Article Text

Abstract
Objectives This systematic review aimed to assess the clinical evidence supporting the use of herbal medicines (HMs) for the treatment of otitis media with effusion (OME).
Design Systematic review and meta-analysis.
Data sources MEDLINE, EMBASE, Cochrane Library, AMED, CINAHL and three trial registries were searched up to January 2015. We also searched five Korean medical databases (KoreaMed, RISS, OASIS, DBPIA and KISS) and three Chinese databases (CNKI, Wanfang and VIP).
Study eligibility criteria This study included randomised clinical trials that reported the effects of HM for OME. The primary outcome was the complete resolution of OME at 2 or 3 months post randomisation. Secondary outcomes included the partial or complete resolution at all possible time points and hearing test. Three authors independently screened the titles and abstracts, selected studies and extracted the data relating to trial quality, characteristics and results.
Results A total of 2141 potentially relevant studies were identified, of which 17 randomised clinical trials met our inclusion criteria. Most were evaluated as having a high or unclear risk of bias. Tongqiao tablets, Tongqiao huoxue decoctions and Tsumura-Saireito were associated with a lower complete or partial resolution rate when compared with conventional medicines (CMs) (p=0.02, p=0.0001, and p=0.04, respectively), and similar outcomes were observed with Huanglong tonger pills, Erzhang decoctions and Shenling baizhu powder when combined with CM versus CM alone (p<0.00001, p=0.02, and p=0.05, respectively). Tongqiao huoxue decoction plus CM appeared to be more effective than CM in terms of improving the pure tone threshold levels (p=0.0007). Tsumura-Saireito was found to affect the proportion of patients with normalised tympanometry (p=0.03).
Conclusions Despite some indications of potential symptom improvement, the evidence regarding the effectiveness and efficacy of HMs for OME is of poor quality and therefore inconclusive.
Protocol registration number CRD42013005430.
- Otitis Media with Effusion
- Systematic Review
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review to provide an evidence of the use of herbal medicine (HM) for the treatment of otitis media with effusion (OME).
Our systematic review involved an unbiased search of various databases without language restriction.
Our systematic review will give readers the opportunity to access studies originally published in East Asian languages that they would otherwise be unable to read.
Despite some indications of potential improvement of symptoms, the evidence regarding the effectiveness and efficacy of HMs for OME is of poor quality and therefore inconclusive.
Introduction
Otitis media with effusion (OME) is characterised by middle ear effusion without symptoms and signs of acute inflammation.1 OME occurs commonly during childhood, affecting 50–90% of children at least once by 5 years of age.2 ,3 At least 25% of OME episodes persist for more than 3 months, and may be associated with hearing loss, balance problems, poor school performance, behavioural problems, ear discomfort, recurrent acute otitis media and reduced quality of life.4–7
The most widely used therapeutic agents for OME attempt to mitigate symptoms and eliminate effusion. The therapeutic agents include antihistamines, decongestants, steroids and antibiotics; however, antihistamines, decongestants and topical nasal steroids are known to be ineffective.8–10 Antibiotics are not recommendable because their adverse effects outweigh their small benefit.11 Short-term treatment with oral steroids is effective, but extending the treatment for longer than 2 weeks has no added benefit.12 The most recommended treatment is ventilation tube insertion, which is considered when OME persists after a 3-month period of watchful waiting.13
Oral administration of herbal medicines (HMs) has been broadly used to manage OME in East Asian countries.14 According to animal experiments involving herbal preparations, a Ginkgo leaf parenteral solution conferred protection against oxidative injuries in rats with otitis media by increasing antioxidant and immune activity,15 whereas the HM Saireito induced much milder pathological changes in the tubotympanum and stimulated ciliary activity in guinea pigs.16 Additionally, the HM, Kami-hyunggyeyungyotang was found to induce antiallergic and antioxidant effects by regulating the production of immunoglobulin G, interleukin-8, cytokines, tryptase, superoxide dismutase and transforming growth factor-β1 in patients with recurrent OME.17–20
Several randomised controlled trials (RCTs) have evaluated the effects of HM on OME. Unfortunately, these studies have reached conflicting conclusions, with only some demonstrating the clinical benefits of HM as a main or adjunct treatment. In this review, we aimed to systematically accumulate evidence regarding the safety and effectiveness of HM for patients with OME.
Methods
Protocol and registration
This systematic review was registered in an international prospective register of systematic reviews under the registration number PROSPERO 2013: CRD42013005430 (available from: http://www.crd.york.ac.uk/prospero/display_record.asp?ID=CRD42013005430#.VWcfac_tlBc).
Data sources and searches
The following electronic databases were searched up to January 2015: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, AMED and the Cumulative Index to Nursing and Allied Health Literature. We also searched five Korean medical databases (KoreaMed, RISS, OASIS, DBPIA and KISS) and three Chinese databases (CNKI, Wanfang and VIP). Additionally, we sought on-going studies in the meta-Register of Controlled Trials (http://www.controlled-trials.com/mrct), Clinical trials.gov (http://www.clinicaltrials.gov) and the WHO International Clinical Trials Registry platform (http://apps.who.int/trialsearch/), all of which list on-going trials. No limits or filters were placed on the searches to ensure maximal sensitivity, and no language or publication type restrictions were applied. The MEDLINE database search strategy is presented in online supplementary appendix 1. Similar search strategies were applied for the other databases.
supplementary appendix 1
Study selection
Study selection was based on the following criteria:
Type of study: RCTs that reported the effects of HM on OME were included. Trials that did not provide detailed information (eg, dosage or comparison data) were excluded.
Type of participant: Studies that evaluated patients with a diagnosis of OME were included. We excluded studies of patients in whom ventilation tubes had been placed, those with an anatomical deformity or those with other chronic immunocompromised states.
Type of intervention: We included trials that evaluated orally administered HM alone or in combination with a conventional medicine (CM) versus CM alone. We included all types of herbal formulations. Trials that incorporated herbal decoctions but did not provide detailed information such as the herbal dosage, preparation, or HM addition and subtraction criteria were excluded. However, we included trials using HMs manufactured by pharmaceutical companies, regardless of sufficient herbal prescription and dosage information.
Type of comparison: Both active control and placebo were acceptable.
Types of outcome measures: The primary outcome was the complete resolution of OME at 2 or 3 months post randomisation (resolution in the affected ear in participants with unilateral OME at randomisation and resolution in both ears of those with bilateral OME). We also planned to evaluate the partial or complete resolution of OME at all possible time points, hearing loss duration, language and speech development, cognitive development, ventilation tube insertion, tympanic membrane sequelae, reduction in OME complications, quality of life and adverse effects likely related to treatment. All studies including any of the above outcome measures were evaluated.
Data extraction and quality assessment
Two authors (MJS, Y-EK) independently screened the titles and abstracts, selected the studies and extracted the data from studies in international and Korean databases using a standard eligibility form; two other authors (MJS, SC) performed the same tasks in Chinese databases.
Data concerning the patient population characteristics, HM treatment regimens and comparators, reported outcomes and assessment modality (if reported) were collected from each trial. The arbitrator (YHK) made decisions regarding study selection and extraction when a consensus could not be reached. The risk of bias in the eligible studies was independently assessed according to the criteria described in the Cochrane Handbook V.5.1.0.21 The quality of each study was classified as a low, unclear or high risk of bias. Any differences in opinion were resolved via discussion or arbitration involving a third author.
Statistical analysis
We used RevMan 5.3.5 (Cochrane Informatics and Knowledge Management Department; available at http://tech.cochrane.org/revman/download) to conduct the statistical analysis. Dichotomous data were expressed as risk ratios (RRs) with 95% confidence intervals (CIs), whereas continuous data were presented as mean differences (MDs) with 95% CIs. We converted other forms of data into either RRs or MDs. The level of significance was set at 0.05. Heterogeneity was assessed using the I2 statistic to quantify inconsistency among the included studies in the meta-analysis.
where Q is the χ2 statistic and df is its degrees of freedom.
An I2 value >50% was considered indicative of substantial heterogeneity according to Cochrane guidelines.21 A Z-test was used for testing overall effects in the meta-analysis. Funnel plots were planned to detect publication bias if more than 10 trials reported the same outcomes. If data were available, a predefined subgroup analysis was planned to evaluate heterogeneity. The predefined subgroup analysis was planned to evaluate the following information: (1) Laterality of OME: bilateral OME versus unilateral OME, (2) Duration of OME: any duration of OME versus persistent OME (lasting for more than 2 or 3 months), (3) Duration of treatment, (4) Type of HMs, (5) Type of control and (6) Type of age group.
If the included studies were sufficient to perform a sensitivity analysis, analyses according to sample size (>40 or <40 participants) and risk of bias (low risk of bias in allocation concealment or the blinding participants/assessors) were planned.
Results
Study selection and description
Our search generated a total of 2141 potentially relevant studies, from which 80 duplicated and 1963 non-relevant studies were excluded after screening the titles and abstracts. Subsequently, 98 full-text articles were reviewed, of which 17 met our eligibility criteria. Five RCTs did not meet our inclusion criteria; four trials included patients who inserted ventilation tubes and one trial evaluated combination therapy of HM plus microwaves.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of our search process and study selection is shown in figure 1.

PRISMA flow diagram.
Of these trials, 1622–37 were conducted in China; of these, 1522–33 ,35–37 were published in Chinese and 134 was published in English. One additional trial38 was conducted in Japan and published in Japanese. In total, 3161 participants with OME were involved in the 17 trials. Fifteen trials22–30 ,32–34 ,36–38 involved participants younger than 18 years, and two36 ,38 involved only children under 7 years of age.
Seven trials24–26 ,28 ,30 ,34 ,38 compared HM treatments with CMs; the remaining trials compared combination treatments involving HM and CM with CM alone. Two trials31 ,34 reported data concerning the complete resolution of clinical symptoms and signs at 2 or 3 months post randomisation. All included trials reported either complete or partial resolution at various time points. Only five trials28–30 ,34 ,38 reported information about adverse events and none of the trials mentioned ethical issues.
Key data points from the included RCTs are summarised in table 1.
Basic characteristics of the included studies
Intervention
Five types of HM prescriptions were evaluated in the included trials, including herbal granules manufactured by pharmaceutical companies (four trials), practitioner-prescribed herbal decoctions (nine trials), pills (two trials), tablets (one trial) and capsules (one trial). No trials described the quality standards of the herbal preparations. Among our included trials, two investigated several different herbal prescriptions that had been prescribed individually. In a majority of the included studies, a 2-week treatment course was provided (range: 1–4 weeks). Shenling baizhu powder, Huanglong tonger pills and a Tongqiao huoxue decoction were each investigated in more than two studies. Details regarding the HM regimens used in the included trials are shown in online supplementary appendices 2 and 3.
supplementary appendix 2
supplementary appendix 3
Oral antibiotics were mainly used as control interventions; other conventional treatments included oral antihistamines, prednisone and mucolytic or secretolytic agents that were provided to either the control group alone or to both groups.
Risk of bias in the included studies
We attempted to contact the authors of all included trials for clarification and details. However, few trial reports provided contact details and no authors could be contacted, despite contact attempts in Chinese via email.
Overall, the studies were found to have a high risk of bias. Most studies featured a randomised design but provided inadequate descriptions of randomisation, allocation concealment and outcome assessor blinding. Only one trial34 reported the use of a random number table for random sequence generation, whereas the remaining trials22–33 ,35–38 did not report any randomisation details. None of the trials described their allocation concealment method. Furthermore, only one trial34 incorporated a double-blind design; the remaining studies22–33 ,35–38 did not appear to implement both patient and practitioner blinding. None of the trials reported details regarding outcome assessor blinding.
Not all trials provided complete outcome data (eg, numbers of participants who were included, finished treatment and dropped out). Selective outcome reporting was not clearly evaluable because we could not find registered protocols for all included studies. In addition, not all trials reported statistical issues such as baseline imbalances and sample size calculations to ensure sufficient statistical power. Only one trial34 reported conducting an intention-to-treat or per-protocol analysis as an effectiveness evaluation. The risk of bias assessment is shown in figure 2.

Risk of bias in the included randomised controlled trials.
Outcomes
Given the heterogeneity of the HM treatment and control groups in the included trials, we could only synthesise data from two trials into a meta-analysis. The effect estimates of the included trials are shown in table 2, and meta-analysis results are indicated in figure 3.
Estimated effects of herbal medicine on improvements in the clinical outcomes of patients with otitis media with effusion
{kind=link}
{kind=link}
{kind=link}
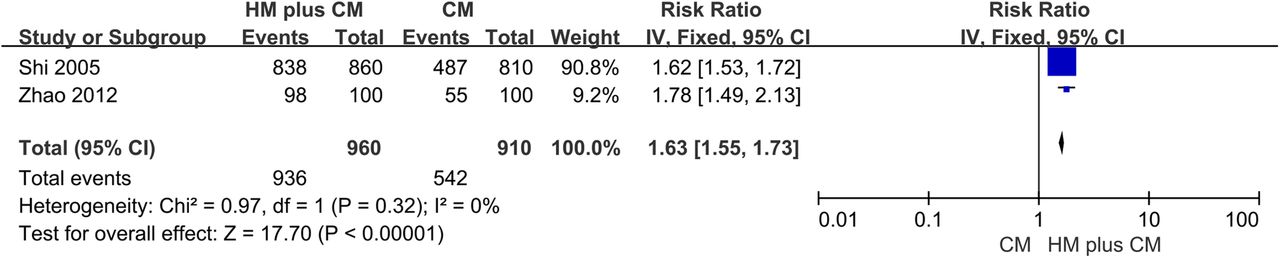
Forest plot of the complete resolution rate achieved with the Huanglong tonger pill.
Complete or partial resolution
Complete or partial resolution was evaluated by two or more of combined assessment of the presence of symptoms, otoscopy and tympanometry in all studies. All trials22–38 evaluated either complete or partial resolution at various time points. Two trials31 ,34 assessed the complete resolution of OME at 2 or 3 months post randomisation, and showed borderline significant improvements with Qingqiao capsule (RR: 2.33, 95% CI 0.98 to 5.53, p=0.05),34 but no differences with an unnamed HM (RR: 1.01, 95% CI 0.51 to 2.00, p=0.98)31 between the treatment groups.
Two trials33 ,36 estimated the complete resolution rate within 1 week and demonstrated statistically significant improvements with the Huanglong tonger pill (RR: 2.12, 95% CI 1.94 to 2.31, p<0.00001) or Erzhang decoction (RR: 1.65, 95% CI 1.07 to 2.54, p=0.02) plus CM versus CM alone. Of the eight trials22 ,23 ,27 ,29 ,31–33 ,37 that evaluated effects between 1 and 2 weeks, three29 ,33 ,37 reported favourable effects with HM plus CM versus CM alone. Compared with CM alone, the Huanglong tonger pill plus CM33 ,37 yielded significant effects after a 10-day treatment course (RR: 1.63, 95% CI 1.55 to 1.73, p<0.00001), and one trial29 reported favourable effects of HM plus CM versus CM alone (RR: 3.15, 95% CI 1.37 to 7.26, p=0.007). No significant improvements were observed in the other trials.22 ,23 ,27 ,31 ,32
Of the five trials25 ,26 ,28 ,30 ,35 that evaluated the effects of treatment between 2 and 4 weeks, one28 reported that Tongqiao tablets were superior to amoxicillin plus terfenadine (RR: 3.05, 95% CI 1.23 to 7.54, p=0.02), and another trial30 reported favourable effects with HM when compared with cephradine plus prednisone plus mucosolvan (RR: 1.43, 95% CI 1.11 to 1.84, p=0.006). Two trials25 ,35 that compared HM plus CM with CM alone reported statistically marginal effects (p=0.05). However, two additional trials that compared HM with CM did not report statistically significant improvements.25 ,26 In one trial38 that estimated partial OME resolution after a 4-week treatment course, Tsumura-Saireito was found to have a more favourable effect than cepharanthin (RR: 2.33, 95% CI 1.03 to 5.30, p=0.04). After 6 weeks, a Tongqiao huoxue decoction24 was superior to roxithromycin plus prednisolone acetate (RR: 3.35, 95% CI 1.80 to 6.24, p=0.0001).
Improvements in hearing
Three trials22 ,34 ,38 provided data regarding improvements in hearing; of these, two trials22 ,38 measured hearing threshold level differences before and after treatment using pure tone audiometry, and one trial34 assessed the hearing restoration rate and elapsed time using pure tone threshold results but did not include detailed criteria. Two additional trials34 ,38 evaluated improvements in clinical hearing symptoms, and one trial38 determined that an improvement in pure tone audiometry exceeding 15 dB indicated efficacy.
In three trials,22 ,34 ,38 the Qingqiao capsule34 yielded significant improvements in the restoration rate (RR: 1.61, 95% CI 1.12 to 2.32, p=0.010) and time (MD: −1.70, 95% CI −2.50 to −0.90, p<0.0001) relative to the cefaclor capsule. The Qingqiao capsule also yielded favourable effects on the proportion of patients who achieved hearing improvements (RR: 1.69, 95% CI 1.04 to 2.75, p=0.03) and the assessed clinical hearing restoration time (MD: −1.80, 95% CI −3.26 to −0.34, p=0.02). Compared with CM alone, the Tongqiao huoxue decoction plus CM26 significantly reduced the hearing threshold levels (MD: 5.80, 95% CI 2.44 to 9.16, p=0.0007), and Tsumura-Saireito38 was found to affect the proportion of patients with normalised tympanometry (RR: 9.14, 95% CI 1.18 to 70.61, p=0.03). In contrast, Tsumura-Saireito38 had non-significant effects on differences in the hearing threshold level (MD: 3.30, 95% CI −1.88 to 8.48, p=0.21) and the proportion of patients who achieved hearing improvements (RR: 1.80, 95% CI 0.68 to 4.78, p=0.24). Detailed data for hearing thresholds before and after therapy are presented in online supplementary appendix 4.
supplementary appendix 4
Adverse events
Only five of the included RCTs28–30 ,34 ,38 mentioned adverse events. None of the RCTs reported any serious adverse effects. Three RCTs28 ,29 ,38 reported no adverse effects during the study period, whereas one RCT34 reported that two patients in the control group suffered from nausea, vomiting, diarrhoea and urticaria, with no reported adverse effects in the intervention group. One trial30 reported the following: one case of headache and dizziness in the intervention group and two cases of headache and dizziness, two of nausea and vomiting and one of xerostomia in the control group.
Other outcomes
We had planned to analyse the effects of treatment on language and speech development, cognitive development, ventilation tube insertion, tympanic membrane sequelae, reductions in OME-associated complications and the quality of life but were unable to determine these results because of a lack of data. Given the inconsistency among the included trials, we were also unable to conduct our planned subgroup and sensitivity analyses.
Discussion
Summary of the main results
From the 17 included RCTs, we determined that several HM formulations (Tongqiao tablets, unnamed HM, Tongqiao huoxue decoction, Tsumura-Saireito) appeared to be more effective than CM in terms of the complete or partial resolution rates of clinical symptoms and signs. Similar effects were observed when Huanglong tonger pills, an Erzhang decoction, two unnamed HM and Shenling baizhu powder were combined with CM and compared with CM alone. Other HM prescriptions and combination therapies involving HM and CM did not yield favourable effects when compared with CM alone.
In the three RCTs that assessed hearing symptoms, Qingqiao capsules were associated with a statistically significant improvement in hearing symptoms when compared with CM. Furthermore, a Tongqiao huoxue decoction plus CM appeared to be more effective than CM alone in terms of improved pure tone threshold levels. These results suggest that each HM prescription has a different bioactive effect with respect to OME. Finally, no severe adverse effects were observed in the HM groups, suggesting that HM may be safe for patients with OME.
Overall completeness and applicability of evidence and implications for clinical practice
Although several HM formulations appeared to be potentially effective against OME, we were unable to draw conclusions regarding the applicability for clinical practice because of the lack of evidence, low quality of the available evidence and heterogeneity of HMs included in this study. By including all types of HMs, we were able to provide overview of the HMs prescribed to OME patients, but we were unable to synthesise the evidence for the use of HM in OME.
Although such limitations do not always mean that the treatment is ineffective, they might indicate that the effectiveness has not been adequately investigated. Larger, more rigorous and adequately powered multicentre randomised clinical evaluations of HM for OME are thus warranted.
Quality of evidence and potential biases in the review
All trials were methodologically weak and had a high risk of bias. Only one of the 17 trials provided information about the randomisation method and implemented double blinding. As the other 16 trials used different types of CM with different appearances, patient and practitioner blinding might have been impossible.
Although we were unable to find protocols for the included trials, selective reporting bias might have been present, as none of the trials reported losses to follow-up and only five trials reported adverse effects. In addition, the sample size calculation was potentially defective because statistical power could not be guaranteed for the studies. In addition, inadequate information was provided about the quality standards used during HM manufacturing, and therefore the ingredients and their compositions were not standardised. All of these potential biases might have interfered with the true evaluation of these interventions.
Comparison with other reviews
No previous reviews of oral administration of HM for OME were identified in peer-reviewed journals. However, one review evaluated CM and complementary medicine for the treatment of paediatric otitis media. Levi et al39 reported that topical HM ear drops might be beneficial, although the efficacy of this treatment was unclear because of variations in the compositions of these drops (usually a combination of marigold (Calendula flores), garlic (Allium sativum), mullein (Verbascum thapsus), St. John's wort (Hypericum perforatum), lavender and vitamin E).
Implications for research
We propose the following suggestions for future research endeavours:
(1) Development of an adequate placebo: The unique formulations of HMs are the main cause of inadequate blinding. For example, even though a double-blinded study might administer treatments in the same shape and format for comparative purposes, the treatments might have different flavours, potentially leading to the failure of participant and practitioner blinding. This is a fundamental challenge of clinical trials of HM. The development of placebos identical in shape and flavour to the experimental HM is an important area of further research.
(2) Development of HM dosage guidelines: HM dosages varied among the included trials, and of the 15 trials that involved participants younger than 18 years, only two mentioned HM dosage rules for paediatric participants (ie, ‘half dose for those younger than 14 years’ or ‘adjust dosage according to age’). Appropriate HM dosages did not appear to be calculated according to the participants' ages and weights, and this omission might have been because of the lack of appropriate herbal prescription dosage guidelines. Further studies to investigate the adequate dosages of HMs based on pharmacokinetic and pharmacodynamic data are greatly needed.
(3) Evaluation of drug compliance: As HMs have distinctive flavours, drug compliance might also have affected the study outcomes. In future, drug compliance should be evaluated.
Conclusions
There are some indications that several HM formulations could potentially improve the rate of complete sign and symptom (including hearing symptoms) resolution among patients with OME. However, given the low quality of evidence, these results should be interpreted with caution. Further investigation of the effects and safety of HM for patients with OME through rigorously designed randomised trials should be conducted.
Acknowledgments
This study was supported by a grant from the Korea Institute of Oriental Medicine (K16124). This review protocol was published in the BMJ Open Journal (http://bmjopen.bmj.com/content/4/2/e004095.full).
References
Footnotes
Contributors YHK contributed to the study conception. MJS drafted the manuscript, which was revised by all authors. The search strategy was developed by all authors and executed by MJS, SC and Y-EK, who screened and selected the potential studies for inclusion. MJS, SC and Y-EK performed the data extraction and bias risk assessment. YHK guarantees this work. All authors have read and approved the final manuscript.
Funding Korea Institute of Oriental Medicine (grant number K16124).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.