Article Text

Abstract
Objectives To systematically review studies of the epidemiology of tinnitus and hyperacusis in children and young people, in order to determine the methodological differences implicated in the variability of prevalence estimates and the influence of population characteristics on childhood tinnitus and hyperacusis.
Data sources Articles were retrieved from PubMed, EMBASE and Scopus databases and from the relevant reference lists using the methods described in the study protocol, which has previously been published. Reporting Items for Systematic Review (PRISMA) guidelines were followed.
Eligibility criteria Studies addressing childhood prevalence, for example, children and young people aged 5–19 years.
Data selection 2 reviewers independently assessed the studies for eligibility, extracted data and assessed study consistency. Owing to the heterogeneity in the methodologies among the reported studies, only narrative synthesis of the results was carried out.
Results Having identified 1032 publications, 131 articles were selected and 25 articles met the inclusion criteria and had sufficient methodological consistency to be included. Prevalence estimates of tinnitus range from 4.7% to 46% in the general paediatric population and among children with normal hearing, and from 23.5% to 62.2% of population of children with hearing loss. Reported prevalence ranged from 6% to 41.9% when children with hearing loss and normal hearing were both included. The prevalence of hyperacusis varied from 3.2% to 17.1%.
Conclusions Data on prevalence vary considerably according to the study design, study population and the research question posed. The age range of children studied was varied and a marked degree of variation between definitions (tinnitus, hyperacusis) and measures (severity, perception, annoyance) was observed. The lack of consistency among studies indicates the necessity of examining the epidemiology of tinnitus and hyperacusis in children and adolescents with a set of standardised criteria.
Trial registration number CRD42014013456.
- Prevalence
- Tinnitus
- Hyperacusis
- Severity
- Child
- Adolescent
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Clearly established purpose, as well as a systematic and transparent approach.
Comprehensive search strategy.
During the article selection process, language was limited to English, German and Scandinavian languages.
Search and data extraction conducted independently by two authors.
This study gathered published articles to determine the prevalence of tinnitus and/or hyperacusis across studies. This knowledge is important in order to know the extent of the problem.
Introduction
The prevalence of tinnitus in children has been studied in several articles with reports ranging from 7.5% to 60%.1 Tinnitus is reported to be more common among children with hearing impairment compared with children with normal hearing.2 In general, studies indicate tinnitus to be relatively common in childhood, but tinnitus impact seems to be lower in children than among adults and it is unusual to see adults with tinnitus that has persisted since childhood.2 ,3 It is rare for a child to present with tinnitus spontaneously.4 Some researchers suggest that the prevalence figures in children are underestimates owing to communication difficulties, but on the other hand, it can be argued that children over-report tinnitus when questioned in an effort to please the questioner.5 A small-scale survey by the British Tinnitus Association in the UK has shown that generally paediatric tinnitus services were multidisciplinary.6
There is limited literature looking at the effects of tinnitus on the health and well-being of children.7 On a small population of 24 children aged 7–17 years, who were referred to a psychological clinic because of tinnitus, Kentish et al8 found that insomnia, anxiety and worry, listening and attention problems were the main psychological factors associated with tinnitus symptoms. The group of children with normal hearing was more affected by tinnitus and presented higher levels of anxiety than those with impaired hearing. Seventy-one per cent of the children had developed coping strategies by the initial assessment to deal with the tinnitus-like sounds, such as watching or listening to TV/music/radio, in order to distract from the tinnitus or to read, or to use hearing aids. Slightly more than half of the children reported specific concerns about tinnitus; for example, it can damage or reflect a worsening of their hearing. The parents generally shared this fear.
Baguley et al9 reported that the number of children seen with a primary symptom of tinnitus represents just a small fraction of the total number of patients seen for tinnitus in four European clinics with an established and internationally known tinnitus programme. Low referral may partly reflect a low number of children seeking help, or the possibility that there are few services for children to be referred to.2
Data on hyperacusis among children are sparse.10 Comparison of prevalence studies in this area is as problematic as with tinnitus studies due to the complexity and inadequacy of terminology and definitions.10
The present systematic review was undertaken to determine the extent to which a reliable view of the epidemiology of childhood tinnitus and hyperacusis can be held in the presence of these methodological challenges. A reliable estimate would underpin the commissioning, provision and design of clinical services for such patients.
Objectives
The following objectives were addressed to:
Determine the methodological differences implicated in the variability of prevalence estimates, including those deriving from the tinnitus/hyperacusis question used, approaches to collecting reliable answers and the characteristics of the tinnitus/hyperacusis sensations.
Systematically review the influence of population characteristics (age, gender, hearing ability, comorbidity) on childhood tinnitus and hyperacusis.
Assess the methodological heterogeneity across studies and to determine if pooling the studies is feasible.
Methods
Study protocol
We previously published the study protocol as an open access article10 and registered the systematic review in Prospero (registration number CRD42014013456). We briefly describe the methods and the modifications that occurred during the review process.
Changes in the review process
We decided to include incidence studies in the review process to determine the extent to which this has been studied in the included articles.
In the study protocol, it was stated that articles should be included in the review if they were original papers from peer-reviewed scientific journals. During the study, we observed that two conference proceeding articles were frequently cited and hence these were included in our review, namely Graham11 and Stouffer et al.12
The aim of the study and the objectives were modified in order to provide methodological consistency and a clear focus.
Studies were rated on their relevance to the present study objectives, and not, as stated in the study protocol, according to an assessment of study quality. On reflection, the consideration of study quality as described in the protocol was more related to consistency issues associated with the methodology of the studies. Therefore, it was decided to use the term methodological consistency instead of study quality as described in the protocol.10 A response to the diversity encountered in the articles identified was to look for common themes. Therefore, the studies were divided into the following population categories, normal hearing participants and hearing-impaired participants, to achieve a consistent way to compare them.
Selection criteria
Articles were screened and selected according to the research question and PICOS criteria.13 Studies were included if they were original articles from peer-reviewed scientific journals published in English, German, Swedish, Norwegian or Danish (except for Graham11 and Stouffer et al12 as indicated above). PICOS were: population, children and young people aged 5–19 years (if the age included in the studies felt outside this range, the study was included if the prevalence was rated separately for different ages); intervention, none; comparisons, none; outcomes: (point) prevalence of tinnitus and/or hyperacusis, consequences of tinnitus and/or hyperacusis; study design, all studies excluding case series and case studies.
Checklists
Three checklists were created especially for this review, and were presented in the study protocol. These checklists related to the description of studies, their methodological consistency (quality checklist in the protocol10) and their results.
Searching methods for identification of studies
One author (SNR) searched PubMed, EMBASE and Scopus from database inception to 26 August 2015 using the search matrices below from the study protocol.
PubMed search
The matrix includes the relevant diagnoses (first category) and the review topics of the studies (second category). As PubMed uses specific terms for various age groups, filters were used in the search to arrive at the right population. Search filters enable restricting the search by date, article type and other characteristics. In this case, age filters from the ages filters list in PubMed were used.
The terms ‘tinnitus’ and ‘hyperacusis’ were both MeSH words. The term ‘misophonia’ was not found in MeSH, so it was searched as a text word (all fields). The term ‘phonophobia’ was linked to the MeSH term ‘hyperacusis’ but was also searched as a text word.
The search details for:
Tinnitus: ‘tinnitus’[MeSH terms] OR ‘tinnitus’ [all fields];
Hyperacusis: ‘hyperacusis’[MeSH terms] OR ‘hyperacusis’ [all fields];
Misophonia Misophonia[All Fields];
Phonophobia: ‘hyperacusis’[MeSH terms] OR ‘hyperacusis’ [all fields] OR ‘phonophobia’[all fields];
OR were used to find articles in which either term appeared.
Truncation was not used in the PubMed search to limit the risk of losing relevant hits. After making the search in each category, the findings were combined with the operator AND to find articles in which both terms have appeared.
Search: ((‘hyperacusis’[MeSH terms] OR ‘hyperacusis’ [all fields]) OR (‘tinnitus’[MeSH terms] OR ‘tinnitus’ [all fields]) OR misophonia[all fields] OR (‘hyperacusis’[MeSH terms] OR ‘hyperacusis’[all fields] OR ‘phonophobia’(all fields])) gave a total of 10 496 hits. Second category: ((‘epidemiology’[subheading] OR ‘epidemiology’[all fields] OR ‘epidemiology’[MeSH terms]) OR (‘epidemiology’[MeSH terms] OR ‘epidemiology’[all fields] OR ‘epidemiologic’[all fields]) OR (‘epidemiology’[subheading] OR ‘epidemiology’[all fields] OR ‘prevalence’[all fields] OR ‘prevalence’[MeSH terms]) OR (‘epidemiology’[subheading] OR ‘epidemiology’[all fields] OR ‘morbidity’[all fields] OR ‘morbidity’[MeSH terms]) OR (‘epidemiology’[subheading] OR ‘epidemiology’[all fields] OR ‘occurrence’[all fields] OR ‘epidemiology’[MeSH terms] OR ‘occurrence’[all fields]) OR (‘epidemiology’[subheading] OR ‘epidemiology’[all fields] OR ‘incidence’[all fields] OR ‘incidence’[MeSH terms])).
The search was carried out individually for each category and was then combined. The first category gave a total of 10 792 hits, and the second category had 2 721 630 hits. Combining the first and the second category reduced the findings to 1757 hits, and using the filters gave a total of 559 hits from the PubMed search.
EMBASE search
The matrix includes the relevant diagnoses (first category), the review topics of the studies (second category) and the relevant population groups (third category).
After making the search in each category, the findings were combined with the operator AND to find articles in which all the terms appeared.
In EMBASE, the thesaurus for ‘tinnitus’ included different spelling (‘tinnitis’) and synonym (‘ear buzzing’). In this search, ‘related terms’ was included, which gave two more hits than without this option.
The term ‘hyperacusis’ was mapped to the subject heading ‘loudness recruitment’ (which we could not use for our aim), so it was needed to search ‘hyperacus*’ as an ‘all fields’ search. Truncation (operator *) was used to find alternate endings. There were no differences in the received results searching ‘keyword’ versus ‘all fields’ search, so ‘all fields’ search was used.
First category: (tinnitus OR hyperacus* OR hyperacous* OR misophonia OR phonophobia).
Second category: (epidemiolog* OR prevalence OR morbidity OR occurrence OR incidence).
Third category (infant OR child OR children OR adolescent OR adolescence OR young adult).
The first category gave a total of 18 324 records, and the second category had a total of 2 425 734 records.
The third category had 3 048 075 hits. Combining the three categories gave a total of 584 hits from the EMBASE search.
Scopus search
The matrix includes the relevant diagnoses (first category), the topic of the studies (second category) and the relevant population groups (third category).
In Scopus, an advanced search using truncation was made. After making the search in each category, the findings were combined with the operator AND to find articles where all terms appeared.
First category (tinnitus OR hyperacus* OR hyperacous* OR misophonia OR phonophobia).
Second category: (epidemiolog* OR prevalence OR morbidity OR occurrence OR incidence).
Third category: (infant OR child OR children OR adolescent OR adolescence OR young adult).
The first category gave a total of 18 863 records, and the second category had a total of 2 687 135 records and the third category had 2 099 080 records. Combining the three searches gave a total of 712 hits from the Scopus search.
Additional records were identified through manual searches including review of reference lists of relevant papers and added nine records.
Study selection and data extraction
Studies identified with electronic and manual searches were listed with citation, titles and abstracts in Endnote (EndNote X7, V.17.4.0.10646, Thomson Reuters). Duplicates were identified using the Endnote function ‘find duplicates’ to compare each set of references. Two authors (SNR and JHS) independently screened the titles and abstracts according to the research question and PICOS criteria. All titles selected by either author were retrieved to screen their full text for final agreement and inclusion. If it was possible to confirm that an article met the inclusion criteria from the abstract alone, the full-text article was retrieved. If it was clear from the abstract that an article was not eligible, it was rejected immediately. The full-text article was retrieved if it was not possible to determine the eligibility of an article from the abstract.
In six articles, we found data missing or data requiring clarification. We were able to locate contact information on three authors, who were contacted for further information and clarification. We obtained additional data from one of these.
Two reviewers (SNR and JHS) extracted data and used the checklists presented in the study protocol, and one of the other reviewers was consulted if necessary to reach consensus.
Assessment of methodological consistency across studies
We had intended to utilise the GRADE14 principles for evaluations of studies, but the variable quality of studies identified precluded this. We therefore developed an assessment tool of methodological consistency described as a quality checklist in the study protocol.10 This assessment was used to determine the methodological differences of the papers considered for inclusion in the review. The decision to develop a new set of criteria was also due to the need to include items specific to the study of tinnitus and hyperacusis, and to address the concern raised regarding methodological challenges.
The methodological checklist was used to assess the methodological consistency of each study. To maximise the methodological consistency in studies to be included, it was decided that each study had to meet at least three of the following five criteria:
Tinnitus/hyperacusis definition: Does the study provide a definition of tinnitus/hyperacusis?
Tinnitus/hyperacusis definition presented to participants: Are other words than ‘tinnitus/hyperacusis’ used in the question asked to the child?
Understanding of question: Is the comprehension of the question assessed and/or is the child tested for giving reliable answers?
Presence of tinnitus versus severity of tinnitus: Does the study have a question regarding troublesome tinnitus? When examining hyperacusis, are distinctions made between sound sensitivity, noise annoyance, sound discomfort or pain in ears? If any questions regarding impact on everyday life of the child were raised in a study, for example, degree of annoyance, discomfort etc, and then the study was defined as addressing troublesome tinnitus.
Separation of aspects of tinnitus/hyperacusis for tinnitus: Are there questions regarding aspects of tinnitus such as location, duration, pitch etc? For hyperacusis: Are there questions regarding aspects of hyperacusis such as the kind of sound that is troublesome, loudness, low pitched, high pitched etc?
The studies were rated as follows: for each of the five criteria, a score of 1 was applied if the study met the criteria and a score of 0 if it did not or if the relevant information was unclear or not stated. The potential overall score could range from 0 to 5. The total scores were used to give an indication of the methodological consistency of each publication.
Data collection and synthesis
As anticipated in the study protocol, the studies identified were heterogeneous and different outcome measures were applied in each study. Clinical heterogeneity was presented. Some of the studies looked at specific populations, and some studies reported the proportion of tinnitus linked to subgroups as gender or hearing status out of the whole population. Methodological heterogeneity in terms of various study designs with differing levels of methodological consistency also resulted in differences among the findings of the studies.
The consequence was that the study findings could not be compared statistically and it was not meaningful to pool prevalence estimates in a meta-analysis. However, studies within the different population groups were compared and the methodological differences identified in order to demonstrate if the study comparison is feasible.
The findings were reported in a table and interpreted in a narrative manner.
Results
Numbers of articles
Once duplicates were removed, the systematic literature search identified 1864 records. Following screening of titles and abstracts, the text of 131 potentially relevant studies were retrieved and evaluated for inclusion.
The overall agreement between the two authors (SNR and JHS) was 89.3%, with an agreement on 117 studies and a disagreement on 14 studies. Any disagreement was resolved by discussion between the two authors, and there was no need to involve a third author during the process.
Of the 131 potentially relevant studies, 40 studies were assessed to evaluate methodological consistency using the checklist. Manuscripts were considered to include more than one study if there was more than one group (eg, age groups or groups of hearing-impaired children/normal hearing) or if there was reported prevalence of tinnitus and hyperacusis. One study was included by hand search since it is a study often cited as one of the early studies of childhood tinnitus, but the study was only to be found as a personal comment in another article (Reich in ref. 15).
Forty-seven individual studies were assessed in 40 different articles. Nineteen individual studies and 15 articles were excluded because the overall level of information was too low. Only one of these studies had a tinnitus definition in the article;16 six of the studies used other words in the question to determine if the child had tinnitus/hyperacusis;17–22 none of the studies tested if the child understood the question or gave reliable answers; four of the excluded questions had a question on troublesome tinnitus or distinguished between sound sensitivity, noise annoyance, sound discomfort or pain in the ear;23–26 and finally 10 of the studies had questions regarding aspects of tinnitus/hyperacusis.4 ,17 ,22 ,24–30
Finally, 25 articles were included in the review. See online supplementary appendix 1 (Methodological consistency checklist) for details of the consistency assessment. The stages and reasons for exclusions are presented in figure 1.
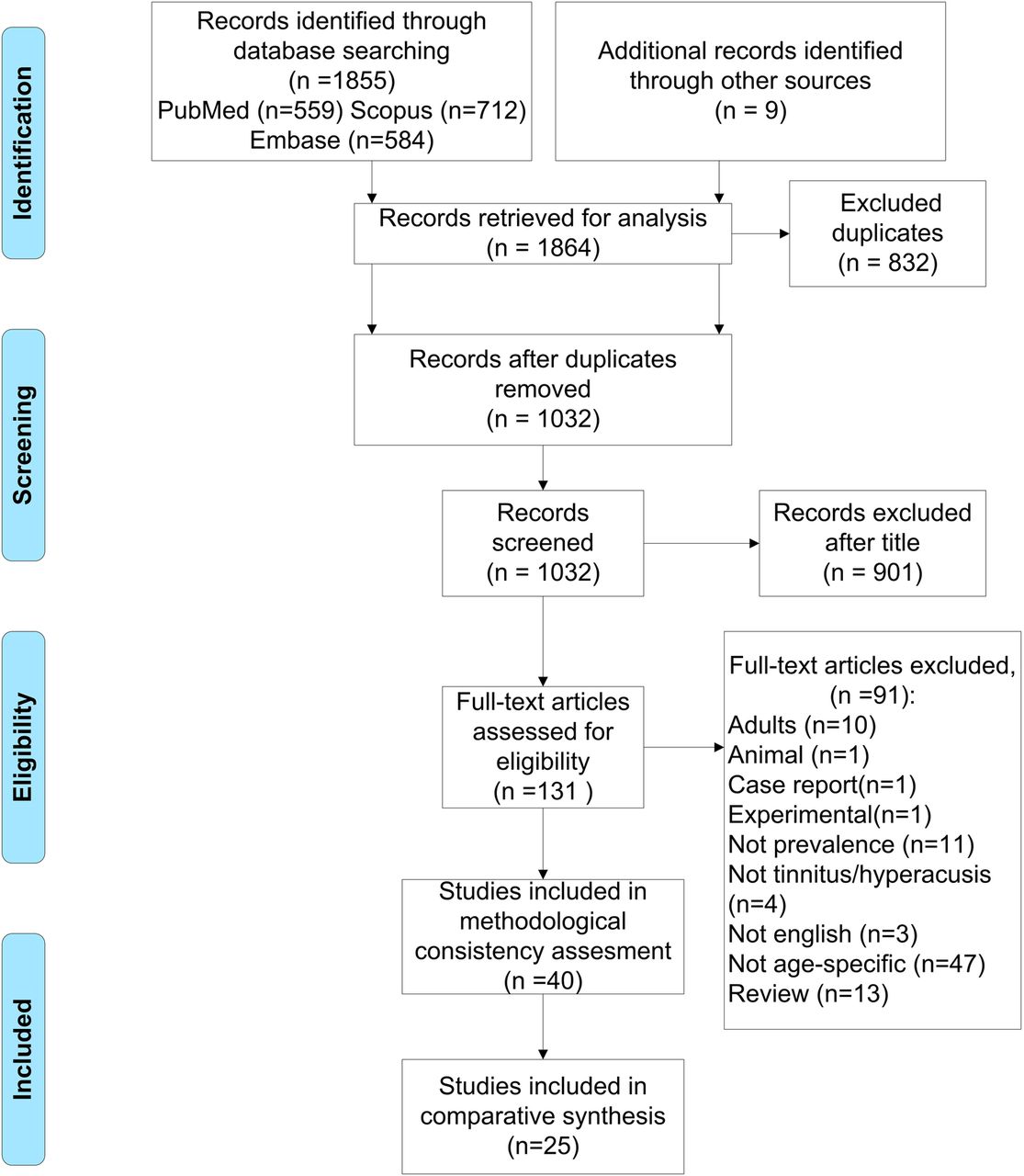
Flow chart.
Supplementary appendix
Description of articles
The 25 eligible articles had all been published since 1972 and five articles presented more than one study: Mills and Cherry31 presented one study with children with middle ear disease seen at ear, nose and throat (ENT)/audiology clinics and one study with children with sensorineural hearing loss seen at ENT/audiology clinics or school. Stouffer et al12 presented one group of children with normal hearing and one group of children with hearing impairment. Widen and Erlandsson32 presented one study of tinnitus prevalence and one study of hyperacusis. Landalv et al33 presented one study of tinnitus prevalence and one study of hyperacusis. Piotrowska et al34 presented one study of children aged 7 years and one study of children aged 12 years.
A comment on Mills et al4 is needed: the paper presented two different studies, but the second study (two otologists recorded brief clinical details including any spontaneous reports of tinnitus, on all children, 5 years and older, seen by them over a 6–7-month period during school medical examinations) was excluded due to poor methodological consistency. This part of the study failed all criteria except criteria 5: clear separation of aspects of tinnitus, which gave the study a rating of one. Mills and Cherry31 also presented two different studies in one paper, with age ranges of 4–15 and 4–17 years.
Chadha et al35 presented age range of 3–15 years. Age distribution of children perceiving tinnitus versus those not perceiving tinnitus were presented in four age groups: 3–5, 6–8, 9–11 and 12+ years. This structured reporting of age meant the study could be included as children aged below 5 years could be set aside.
As illustrated in table 1, the populations of the studies varied primarily between clinical settings and general population-based studies, with the majority performed in school populations. Some of the school-based studies were based on random samples of the study population in a given age range; others were performed on a specific study population; and, for example, six studies were located on schools of the deaf/hearing impaired.11 ,35 ,37 ,38 ,40 ,46 Two studies were performed at ENT/audiology clinics.31 ,45 Four studies were based on a representative sample from the background population.39 ,49–51
Descriptive items regarding populations studied
Fifteen of the studies used a questionnaire to collect data;32–34 ,36 ,38 ,42 ,43 ,46–51 eight used interviews;4 ,12 ,31 ,35,39–41 ,45 and four studies used a mixed method.11 ,37 ,44 ,52
Tinnitus was studied in 22 of the studies, 2 studied both tinnitus and hyperacusis,32 ,33 whereas 1 study dealt with hyperacusis alone.52
The study population size varied from 21 to 7918 participants in the age range of 5–19 years. It was decided to include one article with participants below the age of 5 among the participants, since this was a small study in a very specific population of cochlear-implanted children.35
Another article including children below the age of 5 years were also included, because the author in general restricted the study to those of 5 years and over, and only included ‘one or two’ (the specific number is not stated in the article) children under 5 years, who gave descriptions of tinnitus.31
Tinnitus: Varied testing methods for establishing hearing status were described: audiometry,31 ,34 ,39 ,42 ,47 tympanometry and audiometry,12 ,41 ,50 ,51 otoscopy, tympanometry and audiometry,40 ,45 ,49 otoscopy and audiometry,4 ,46 otoscopy, tympanometry, audiometry and loudness discomfort levels (LDLs),44 and audiometric screening.36
Furthermore, subjective information regarding the hearing status were collected from self-reported questionnaires,32 ,33 and school records.37 Two studies did not establish hearing status,35 ,48 and finally four studies only established hearing status on children they had included as having tinnitus.11 ,31 ,38 ,43
Seventeen studies included a description of tinnitus, including aspects such as duration, pitch and location.4 ,11 ,12 ,31 ,33 ,35–40 ,42–46 ,49
Eighteen of the articles provided no clear tinnitus definition;4 ,11 ,12 ,31–33 ,35–38 ,40 ,43–46 ,48 ,50 ,51 five studies either defined tinnitus as a sound lasting for more than 5 min or excluded noise-induced tinnitus in their study39 ,41 ,42 ,47 ,49 and one article defined tinnitus as a sound lasting more than 5 min and excluded noise-induced tinnitus.34
Seventeen studies asked for a description of tinnitus.4 ,11 ,12 ,31 ,33 ,35–40 ,42–46 ,49
Fourteen studies considered the consequences of tinnitus.4 ,11 ,33 ,35 ,37 ,38 ,40 ,42–46 ,49 ,50
Hyperacusis: All three studies were performed in a school setting. Otoscopy, tympanometry, audiometry and LDLs were tested in one study,52 while two studies used a questionnaire to establish the hearing status.32 ,33
All three included studies had a definition in their article and used words other than hyperacusis in their prevalence question.
Missing data
Nodar36 reported the prevalence (though not how prevalence was calculated) and the incidence of tinnitus during a 3-year period in children with normal hearing and with hearing impairment. No information was given as to the number of children in each of the age groups in the background population. It was also difficult to determine if the numbers reflect new cases of tinnitus in each year or if some of the children have been counted more than once. The article was published in 1972 and it has not been possible to find contact information to the author to address these issues.
The reported gender-specific prevalence in Drukier38 was taken directly from the article as it was not possible to interpret why the gender-specific prevalence do not add up to 100%. The article was published in 1989 and it has not been possible to find contact information to the author to address this issue.
Savastano45 reported the proportion of children with normal hearing and those who are hearing impaired with tinnitus. It was not possible to estimate the prevalence of participants with normal hearing and those who are hearing impaired from this article since audiometry was performed only on the participants with tinnitus. Therefore, these numbers are not comparable. Instead, the study has shown that 76.4% of the participants with tinnitus had normal hearing and 23.5% had hearing impairment. The overall prevalence number was calculated for the age range 6–16 years, although the author concluded in her study that the data on tinnitus measurements below 8 years of age were non-reproducible but an analysis was not performed. The author was contacted for clarification, but without response.
Mahboubi et al49 were contacted for information regarding prevalence of troublesome tinnitus, but without response.
Gilles et al48 was contacted and provided additional information on how the prevalence number linked to gender was calculated.
Celik et al46 reported a total of 167 children with tinnitus, but when they reported the prevalence linked to gender, 30 children were missing. This missing data were belatedly discovered, and it was not possible to contact the authors for clarification.
Findings of the review
A wide variation from 4.7% to 62.2% was evident in the reports on tinnitus prevalence in children. In table 2, results are reported separately for comparable population groups. In the general paediatric population and among children with normal hearing, the prevalence ranged from 4.7% to 46%. The prevalence ranged from 6% to 41.9% when children with hearing loss and normal hearing were both included. In the population of children with hearing impairment, the prevalence ranged from 23.5% to 62.2%.
Results items
The prevalence of hyperacusis varied from 3.2% to 17.1%.
Methodology differences (tinnitus)
The methodological consistency of studies was rated in relation to five characteristics as described in the Methods section and the study protocol article. Details of the consistency assessment are contained in the online supplementary appendix 1 (Methodological consistency checklist). Seven out of 24 articles on tinnitus scored the maximum possible score (5) on the previously described checklist of methodological consistency;35 ,38 ,40 ,43 ,45 ,46 ,50 6 articles had a score of 44 ,11 ,31 ,36 ,44 ,49 and 11 articles had a score of 3.12 ,32–34 ,37 ,39 ,41 ,42 ,47 ,48 ,51
A definition of tinnitus in the article was present in 14 of the included articles.32 ,34–36 ,38–40 ,43 ,45 ,46 ,48–51 All included articles used another word than tinnitus in the prevalence question.
Sixteen studies provided approaches to ‘understanding of questions either by collecting reliable answers from the children or assess the comprehension of the question’.4 ,11 ,12 ,31 ,34–36 ,38 ,40 ,41 ,43–47 ,50 Sixteen studies distinguished between tinnitus sensation and troublesome tinnitus.4 ,11 ,31 ,33 ,35 ,37 ,38 ,40 ,42–46 ,49–51 All studies except two34 ,51 included aspects such as location, duration and pitch in their article, showing separation of different aspects of tinnitus.
Tinnitus questions used
The primary challenge for studies investigating the prevalence of tinnitus lies in the applied definition of tinnitus. The exact wording of the question regarding tinnitus varied across studies between the year 197236 to the most recently published article included from 2015,34 with a trend of development from a rather broad tinnitus question (noises in the ears) moving towards more specific tinnitus questions including aspects such as duration of the sensation of tinnitus.
Considering prevalence finding with the tinnitus questions used and the population studied indicates that the article with the highest reported prevalence involved children with hearing impairment.37 This article utilised the question: ‘Do any of you get noises in your ears’, followed by an explanation that tinnitus does not include any of the sounds produced by hearing aids or from the child's surroundings. The research question used in the article reporting the lowest prevalence is very specific sounds: ‘In the past 12 months, have you been bothered by ringing, roaring or buzzing in your ears or head that lasts for 5 min or more?’49 This study was performed within a representative sample from the general childhood population.
Two articles used the same phrasing of the questionnaire among 7-year school children.41 ,47 The studies were performed in a mixed population of children with normal hearing and with hearing impairment separated by 9 years and demonstrate a prevalence of 12.4% in the article from 1997 and a prevalence of 41.9% in the article from 2006. In the 2006 article, an additional question was added regarding noise-induced tinnitus which may have affected the response to the main tinnitus question.
Approaches to collecting reliable answers
The approach to the collection of reliable answers was reported in 16 articles4 ,11 ,12 ,31 ,34–36 ,38 ,40 ,41 ,43–47 ,50 Eight studies did not clearly deal with the issue of making sure that the child understood the prevalence question or was capable of giving reliable answers.32 ,33 ,37 ,39 ,42 ,48 ,49 ,51
The approach to collect reliable answers included attempts to ensure that the child had understood the question,34 ,36 ,40 ,44 ,47 communication at the child's level,34 ,38 re-explanation of the question if necessary43 ,46 or explained to the child that tinnitus were not noises from their hearing aids or surroundings.11 ,40 One article did not test if the question has understood, but the children were accompanied by their parents,35 and in another article50 answers from parents were compared with the answers from their children. The ability of the child participants to describe their tinnitus was reported in four studies.4 ,12 ,31 ,45 As a part of collecting this description, Mills and Cherry31 added that they avoided ‘suggesting possible descriptions of tinnitus to the children in case they seized on them in an effort to please’.
The overall prevalence of studies with an approach to collect reliable answers was in a range from 6% to 49.4% and the overall prevalence of studies without this approach was in a range from 4.7% to 62.2%. There may be a number of factors reflecting the prevalence differences. The studies without a check for reliable answers were performed in children aged 9 years or older, where studies with focus on reliable answers were performed in children aged between 5 and 18 years. Different tinnitus questions were used, which could potentially contribute to differences in prevalence estimates.
All articles presented from the mixed population and all articles except one from the hearing-impaired population checked the reliability of answers. Three out of the 13 studies performed in the general paediatric population and among children with normal hearing checked the reliability. These articles had different age ranges and all used different tinnitus questions.
Two studies presented in the same year by the same author used identical phasing of the question among children of 12–18 years with hearing impairment.11 ,37 Both studies explained that tinnitus did not include any of the sounds coming from the hearing aids or from the child's surroundings. One article made sure that each child understood the question and found a prevalence of 49.4%;11 the other article did not, and found a prevalence of 62.2%.37
Savastano45 used a previously published protocol53 for the study of tinnitus childhood in which the child is tested for issues like the capacity to describe tinnitus and degree of annoyance. The protocol provided no age frame for use, but only children aged 6 years and over were included, since below this age consistent answers could not be obtained.45 As mentioned in the section of missing data, this article reported the fraction of individuals with normal hearing and those who were hearing impaired with tinnitus and it is not comparable to the prevalence reported in the rest of this section.
Three4 ,31 ,43 other studies also reflected on the influence of age when collecting reliable answers. Mills and Cherry31 found that below the age of 5 years, consistent answers could not be obtained, and Aksoy et al43 evaluated children individually without their peers'.
One article excluded children younger than 9 years of age owing to their difficulty in estimating the time aspects of tinnitus.42
Characteristics of the reported tinnitus sensation
The prevalence of troublesome tinnitus was reported in 16 articles4 ,11 ,31 ,33 ,35 ,37 ,38 ,40 ,42–46 ,49–51 with a range from 0.6%50 to 49.2%.42 The question regarding troublesome tinnitus used different words for description, such as bothersome, uncomfortable, worried and concerned. Four studies used a yes/no response.4 ,31 ,43 ,44 In the article with the highest prevalence report, the number of participants with troublesome tinnitus is not stated, only the per cent of annoyed participants in the total population was reported.42
As shown in table 3, the degree of troublesome tinnitus is evaluated and described differently in the different studies. In this review, we have calculated and reported the prevalence of the participants with the highest category of troublesome tinnitus.
Question used to identify troublesome tinnitus and prevalence reported
Six articles used the word ‘bothersome’ to measure troublesome tinnitus with a prevalence range from 12% to 44.7%. Savastano45 found 12.0% of children aged 6–16 years to be always bothered and 4.8% of the children were severely worried. Coelho et al44 found that 44.7% of the children surveyed (5–12 years old) were bothered. Both studies used quite different questions asking if children were troubled by tinnitus. Coelho et al used a broader definition of troublesome tinnitus. In this study, tinnitus was bothersome if children answered yes to the question: ‘does it bother or annoy you?’ In contrast to the article by Savastano, where the severity of bothersome tinnitus was graduated into four categories. These differences in the characterisation of the severity of tinnitus may explain the reported prevalence differences.
Park et al50 asked if the surveyed children aged 12–19 years found tinnitus annoying with the possible answers: no/a little annoying/very annoying. Holgers and Juul42 asked if tinnitus was troublesome for the child, aged 9–16 years with possible answers: no/sometime/often. The first article checked for reliable answers; the second did not. It is questionable if it is possible to compare studies, when both the questions and the possible answers are as different as in this example. Both articles presented data from the general paediatric population and among children with normal hearing.
Landalv et al33 addressed patient concern about temporary tinnitus with a prevalence of 30.8%. Celik et al46 found a prevalence of 13.2% asked the question ‘bothersome yes/no’, but the article reported troublesome tinnitus as the number of children who presented with tinnitus all the time. Two articles did not state the prevalence question, but just reported that 20% described that tinnitus had any impact on their quality of life35 and that 33% were occasionally concerned.40
Savastano45 reported the prevalence of troublesome tinnitus to be 12% of the children being very bothered and 4.8% of the children being more severely worried. This indicates that it does make a difference if we use the word ‘bothered’ or ‘worried’ is used as an indicator of troublesome tinnitus.
Population characteristics (tinnitus)
Age
While some studies reflected on age as a parameter for collecting reliable answers as already reported, other studies provided information on each individual age in a particular age range. Some studies reported the age distribution and others reported prevalence related to each age group, which make the results difficult to compare.
As shown in figure 2, the studied population age varied from 3 to 19 years.

{kind=link}
{kind=link}
Shows the age range of studies included.
Three articles reported tinnitus prevalence among children aged 7 years with a range of 6.5–41.9%.34 ,41 ,47 The prevalence of 12.4%41 and 41.9%47 using the same phrasing of the question was found in two articles, these being published 9 years apart. The prevalence was 6.5% of the children aged 7 years if a more narrow tinnitus definition was used, which could explain the lower prevalence.34 The same article also investigated a group of children aged 12 years, and found a lower prevalence in the subjects aged 12 years (4.8%) compared with the 7 years old.
Permanent tinnitus (present all the time) was reported with a prevalence of 6.8% among the children aged 13–15 years and a prevalence of 10.3% among the 16–19 years.32 A similar prevalence of 9.2% of constantly perceived tinnitus in children aged 14 years was shown to be significantly lower compared with the older categories (more than 15%).48
Furthermore, a prevalence of 3% in the children aged 12–15 years and a prevalence of 6.5% in the 16–19-years old, with tinnitus lasting 5 min or more for at least 3 months during the past 12 months, were demonstrated in another article.49
Thus, all three articles found that tinnitus seems to increase with age. The phrasing of the question asked could influence the numbers, since the article with the lowest prevalence had a narrower definition.
Coelho et al44 looked at children aged 5–12 years, and reported the 12 years old as most commonly reporting tinnitus. Aksoy et al43 investigated children aged 6–16 years with tinnitus and found that the age group most commonly reporting tinnitus was between 12 and 14 years and the children reporting less tinnitus was 16 years old. Savastano45 looked at children aged 6–16 years and found that the age group most commonly reporting tinnitus was the 12 years old. Drukier38 reported that the age group most worried about the sound was the 6–10 years.
Two articles regarding tinnitus in children with hearing loss are directly comparable (age range of 6–16 years), as they both provide prevalence of tinnitus within each age group.40 ,46 Tinnitus prevalence in children aged 10 years or under was reported within a range of 0–30%, with an exception of the 10 years in the article by Viani40 that reported a prevalence of 60%. Prevalence aged 11 years or older was reported in a range of 7–66%.
Nodar36 reported the number of children with tinnitus aged 10–18 years, and was the only incidence study found in this review. Data on more than 2000 participants were collected during a 3-year period. The percentage remained relatively constant (ca. 15%) with a relatively low incidence in the early and late teens, and higher incidence in mid-teens.
Gender
The prevalence of tinnitus in men varied from 15.4% to 54.5% and tinnitus in women varied from 17% to 56.8% with varying population sizes (40–3842 participants).
Six articles40 ,42 ,44–46 ,48 presented prevalence linked to gender from the total number of children with a male prevalence range of 20–35.6% and a female prevalence range of 17–42.4%. Two articles presented prevalence among the total number of children with tinnitus. Aksoy et al43 reported a distribution of 54.5% men and 45.5% women and Holgers41 found a distribution of 47.5% men and 52.5% women.
Two articles did not provide information regarding how they calculated the prevalence linked to gender. They found a male prevalence of 15.4%50 and 22%38 and a female prevalence of 20.3%50 and 40%.38 One article provided data on children with cochlear implants, and was not suitable for this comparison.
Hearing ability
The prevalence of tinnitus in the general paediatric population and among children with normal hearing varied from 5.4% to 46% across 10 articles4 ,32 ,33 ,39 ,42 ,43 ,48–51 with varying population sizes (30–3520 participants). Age range varied from 5 to 19 years.
The prevalence of tinnitus in children from mixed-study populations (children with hearing loss and normal hearing) varied from 6% to 41.9% across seven articles12 ,34 ,36 ,41 ,44 ,45 ,47 with varying population sizes (140–7918 participants). Age range varied from 5 to 18 years.
For the group of children with normal hearing, the prevalence of tinnitus varied from 0.8% to 76.4%. The prevalence number reported from children with hearing impairment varied from 1.0% to 58.6%.
The prevalence of tinnitus in children aged 5–18 years with hearing impairment varied from 23.5% to 62.2% across six articles11 ,31 ,37 ,38 ,40 ,46 with varying population sizes (44–500 participants). A study was performed on tinnitus in children with cochlear implants,35 and was not suitable for this comparison.
Comorbidity
Only one article42 of 274 children aged 9–16 years considered anxiety, and found that 32% of the patients scored above the cut-off level for possible/probable clinical emotional/anxiety disorder for adolescents, and 14.5% scored above the cut-off level for possible/probable clinical depression. No gender differences in depressive disorders were seen, but more girls (49%) than boys (26%) had anxiety disorders. No difference in the duration of tinnitus in children with or without anxiety disorders was reported, but children with depressive disorders had experienced tinnitus for a period of 24 months as compared with 17 months in the group without depression.
Methodology differences (hyperacusis)
The methodological consistency of studies was rated in relation to five characteristics as described in the Methods section and the study protocol article. See online supplementary appendix 1 (Methodological consistency checklist) for details of the consistency assessment. Three articles were included in this review. One reached the maximum score of methodological consistency;52 one article had a score of 4,33 and another had a score of 3.32
All articles included had a definition and used another word than hyperacusis in the prevalence study. One study made sure the child understood the question.52 Two articles provided a separation between sound sensitivity, noise annoyance, sound discomfort and pain in ears in their investigation,33 ,52 and all three articles had questions on aspects such as the kind of sounds, loudness, low pitched, high pitched and so on.
The prevalence of hyperacusis varied from 3.2% to 17.1% across an age range from 5–12 to 13–19 years with a population size from 242 to 1285 participants.32 ,33 ,52
Hyperacusis definition and question used
In one article, hyperacusis was defined as extreme sensitivity to everyday sounds of low intensity,33 with a description explaining that persons with hyperacusis may experience annoyance of some sounds, that it may also be due to a fear of getting or worsen a hearing loss or tinnitus.
One article did not provide a clear definition of hyperacusis or sensitivity to sound, but explained how people can feel and react to sounds.32
One article defined hyperacusis as unusual (low) LDL associated with annoyance from normal sounds.52 The study classified children as having ‘phonophobia’ if they were afraid of sounds.
Two articles used very similar questions. The first study performed in 2014 by Widen and Erlandsson32 reported that 17.1% considered themselves being oversensitive to noise with a yes/no response. The second investigation performed in 2013 by Landalv et al33 reported that 3.3% experienced themselves being overly sensitive to sounds more than 50% of the time and 14% of the participants noticed discomfort with sound about 50% of the times. Recalculating the answers to a yes/no response would give a positive response to the question of 39.2%. Changing the threshold for the prevalence reported in the second article can make the two studies more comparable, but it is uncertain if experience yourself being overly sensitive to sound and considering yourself to be oversensitive to noise are measuring the same thing.
Only one of the studies tested the prevalence question for comprehension.52
Population characteristics (hyperacusis)
One study looked at children aged 5–12 years, and found that the highest number of children with hyperacusis was at the age of 8 years (4 out of 16).52
The article by Widen and Erlandsson32 reported that 19.7% of the 16–19 years and 14.0% of the 13–15 years considered themselves being oversensitive to noise.
The prevalence rate was linked to gender in two articles with a higher female prevalence (4.4% and 20.9%),32 ,52 compared with the prevalence found in men (2.3% and 12.4%).
One article linked the prevalence to hearing ability and found that 2.5% of the children with normal hearing, and 6.6% of the children with hearing loss had hyperacusis.52
None of the articles reported information regarding comorbidity.
Heterogeneity across studies
Table 2 presented the findings linked to groups to achieve a uniform way to compare them and to determine the possible methodological consistency across studies within each population group by pooling the estimates of tinnitus. However, due to the very different ways of defining and asking the child about tinnitus, it was not possible to estimate if they were measuring the same thing.
It was not feasible to pool the studies. The synthesis of the results was focused to demonstrate variability in prevalence estimates in the comparable groups instead as reported above. However, it should be noted that even within comparable groups, it can be impossible to compare studies directly due to large differences in the wording of the tinnitus question and the underlying definition of tinnitus.
Table 3 presented the research question used to identify the degree of troublesome tinnitus. Bothersome tinnitus was described in three different population types. Only two articles4 ,43 may reasonably be compared and could potentially be pooled, but as the study populations are very different in size, it is more appropriate to report that 33–39% of children with tinnitus regarded it as bothersome.
Worries about tinnitus were also described in three different population types. Two articles11 ,38 asked the same question and may reasonably be compared. Since the distribution of age for the children in the article by Drukier38 are reported into three age groups, it is possible to look at children aged 11–16 years and compare them with the 12–18 years old studied by Graham.11 However, the wording used for the highest extent of troublesome tinnitus is ‘all the time’ in the study by Graham and ‘very much’ in the article by Drukier. Therefore, it is more appropriate to report that 11–22% of the children with tinnitus were very worried.
Discussion
With the current review, the epidemiological studies of tinnitus and/or hyperacusis prevalences in children and adolescents in different population types were systematically examined. Furthermore, a set of criteria was developed to assess the methodological consistency of the articles included in this review. To our knowledge, this is the first systematic review of epidemiological studies of participants with paediatric tinnitus/hyperacusis where methodological consistency across studies was assessed.
Methodological differences (tinnitus)
The first objective of this review was to determine the methodological difference implicated in the variability of prevalence estimates. Differences in definition of tinnitus, in the tinnitus question used and in the populations studied make comparison across studies challenging. The definition of tinnitus and the research question asked were found to be the most salient issues.
The definition of the term ‘tinnitus’ by the authors varied substantially. There was not necessarily a connection between the way tinnitus was defined by the authors in their article and the research question used in their study. For example, one article defined tinnitus as an auditory sensation without any external stimulus and asked the question: Have you ever had noises in your head or ears?43 Furthermore, participants indicated if they had tinnitus with a duration of 5 min to separate more chronic tinnitus from occasional ear/head noise although it did not provide a clear definition of tinnitus. Thus, the authors rely on that definition of tinnitus being understood by the reader/hearer of the question.12
Depending on the questions used in each individual study, the reported data may represent the prevalence of anything from brief to lifetime experiences of tinnitus, with or without considerations about duration or severity. Altogether, the phrasing of the tinnitus question along with the definition can influence the prevalence estimates heavily and challenges the comparison across studies.
To ensure that studies of childhood tinnitus are robust, it is necessary that answers from the children can be relied upon. The question should be phrased in such a way that it is understandable by the child and the answers should be reliable. Researchers should avoid the child telling them what they think they want to hear, or changing their answer, if the question is asked twice, because they may then think it was an incorrect answer that was given the first time. One should also be sure that the questions used are suitable for the target age group.
Different approaches to the collection of reliable answers were revealed among the studies, for example, a test if the child understood the question,34 ,36 ,40 ,44 ,47 or if the child was able to give consistent answers,12 and in some studies lower age was used as exclusion criteria.4 ,31 ,42 ,45 Recall bias has been addressed in an investigation on annual injury rates among children.54 The study investigated the effects of recall bias on estimating annual injury rates among children aged 0–17 years. It showed marked differences in recall decline among children in all age groups for a 12-month recall period. Looking more directly at children and tinnitus, the issue related to age and interviewing children has recently been addressed by Kentish2 stating that even very young children can provide highly reliable information, given the right circumstances, and with reasonably skilled interviewing techniques.
Owing to population differences such as age, hearing status and differences in tinnitus definition and tinnitus questions used, it is not possible to compare and conclude if there is a difference in articles checking for reliable answers compared with articles that do not. Nevertheless, it is crucial that researchers make sure the questions put to participants are understood and the answers received are reliable, so as to be able to rely on and compare future studies.
In this review, variations in how the authors asked and reported answers of troublesome tinnitus were found. Different words to measure troublesome tinnitus such as ‘bothered’, ‘worried’ and ‘concerned’ were used, making it uncertain that the studies are addressing the same thing. Furthermore, some articles graduated the answer possibilities into different categories, while other articles used a yes/no response. These differences make it very difficult to compare the prevalence in troublesome tinnitus across studies.
It is unknown how many children are troubled by tinnitus to such a degree that they need help to cope with it. A previous study showed that only few children were seen in established tinnitus clinics.9 In an article of children's experience of tinnitus, a low rate of spontaneous symptoms of tinnitus was reported,8 and Mills et al4 stated that children seldom present openly of their symptom. Adult prevalence studies in tinnitus shows a prevalence of 10–15% of the population, with 0.5–3% being significantly troubled by it.3
Holgers and Juul42 and Widen found that most of the children between 8 and 20 years seeking help for tinnitus were in their teens. Additionally, children referred to a specialised tinnitus centre between 6 and 18 years had a mean referral age of 13.8 years.9
Furthermore, a study of troublesome tinnitus found children with normal hearing to be more troubled by tinnitus than those with some level of hearing impairment.8 This finding cannot be confirmed in this review, properly because the diversity of the tinnitus questions affects the prevalence estimates across the different studies.
The different ways of asking and reporting answers of troublesome tinnitus must be considered as a bias in comparing across studies. Different tinnitus measurement indexes are developed and used for adults, for example, the Tinnitus Handicap Inventory (THI)55 and the Tinnitus Functional Index (TFI),56 but there are no standard measures suitable and tested for children as yet.
Population characteristics (tinnitus)
The second objective was to review the influence of population characteristics. It was found that age, gender and hearing ability had an impact on the reported prevalence.
It was shown that tinnitus prevalence increases with age32 ,48 ,49 as well as a report of a higher prevalence in the mid-teens.36 The group of children aged 12–18 years had a higher prevalence than the age groups from 19–49 years, but was less annoyed by the sound than any of the other groups.51 This finding could support the hypotheses stated by Mills and Cherry31 that children tend to accept experiences, which, as far as they are concerned, have always existed.
An investigation in a general paediatric population and among children with normal hearing found that the 12–14 years was the age group most commonly reporting tinnitus, and the age group less commonly reporting tinnitus was 16 years.43 The study found 154 children with tinnitus out of 1020 children, and potentially this result is due to the small size of the tinnitus cohort.
Furthermore, a lower prevalence of the 12 years old (4.8%) compared with the 7 years old was shown in a mixed-study population of normal hearing and hearing-impaired children.34
Potentially this is due to recall bias or due to the complexity of the tinnitus question: within the past 6 months, have you experienced any noise such as ringing, buzzing, hissing, or any other sort of sound in your ear or your head that had no apparent cause?, although the study made an effort in communicating at the child's level both developmentally and linguistically. However, it may reflect true differences in the population.
The issue of reliable answers and age was addressed in some of the articles. This issue is related to the impact of recall bias, and to the younger children's difficulties in estimating the time aspects of tinnitus. In future studies, a point prevalence approach may glean useful data.
Findings in this review indicate a slightly higher rate of prevalence in women. An adult study57 with 99 435 participants shows that the prevalence of tinnitus for men and women increases with age and is higher for men than for women from the age of 25 years up to the age of 75years. However, for the age group of 20–25 years, the prevalence for women is slightly higher than for men. This study did not include younger participants, but the female gender has been identified as a risk factor in children and adolescents.25 ,44 ,50 Possible explanations according to Coelho1 are that girls are more likely to express symptoms than boys, and that spontaneous otoacoustic emissions are more frequent among girls.
The articles were divided into three different population groups according to the hearing status (normal hearing, mixed population with and without hearing loss and hearing impairment) to achieve a uniform way to compare them. Hearing ability in relation to the tinnitus prevalence was therefore addressed in this review. The prevalence of tinnitus was highest among children with hearing impairment with a variation from 23.5% to 62.2%. The prevalence of tinnitus varied from 6% to 41.9% among children in mixed-study populations and had a variation from 5.4% to 46% among children in the general paediatric population and among children with normal hearing. Adult studies find hearing loss to increase the risk of tinnitus sensation, but not the degree of potential troublesome tinnitus.3
As stated earlier, two articles presented in the same year by the same author used identical phrasing of the question among children aged 12–18 years with hearing impairment. It was made sure that each child understood the question in one article,11 which found a prevalence of 49.5%. The other article did not test for understanding and found that 46 out of 74 children had tinnitus (a prevalence of 62.2%).37 The low numbers of participants could also have contributed to the variation in the prevalence numbers reported.
Holgers and Juul42 suggested that children with tinnitus have a higher rate of associated psychological difficulties, including anxiety and depression. A study by Kim et al25 drew similar conclusions. This article was excluded from the present review due to a total methodological consistency score of 2 because the article did not provide a definition of tinnitus; did not present the tinnitus research question used to investigate the prevalence; and did not test if the child understood the question or gave reliable answers.
Nevertheless, the article provides useful information on the associated psychological difficulties. The authors suggested that tinnitus in children has a considerable influence on their levels of stress and anxiety.25 Future studies should address the psychological factors to investigate if this aspect can affect the overall prevalence of tinnitus and hyperacusis.
Methodological differences and population characteristics (hyperacusis)
Methodological differences and the influence of population characteristics among studies on childhood hyperacusis were also assessed. Three articles were reviewed, but the diversity among them made it impossible to compare them directly.
Reports on the prevalence of hyperacusis in children range from 3.2%52 of the general population to 95% of children with Williams syndrome.58 Childhood hyperacusis has been linked to specific conditions such as autism29 ,30 or Williams syndrome,58 but has also been examined within a general paediatric population.32 ,33 ,52
Heterogeneity across studies
The final objective aimed to assess the heterogeneity across studies and to determine if pooling of the studies is feasible. In this review, it has not been meaningful to pool studies giving the wide variation of populations and questions used to assess tinnitus. However, it is possible to compare the study CIs among different population sizes especially within identical population groups, as can be from table 2.
Furthermore, it has been attempted to compare different studies in relation to identical tinnitus questions, tinnitus severity and different age groups as described above, but often these comparisons are only meaningful between very few studies due to the large differences in methodological consistency across studies.
A consensus for standard measures of tinnitus patient assessment and treatment in adults has been established,59 and in 2015 the Pediatric Audiology Interest Group (PAIG) of the British Society of Audiology (BSA), supported by the British Tinnitus Association, has developed Practice Guidance60 for working with children with tinnitus. Hopefully, this will lead to an end to the lack of standard measures for children with tinnitus, and will provide more consistency across studies performed in the future. This will enable future researchers to compare studies more easily with direct comparison of measured population prevalence. No guidance for working with children with hyperacusis has been developed as yet. Hopefully this area will be addressed as well.
Limitations of this study
Although the information in the published literature sometimes was difficult to extract and interpret, partly because not all articles had the same primary research objectives as the present review, all discrepancies were resolved without the need for a third author as arbitrator. This indicated good consensus between reviewers; however, it is not a guarantee for accuracy.
The methodological consistency checklist was specifically developed for this study and has been presented in a previously published protocol article.10 Since the methodological consistency checklist used was designed to meet our needs for the present review, we risked excluding articles which might have been included, if another type of consistency checklist had been used.
Studies included in this review were selected through a check of methodological consistency, since no fixed set of generally accepted criteria was found useful to handle the methodological challenges in comparing childhood prevalence studies on tinnitus.
There is a risk that relevant articles have been excluded for this reason.
In this review, we have calculated and reported the prevalence of troublesome tinnitus using numbers for the participants reported to be mostly impacted by the sound. This is a potential bias when these studies are compared.
The tinnitus or hyperacusis question asked, how it is asked and that making sure the question is understood will potentially affect the answers and results given. It is worth noting that eight of the studies32 ,33 ,37 ,39 ,42 ,48 ,49 ,51 included in this review did not clearly deal with the issue of making sure that the child understood the prevalence question or was capable of giving reliable answers. Six of the studies had a tinnitus definition.32 ,33 ,39 ,48 ,49 ,51 All eight studies used another word than tinnitus in the question asked to the child. Five of the studies had a question regarding troublesome tinnitus,33 ,37 ,42 ,49 ,51 and finally were aspects of tinnitus such as location, duration and pitch examined in all studies except one.51
None of the studies used more than one tinnitus question, and there was an implied expectation that these single questions would be equally accessible to younger and older children alike, which is open to question.
Implications for further research
The lack of consistency among studies indicates the necessity of examining the epidemiology of tinnitus in children and adolescents with a set of standardised methodological consistency criteria. This study provided a set of criteria, which showed that only a small proportion of the published studies successfully met all of them. Future studies should adhere to a set of methodological consistency criteria to allow a more direct comparison of their results, as well as advancing understanding of prevalence rates of paediatric tinnitus. An increased focus on study consistency would facilitate combination of studies for the purpose of obtaining overall prevalence rates.
There is currently neither an internationally recognised standard definition for tinnitus/hyperacusis nor a unique internationally recognised classification of these diagnoses. This raises additional difficulties in comparing results across studies.
Depending on the questions used in each individual study, the reported data may represent the prevalence of anything from brief to lifetime experiences of tinnitus, with or without considerations about duration or severity. Study design and the study population need to be closely linked and the tinnitus question asked must reflect the age of the child.
Recall bias and interview bias should be carefully reflected upon in future studies, as well as potential confounders such as gender, socioeconomic situation, geographical location and other health issues like hearing status.
There is an opportunity for researchers within the field of paediatric tinnitus and hyperacusis to find agreement on a standard way of assessing, defining and reporting prevalence and severity of tinnitus/hyperacusis. It would be valuable to obtain standardised information on prevalence, with well-defined questions and tight age ranges, or sampling at a specific age. The most important aspects of designing a questionnaire about tinnitus in children will lie in phrasing the question; so it is age-relevant, making sure the children understands the words used and asking about something the child can remember. Younger children should be asked about the present rather than the past. Questions should be tested in a pilot study and reframed if necessary. It is also important to reflect on the tester–participant relationship.
While the literature is variable, a consensus exits that tinnitus and hyperacusis do exist among children, and can be severe. This has implications for the commissioning and design of services for childhood tinnitus and hyperacusis.
Conclusion
Data on the prevalence of tinnitus and hyperacusis in children and young people vary considerably according to the study design, study population and research question with a variation from 4.7% to 74.9% (tinnitus) and from 3.2% to 17.1% (hyperacusis) in 25 articles. Age, gender and hearing status of the study population are factors implicated in the variability of estimates. This review finds differences in tinnitus definitions, the tinnitus question used to establish prevalence and whether or not it has been tested if the child understands the question as the biggest bias for comparing studies.
The lack of methodological consistency among studies indicates the necessity of examining the epidemiology of tinnitus and hyperacusis in children and adolescents with a set of standardised and consistent criteria.
Acknowledgments
The authors thank the postgraduate student (Bachelor of Arts (BA) in Audiologopaedics) Anestis Kapandais for his help in develop the design for data collection and extraction and for making figure 2, prevalence linked to age.
References
Footnotes
Contributors All authors take responsibility for the integrity of this manuscript. SNR and JHS were involved in study design, implementation, analysis and writing. NW and DMB were involved in study design, writing and editing.
Funding This review is part of a doctoral study, which has been funded by The Capital Region of Denmark, The University of Southern Denmark and The Danish Association of the Hard of Hearing.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All recorded data from the data extraction process will be available on request to the extent that it is not included in the systematic review article.