Article Text

Abstract
Introduction Repetitive loading of the musculoskeletal system is suggested to be involved in the underlying mechanism of the majority of running-related injuries (RRIs). Accordingly, heavier runners are assumed to be at a higher risk of RRI. The cushioning system of modern running shoes is expected to protect runners again high impact forces, and therefore, RRI. However, the role of shoe cushioning in injury prevention remains unclear. The main aim of this study is to investigate the influence of shoe cushioning and body mass on RRI risk, while exploring simultaneously the association between running technique and RRI risk.
Methods and analysis This double-blinded randomised controlled trial will involve about 800 healthy leisure-time runners. They will randomly receive one of two running shoe models that will differ in their cushioning properties (ie, stiffness) by ~35%. The participants will perform a running test on an instrumented treadmill at their preferred running speed at baseline. Then they will be followed up prospectively over a 6-month period, during which they will self-report all their sports activities as well as any injury in an internet-based database TIPPS (Training and Injury Prevention Platform for Sports). Cox regression analyses will be used to compare injury risk between the study groups and to investigate the association among training, biomechanical and anatomical risk factors, and injury risk.
Ethics and dissemination The study was approved by the National Ethics Committee for Research (Ref: 201701/02 v1.1). Outcomes will be disseminated through publications in peer-reviewed journals, presentations at international conferences, as well as articles in popular magazines and on specialised websites.
Trial registration number NCT03115437, Pre-results.
- sports injury prevention
- footwear
- epidemiology
- impact forces
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Double-blinded randomised controlled trial (assessor and participant blinding) and intention-to-treat analysis.
This study compares two shoe versions with widely differing cushioning properties while remaining within the cushioning range of models available on the market.
A biomechanical analysis will be performed for each participant prior to the 6-month follow-up, which allows to investigate the association between running biomechanics and injury risk in a large cohort of runners.
The running test will be carried out on a treadmill using a standardised protocol, which might not be reflective of the participants’ habitual training conditions.
Introduction
Running is an increasingly popular form of physical activity. From a public health perspective, the promotion of leisure-time running might be a powerful strategy to combat the pandemic of physical inactivity worldwide,1 and its consequence on non-communicable diseases.2 Although regular running activity has a massive beneficial impact on health,3 it also generates a relatively high number of injuries, especially at the lower limb.4 The risk of sustaining a running-related injury (RRI) cancels out part of the benefits of running practice, since the long-term consequences of injury might include, among others, increased risk of osteoarthritis,5 a reduction of physical activity,6 as well as an increase in healthcare costs.7 8 RRI incidence has remained high during the last 40 years, with an overall incidence rate ranging between 18.2% and 92.4%.9 The role of footwear on RRI risk has been strongly emphasised ever since jogging became popular in the 1970s, but there is currently no evidence that developments in running shoe technology and new concepts regularly emerging on the market have helped to tackle the RRI burden.10–12
Most RRI are overuse injuries, as they develop progressively over the kilometres run. The aetiology of these injuries is multifactorial,13 which implies that to understand the mechanisms leading to injury, a holistic approach is warranted, including the study of a large set of potential risk factors. These factors could be classified as being related to training characteristics, running mechanics and anatomy of the runners. Some authors suggested that anatomical and biomechanical factors influence the tolerance to physical strain and thus the relationship between training load and injury occurrence.14 15
Biological tissues such as bones, muscles and tendons can endure a certain amount of stress, provided that the product of stress level (eg, intensity and external load) and the number of repetitions within a certain time period (eg, strides and training sessions) remains below a threshold that is specific to each structure.14 In running, the ground reaction force is the main external stress that acts on the body. Vertical ground reaction force (VGRF) is a biomechanical factor that has been extensively studied in running.16 17 A recent meta-analysis found that the loading rate of the vertical ground reaction force was higher in patients with a history of stress fracture.16 High impact-related variables were shown to increase the risk of bony and soft tissue injuries.17 Moreover, running retraining interventions have proven their efficiency in modifying some VGRF parameters and decreasing pain, which suggest that running retraining represents an interesting paradigm to treat RRI.18–20 Other biomechanical factors such as step length,21 step frequency22 or leg stiffness23 have previously been suggested as potential biomechanical risk factors for RRI, yet no causal relationship has been established.
Since running biomechanics are associated with injury risk, any effect of shoe features on the running pattern and VGRF parameters deserve attention. Given that repetitive loading of the musculoskeletal system is an injury risk factor, cushioning has been one of the most extensively investigated shoe features. The shock absorption properties of footwear mainly result from the materials used in the sole (ie, their type, density, structure and combination) as well as from the geometry of the shoe (ie, the midsole thickness and the design of inserts). One of the most popular approaches has been to change the hardness of the shoe midsole.24–26 Overall, the studies investigating the effect of shoe cushioning on VGRF did not provide consistent results. In theory, peak impact forces should be reduced by softer or more compliant shoes,27 which was indeed confirmed in some in vivo studies.28 29 Conversely, some investigations did not find any effect of cushioning,30 or reported increased peak impact forces in softer shoes.24 31 Recently, a large cross-sectional study revealed that softer midsole hardness was associated with higher vertical force impact peak.24 Unfortunately, very few studies have investigated the association between shoe cushioning and injury risk.32 33 In a previous randomised controlled trial, midsole hardness was not associated with RRI risk. However, the difference in shoe stiffness between the shoe conditions was limited (15%).32 Therefore, the role of shoe cushioning systems in RRI prevention remains unclear.
Body mass index (BMI) has been associated with injury risk in novice34 35 as well as in recreational runners,32 though other results suggest a protective effect of BMI.9 It is common belief that individuals with higher BMI have a higher injury risk, because of the increased physical stress that results from extra body weight. Surprisingly, body mass as such has hardly ever been considered as a potential risk factor for running injury.9
Surprisingly, the literature on the association between single shoe features and RRI risk is still poor.11 36 37 Until now, no relationship has been found between the cushioning properties of modern running shoes and RRI risk,32 but body mass should be taken into account here. Therefore, the main purpose of this study is to investigate the association between shoe cushioning and body mass on the one hand, and RRI risk on the other hand in recreational runners. The secondary aims are to identify which of the running technique-related characteristics (timing variables and VGRF parameters) are associated with injury risk, as well as with the cushioning properties of the shoes. Shoe cushioning will be characterised by the stiffness at the heel (N/mm) and quantified by standardised impact test.38 The following hypotheses (H) will be tested:
H1. Running shoes with greater stiffness are associated with a higher injury risk in leisure-time runners.
H2. High body mass is associated with a higher injury risk in leisure-time runners.
H3. Runners with a high body mass experience a lower injury risk in shoes with greater stiffness.
H4. A higher step length, a lower step frequency, and higher vertical loading rate are associated with a higher injury risk.
H5. Running shoes with greater stiffness will be associated with higher vertical loading rate and a shorter contact time.
H6. High body mass will be associated with higher vertical loading rate, increased contact time, increased duty factor and decreased step frequency.
Furthermore, exploratory risk factor analyses will be performed on the biomechanical variables obtained from the running analysis, anthropometric measurements, running experience and habitual running speed. The focus of the analyses is the effect modification of body mass and other above mentioned risk factors on the association between shoe cushioning and injury risk.
Methods and analysis
Trial design
The design of this study is a randomised controlled trial with a 6-month follow-up and a biomechanical analysis of running pattern at baseline. The study is based on the comparison between two running shoe prototypes, which only differ with respect to the cushioning (ie, stiffness). The cushioning properties of the two shoe versions are within the range of those from available models on the market. Running footwear is provided by a renowned sport equipment manufacturer. The main outcome is RRI (cf. definition in Data on outcome section). The participants as well as the assessors are blinded to group allocation. The design of the trial is illustrated in figure 1. The protocol conforms to the Recommendations for Interventional Trials (SPIRIT) and has been registered on https://clinicaltrials.gov/ (NCT03115437, 11 April 2017).

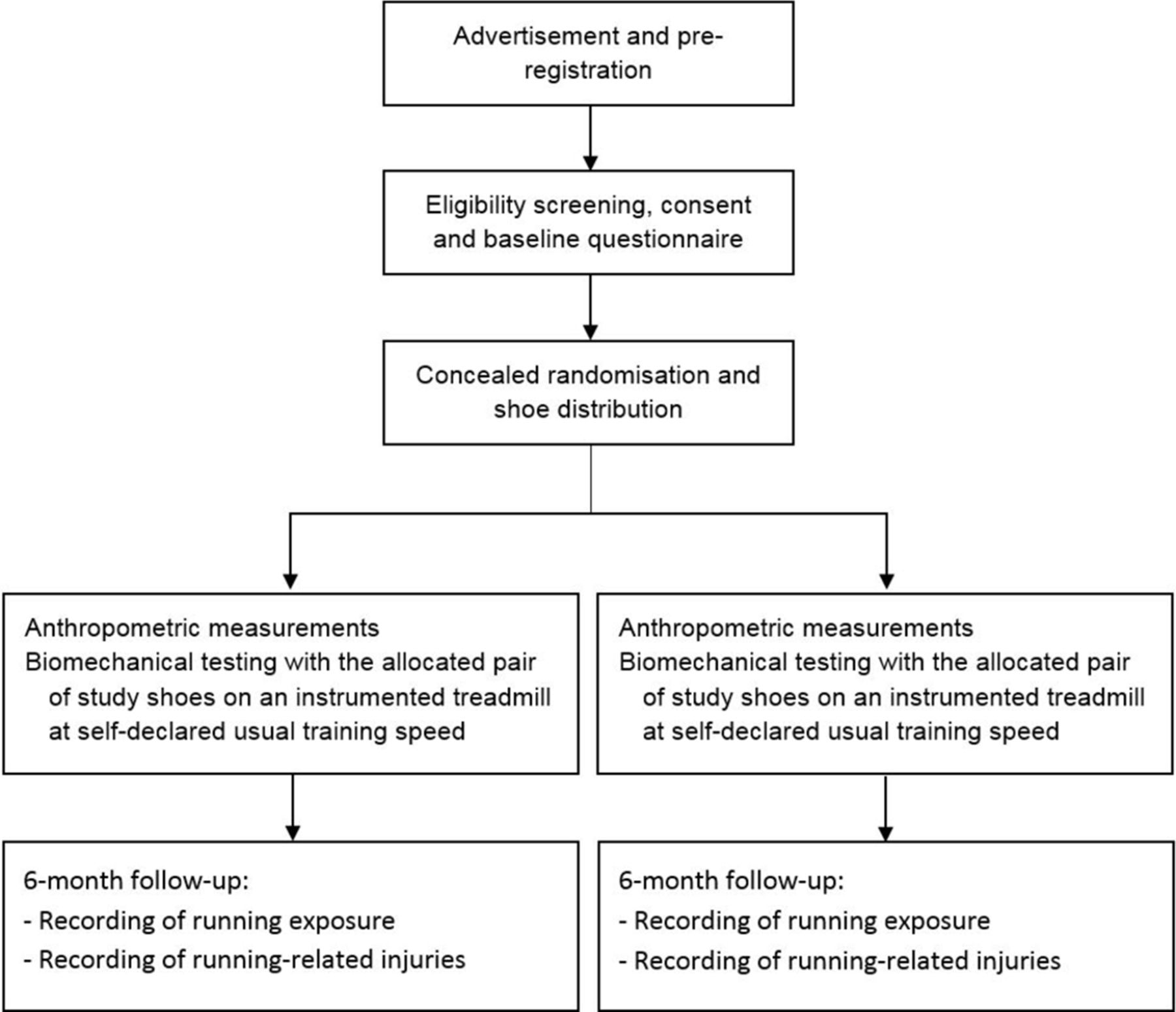{kind=link}
Trial design.
Study population
The target population is leisure-time runners, regardless of running experience, fitness level or body mass. Participants will be recruited through advertisements in local newspapers, social media, running magazines and press releases within the country during the months of September 2017 to January 2018. Healthy volunteers will be considered eligible if they are aged between 18 and 65 years and capable of performing 15 min of consecutive running. Volunteers will be excluded in case of any contraindication to perform running activity, prior (<12 months) surgery or major trauma to the lower limbs or lower back region, any running impeding injury over the previous month, or use of orthopaedic insoles for running activities. Additionally, the participants will have to agree on the following requirements: (1) to practice running at least once a week, (2) to use the provided study shoes for all their running sessions and (3) to report, at least once per week, all sports activities, as well as any injury or pain experienced during the follow-up period on an internet-based database called TIPPS (Training and Injury Prevention Platform for Sports, www.tipps.lu). Volunteers first have to create a personal account on TIPPS, preregister to the study via their personal account, and answer an online inclusion/exclusion questionnaire as well as a baseline questionnaire. Answers to both questionnaires will be assessed by the investigators during the initial visit.
Randomisation
Participants must understand and agree on the randomised design of the study. Those who meet the eligibility criteria and sign the informed consent form will be randomly allocated to one of the two study arms. They will be stratified according to their sex, which is known to influence body mass as well as many other anthropometric characteristics. Therefore, two pre-established randomisation lists (block size=40) will be prepared by a statistician not involved in any other part of the study before the beginning of the recruitment. To ensure allocation concealment, the study groups and shoes will be coded and the randomisation lists will be uploaded in the TIPPS system by an IT specialist who will not be involved in any other part of the study. Then, the TIPPS system will provide the investigator in charge of the recruitment with a study group number for each participant, according to the randomisation lists. The investigator will upload the shoe number according to shoe size chosen and study arm so that a cross-validation will be performed by the electronic system. The investigators in charge of the recruitment, the follow-up and data quality check, as well as the participants, will be blinded regarding the shoe version distributed. The shoe code will be broken after completion of data analysis.
Intervention
The study shoes are prototypes and will be anonymised for the purpose of this trial. The sole of the shoes will be customised so that the two running shoe prototypes will be exactly the same (same midsole, same outsole and same upper), except for their cushioning properties which will differ by about 35%, while remaining within the range of the models available on the market (stiffness: ~53–97 N/mm). The differences in cushioning properties between shoe versions will be created by modifying the midsole material, that is, chemistry, density and therefore the hardness of the ethylene-vinyl acetate (EVA) foam. In order to provide accurate data on the technical specifications (ie, shoe stiffness) of each prototype, a set of 40 shoes (10 pairs per condition) will be tested for stiffness properties by the manufacturer according to a standardised protocol (Impact test: ASTM1614, Procedure A).38
Data collection
Baseline questionnaire
During the online registration process, the participants have to fill in a baseline questionnaire to report information regarding running experience, training habits, recent running competitions performed and injury history. A standardised questionnaire concerning the risk of sports participation must also be completed by the volunteers (online supplementary file 1). Every participant responding positively to any of the symptom-based questions or presenting more than one cardiovascular risk factor will be invited for a clearance check by a sports medical doctor prior to the test.
Supplementary file 1
Biomechanical testing
The biomechanical running analysis will be performed on an instrumented treadmill (M-Gait; Motekforce Link Amsterdam, The Netherlands) in the randomly allocated study shoes. The test (10 min) consists of a 5 min warm-up followed by a 5 min run at the self-declared preferred (habitual) running speed. Two records of 45 s will be obtained at a sampling rate of 1 kHz over the last 2 min of the test. No data will be recorded during the first 8 min, which was shown to be enough time to provoke short-term adaptations of running style with respect to the shoe type.25 39 The main biomechanical variables of interest are presented in table 1.
Biomechanical variables of interest
Anthropometric measures
Body mass and height of each participant will be measured barefoot and in running clothes before the treadmill running test. Also, the participants will have to report their body mass on a monthly basis onto their TIPPS account. Pop-up windows will inform the participants when an update is needed. In clinical settings, leg length is usually assessed as the measure between the anterior superior iliac spine and the medial malleolus (supine position), and is referred to as the ‘direct’ clinical method.40 The measurements will be performed on both legs and the average value will be used for the normalisation of step length. Additionally, the distance between the greater trochanter and the ground will be measured (standing position) to assess leg stiffness.41 Body composition will be evaluated by bioelectrical impedance analysis (Tanita SC-240 MA). The proportion of fat mass will be included in the analyses as a potential confounder for the association between body mass and injury risk.
Data on exposure
Data on running practice will be collected using the TIPPS system.32 42 Required information in the sport activity report includes the type of activity, context, duration, subjectively perceived intensity, distance, shoe pair used, running surface (hard or soft) and whether the participant had experienced any pain during the session forcing him/her to reduce practice volume or intensity, or to interrupt the practice. Session intensity is determined using the Borg’s rating of perceived exertion scale, a subjective 10-point scale.43
Data on outcome
The primary outcome is the first RRI occurring during the follow-up. A consensus definition of RRI in recreational runners has been recently published.44 The definition of RRI is a ‘running-related (training or competition) musculoskeletal pain in the lower limbs that causes a restriction on or stoppage of running (distance, speed, duration, or training) for at least 7 days or 3 consecutive scheduled training sessions, or that requires the runner to consult a physician or other health professional.’
In previous studies, an RRI was defined as ‘any physical pain located at the lower limbs or lower back region, sustained during or as a result of running practice and impeding planned running activity for at least 1 day’ (time-loss definition).15 32 36 37 42 All painful episodes reported by the participants during the follow-up will be assessed by a member of the research team according to each of the two definitions presented above. The consensus definition will be considered as the reference, while a sensitivity analysis will reveal if the results would be impacted when using the former definition of RRI.
Similarly to uploading a training session or competition, the TIPPS provides a complete yet easy to fill in questionnaire when reporting an injury. Information regarding the following is required: injury date, context, sports discipline, injury mechanism (acute or progressive), anatomical location, type of injury, description (free text field) and estimated return date. RRIs will be classified according to the Orchard Sports Injury Classification System version 10 (OSICS-10).45 Injury severity will be measured in days of modified or interrupted training.
Follow-up
Given that the participants are required to practice running at least once a week, individual email reminders will be sent to the participants who do not provide the system with any data for the preceding week. Personal phone calls will be made if the participants do not react to the email reminders and if the reported information in either the training log or on the injury form is found to be inconsistent.
Participants reporting any injury will be systematically contacted by one of the investigators to verify completeness and coherence of the reported data and to check if the episode qualifies as an RRI. Participants who do not complete their entire running calendar with weekly information will be contacted by one of the investigators to ensure that a RRI is not the reason for non-compliance or dropping out. The intervention period will last 6 months, allowing enough time for the participants to cover a large distance with the study shoes.
Sample size
A sample size calculation for Cox regression was used to determine the number of participants needed for the primary hypothesis of the study. With an alpha of 0.05 and a power of 80%, an average injury rate of 30%,15 36 37 an expected HR=1.50 between groups, 50% of participants randomised to each shoe group and an expected drop-out rate of 20%, the total number of participants required is 802.
Statistical analysis
Descriptive data for the personal, anthropometric, biomechanical and training-related characteristics will be presented as count and percentage for dichotomous variables, and as mean and SD, or as median and range, respectively, for normally and non-normally distributed continuous variables. Average sport-related characteristics will be computed for each participant over their specific period of observation. Shock absorption properties (stiffness, N/mm) of the two types of shoes will be compared using a Student’s t test.
Cox proportional hazards regressions will be used to compute the hazard rates in the exposure groups, using first-time injury as the primary outcome. Date of inclusion (baseline evaluation date) and date of injury or of censoring will be basic data used to calculate the time at risk, which is expressed in hours spent running and defined as the time-scale.35 A participant will be right-censored if injury unrelated to running or severe disease caused a modification of the running plan, or at the end of follow-up. Reasons for right-censoring will be reported. The assumption of proportional hazards will be evaluated by log-minus-log plots.
Unadjusted Cox regressions will be performed to present the crude estimates of HRs for shoe model, body mass and other potential risk factors such as running biomechanics variables (see table 1) and training-related characteristics. Body mass is an exposure that can change over time (time-dependent covariate). This means that each participant could move between exposure states continuously (every month in our study). A delayed entry will be used in the unadjusted Cox regression model for body mass.46
Subsequently, the variables with a p<0.2 will be included in the adjusted Cox regression analysis to determine whether shoe cushioning and/or body mass are associated with injury risk, controlling for potential confounders. The recommendation for using at least 10 injuries per predictor variable included in the Cox regression analysis will be strictly followed.47
Finally, to investigate if the effect of shoe cushioning on RRI risk is modified by body mass, a stratified analysis will be performed using the median value of body mass as cut-off. HRs and their 95% CI will be determined within each stratum.48 All analyses will be performed using STATA/SE version 14.
Discussion
It is common belief that shoe cushioning technology protects the runner against harmful consequences of repetitive high-load impacts. Therefore, heavier runners are generally advised to use footwear with adapted shock absorption properties. Surprisingly, few studies have investigated the impact of shoe cushioning on injury risk.32 33 These studies did not provide any evidence on the beneficial effect of increased shock absorption properties. However, none of them included anthropometric measures in their analyses. Also, one study compared different types of insoles added in the shoes,33 while the other compared two versions of a standard running shoe with a limited difference in midsole hardness (~15%).32 Other study limitations such as the sample size (n<250)32 or the study population (Royal Air Force recruits)33 suggest that these results should be interpreted with caution.
The evidence on the association between running shoe cushioning and RRI is still poor and inconclusive. One of the main reasons is the practical constraint of investigations trying to combine biomechanical analyses with a long-term prospective follow-up in a large number of runners.11 This study is the first randomised controlled trial investigating the influence of shoe cushioning on RRI risk including an evaluation of running technique in all participants. The results will provide information on the real benefits provided by additional cushioning as well as on the mechanisms that might explain any potential preventive effect.
Ethics and dissemination
This study will be conducted in accordance with the Declaration of Helsinki and the Medical Research Involving Human Subjects Act. Also, the study protocol (Ref: 201701/02 v1.1) was approved by the National Ethics Committee for Research (www.cner.lu). Written informed consent will be obtained from all participants (online supplementary file 2). All collected data will be stored electronically using a coding system. This will ensure that the data is used in the strictest confidence and will not reveal the identity of the participants. Collected raw data will not be passed on to unauthorised third parties. Results presented or published in articles and reports will be depicted in general terms, to maintain participant anonymity. Electronic data will be stored on a secure server in data files only accessible to the project leader and coinvestigators of the project. A notification of this study was sent to the National Data Protection Agency. Study results will be submitted for publication in peer-reviewed journals and for presentation at international conferences. Furthermore, we aim to disseminate our results through popular specialised magazines and websites.
Supplementary file 2
References
Footnotes
Contributors LM, ND, AU and DT contributed to the study conception and study design. LM is the main investigator, wrote the article with input from other investigators and will be responsible for the acquisition and analysis of the data. ND will be responsible for the shoe design, production and testing. LM and DT will be responsible for data interpretation and manuscript drafting. ND, AU and DT commented on the various versions of the study protocol. All authors approved the final manuscript.
Funding This study is cofunded by Decathlon, Villeneuve d’Ascq, France, and by the Ministry of Higher Education and Research of Luxembourg.
Competing interests A research partnership agreement was signed between Decathlon and the Luxembourg Institute of Health (LIH). ND is employed at Decathlon SA. Decathlon will not be involved in the collection, management, analysis and interpretation of data. LM, DT and AU may not gain or lose financially from the results of the study in any way.
Patient consent Obtained.
Ethics approval All procedures were approved by the National Ethics Committee for Research (Ref: 201701/02 v1.1).
Provenance and peer review Not commissioned; externally peer reviewed.