Article Text

Abstract
Objectives To evaluate symptoms presented by the caller during emergency calls regarding stroke, and to assess if symptoms in the Face-Arm-Speech-Time Test (FAST) are related to identification of stroke.
Setting Emergency calls to the Emergency Medical Communication Center (EMCC) concerning patients discharged with stroke diagnosis in a large teaching hospital in Stockholm, Sweden, in January–June 2011.
Participants The emergency calls of 179 patients who arrived at hospital by ambulance, and who were discharged with a stroke diagnosis and consented to participate were included in the study.
Outcome measures Frequencies of stroke symptoms presented and a comparison of symptoms presented in calls with dispatch code stroke or other dispatch code.
Results Of the 179 emergency calls analysed, 64% were dispatched as ‘Stroke’. FAST symptoms, that is, facial or arm weakness or speech disturbances, were presented in 64% of the calls and were spontaneously revealed in 90%. Speech disturbance was the most common problem (54%) in all calls, followed by fall/lying position (38%) and altered mental status (27%). For patients with dispatch codes other than stroke, the dominating problem presented was a fall or being in a lying position (66%), followed by speech disturbance (31%) and altered mental status (25%). Stroke-specific symptoms were more common in patients dispatched as stroke. FAST symptoms were reported in 80% of patients dispatched as stroke compared with 35% in those dispatched as something else.
Conclusions This study implicates that fall/lying position and altered mental status could be considered as possible symptoms of stroke during an emergency call. Checking for FAST symptoms in these patients might uncover stroke symptoms. Future studies are needed to evaluate if actively asking for FAST symptoms in emergency calls presenting falls or a lying position can improve the identification of stroke.
Trial registration number Stroke2010/703-31/2.
- STROKE MEDICINE
- ACCIDENT & EMERGENCY MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The findings showed that mostly unspecific stroke symptoms were presented when the dispatch code was other than stroke and that fall or lying position was the dominating problem.
The strength of the study is that authentic calls were analysed without the dispatcher or caller being aware of the study, and thus the study gives a view of real life situations.
A limitation of the study is that only 57% of eligible patients consented to participate in the study. It is possible that severe stroke, dysphasia or limited knowledge of Swedish may have hindered patients’ consenting to participation.
Another limitation is that the patients with stroke mimics and transient ischaemic attacks were not included. Calls dispatched as stroke but not discharged from hospital as such could undoubtedly yield an interesting comparison but were not included in the study due to methodological issues.
Introduction
Treatment of acute ischaemic stroke is time critical and requires immediate initiation to restore circulation.1 As many patients with stroke arrive by ambulance, time to treatment can be decreased with high priority dispatch of ambulance if stroke is already identified from the Emergency Medical Communication Center (EMCC).2 Thus, identification of stroke during the emergency call is of great importance as delay can jeopardise the possibility of thrombolysis and vascular intervention.
Stroke identification by dispatchers during emergency calls has been shown to vary between 31% and 57%.3–8 Identifying stroke during an emergency call can be a challenge as the patient can neither be seen nor examined and the caller is usually a third person.9 To improve identification of stroke, different protocols are used in the prehospital setting.5 ,10–16 One of the tests used to detect stroke is the Face-Arm-Speech-Time test (FAST), which is similar to the American Cincinnati Prehospital stroke scale. The test was developed for prehospital identification of stroke by checking for facial weakness, arm weakness and speech disturbances.14–16 FAST symptoms have been shown to be common in patients with stroke and the test is easy to perform for paramedics, physicians14 ,15 ,17 and laypeople.18 Through lectures on stroke, the test was introduced to dispatchers and ambulance personnel in Stockholm in 2008, when preparing for another study on priority of stroke.19 Since then, FAST can be found under the heading ‘Stroke’ in the electronic criteria-based index, ‘Medical Index’, used by dispatchers.
A previous study from our group showed a positive predictive value of 56% using FAST during emergency calls, which indicates limitations in identifying stroke using FAST by phone.19 In another study, it was shown that although FAST symptoms were noted in 27% of the medical records, FAST symptoms were mentioned during the initial emergency call in less than 5%.20 This implies that there is a need for more knowledge of how symptoms and findings of stroke are expressed during emergency calls, and raises the question of how FAST is used in the EMCC.
The aims of this study are to evaluate what findings callers present during an emergency call concerning stroke, if FAST symptoms are communicated and/or asked for, and if described FAST symptoms correlate to identification of stroke at the EMCC.
Materials and methods
This is a descriptive study of authentic emergency calls to the EMCC concerning patients with stroke in Stockholm, Sweden.
Participants and setting
The patients were recruited from a large teaching hospital with a catchment area of ≈600 000 inhabitants in Stockholm. Patients with a discharge diagnosis of stroke (International Classification of Diseases (ICD) 10 codes; I61, I63, I64) during January–June 2011 were identified from medical records and patients transported by ambulance to the hospital were eligible for the study.
In Stockholm, emergency calls are answered by call takers serving all emergency rescues. Health-related emergency calls are directed to nurses after relevant information such as address, condition of the patient, level of consciousness and breathing pattern has been obtained. The nurses summarise the complaint and the urgency in a predefined dispatch code associated to priority level. The ambulance is dispatched simultaneously. For support in evaluation and priority, the nurses can use an electronic criteria-based index of medical guidelines, the Medical Index. The Medical Index, containing 30 chapters, is mostly based on symptoms with some exceptions, for example, the stroke chapter. Thus, in order to be guided by the Medical Index, stroke needs to be suspected. There are no chapters describing unilateral weakness, facial weakness or speech disturbance. The guidelines recommend the highest priority (priority 1) for patients with suspected stroke and symptom onset within 6 h. The priority ranges from 1 to 4 where priority 1 indicates immediate dispatch and is used for life-threatening conditions.
Data collection
A data collection tool was used to retrospectively document the findings from recorded emergency calls. The recordings of the emergency calls were listened to repeatedly by AB and the findings were transferred to the data collecting tool.
The data colleting tool was developed by AB and KB through discussion and listening to 10 emergency calls; the tool included the first mentioned problem, described FAST symptoms and other presented symptoms. Additional data, such as priority, diagnosis and treatment, were retrieved from EMCC data and hospital medical records. In the data collection tool, lying position was added to fall, as a lying position may indicate an unwitnessed fall and inability to stand up due to stroke symptoms, and is therefore relevant. For the same reason, problems in walking were added to leg weakness.
Statistical analysis
Descriptive statistics are presented in frequencies and proportions with calculation using SPSS Statistics, V.22 (IBM Corporation 2010, Route 100, Somer, New York 10589, USA). For categorical data, the Fisher exact test was used to test significance. The 95% CI was calculated.21
Ethical consideration
The study was registered at http://www.clinicaltrials.gov, protocol ID; Stroke2010/703-31/2. The patients or their relatives were asked for consent to participate in the study, orally or by letter, in Swedish.
All patients received written information on the study and its purpose, and were notified that participation was voluntary, with patients having the right to terminate participation at any point without providing a reason. The consent included permitting the reading of medical records from the hospital and the ambulance, and allowing the recording of the authentic emergency call to be listened to. Consent to listen to the emergency calls was also obtained from the EMCC.
Results
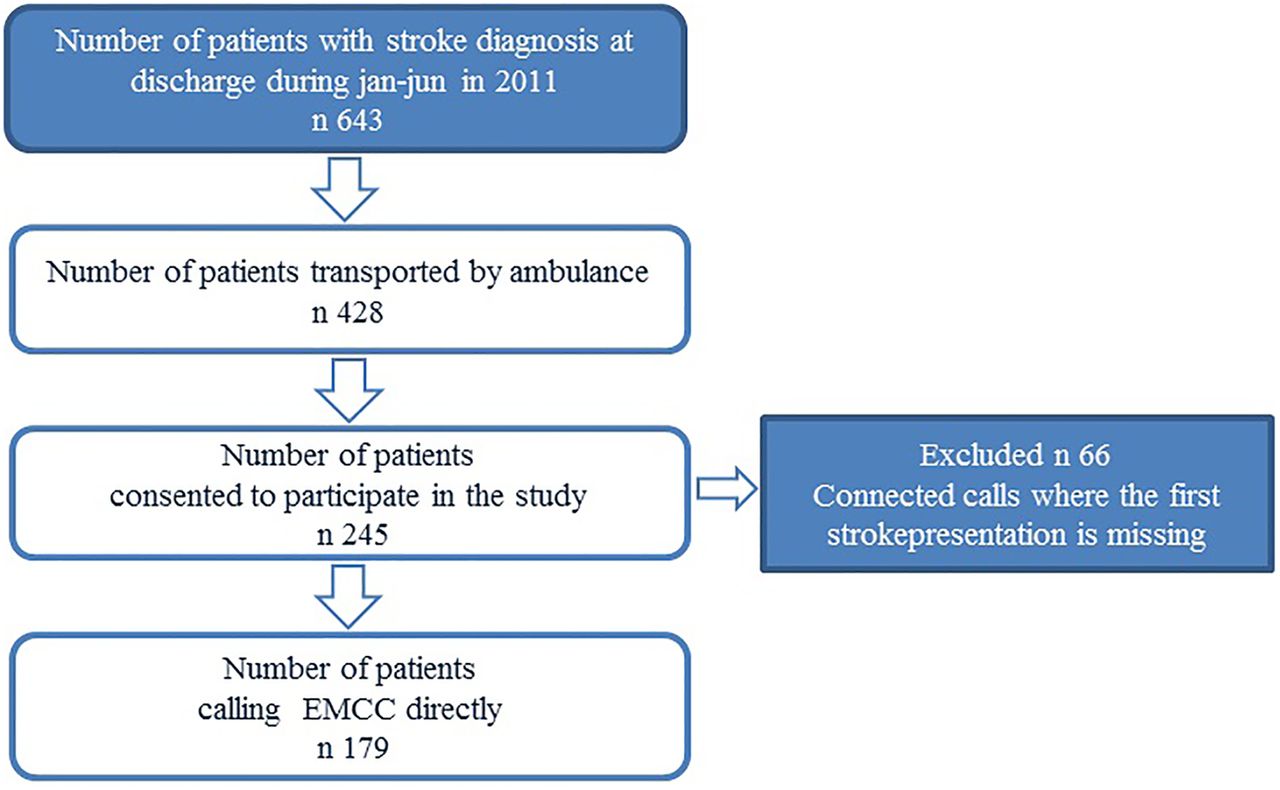
During the study period, 428 patients arriving at hospital by ambulance and discharged with a stroke diagnosis were identified and asked to participate in the study. Consent was given by 245 patients (57%). Of these, 66 patients were excluded as their calls were not direct calls to the EMCC (figure 1).

{kind=link}
Flow chart over study recruitment (EMCC, Emergency Medical Communication Center).
Finally, 179 patients were included in the study. Patients’ characteristics and background data are described in table 1. Median age was 79 years (26–97 minimum/maximum). In 85% (n=152), the patients’ diagnosis was ischaemic stroke and in 15% (n=27), intracerebral haemorrhage. An ambulance was dispatched with priority 1 in 64% of all calls (table 1). For patients with recorded symptom onset within 6 h, an ambulance was dispatched with priority 1 to 89% of patients. For patients with symptom onset after the 6 h window, an ambulance was dispatched with priority 1 to 43% of patients.
Patients’ characteristics and background data divided between patients with dispatch code ‘Stroke’ and dispatch code other than stroke
Symptoms presented
Speech disturbance was the most frequently presented problem (54%), followed by fall or lying position (38%) and altered mental status (27%; table 2). Suspicion of stroke was mentioned by the caller in 87 of the calls (49%; table 1) and coded ‘Stroke’ in 66 (76%) of these. The remaining 21 calls coded non-stroke presented symptoms and were prioritised similarly to the rest of the calls coded non-stroke without suspicion of stroke by the caller. At least one FAST symptom was presented in 64% of all calls and was presented spontaneously by the caller in 90% of those. A FAST symptom was mentioned by the caller first in the conversation in 35% of all calls.
Symptoms revealed during the emergency call, from the call taker and the nurse
Patients coded as ‘Stroke’
Stroke-specific symptoms were more commonly presented in the calls coded as ‘Stroke’ (table 2). A FAST symptom was presented in 80% of the calls and the most noted problem was speech disturbance (68%). In addition to stroke-specific symptoms, altered mental status (29%) and fall or lying position (22%) were commonly presented (table 2). Unconsciousness was described in 4% of the patients coded as stroke. Most patients with symptom onset within 6 h were coded ‘Stroke’ (74%), and ambulance was dispatched with priority 1 in 81% of those patients with symptom onset within 6 h, and dispatched as stroke.
Patients coded as other than stroke
Among calls coded as other than stroke, the most common code was ‘Uncertain data/seriously ill patient’ (52%) and half of those calls were dispatched with priority 1 (table 3). As presented in table 2, fall or lying position (66%) was the most frequently presented problem followed by speech disturbance (31%) and altered mental status (25%). FAST symptoms (35%) were presented less in these calls. Unconsciousness was reported in 25%, all dispatched as priority 1. Of the non-stroke dispatched calls, 32% were reported with onset within 6 h, and an ambulance was dispatched with priority 1 in 67% of the non-stroke dispatched calls with onset within 6 h.
An overview of the dispatch codes, in numbers, and the dispatch priority of the calls in the study
Sex differences
Women were older, median age 83 vs 74 years for men. The reported symptoms were similar except for altered mental status, which was more frequently reported in women (36%) than in men (18%; p=0.012).
Thrombolytic treatment was given to 21% of the patients with ischaemic stroke, 16% and 27% in women and men, respectively. Women treated with thrombolysis were older, median age 81 years for women compared with 65 years for men (p=0.001). Most callers were relatives of the patients, in 53% and 44% of male and female patients, respectively, or a healthcare provider, in 10% and 36% of male and female patients, respectively.
Discussion
In this descriptive analysis of emergency calls concerning patients with stroke, we found that a FAST symptom, that is, facial weakness, arm weakness or speech disturbance, was mentioned first in one-third of the calls. If a FAST symptom was mentioned, as it was in 64% of the calls, it was almost always spontaneously presented. We found that identification of stroke in emergency calls was more common in patients with one or more FAST symptoms. However, the presence of FAST symptoms was not synonymous with an identification of stroke, which was obvious from the finding that in 1/3 of calls coded as non-stroke, FAST symptoms were expressed. Presentation of FAST symptoms is not unique for stroke, which has previously been reported in emergency calls of non-stroke.6 ,22 In one of our previous studies, FAST symptoms were reported in 50% of the emergency calls with non-stroke diagnoses.19 It has to be noted that FAST was constructed based on data from medical records and physical examinations of patients with stroke prehospital and at hospital.10 ,14 ,17 When used in emergency calls, this study shows that if FAST symptoms are not obvious to the caller and mentioned the EMCC, dispatcher rarely asks for them.
An interesting finding in this study was the high frequency of fall or lying position presented and that this dominated the calls when stroke was not identified. In previous studies, fall or collapse has been reported as the first mentioned problem in 26%,20 and as the main problem in 21%, in the emergency calls of patients with stroke.23 A fall can be a consequence of stroke but a fall is also a common problem among elderly people in general.24 In a British study, falls were reported as the reason for emergency calls in 8%.25 In a study comparing stroke calls to non-stroke calls, fall/collapse was found to dominate in the stroke calls in 38%, and was present in 26% of the non-stroke calls.22 Another study showed falls to be a factor increasing the risk of misdiagnosing stroke.8 This is confirmed in our present study, and the risk seems particularly high if a combination of fall/lying position and less typical stroke symptoms are presented.
Previous study results vary according to sex differences in symptoms of stroke. When evaluating presence of symptoms in the clinic, no differences were detected,26 but in interviews, females have presented significantly more non-traditional stroke symptoms.27 ,28 Our results are in concordance with a study finding altered mental status to be significantly more frequent in female patients.28 As this is a non-specific symptom, stroke is less often suspected.
Altered mental status was another non-specific stroke symptom commonly expressed in the calls and was also previously reported to be a frequent symptom from patients in the emergency department, where 28% had a neurological aetiology.29 A previous study reported altered mental status to be one of several symptoms of patients with stroke not identified as stroke in hospital.30 Presentations of altered mental status and falls are common symptoms in emergency calls,24 ,29 and generally not acknowledged as symptoms of stroke. However, altered mental status might reflect symptoms such as speech disturbance, neglect or apraxia, which are stroke-specific symptoms but may be difficult to identify for a layman.
In this study, the dispatchers coded stroke in 64% of the stroke calls, which is comparable to the results of a recent study.8 It has been shown that mentioning of a suspicion of stroke by the caller has a strong association to stroke diagnosis.10 ,20 ,22 In view of that, it is notable that in one of four calls in our study, where suspicion of stroke was mentioned by the caller, no code of stroke was given by the dispatching nurse.
Priority in acute stroke is of the essence, as thrombolysis and thrombectomy depend on fast identification.1 ,31 The calls with dispatch codes other than stroke were less highly prioritised, 54% compared with 70% of the calls dispatched as stroke. The ambulance dispatch risks delay when stroke is not identified during an emergency call.2 ,20 ,32 Time of symptom onset was also noted as unknown more frequently in patients coded as non-stroke and probably reflects that time of onset was not asked for if stroke was not suspected.
A limitation of this study is the 57% participation rate. Ethical concerns hindered analyses of the non-participants and it is possible that severe stroke, dysphasia or limited knowledge of Swedish could have hindered patients’ consenting to participation. However, the findings are similar to other studies of emergency calls concerning stroke.3 ,6 ,8 ,19 ,20 ,22 ,23 ,33
Conclusion
The presence of FAST in the calls identified as stroke demonstrates advantages of the test. However, FAST symptoms were found to be present but not recognised in many calls coded as non-stroke. Almost all FAST symptoms were spontaneously reported by the caller. To increase the identification of stroke, the results imply that if fall/lying position or altered mental status are presented during the emergency call, the dispatcher should check for stroke, for example, by FAST test. Also, the callers’ suspicion of stroke should be a strong indicator for stroke during the emergency call.
Acknowledgments
The authors are grateful for the support and cooperation of the personnel at SOS Alarm AB in Stockholm and Lina Benson at Karolinska Institutet, Department of Clinical Science and Education, Södersjukhuset, for statistical discussion.
References
Footnotes
Contributors AB, MvE, MC and KB contributed with design, analysis and drafting the result. AB collected data. KS-G contributed with the design and drafting of the result. All authors approved publication of the paper and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Financial support was provided through the Erika Lederhausen Foundation for Center for Gender Medicine, Karolinska Institutet, the foundation for Women and Health (Stiftelsen Kvinnor och Hälsa), the Swedish Stroke Association and from the regional agreement on medical training and clinical research (A.L.F.) between the Stockholm County Council and Karolinska Institutet and Falck foundation. This study is part of the Fighting Stroke Project (Uppdrag Besegra Stroke) supported by the Swedish Heart and Lung Foundation, and Karolinska Institutet; funding from Friends of Karolinska Institutet, USA, and Johanniterorden, supports the project.
Competing interests None declared.
Ethics approval Regional Ethics Board (EPN:2010/703-31/2 and 13-2010 ).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.