw (in response to unpleasant experiences),approach (in response to pleasant experiences) and protect (in response to threatening experiences). Mindfulness skills will be used to strengthen awareness of these urges; the preceding external (eg, situations/context, people and places) and associated internal (eg, thoughts, feelings and sensations) experiences and subsequent actions taken. Learning theory and personally held values will be used to guide group discussion surrounding the short-term and long-term costs and benefits of identified actions. Specifically, the short-term benefits of actions performed in response to each type of urge (eg, pleasure, relief and safety) will be elicited and the role of any immediate benefits in strengthening the behaviour will be explored. The short-term and long-term impact on personally held values will be explored and used to guide discussion around whether/when a change in response may be useful. The role of evidence-based strategies (eg, self-monitoring; arousal modulation; distress tolerance; graded exposure; stabilising routine and so on43) in supporting desired changes will be explored. Final sessions will focus on developing individual wellness plans.
Dosage and administration
The intervention will consist of eight RfGT sessions (2 hours per session, plus a 15–30 min mid-session break) held over 8 weeks. We have chosen eight sessions to allow flexibility for future iterations to incorporate participant feedback regarding intervention timing and content and remain within the proposed 10 sessions maximum. All sessions will be led by the same clinical psychologist (Dr Alison Beck) and co-facilitated by the same Masters Level Trained Clinical Psychologist Registrar (Nathan Beehag). Prior to the first session (ie, upon completion of baseline assessments), all participants will be provided with a brief orientation to the group programme by the lead facilitator and assigned a task to complete in preparation for the first session. Participation is completely voluntary and participants are free to withdraw from the intervention at any time and/or decline to participate in any intervention element. Pending the outcome of the study, the treatment manual will be available upon request.
Integrity
All group therapy sessions will be audio recorded and rated for intervention fidelity by a trained, independent researcher not involved in intervention delivery or participant assessment. A 20% sample will be re-rated by a second, trained independent researcher for inter-rater reliability. Assessors will receive training in the assessment instruments and will have (at a minimum) Master’s level training in psychology. Group facilitators will participate in regular supervision, consisting of weekly self-reflection (eg, experience of delivering the group, challenges, successes and questions) which will be distributed to all study investigators for comment/feedback. Written feedback will be supplemented by regular phone consultations with ALB (fortnightly or ‘as needed’).
Study setting
Baseline assessments and the RfGT intervention will be conducted at a community-based private psychology clinic (The R.E.A.D. Clinic) located at Erina, on the Central Coast, New South Wales, Australia. Post-treatment follow-up assessments will be conducted at the R.E.A.D. Clinic or remotely (over the phone or Skype, as per participant preference). Aside from the Client Services Receipt Inventory (which will be administered over the phone by a trained research assistant), mid-treatment assessments will be completed online.
Outcomes
Feasibility and acceptability
To address the primary objective of evaluating the feasibility and acceptability of delivering and evaluating a RfGT intervention for BD, the following data will be collected throughout the trial:
Enrolment—including the number of participants referred, the proportion who were eligible and the number consented.
Frequency, duration and source of referrals (self vs various service providers across each month of the trial).
Number of group therapy sessions attended (and the reasons for any non-attendance).
Retention to the study (including screening, baseline, intervention and follow-up) and reasons for ineligibility/withdrawal.
Number of assessments completed; amount of missing data and detailed participant feedback regarding acceptability of data collection methods (including the number, frequency, duration, content and delivery method of study assessments).
Number and type of AEs (if any).
Detailed participant feedback to explore their experience of and satisfaction with the RfGT intervention and study methods.
Guided by the ADePT Framework,20 we aim to inform our feasibility assessment by exploring what worked well and what worked less well within the three overarching domains of intervention, study design and setting/context. Barriers to a large-scale evaluation will be explored, including what amendments and/or information would be needed to improve the success of a follow-on evaluation and the (im)practicality of addressing these. This information will be used to determine whether a main study is (a) not feasible, (b) feasible pending modifications to study protocol or (c) feasible as is.
Clinical outcomes and process measures
To address our secondary aim of informing the design of any follow-on evaluation, several clinical outcomes and process measures (table 1 and detailed below) will also be assessed to explore the following parameters:
Schedule of participant assessments
The number of participants who also demonstrate comorbid anxiety and substance (mis)use (as indexed by clinical interview and self-reported experience).
Concurrent treatment and support services accessed by study participants (including type, amount, frequency and duration).
The most appropriate primary outcome measure.
Potential mechanisms of change, including (i) mindfulness, (ii) experiential avoidance, (iii) meaningful action, (iv) impulsivity and/or (v) behaviours and/or attitudes towards medication.
Clinical outcome measures—interviewer administered
The Structured Clinical Interview for DSM-V disorders (SCID-V44) is a semistructured interview for making the major DSM-V Axis I diagnoses. The instrument is designed to be administered by a clinician or trained mental health professional and can take up to 90 min to complete (given a history of comorbidity). We will administer the mood, psychotic, substance use, anxiety and differential diagnosis modules at baseline to confirm BD diagnosis and provide information about concurrent conditions.
The Longitudinal Interval Follow-Up Evaluation (LIFE45) is a semistructured interview and rating system for assessing the longitudinal course of psychiatric illness. The SCID-LIFE includes items from the SCID, the Hamilton Depression Rating Scale46 and the BecheRafaelsen Mania Rating Scale.47 Separate severity ratings for mania and depression are generated using a six-point psychiatric status rating. Scores will be used to assess time to first episode of depression and mania, number of weeks out of episode (<4) and number of weeks without impairment (<2).
Health service and medication use will be assessed using an adapted version of the Client Service Receipt Inventory— ‘Generic’ UK Mental Health.48 The content of this inventory has been updated to reflect key sources of mental health expenditure in Australia (eg, ref 49). These data will allow us to identify elements of ‘treatment as usual’ used by study participants across the trial and provide some insight into costing.
The Social and Occupational Functioning Assessment Scale50 is a 100-point scale used by the clinician to rate current social and occupational functioning on a continuum from excellent to grossly impaired, with lower scores reflecting poorer functioning. Unlike other widely used global rating scales (eg, Global Assessment of Functioning), the SOFAS is designed to provide an index of social and occupational functioning independent of the overall severity of psychological symptoms—this is particularly important in the current study considering the likely heterogeneity of symptoms and severity. A Global Rating Scale has been chosen in preference to the multidomain assessment of functioning recommended in the DSM-V (ie, WHO-DAS 2.0) to streamline assessment and minimise burden.
Clinical outcome measures—self-report
The Brief Quality of Life in Bipolar Disorder Questionnaire51 is the condensed 12-item version of a 56-item instrument designed to specifically assess quality of life in individuals with BD.51 Preliminary evidence supports the feasibility, reliability and validity of this tool for assessing BD-specific quality of life.51
The Bipolar Recovery Questionnaire (BRQ3) is a 36-item questionnaire designed to assess personal recovery, specifically, as it pertains to adults with BD-I or BD-II. Preliminary evidence supports the psychometric properties of this tool.3
The short-form version of the Depression, Anxiety and Stress Scales (DASS-2152) is a 21-item version of the original 42-item DASS.52 It includes three, seven-item self-report scales designed to measure emotional states of depression, anxiety and stress. The Depression Scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia and inertia. The Anxiety Scale assesses autonomic arousal, tension, situational anxiety and subjective experience of anxious affect. The Stress Scale is sensitive to chronic, non-specific arousal (eg, difficulty relaxing, agitation and irritability). Each item is rated on a four-point scale of severity/frequency over the preceding 1 week. The DASS-21 demonstrates sound reliability and validity53 and Australian normative data are available.
The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST 3.154) is an eight-item questionnaire designed to screen for the use (3 months and lifetime) of tobacco, alcohol, cannabis, cocaine, amphetamine-type stimulants, sedatives and sleeping pills, hallucinogens, inhalants, opioids and ‘other’ drugs. The ASSIST generates a risk score (lower, moderate and high) for each substance category. It was originally designed to be administered by a health worker, but preliminary evidence supports the feasibility,55 reliability and validity56 57 of self-report administration.
The EuroQol five dimensions’ questionnaire (EQ-5D) is a widely implemented instrument for assessing health-related quality of life and estimating quality-adjusted life years in cost–utility analyses. This five-item self-report inventory assesses five domains of quality of life (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). We will use the newest version– the EQ-5D-L.58 To correct potential ceiling effects associated with the original version, the EQ-5D-L uses five (relative to three) response categories to assess the severity of problems experienced (no problem, slight, moderate, severe and extreme).
Process measures
The Five Facet Mindfulness Questionnaire-SF (FFMQ-SF59) is a 24-item version of the FFMQ.60 It comprises five domains (observing; describing; acting with awareness; non-judging of experiences and non-reactivity to experiences), which can also be summed to produce an overall score. Higher scores reflect greater mindfulness. Each item is rated on a five-point scale from one (never or very rarely true) to five (very often or always true) in terms of what is ‘generally true for you’. Evidence supports the reliability, validity and sensitivity to change of this condensed version of the FFMQ.59
The Acceptance and Action Questionnaire (AAQ-261) is a seven-item questionnaire designed to assess experiential avoidance versus psychological flexibility, with higher scores reflecting greater experiential avoidance. The AAQ-2 has demonstrated good internal consistency and test–retest reliability.61 62
The Valuing Questionnaire63 is a 10-item self-report inventory designed to assess the extent of past values enactment over the preceding 1 week. It comprises two factors: progress (awareness of and enactment on what is truly important) and obstruction (disruption to valued living arising from avoidance, distraction and/or inattention). Preliminary evidence supports the psychometric properties of this instrument.63
The Positive Urgency Measure (PUM64) is a 14-item self-report measure of positive urgency—the tendency to act impulsively in response to positive moods. Each item is rated on a four-point Likert scale from one (agree strongly) to four (disagree strongly). The scale demonstrates sound psychometric properties, including high internal consistency (α=0.94–0.9564; α=0.8265), and PUM scores have been associated with addictive behaviours (eg, gambling and drinking64).
The urgency, premeditation, perseverance and sensation seeking Impulsive Behaviour Scale66 is a 45-item self-report inventory designed to assess impulsivity across dimensions of the five-factor model of personality. In accordance with prior research (eg, ref 65), we will use the 12-item urgency subscale as an index of impulsive behaviour in response to negative affect, including difficulty resisting craving and temptation. As per the PUM, each item is rated on a four-point Likert scale from one (agree strongly) to four (disagree strongly). The Urgency Subscale demonstrates high internal consistency (eg., α=0.86–0.8967 and see 65 α=0.89).
The Self-Control Schedule68 is a 36-item self-report inventory designed to assess the use of different self-control methods to solve behavioural problems (including ‘self-statements’/cognitions; problem solving; delaying immediate gratification and belief in self-efficacy). Each item is rated from minus three to plus three, with higher scores indicating greater utilisation of self-control methods. Good reliability and validity are reported by the author.68 Preliminary findings also support the sensitivity of the instrument for detecting change after psychological therapy for BD.69
The Medication Adherence Rating Scale70 is a 10-item (yes/no) self-report instrument designed to assess behaviour and attitude towards medication over the preceding 1 week. The instrument is designed to be scored from 0 to 10, with higher scores indicating greater medication adherence.
Therapeutic alliance
The Group Session Rating Scale (GSRS71) is a four-item Visual Analogue Scale designed to be a brief tool to assess group-therapy alliance. The items assess ‘relationship’, ‘goals and topics’, ‘acceptability of approach’ and ‘overall fit’ and are ranked from low to high according to prespecified anchors. GSRS scores are obtained by measuring the marks made by the client and summing the lengths (nearest centimetre) of each line (maximum total score=40). Evidence supports the reliability and concurrent validity of this instrument for use in substance use populations.72
Adherence to treatment protocol
The schedule of fidelity assessments is detailed in table 2. Adherence to recovery-oriented service provision will be guided by the Recovery-Oriented Service Self-Assessment Toolkit (ROSSAT).73 The ROSSAT was developed by the Mental Health Coordinating Council in consultation with consumer advocacy group being as a mechanism for workers74 and organisations75 to assess their level of recovery-oriented service provision. Item content reflects six key indicators of recovery-oriented service provision identified during the ROSSAT development process (relationships; respectful practice; consumer self-directed focus; belief in consumers recovery; obtaining and sharing knowledge and information and participation and social inclusion4).
Schedule of fidelity assessments
Both RfGT facilitators will complete the ROSSAT Tool for workers74 after sessions one, four and eight. This tool comprises 37 items across four domains: values, principles and philosophy underpinning service provision; recovery-oriented service provision; workers’ responsibilities, roles and attributes; education and training. Each item is rated on a five-point Likert scale from one (needs significant development) to five (outstanding achievement). Objective assessment will also be conducted by having an independent assessor rate all audio recordings of the RfGT sessions against a subscale (recovery-oriented service provision) of the corresponding ROSSAT Tool for organisations.75 Each item is rated on a four-point Likert scale from one (needs significant development) to four (outstanding achievement).
Adherence to intervention content will be guided by a checklist specifically designed for the current study. The checklist will reflect the key aims, activities and discussion points for each RfGT session. At the end of each session, facilitators will be asked to rate the degree to which each item was addressed and to note any deviations. An objective rating of this checklist will also be undertaken by an independent assessor based on their review of session audio recordings. As the intervention is grounded in CBT, audio recordings will also be rated for fidelity using the Cognitive Therapy Scale—revised version.76
Participant timeline
Data collection, management and analysis
Data collection
To facilitate engagement and working alliance, the baseline assessment will be conducted face to face at the R.E.A.D. Clinic by the lead facilitator. Post-treatment follow-up assessments will be conducted face to face or remotely (eg, Skype and telephone) as per participant preference by a trained research assistant not involved in intervention delivery. Aside from the Client Services Receipt Inventory (which will be administered over the phone by a trained research assistant), mid-treatment assessments will be completed online.
Interviewer-administered instruments will be collected in hard copy and electronic formats (ie, hard copy scanned into a computer and/or directly entered into an electronic database). Baseline and follow-up self-report questionnaires will be collected online (eg, using Survey Monkey or similar). As the BRQ3 uses a Visual Analogue Scale, this questionnaire will be completed by hand and returned electronically (eg, faxed, scanned or photographed and returned by email). The score will be calculated and entered into an electronic database. The GSRS71 also employs a Visual Analogue Scale. Hard copies will be completed by intervention participants at the end of each group therapy session. The score will be calculated and entered into an electronic database. Group therapy sessions will be audio recorded using hand-held audio recorders. Audio files will be uploaded onto a secure electronic server for storage and analysis.
Data management
Data entry will be performed by AKB. All hard copy data will be entered into Microsoft Excel. All data collected online will be downloaded and saved into the Excel database. Several mechanisms will be used to ensure data integrity, including referential data rules, valid values and range checks. Data query reports will be used to check for errors in data entry. Identified queries will be cross-checked against the original data source. A log of any changes made to the original data source or electronic database will be maintained throughout the trial.
Statistical methods
The following statistical analysis plan has been developed in collaboration with the Clinical Research Design, IT and Statistical Support (CReDITSS) Unit at the University of Newcastle. Considering the primary aim of exploring feasibility and acceptability, we expect that outcome data will primarily use descriptive statistics (summarising recruitment, demographics, attendance, attrition and intervention adherence). For the secondary outcomes, that is, scores on various measures at baseline, mid-treatment and at post-treatment follow-up, we intend to use repeated-measures analysis of covariance across all time points (including change, effect size and variability); this will minimise the number of statistical tests and reduce the risk of inflated type I error. These models will include group, time and group x time interaction terms. This approach also provides an omnibus test, which, if significant, will reduce type I error when doing post hoc analyses of pairwise contrasts, for example, baseline versus midpoint and baseline versus post-treatment values. The level of significance will be set at P<0.05.
Monitoring
Potential harms
Dealing with risk
We acknowledge that discussing mood and related experiences may be associated with feelings of distress. Accordingly, participants will be offered a ‘support call’ 24–48 hours after each assessment occasion to assess any adverse impact of the assessment process. In the event that a participant raises concerns about feelings of distress, this will be documented and responded to as per guidelines for reporting AEs (see below) and/or assessing and responding to suicide risk (as appropriate77).
Although suicidal ideation is a common feature of BD78 and not necessarily accompanied by intent and/or attempt,78 79 regular risk assessment will be undertaken throughout the study. Risk of suicide will be assessed at screening and then at each assessment occasion (and as needed, at each follow-up ‘support call’). Consistent with New South Wales Health Guidelines for assessing and managing risk of suicide,77 in the first instance, a hierarchy of screening questions will be used, and as needed, supplemented by a follow-up comprehensive risk assessment. Any participant endorsing suicidal ideation will be asked whether they would like written information about available support services (eg, Lifeline and Suicide Call Back Service) and/or a self-help ‘tip sheet’ developed by the suicide call back service.
Adverse events
An AE, also referred to as an adverse experience, will be defined as any unfavourable/unintended psychiatric occurrence in a study participant necessitating acute or crisis intervention—whether it is considered to be intervention related or not.
‘Psychiatric occurrence’ will be defined in terms of any change in mental state that precipitates acute care and/or crisis intervention. This may include suicidality, self-harm, acute mood episode and/or intoxication from alcohol and/or substances.
A subset of AEs will be classified as ‘serious AEs’ and will require expedited reporting. Serious AEs will be defined as:
Any AE resulting in hospitalisation.
Any AE resulting in persistent or significant disability/incapacity.
When the untoward psychiatric occurrence is life threatening (NOTE: the term ‘life threatening’ refers to an event in which the patient was at risk of death at the time of the event; it does not refer to an event which hypothetically might have caused death if it were more severe).
When the untoward psychiatric occurrence results in death.
AEs will be assessed at each follow-up occasion via questions pertaining to treatment history. Any instance of acute/crisis intervention will be documented by the research assistant and reported to the responsible human research ethics committee (HREC). The lead facilitator of the RfGT intervention (AKB) will also document and report any utilisation of acute/crisis intervention they learn about while delivering the intervention.
The University of Newcastle HREC will be informed about any AEs, unforeseen events and complaints within 72 hours of learning about them. The relevant University of Newcastle template for reporting trial events will be used. The reports will be independently reviewed by the University of Newcastle HREC (sub)committee or executive to determine whether the event is trial related and the appropriate course of action. If the HREC (sub)committee or executive deems further information is required, it will request this from:
An independent expert in the area or
The coordinating investigator
AE reports and outcomes will also be reported to the Northern Sydney Local Health District (NSLHD-HREC) for independent review.
Data monitoring
An independent data safety monitoring board will not be convened. The current study is a one-arm trial of a non-invasive psychological intervention that will be developed in close consultation with consumers to reflect evidence-based principles and strategies. It will be delivered in the context of ‘treatment as usual’, does not involve experimental administration of medicine or experimental therapeutic devices and no interim analyses are planned. For each assessment occasion, AKB will review the first three assessments and every one in five thereafter for completeness and accuracy. To inform feasibility assessment, a log will be maintained of any missing data, errors in administration and corrective feedback provided to study assessors.
Auditing
Written updates and project meetings will be held at least quarterly or more frequently as needed. Written updates and meetings will focus on consumer involvement, intervention development, recruitment rates, treatment fidelity, progress with follow-ups, discussion of AEs (if any), data management and project timelines. Identified problems will be discussed and potential solutions posed.
Discussion
In accordance with calls to improve the transparency and quality of complex behaviour change research,80 the current paper details the protocol for an open feasibility study of a RfGT intervention for adults with experience of BD. Preliminary evidence supports the feasibility and acceptability of recovery-focused interventions in BD.6 8 9 Mindfulness and acceptance-based therapies also show promise (refs 17, 18 and 81, see also ref 10 for a recent systematic review). To our knowledge, only one other group therapy protocol has combined these approaches for treatment of BD (currently being investigated by a team at the University of Exeter). However, unlike the current study, the University of Exeter "Thrive" protocol specifically targeted individuals who experience rapid cycling and at 16 sessions, is less practical for an Australian healthcare setting. As this is the first trial whereby recovery-oriented and third-wave approaches have been combined into a time-limited (ie, <10 sessions) group therapy intervention for adults with BD, feasibility assessment is warranted. Specifically, to identify what challenges would undermine the success of a follow-on evaluation, explore the practicality of addressing these and discuss the best pathway forward.19 Accordingly, this study reflects vital preparatory work to maximise the success of any future full-scale evaluation, and conversely, to curtail further investment in an untenable proposal.
Strengths
Feasibility studies represent an important, but often under-utilised and under-reported phase of intervention development and evaluation.19 This feasibility study was prospectively registered and is reported here in accordance with best practice recommendations for intervention protocols.82 Interpretation of outcome data will be informed by published guidelines20 and recommendations will be made regarding what further information and/or amendments to the intervention, context and/or design would be needed to maximise the success of a follow-on evaluation (and the practicality of same).
Innovation in the psychological treatment of BD is an important priority and there is a need for improved access to recovery-focused interventions.11 The findings from the current study will contribute to both. The proposed intervention is theory driven, incorporates evidence-based principles and strategies and will be developed to reflect expert opinion from consumers, clinicians and researchers. Intervention duration and setting have also been selected to reflect the central pathway for accessing community-based psychological treatment in Australia, thereby minimising the gap between research and ‘real-world’ practice. To this end, we have also chosen to recruit participants with a bipolar spectrum disorder (ie, relative to limiting to BD-I and/or BD-II) to reflect both the heterogeneity and the diagnostic ambiguity that are often characteristic of patients who present to primary care settings.83 84 Furthermore, our decision to exclude participants from the group if they are experiencing a current episode of depression or mania (ie, relative to specifying a symptom threshold) means that our sample is more likely to reflect the between episode symptoms that often characterise the course of BD. Additional strengths include our carefully characterised sample, use of an independent assessor to conduct follow-up assessments, structured attempt to characterise treatment as usual and comprehensive fidelity assessment.
Limitations
Some limitations are also apparent. First, although group therapy can be of benefit for adults with experience of BD,85 our decision to use a closed group format is not without logistical challenges. For example, participant flow must be sufficient to form a group within a reasonable time frame, as risk of dropout has been found to increase with increased wait-time (eg, ref 86). Furthermore, if attrition remains high, membership of closed groups may diminish such that the group itself is no longer viable. Second, using a private facility to deliver the intervention may inadvertently impact study recruitment. For example, beliefs by service users and/or providers surrounding private psychology (eg, high cost unsuitable for severe mental illness) may interfere with willingness to refer. However, from a translational perspective, as private psychology providers represent a key mechanism for accessing psychological support in Australia, willingness of individuals and/or service providers to refer to a private facility is an important feasibility question. Third, detailed qualitative evaluation of acceptability is also currently limited to group members. Pending acceptability at the level of the client, further research would be needed to explore acceptability to healthcare providers. The study will also involve a relatively small number of participants from a limited geographic region (Central Coast, New South Wales, Australia). However, the proposed sample size is within the range of related feasibility studies (eg, ref 8) and above the acceptable floor (n=10 per study arm) for feasibility studies.22 Finally, this is an open trial with no comparison group and limited follow-up period. Although this design is appropriate for addressing our objectives of feasibility and acceptability,87 pragmatic considerations (funding and time constraints) meant that the current protocol was amended from a pilot randomised controlled trial (RCT) with 3-month post-treatment follow-up (see ref 88 for details of original registration on the Australian New Zealand Clinical Trials Registry).
Conclusions
Treatment innovation in BD is an important priority.11 Improved focus on personally meaningful recovery relative to traditional clinical outcomes is needed. To accommodate individual needs and preferences, choice over treatment modality is important.89 Group therapy confers a range of therapeutic benefits, including universality, belonging, giving and receiving emotional support, modelling, practising interpersonal skills and bonding.16 Group therapy also represents a considerable under-utilised resource within the Australian primary healthcare setting (representing less than 1% of Medicare funded services with a clinical psychologist in 2015).90 To ensure that the proposed intervention is directly transferrable to existing models of time-limited, government subsidised mental healthcare in Australia, a protocol with a maximum of 10 sessions is needed. The current study represents an important step in bridging the gap between research and clinical practice by working closely with consumers to develop an acceptable intervention that is also accessible under existing service delivery models.
Ethics and dissemination
Protocol amendments
Any amendments will be submitted to the Northern Sydney Local Health District HREC for review and registered with the University of Newcastle HREC prior to implementation as per HREC guidelines. AKB will oversee the submission of amendments and associated update of trial registration. Version control using protocol identifiers and dates and a list of amendments will be maintained to track the history of amendments and identify the most recent version of study documentation.
Confidentiality
Assessment data will be labelled with a unique alphanumeric code. All hardcopy data will be securely stored in a locked filing cabinet. In accordance with University policy and ethical approval, all electronic data and data sets will be password protected and stored on a secure university server (ownCloud). The encrypted file containing the link between participant details and each unique alphanumeric code will be password protected, stored separately to study data and accessible only to key research personnel. At the completion of the project, the encrypted document containing participant codes and associated participant contact details will be destroyed. In accordance with the Research Data and Materials Management Procedure (University of Newcastle, 2015), this non-identifiable data will then be retained for a minimum of 20 years after date of publication or termination of the study.
Ancillary and post-trial care
Throughout the study, participants will not be asked to change any of their usual treatment. They will also be able to access additional treatment and/or services as per usual. As this is a one-arm feasibility study, no provisions for post-trial access to the intervention will be made. The proposed RfGT intervention will be developed in close consultation with consumers and will use non-invasive, evidence-based psychological strategies. In the unlikely event of harm, participants enrolled into the study will be covered as per the conditions set out in The University of Newcastle Medical Malpractice & Professional Indemnity and Public Liability insurance policies.
Dissemination policy
At the time of consent, all study participants will be invited to indicate whether they wish to receive a summary of findings. A written lay summary will be produced and sent to study participants. The results will also form the basis of several articles that will be submitted to peer-reviewed journals to be considered for publication. A list of potential publications will be generated at the beginning of the trial and author order and respective contribution agreed upon. All authors will be required to fulfil the criteria set out within the recommendations of the International Committee of Medical Journal Editors.91 The findings will also be disseminated via conference, seminar, in-house and/or poster presentations. A summary of findings and links to journal articles and other publications/presentations resulting from the study may also be published on academic, health and/or consumer-oriented websites. A copy of all publications arising from this study will be housed in the University of Newcastle Online Repository. As appropriate, this study will be used to inform grant applications to fund future investigations.
Acknowledgments
We gratefully acknowledge the volunteers of ACACIA: The ACT Consumer and Carer Mental Health Research Unit for their valuable feedback on the recovery-focused group therapy intervention. Thanks also to The R.E.A.D. Clinic for providing facilities to conduct study assessments and intervention delivery and The Centre for Mental Health Research, Australian National University for providing facilities to conduct the focus groups.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
Footnotes
Contributors AKB is a trial coordinator and led the development of the study protocol, recovery-focused group therapy intervention and manuscript in collaboration with all investigators listed. All investigators contributed to study design, selection of assessment instruments and informing the duration and content of the group therapy intervention. Specifically, ALB contributed expertise on motivational interviewing and multiple health behaviour change; SHJ contributed expertise on recovery focused interventions in bipolar disorder (BD); FL contributed expertise on the conduct and process of group therapy interventions in BD; FK-L contributed expertise on cognitive behaviour therapy for severe mental illness and potential opportunities for integrating technology (eg, self-monitoring); MB provided expertise from the perspective of a person with lived experience of BD (including co-facilitating focus groups with AKB)—ensuring that the perspective of the service user was represented throughout all stages of the research process. JA led the statistical analysis plan and contributed to study design (eg, advising on sample size and outcome measures). In summary, all authors made substantial contributions to study conception and design. All authors also offered critical revisions to the manuscript for important intellectual content, have approved the final version of this manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Dr Beck is supported by a stipend from the NHMRC Centre for Research Excellence in Mental Health and Substance Use (APP1041129; G1200943). In-kind support (therapy room) is provided by the R.E.A.D. Clinic. Dr Banfield is supported by Australian Research Council Discovery Early Career Researcher Award DE150100637.
Competing interests We have read and understood BMJ policy on declaration of interests and declare the following interests: AKB is the CI and will be responsible for conducting the baseline assessments and group therapy intervention. She is also a contract clinical psychologist at the R.E.A.D. Clinic Erina, where the research is to be conducted. Nathan Beehag (co-facilitator) is a contract psychologist at the R.E.A.D. Clinic. The nature of the study minimises the likelihood of potential conflict of interest, in that study participation involves routine elements of psychological assessment (completion of self-report questionnaires, clinician-administered questionnaires and clinical interview) and participation does not require participants to change their current involvement with services.
Patient consent Obtained.
Ethics approval This study has been approved by the Northern Sydney Local Health District human research ethics committee, reference number RESP/16/45; HREC/16/HAWKE/69 and The University of Newcastle HREC, reference number H-2016-0107.
Provenance and peer review Not commissioned; externally peer reviewed.