Article Text

Abstract
Objective The aim of this meta-analysis was to explore the efficacy of sodium bicarbonate in preventing contrast-induced nephropathy (CIN).
Methods We searched PubMed, Medline and the Cochrane Library from 1 January 2004 to 1 August 2014. The effect estimate was expressed as a pooled OR with 95% CI, using the fixed-effects or random-effects model.
Results 20 randomised controlled trials (n=4280) were identified. Hydration with sodium bicarbonate was associated with a significant decrease in CIN among patients with pre-existing renal insufficiency (OR 0.67, 95% CI 0.47 to 0.96; p=0.027). However, moderate heterogeneity was noted across trials (I2=48%; p=0.008). Subgroup analyses indicated a better effect of sodium bicarbonate in studies using low-osmolar (OR 0.59, 95% CI 0.37 to 0.93; p=0.024) compared with iso-osmolar contrast agents (OR 0.76, 95% CI 0.43 to 1.34; p=0.351). The odds of CIN with sodium bicarbonate were lower in studies including only patients undergoing emergency (OR 0.16, 95% CI 0.05 to 0.51; p=0.002) compared with elective procedures (OR 0.76, 95% CI 0.54 to 1.06; p=0.105). Sodium bicarbonate was more beneficial in patients given a bolus injection before procedures (OR 0.15, 95% CI 0.04 to 0.54; p=0.004) compared with continuous infusion (OR 0.75, 95% CI 0.53 to 1.05; p=0.091). Sodium bicarbonate plus N-acetylcysteine (OR 0.17, 95% CI 0.04 to 0.79; p=0.024) was better than sodium bicarbonate alone (OR 0.71, 95% CI 0.48 to 1.03; p=0.071). The effect of sodium bicarbonate was considered greater in papers published before (OR 0.19, 95% CI 0.09 to 0.41; p=0.000) compared with after 2008 (OR 0.85, 95% CI 0.62 to 1.16; p=0.302). However, no significant differences were found in mortality (OR 0.69, 95% CI 0.36 to 1.32; p=0.263) or requirement for dialysis (OR 1.08, 95% CI 0.52 to 2.25; p=0.841).
Conclusions Sodium bicarbonate is effective in preventing CIN among patients with pre-existing renal insufficiency. However, it fails to lower the risks of dialysis and mortality and therefore cannot improve the clinical prognosis of patients with CIN.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
In this updated meta-analysis, we demonstrated that pre-procedural hydration with sodium bicarbonate was associated with a significant decrease in the incidence of contrast-induced nephropathy (CIN) among patients with pre-existing renal insufficiency.
-
We found that sodium bicarbonate did not lower the risks of dialysis and mortality and so did not improve the clinical prognosis of patients with CIN.
-
The new Jadad scale was used to assess the quality of reviewed articles.
-
Publication bias and moderate heterogeneity were found among the included trials.
Introduction
Contrast-induced nephropathy (CIN) is the third leading cause of in-hospital acute kidney injury,1–3 which is a serious complication of angiographic procedures resulting from the administration of contrast media. Although the definition of CIN varies, it is usually defined as an increase in the serum creatinine (Scr) level of 25% or an increase of 0.5 mg/dL (or 44 μmol/L) from baseline within 48–72 h of contrast exposure. CIN results in increased morbidity, prolonged hospital stay and increased healthcare expenditure, and is associated with higher mortality.4
The incidence of CIN in the general population is low, but increases exponentially in patients with high-risk factors, such as pre-existing renal insufficiency or diabetes mellitus.5 In a recent study, 21.7% of a group with pre-existing chronic renal insufficiency and 6.3% of a group without pre-existing chronic renal insufficiency developed CIN.6 Thus, baseline renal insufficiency may be a significant predisposing factor for CIN.
Sodium bicarbonate-based hydration has been proposed to prevent CIN. Some recent studies suggested that sodium bicarbonate had a more protective effect compared with sodium chloride for the prevention of CIN, while others did not.7–17 Although most previous meta-analyses supported the use of sodium bicarbonate, there may have been publication bias and none of the studies focused on patients with pre-existing renal insufficiency. Therefore, we performed this meta-analysis to determine the efficacy of sodium bicarbonate in preventing CIN among patients with renal insufficiency undergoing procedures needing contrast agents. In addition, differences in the requirement for dialysis and post-procedural death between the two groups in various studies were compared in this analysis.
Methods
Data sources and searches
We searched PubMed, Medline and the Cochrane Library from 1 January 2004 to 1 August 2014 without language limitations. Medical subject headings and keyword searches included the terms ‘contrast induced nephropathy’, ‘sodium bicarbonate’, ‘sodium chloride’, ‘saline’, ‘acute kidney injury’ and ‘renal failure’. The reference lists of selected articles were reviewed for other potentially relevant citations. In addition, the top 50 citations for each identified relevant study were searched by using the ‘related articles’ function of PubMed.
Study selection
Two investigators (BZ and LL) independently reviewed the titles and abstracts of all studies to identify those of interest. The online publications identified from the preliminary selection were then reviewed in full text to assess if the studies met the following inclusion criteria:
-
Participants: adult patients (≥18 years) with pre-existing renal insufficiency, defined as an Scr concentration of >1.1 mg/dL or estimated glomerular filtration rate (eGFR) of <60 mL/min18 or creatinine clearance rate of <60 mL/min9
-
Comparison: sodium bicarbonate (and/or N-acetylcysteine) versus saline (and/or N-acetylcysteine)
-
Outcome: relevance to the primary outcome of this study which is the incidence of CIN, while the secondary outcomes include the requirement for dialysis and mortality
-
Type of study: only randomised controlled trials (RCTs) were considered.
Exclusion criteria were as follows:
-
Insufficient data for extraction and analysis
-
Using N-acetylcysteine in only one arm.
Reviewers were not blinded to study authors or outcomes. The final inclusion of studies was based on the agreement of both reviewers.
Data extraction and quality assessment
Two independent reviewers (BZ and WBC) extracted relevant information from the literature including baseline clinical characteristics (mean age, percentage of males, risk factors other than renal insufficiency, baseline Scr, eGFR, procedures, interventions, type and volume of contrast media, hydration regimen, definition of CIN) (table 1), and data on primary (the incidence of CIN) and secondary outcomes (ie, the requirement for dialysis and mortality). CIN was defined variously in the studies, but was usually described as an absolute or relative increase in Scr level. Three studies defined CIN as a rise in Scr of 25% or more within 2–5 days of contrast exposure,12 ,19 ,20 while 13 studies regarded CIN as a rise of 0.5 mg/dL or a 25% increase in Scr within 2–4 days of contrast exposure. Two studies defined CIN as an increase in Scr of 0.5 mg/dL after the procedures.9 ,15 However, the remaining two trials differed from the above: CIN was defined in one trial as a decrease in eGFR of 25% within 4 days, and in the other as an absolute increase in Scr of at least 0.3 mg/dL or 50% or urine output of <0.5 mL/kg/h (>6 h) within 5 days.8 ,17 We assessed the quality of articles using the new Jadad scale after they were reviewed (table 2).
Quality assessment of included studies
Data synthesis and analysis
Data from included studies were combined and expressed as pooled ORs with 95% CIs. All analyses were performed on an ‘intention-to-treat’ basis. Initially, a fixed-effects model (Mantel–Haenzel method) was used in this meta-analysis. We evaluated heterogeneity across studies with Cochrane's Q test and I² statistics. If p<0.10, statistically significant heterogeneity was considered to be present. The I² statistic was used to quantify the magnitude of heterogeneity, with values of 0–30%, 31–50% and >50% representing mild, moderate and substantial heterogeneity, respectively. The outcome of fixed-effects model analysis demonstrated statistical heterogeneity, so we selected the random-effects model (Dersimonian and Laird method).
In light of the clinical and statistical heterogeneity across studies, subgroup analyses using the random-effects model were performed to assess the effect of sodium bicarbonate in various conditions, such as low-osmolar versus iso-osmolar contrast agent, emergency versus elective procedures, articles published before versus after 2008, and continuous versus bolus infusion of sodium bicarbonate (table 3). An influence analysis was carried out to evaluate how robust the pooled estimator was after individual studies were removed one at a time (figure 4). An individual study was suspected of exerting excessive influence if the point estimate of its omitted analysis lay outside the 95% CI of the summary analysis. Publication bias was assessed using Begg’s funnel plot and Egger’s regression asymmetry test (figure 5). All statistical analyses were performed using STATA software, V.12.0 (Stata Corp LP, College Station, Texas, USA).
Subgroup analyses used to assess the effect of sodium bicarbonate in various conditions
Results
A total of 837 articles were reviewed and the 20 studies meeting the inclusion criteria were included in the study (figure 1).

Flow diagram of included studies. NAC, N-acetylcysteine.
A detailed description of the baseline characteristics of the included studies is given in table 1. Patients in most studies underwent coronary angiography or interventional procedures. There were also seven studies which examined peripheral procedures, angioplasty, cardiopulmonary bypass and CT.8 ,18 ,19 ,21–24 The sodium bicarbonate hydration regimen in 13 studies was as described by Merten et al and consisted of sodium bicarbonate infusion at a rate of 3 mL/kg/h for 1 h before and 1 mL/kg/h for 6 h after the procedure.
The baseline characteristics of included studies
Primary outcome
CIN occurred in 158 of 2130 patients who received sodium bicarbonate compared with 217 of 2150 patients who received saline, demonstrating a lower overall incidence of CIN in the sodium bicarbonate group (figure 2). The pooled OR was 0.67 (95% CI 0.47 to 0.96; p=0.027), also in favour of sodium bicarbonate (figure 2).
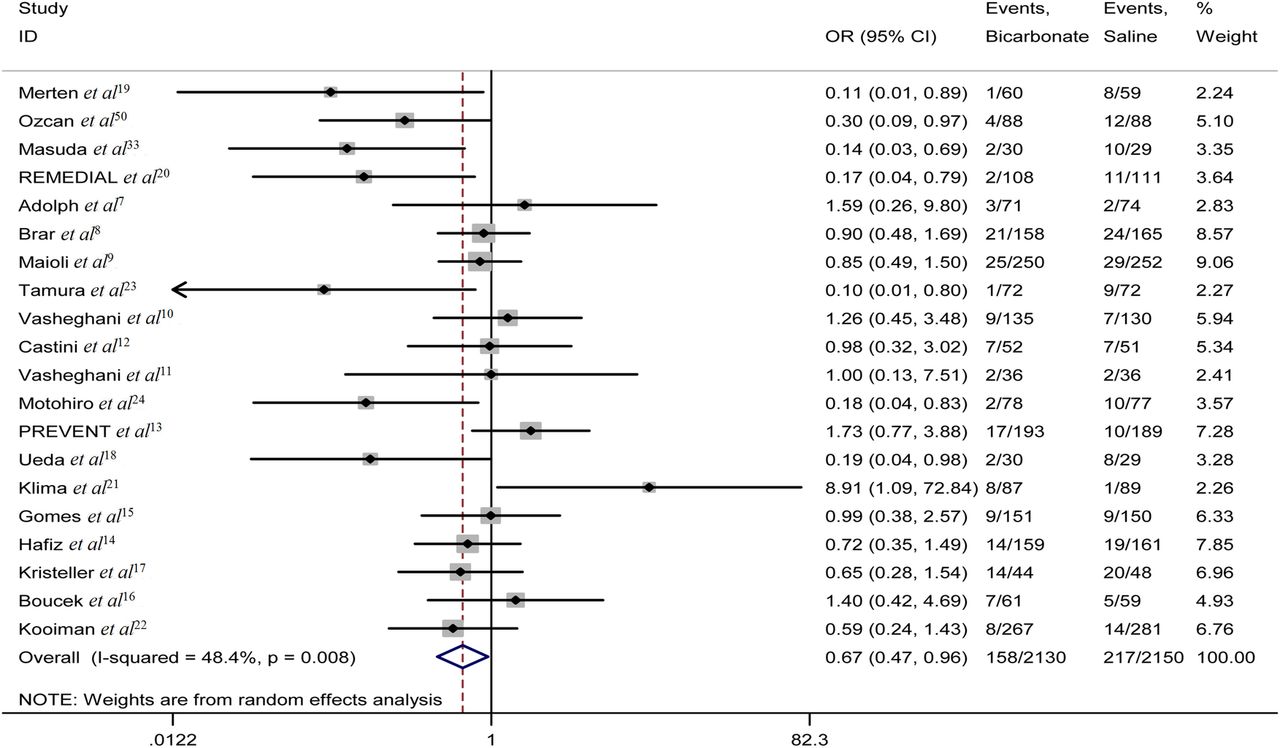
The forest plot of ORs of contrast-induced nephropathy.
However, moderate heterogeneity (I2=48%; p=0.008) across studies was found (figure 2). Therefore, subgroup analyses were conducted using a random-effects model and showed a more pronounced effect of sodium bicarbonate in studies using low-osmolar contrast media (OR 0.59, 95% CI 0.37 to 0.93; p=0.024) (table 3). Similarly, subgroup analysis by setting suggested a lower incidence of CIN with sodium bicarbonate in studies of patients undergoing emergency procedures (OR 0.16, 95% CI 0.05 to 0.51; p=0.002) (table 3). The effect of sodium bicarbonate was considered greater in articles published before 2008 (OR 0.19, 95% CI 0.09 to 0.41; p<0.001) (table 3). Subgroup analysis based on the method of sodium bicarbonate administration indicated a better effect in patients given a bolus injection (OR 0.15, 95% CI 0.04 to 0.54; p=0.004) (table 3). Sodium bicarbonate in combination with N-acetylcysteine (NAC) was better at preventing CIN (OR 0.17, 95% CI 0.04 to 0.79; p=0.024) (table 3).
Influence analysis showed that no individual study had an excessive influence on the overall estimate ORs or 95% CIs (figure 4).
Begg’s funnel plot and Egger’s test (p=0.396) implied there was no significant publication bias in this study (figure 5).
Secondary outcomes
The requirement for dialysis
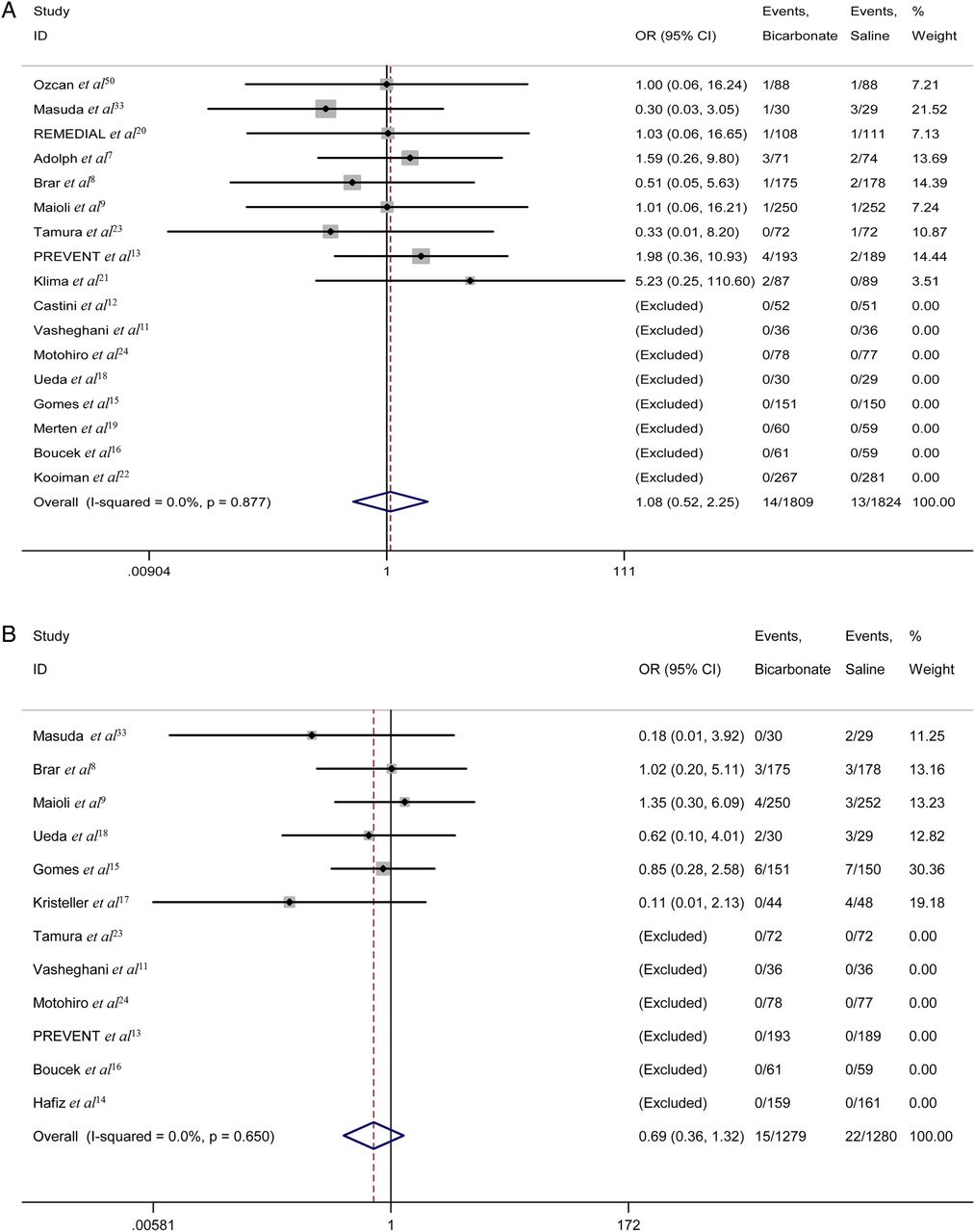
The requirement for dialysis was described in 17 studies (n=3633). In eight of these studies, no dialysis was carried out in either group.11 ,12 ,15 ,16 ,18 ,19 ,22 ,24 Overall, 14 of 1809 patients treated with sodium bicarbonate compared with 13 of 1824 patients treated with saline underwent dialysis. No statistically significant difference was observed (OR 1.08, 95% CI 0.52 to 2.25; p=0.841) (figure 3A). Nonetheless, the OR for the requirement for dialysis suggested that sodium bicarbonate was not better than saline in reducing the number of dialysis events.

(A) The forest plot of the requirement for dialysis. (B) The forest plot of mortality ORs.

The influence of an individual study on the overall estimates.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot with pseudo 95% confidence limits.
Mortality
Post-procedural death was described in 12 studies (n=2559). No deaths were reported in either group in six of these studies.11 ,13 ,14 ,16 ,23 ,24 There were 15 deaths in 1279 patients treated with sodium bicarbonate and 22 in 1280 patients treated with saline. Although there was no significant difference between the two arms (OR 0.69, 95% CI 0.36 to 1.32; p=0.263) (figure 3B), a trend toward lower mortality risk was found in the sodium bicarbonate arm compared with the saline arm.
Discussion
Although CIN is generally regarded as a transient decline in renal function after contrast procedures, it cannot be regarded as a benign complication25 ,26 as it accounts for 12% of all cases of acute renal failure.27 In an observational study, 0.8% of patients undergoing coronary angiography or interventional procedures started dialysis and 13% of them needed permanent dialysis.28 Furthermore, the development of CIN is associated with longer hospital stay, increased morbidity and mortality, and higher financial cost.
Various patient- and procedure-related risk factors may contribute to CIN.29 Pre-existing renal insufficiency and diabetes mellitus are the two main patient-related risk factors. Renal insufficiency was usually defined as a decrease in eGFR, and since the eGFR has to fall by 50% before a rise in Scr occurs, an elevated Scr level was used as the cut-off point for the definition of renal insufficiency.21 In a retrospective review of 938 patients with stable renal insufficiency, the overall incidence of CIN was 6.1%, while the incidence was 4.4%, 10.5% and 10.0% in patients whose eGFR was 45–60, 30–45 and ≤30 mL/min, respectively.30 Hence special care should be taken with patients with renal insufficiency.
Various mechanisms have been proposed to explain how sodium bicarbonate administration prevents CIN.31 ,32 One suggestion is that sodium bicarbonate makes tubular urine more alkaline, thus attenuating free radical formation and peroxide injury.28 Oxygen free radicals and peroxide are usually generated in acidic conditions, and so sodium bicarbonate infusion could increase the pH of local renal tissue to neutral or slightly alkaline, thereby reducing the production of free radicals and peroxide. Merten et al19 first introduced the administration of sodium bicarbonate at a concentration of 154 mmol/L to prevent CIN. In our study, the hydration regimens of 13 trials9–17 ,19–21 ,33 were similar to the Merten protocol. Although most previous systematic reviews and relevant meta-analyses demonstrated that sodium bicarbonate infusion could decrease the incidence of CIN,25 ,26 ,34–42 secondary clinical endpoints as diverse as renal replacement therapy and mortality were not improved. Furthermore, a retrospective cohort study of 7977 patients at Mayo Clinic drew a surprising conclusion: sodium bicarbonate was associated with an increased incidence of CIN.43 In contrast to most RCTs which used creatinine elevation within 48–72 h after contrast exposure to define CIN, From et al extended the definition time of CIN to a week as creatinine may peak 3–7 days after exposure to contrast. However, this issue remains to be discussed. Since all patients in our study had a history of renal insufficiency, Scr levels may have peaked earlier.
The underlying sources of moderate heterogeneity should be taken into account in this meta-analysis, because the study subjects, study settings and types of contrast media varied. In this case, subgroup analyses were conducted and the results revealed significant differences between emergency and elective procedures, with sodium bicarbonate providing more protection in the former than the latter. In a meta-analysis42 of the effect of sodium bicarbonate on preventing CIN, subgroup analyses also showed a more pronounced efficacy of sodium bicarbonate in three trials18 ,33 ,44 including patients undergoing emergency procedures compared with those undergoing elective procedures. However, the exact mechanism by which sodium bicarbonate results in a decrease incidence of CIN remains unknown; perhaps it is related to the method of administration and dosage. Similarly, sodium bicarbonate was more beneficial in patients who received low-osmolar contrast agents.45 ,46 However, since a significantly fewer number of patients received iso-osmolar contrast media (n=1189) compared with those receiving low-osmolar contrast media (n=2823), the main reason for the better effect of sodium bicarbonate was difficult to determine.
Although the use of NAC has been reported to reduce the incidence of CIN in many studies, the definitive effect of NAC has not yet been established. A number of trials and meta-analyses indicated that the combination of sodium bicarbonate and NAC is superior to either regimen alone in preventing CIN. Three studies20 ,44 ,47 included patients who received NAC in both groups after infusion of sodium bicarbonate or saline and the results favoured sodium bicarbonate. The BINARIO study48 indicated that hydration with sodium bicarbonate in addition to high-dose NAC in the setting of urgent percutaneous coronary intervention for ST-elevation myocardial infarction was associated with a net clinical benefit. However, Yang et al27 and Thayssen et al49 concluded that the use of NAC did not result in a significant reduction in the incidence of CIN. In our study, only one trial20 using NAC was included in the sub-analysis, the effect of which may be overestimated (OR 0.17, 95% CI 0.04 to 0.79; p=0.024). Accordingly, more large-scale and well designed RCTs are warranted to determine whether sodium bicarbonate plus NAC is more useful in preventing CIN than either alone.
Many studies have shown that patients with CIN are at greater risk of renal replacement therapy and death. In fact, almost all the dialysis and death events occurred in patients at high risk of CIN. Therefore, sodium bicarbonate alone would not have been effective in the presence of CIN and underlying disease, such as renal insufficiency and diabetes mellitus, perhaps explaining why we did not find significant differences in dialysis and mortality. However, insufficient power of included RCTs could be another reason. In this meta-analysis, as not all studies described renal replacement therapy, and mortality and sample sizes were relatively small, this issue remains to be explored in the future.
Conclusions
Our meta-analysis demonstrates that sodium bicarbonate is superior to saline for the prevention of CIN in patients with pre-existing renal insufficiency undergoing procedures using contrast media. However, use of sodium bicarbonate did not result in obvious benefit in decreasing the requirement for dialysis or reducing mortality. Therefore, larger trials are required to determine the efficacy of sodium bicarbonate in preventing CIN and improving the clinical prognosis of patients with CIN.
References
Footnotes
-
Twitter Follow Bin Zhang at @zhangbin
-
Contributors BZ, LL and WbC conducted the literature search. BZ wrote the manuscript. LL, WbC, ChL and SxZ reviewed, analysed and helped to write the manuscript. All authors contributed to the conception and design of this study.
-
Funding This study was supported by grants from the National Scientific Foundation of China (81171329) and the Guangdong Science Foundation (S2011010000790).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.