Article Text

Abstract
Objectives To determine whether statin treatment is associated with increased risk of haemorrhagic stroke (HS) in older women. A secondary objective was to evaluate HS risk in users of combined statin and antiplatelet treatment.
Design Observational study: secondary data analysis from the Women's Health Initiative (WHI) clinical trials.
Setting Women were recruited from 40 participating sites.
Participants Cohort of 68 132 women followed through 2005 (parent study) and for an additional 5 years in the extension study.
Main outcome measures Statin use was assessed at baseline and at follow-up visits (1, 3, 6 and 9 years). Women brought medications in original containers for inventory. Strokes were ascertained semiannually and centrally adjudicated. Risk of HS by statin use (time-varying covariate, with the ‘no use’ category as the referent) was estimated from Cox proportional hazard regression models adjusted for age (model 1); risk factors for HS (model 2); and possible confounders by indication (model 3). Prespecified subgroup analyses were conducted by use of antiplatelet medications.
Results Final models included 67 882 women (mean age, 63±7 years). Over a mean follow-up of 12 years, incidence rates of HS were 6.4/10 000 person-years among statin users and 5.0/10 000 person-years among non-users (p=0.11). The unadjusted risk of HS in statin users was 1.21 (CI 0.96 to 1.53); after adjusting for age and HS risk factors the HR was 0.98 (CI 0.76 to 1.26). Risk of HS was higher among women on statins and antiplatelet agents versus women on antiplatelet medications alone (HR=1.59; CI 1.03 to 2.47); p for interaction=0.011.
Conclusions This retrospective analysis did not show an association between statin use and HS risk among older women. HS risk was higher among women taking statins with antiplatelet agents. These findings warrant further investigation, given potential implications for clinical decision-making.
- PREVENTIVE MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Use of a large cohort of older female participants for which there is limited information on the association between statin use and haemorrhagic stroke (HS) and whether use of combined treatment with statin and antiplatelet medications poses additional risk.
-
Long duration of follow-up and excellent adjudication of HS.
-
Lack of plasma low-density lipoprotein (LDL) cholesterol data does not allow assessment of whether HS was associated with lower LDL levels.
-
Analysis conducted among a cohort of older women enrolled in the Women's Health Initiative Clinical Trials, limiting generalisability.
Background
Based on a number of randomised clinical trials that have established the efficacy of statins in the primary and secondary prevention of cardiovascular events,1 statin therapy is widely recommended for the treatment of hypercholesterolaemia and for the prevention of cardiovascular events.2 The implementation of the most recent guidelines on the treatment of blood cholesterol, however, may result in a number of individuals receiving statins that may reach up to one billion worldwide.3 Given the potential for large-scale ‘statinisation’ concerns about safety become more compelling.3
Consistent with the evidence from observational studies of an inverse association between plasma cholesterol levels and risk of intracerebral haemorrhage,4–7 some studies have reported an excess of haemorrhagic strokes (HSs) in patients treated with statins, particularly among individuals with a previous stroke.8–12 A meta-analysis of large randomised clinical trials of statin (or more statin) versus controls (or less statin) showed that statin treatment, compared with no statin, was associated with a 15% reduction in the overall risk of stroke which was largely driven by a reduction in the risk of ischaemic stroke, while there was a non-significant increase in the risk of HS (risk ratio (RR)=1.15; CI 0.93 to 1.41). A recent meta-analysis from the same group has confirmed a non-significant increase in the risk of HS (HR=1.15; CI 0.97 to 1.38 per 1.0 mmol/L reduction in low-density lipoprotein (LDL) cholesterol) among participants receiving statin treatment or a higher statin dose compared with those receiving no statin or a lower statin dose. However, only about 30% of participants in these trials were female and the median follow-up was 5 years.1
The primary aim of this analysis was to evaluate whether statin treatment is associated with an increased risk of HS in a female cohort of community-dwelling women enrolled in the Women's Health Initiative (WHI). This study has several important advantages: a large female population, a long follow-up duration (mean, 12 years) and the adjudication of all cerebrovascular events. In addition, since statins and antiplatelet agents are both recommended for the secondary prevention of cardiovascular disease and are frequently prescribed together in clinical practice, we evaluated whether women on statins who received concurrent treatment with antiplatelets medication were at increased risk.
Methods
Design and population
The WHI included a set of randomised clinical trials and a separate observational study.13 The present study is a secondary analysis of 68 132 women enrolled in the WHI clinical trials. Women enrolled in the observational study were not considered for this analysis because in this subcohort information about statin use was collected only at baseline and year 3 of follow-up. The clinical trials included randomised trials on hormone replacement therapy, diet modification and a calcium and vitamin D trial. To be eligible, women had to be 50–79 years old, postmenopausal and plan to reside in the study recruitment area for at least 3 years following enrolment. Exclusion criteria were medical conditions predictive of a survival time of less than 3 years, conditions inconsistent with study participation and adherence such as alcoholism, drug dependency, mental illness or dementia, and enrolment in another clinical trial. In addition, women were excluded from participation in the clinical trials for (1) reasons related to competing risk (invasive cancer in the past 10 years, breast cancer at any time or suspicion of breast cancer at baseline screening, acute myocardial infarction, stroke, or transient ischaemic attack (TIA) in the previous 6 months, known chronic active hepatitis or severe cirrhosis); (2) safety reasons (blood counts indicative of disease, severe hypertension or currently use of oral corticosteroids); (3) reasons related to adherence or retention. Each clinical trial also incorporated specific exclusion criteria. Among these, most relevant for the current analysis were exclusion criteria for enrolment in the hormone replacement therapy trial such as bleeding disorders, history of pulmonary embolism or deep vein thrombosis, current use of anticoagulants and tamoxifen, and unwillingness to discontinue outside use of hormone therapy (HT) at enrolment.14 All participants provided written informed consent according to the human subjects’ protection oversight at the 40 participating sites. Recruitment (1993–1998) was conducted through mailings to eligible women from large mailing lists and other strategies. Women were followed through 2005 as part of the original study and were offered the opportunity to continue for an additional 5 years in the WHI extension study. After obtaining informed consent for the extension study, yearly questionnaires were administered by mail between 2005 and 2010.
All participants in the clinical trials underwent a baseline visit including physical measurements (height, weight, blood pressure, heart rate, waist and hip circumferences), blood specimen collection, a medication/supplement inventory, and completion of questionnaires on medical and family/reproductive history, lifestyle/behavioural factors, and quality of life. Follow-up included a yearly on-site clinic visit and annual mailings (a medical history update and questionnaires about lifestyle and dietary habits, demographics, HT, and psychosocial variables). The main outcomes of the clinical trials were coronary heart disease (CHD), stroke, breast and colorectal cancer, osteoporotic fractures and total mortality.
Assessments
Exposure
The exposure was statin use. Study participants were instructed to bring all current medications and supplements in their original containers including prescription medications, over-the-counter medications, vitamins, minerals and supplements to clinic for inventory at baseline, 1-year, 3-year, 6-year and 9-year follow-up visits. The product or generic name of the medications on the label was entered into the database and matched to the corresponding item in a pharmacy database (Master Drug Data Base, Medi-Span, Indianapolis, Indiana, USA).
Since the prevalence of baseline statin use (7%) in the early years of recruitment for the WHI clinical trials (1993) was not representative of statin use during the following years, statin use was modelled as a time-varying variable in the analyses; that is, USE(t)=0 when the participant is not taking statin and USE(t)=1 once the participant begins taking statin. Information about statin dose (or dose of any other medication) was not available.
Antiplatelet drugs and anticoagulants
Use of these medications was assessed through a medications inventory at each planned visit as described above. Baseline assessments of both medications were used in this analysis.
Outcome
Stroke was defined as the rapid onset of a persistent neurological deficit attributable to an obstruction or rupture of the arterial system not known to be secondary to brain trauma, tumour, infection or other cause lasting more than 24 h and accompanied by a lesion compatible with acute stroke on a CT scan or MRI. Stroke was classified as ischaemic, haemorrhagic or other. Potential strokes were identified every 6 months through self-report from study participants or from family members and proxies. Details regarding the illness and hospitalisations were obtained via a standardised questionnaire administered by phone, in-person interview or self-completed form. Next, medical records were obtained for potential strokes, and trained physicians centrally adjudicated all strokes requiring a hospital stay using standard diagnostic criteria.15
Confounders
In addition to age, marital status (never, divorced or separated, widowed, married), education (high school or less, college or some college, postgraduate), income (less than $20 000, $20 000–$34 999, $35 000–$49 999, $50 000–$74 999, $75 000 or more, don’t know, unknown) and racial/ethnic background (Caucasian, African-American, other), we included variables that based on the literature are associated with a higher risk of HS.4 ,16 For hypertension, the available information in the WHI data set included self-reported history of hypertension as well as annual measurements of systolic and diastolic blood pressure. Blood pressure was measured in the right arm after participants had been seated quietly for at least 5 min according to standard procedures.17 For this analysis, hypertension was defined as self-reported history of treated hypertension OR measured baseline blood pressure ≥140/90.17 Alcohol intake (servings per week), history of stroke, smoking (never, former, current)16 and history of TIA or carotid endarterectomy/angioplasty were assessed using self-reported questionnaires. Waist and hip measurements were obtained to the nearest 0.5 cm at the level of the umbilicus and the fullest hip circumference, respectively. Physical activity was calculated from a self-reported questionnaire as energy expenditure from recreational physical activity (total MET-hours per week).
In addition to risk factors for HS, we included covariates that may lead to confounding by indication for statin use, such as diabetes, family history of CHD, body mass index ((weight in kilograms)/(height in metres)2 computed based on assessments of weight and height conducted at the baseline visit) and history of cardiac disease (a composite of previous coronary revascularisation procedures, atrial fibrillation, angina, myocardial infarction, cardiac arrest and heart failure), all assessed using self-reported questionnaires. Cholesterol levels were measured in only a small group of women, and thus we used history of elevated cholesterol needing pharmacological treatment as a proxy. For all analyses, we used baseline assessments of the variables listed above.
Statistical analysis
The baseline characteristics of the study population were computed and compared by appropriate statistical tests (Pearson's χ2 test for proportions and Student t test for continuous variables) according to HS status. The association between statins use and risk of HS was assessed using a Cox proportional hazards regression model with the ‘no use’ category as the reference group. Time to event was calculated as the interval between enrolment and the earliest of the following: date of adjudicated HS, date of last annual medical update or death. Women in the last two categories were censored at that date. Women who did not consent to join the extension study were included in the cohort and censored at the date of last medical update or death.
The following models were generated: unadjusted; age-adjusted; adjusted for demographics, risk factors for HS, and enrolment status in the HT, dietary modification and extension study (model 1); adjusted for variables included in model 1 plus variables that may lead to confounding by indication (model 2). A subgroup analysis was planned in women concurrently receiving antiplatelet medications to investigate whether women on statins and receiving concurrent treatment with these widely used medications were at increased risk.
Results are presented as unadjusted and adjusted HRs with 95% CIs; p values<0.05 were considered significant. All statistical analyses were performed using SAS/STAT V.9.3, SAS Institute, Cary, North Carolina, USA.
Results
Study population
Of the original cohort of 68 132 women enrolled in the WHI Clinical Trials, 67 882 were included in this analysis. Participants with no follow-up assessments (n=250) were excluded from the analysis and those missing covariate information (n=9747) were excluded from multivariate analyses requiring that covariate. A complete-case analysis gave substantially similar results.
Twenty-five per cent (n=17 192) of women received statin treatment at some time during the study period. The most commonly used statin was atorvastatin (n=5773; 33% of statin users) followed by simvastatin (n=4430; 25%). As for antiplatelet and anticoagulant agents, aspirin (n=12 617, 98.5%) was most commonly used at baseline, while only a minority of women received dipyridamole (n=109, 1%) or ticlopidine (n=59, 0.5%), and none received clopidogrel. Warfarin was the most commonly prescribed anticoagulant at baseline, however <1% of the study population was on anticoagulants.
Certain demographic features such as older age and low socioeconomic status were more prevalent in women who suffered HS during the study while there was no association with racial/ethnic background or education (table 1). As expected hypertension was strongly associated with HS while we did not observe associations with other known risk factors for HS such as smoking, alcohol intake, physical activity and waist-to-hip ratio. Moreover, with the exception of history of cardiac disease, there was no association between HS and factors that might lead to confounding by indication. Use of anticoagulants (2.4% vs 0.6%) or antiplatelet drugs (23% vs 19%) as well as a previous diagnosis of cerebrovascular disease or CHD was more prevalent among women who suffered a HS during the study.
Baseline characteristics by haemorrhagic stroke
Main analysis
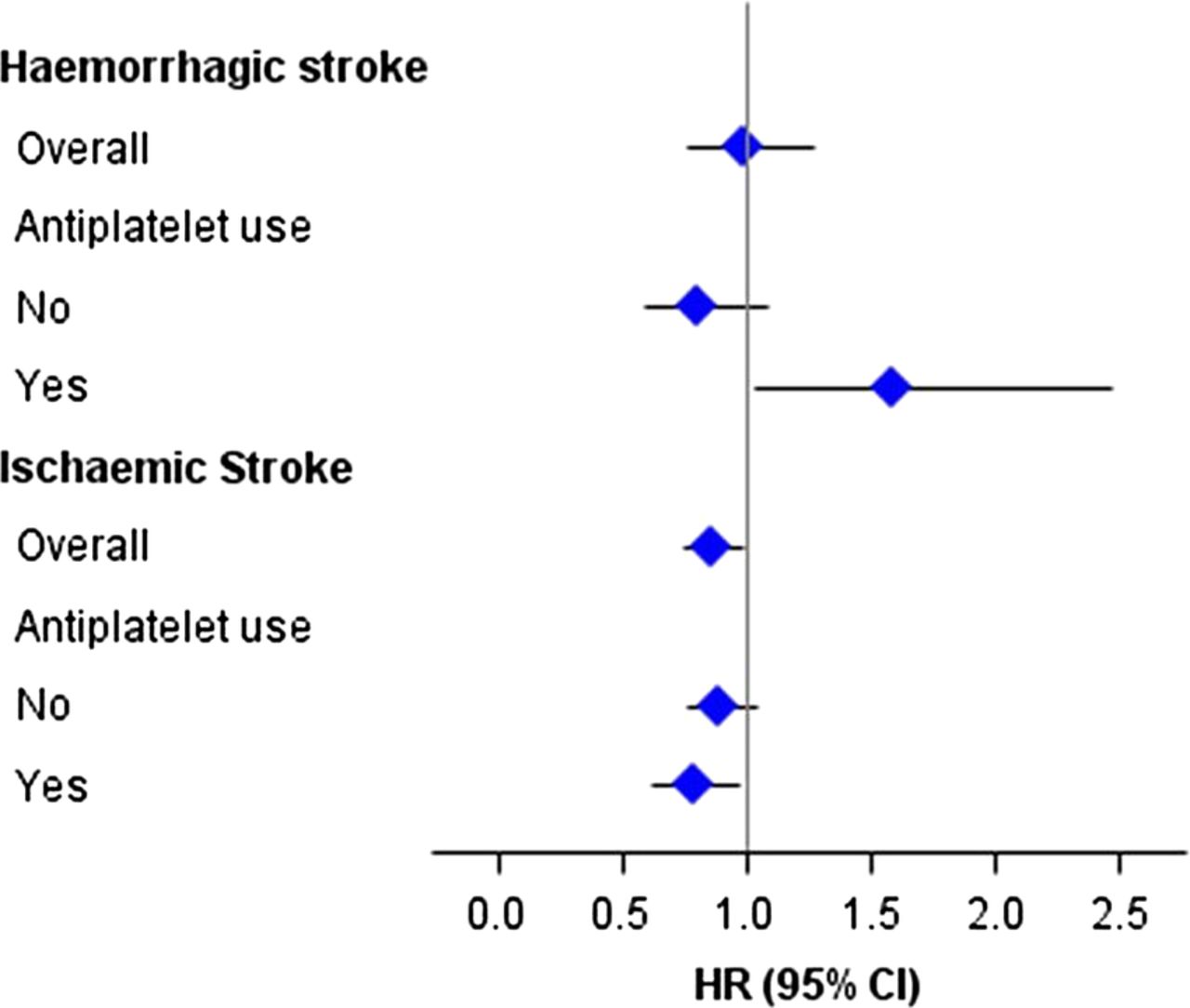
Over a mean duration of follow-up of 12 years, 421 HSs were documented: subarachnoid haemorrhage (n=104, 25%); intracerebral haemorrhage (n=296, 70%); other intracranial haemorrhage (n=21, 5%). The incidence rate of HS was 6.4/10 000 person-years among women on statins and 5.0/10 000 person-years among women not taking statin (p=0.11). The unadjusted risk of HS among women using statins was higher than among those who did not (HR=1.21; CI 0.96 to 1.53; table 2 and figure 1). After adjusting for age, hypertension and other risk factors for HS, the HR was 0.98 (CI 0.76 to 1.26). There was no evidence of confounding by indication, as variables included in model 2 did not substantially modify the HR.
Crude and adjusted HRs of haemorrhagic stroke by statin use

{kind=link}
Adjusted HRs of haemorrhagic and ischaemic stroke by statin use. Haemorrhagic stroke models adjusted for age, income, marital status, enrolment status in the hormone therapy (HT), dietary modification (DM) and extension study, baseline history of cerebrovascular disease, hypertension, use of antiplatelet agents and anticoagulants. Ischaemic stroke models adjusted for age, income, marital status, enrolment status in the HT, DM and extension study, baseline history of cerebrovascular disease, hypertension, use of antiplatelet agents, anticoagulants, body mass index, waist-to-hip ratio, physical activity, smoking status, baseline history of diabetes, and baseline history of high cholesterol requiring pharmacological treatment and history of cardiac disease.
Subgroup analyses by use of antiplatelet drugs at baseline indicated a higher risk of HS among women using both statins and antiplatelet drugs compared with women who were on antiplatelet treatment only (HR=1.59; CI 1.03 to 2.47), whereas women on statins who did not take antiplatelet medications had no risk elevation (HR=0.80; CI 0.58 to 1.09; p for interaction=0.011, table 2 and figure 1). The interaction term for anticoagulant use was non-significant (p=0.72); however, given the limited number of women on anticoagulants, the statistical power for these analyses was low. Analyses were repeated excluding women who were taking antiplatelet agents other than aspirin and yielded similar results.
Post hoc analyses
To put the above findings into a risk/benefit context, we examined whether statin treatment was associated with a lower risk of ischaemic stroke in the overall population and whether there was evidence for additional benefit among women taking aspirin and statin versus statin alone (table 3). Statin use was associated with a 14% reduction in the risk of ischaemic stroke (HR=0.86; CI 0.74 to 0.98). Subgroup analyses by use of antiplatelet drugs showed that women on statin and antiplatelet medications had a lower risk of ischaemic stroke compared with women on antiplatelet medications alone (HR=0.78; CI 0.62 to 0.97), but this reduction in risk was not significantly different from that of women on statin alone (p for interaction=0.27).
Crude and adjusted HRs of ischaemic and total stroke by statin use
Discussion
In this large population of ageing but otherwise healthy community-dwelling women, women who took statins at any time during follow-up had no increase in the risk of HS compared with women who received no statin treatment after adjustment for age and known risk factors for HS. A prespecified subgroup analysis by use of antiplatelet drugs showed a significantly higher risk of HS among women taking statins in association with antiplatelet drugs (such as aspirin) compared with women taking antiplatelet drugs alone.
Comparison with other studies
A large randomised clinical trial (40% women) found that patients with a history of stroke within the previous 6 months treated with high-dose atorvastatin had a 66% increase in the relative risk of HS compared with the placebo group.8 The risk was higher among males, older individuals and patients with a HS as the study entry event.9 ,10 The risk of HS was likewise increased in a subgroup of patients with a history of cerebrovascular disease but no prior HS enrolled in the Heart Protection Study.12 A systematic review of the effect of statin treatment in patients with a history of cerebrovascular disease showed an increased risk of HS persisting even after excluding patients with a HS as the entry event.11 The Cholesterol Treatment Trialist (CTT) meta-analysis of large randomised clinical trials of statin (or more statin) versus controls (or less statin) showed that statin treatment, compared with no statin, was associated with a non-significant increase in the risk of HS (RR=1.15; CI 0.93 to 1.41).18 A recent meta-analysis from the same group confirmed a non-significant increase in the risk of HS (HR=1.15; CI 0.97 to 1.38) per 1.0 mmol/L reduction in LDL cholesterol among participants receiving statin treatment or a higher statin dose compared with those receiving no statin or a lower statin dose.1 No subgroup analysis by use of antiplatelet agents or anticoagulants was performed in either meta-analysis. Another meta-analysis of primary and secondary prevention trials comprehensive of studies excluded from the CTT study found a small non-significant excess of intracranial haemorrhage in the statin group compared with controls (OR=1.08; 95% CI 0.88 to 1.32) and higher risk in secondary versus primary prevention studies.19 Since the authors did not have access to patient data, no subgroups analyses were conducted by use of antiplatelet agents or oral anticoagulants. In our analysis, models adjusted for demographics, socioeconomic variables and risk factors for HS did not show an increased risk of HS with statin use. Compared with the large meta-analyses and the clinical trials aforementioned, however, our study included an exclusively female population and less than 3% of participants had a history of stroke.
Our findings are consistent with those of other observational studies. A meta-analysis of observational studies20 as well as a retrospective study conducted among individuals with a history of ischaemic stroke21 indicated a lack of association between statin exposure and intracerebral haemorrhage (RR=0.94; 95% CI 0.81 to 1.10 and HR=0.87; 95% CI 0.65 to 1.17, respectively). In the latter study, subgroup analyses by use of anticoagulant and antiplatelet drugs showed a non-significant increase in the risk of intracerebral haemorrhage with anticoagulants, but not with antiplatelet agents use; antiplatelet agents however did not include aspirin.
There are several possible explanations for the association between statin treatment and increased risk of intracerebral bleeding. First, since cholesterol plays an important role in the integrity of the cerebral circulation,22 low levels of cholesterol could potentially increase the risk of vessel rupture. Several4–6 (but not all)23 epidemiological studies have in fact reported an inverse association between plasma cholesterol levels and risk of intracerebral haemorrhage. Second, statins have been shown to produce antithrombotic effects:24–26 mechanisms could involve inhibition of platelet aggregation, enhancing fibrinolysis, and reduced platelet expression of the protease-activated thrombin receptor.27
Possible implications
The finding of an increased risk of HS in women using a combination of statin and antiplatelet treatment could have important implications for populations at higher risk of HS. The incidence of HS in East Asian countries is relatively higher than in Western countries with a ratio of cerebral infarction to cerebral haemorrhage of 2:1 to 3:1, whereas in Western countries the ratio is 5:1 to 10:1.28 This finding should also be interpreted considering the benefits produced by statin treatment on ischaemic stroke. Post hoc analyses indicated that statin use was associated with a 14% reduction in the risk of ischaemic stroke in our population, a reduction in risk that is similar to that reported in meta-analyses of large clinical trials conducted in predominantly male populations.1 ,18 We did not find evidence for an additional effect of the combined treatment with antiplatelet agents and statins on ischaemic stroke to counterbalance the increased risk of HS observed with the combined treatment. The assessment of the benefit of combined aspirin and statin treatment on ischaemic stroke, however, was beyond the scope of this paper. A number of studies are currently studying the effect of the combined use of these and other medications (ie, the polypill) on cardiovascular events.29–31
Strengths and limitations
This study has a number of strengths, namely a large, healthy, ageing female population as well as a long duration of follow-up. To the best of our knowledge, there are no published studies assessing the risk of HS among female statin users. Furthermore, all HSs were adjudicated and statin exposure was assessed at each follow-up visits through an inventory of all medications.
There are also several limitations, of which the most important is the lack of measurements of LDL cholesterol. We used baseline history of high cholesterol as a proxy in multivariate analyses; however, adjustment for this important confounder was not optimal. Most importantly, we were unable to assess whether the risk of HS was higher among women with lower LDL levels. A second limitation was the design of this study, namely, a retrospective, post hoc analysis conducted among women enrolled in the WHI clinical trials. Third, although WHI participants were recruited among community-dwelling women, women included in this analysis were enrolled in clinical trials and thus subjected to intensive follow-up. The number of follow-up assessments, however, was similar between women receiving statins versus women who did not (data not shown). Fourth, despite adjustment for enrolment status in the different clinical trials we could not eliminate selection bias. In order to be enrolled, a series of conditions had to be excluded, and thus our findings do not apply to women presenting any of the exclusion criteria for participation in the WHI clinical trials, such as bleeding disorders or recent (<6 months) cardiovascular events. Our findings are also not generalisable to younger women, to men of any age and to non-white minorities. Fifth, information about the intensity of statin treatment was not collected and we were unable to determine if statins were used for the entire interval between visits (1–3 years) and if women were compliant with their medications. Sixth, HS is a term that actually embraces different clinical conditions, that is, among others, intracranial haemorrhage and subarachnoid haemorrhage. We did not have the power to assess whether statin treatment may differentially increase the risk of each specific condition. Since we did not have the power to assess effect modification by ethnicity, these findings need further exploration particularly among Asian women, who are at higher risk of HS.28 Finally, while statin use was modelled as a time-varying covariate, baseline assessments of antiplatelet and anticoagulant treatment as well as of other variables were used in this analysis.
Conclusions and future research
Statin use was not associated with an increased risk of HS among older community-dwelling women. A subgroup analysis showed that treatment with statins together with antiplatelet agents was associated with an increased risk of HS. Owing to the observational design of this study and the other limitations described above, these findings need to be interpreted with caution. Considering the widespread use of combined antiplatelet and statin treatment for the secondary prevention of cardiovascular events, our findings deserve further study and replication, in particular among older women and minorities at higher risk of HS.
References
Footnotes
-
Collaborators Short list of WHI investigators: Program Office: (National Heart, Lung, and Blood Institute, Bethesda, Maryland) Elizabeth Nabel, Jacques Rossouw, Shari Ludlam, Joan McGowan, Leslie Ford, and Nancy Geller. Clinical Coordinating Center: (Fred Hutchinson Cancer Research Center, Seattle, Washington, USA). Ross Prentice, Garnet Anderson, Andrea LaCroix, Charles L. Kooperberg, Ruth E. Patterson, Anne McTiernan; (Medical Research Labs, Highland Heights, Kentucky, USA) Evan Stein; (University of California at San Francisco, San Francisco, California, USA) Steven Cummings. Clinical Centers: (Albert Einstein College of Medicine, Bronx, New York, USA) SW-S; (Baylor College of Medicine, Houston, Texas, USA) Aleksandar Rajkovic; (Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA) JEM; (Brown University, Providence, Rhode Island, USA) Charles B Eaton; (Emory University, Atlanta, Georgia, USA) Lawrence Phillips; (Fred Hutchinson Cancer Research Center, Seattle, Washington, USA) Shirley Beresford; (George Washington University Medical Center, Washington District of Columbia, USA) LWM; (Los Angeles Biomedical Research Institute at Harbor- UCLA Medical Center, Torrance, California, USA) Rowan Chlebowski; (Kaiser Permanente Center for Health Research, Portland, Oregon, USA) Yvonne Michael; (Kaiser Permanente Division of Research, Oakland, California, USA) Bette Caan; (Medical College of Wisconsin, Milwaukee, Wisconsin, USA) Jane Morley Kotchen; (MedStar Research Institute/Howard University, Washington DC, USA) Barbara V Howard; (Northwestern University, Chicago/Evanston, Illinois, USA) Linda Van Horn; (Rush Medical Center, Chicago, Illinois, USA) Henry Black; (Stanford Prevention Research Center, Stanford, California, USA) Marcia L Stefanick; (State University of New York at Stony Brook, Stony Brook, New York, USA) Dorothy Lane; (The Ohio State University, Columbus, Ohio, USA) Rebecca Jackson; (University of Alabama at Birmingham, Birmingham, Alabama, USA) Cora E Lewis; (University of Arizona, Tucson/Phoenix, Arizona, USA) Cynthia A Thomson; (University at Buffalo, Buffalo, New York, USA) Jean Wactawski-Wende; (University of California at Davis, Sacramento, California, USA) John Robbins; (University of California at Irvine, California, USA) F Allan Hubbell; (University of California at Los Angeles, Los Angeles, California, USA) Lauren Nathan; (University of California at San Diego, LaJolla/Chula Vista, California, USA) Robert D Langer; (University of Cincinnati, Cincinnati, Ohio, USA) Margery Gass; (University of Florida, Gainesville/Jacksonville, Florida, USA) Marian Limacher; (University of Hawaii, Honolulu, Hawaii, USA) J David Curb; (University of Iowa, Iowa City/Davenport, Iowa, USA) Robert Wallace; (University of Massachusetts/Fallon Clinic, Worcester, Massachusetts, USA) JO; (University of Medicine and Dentistry of New Jersey, Newark, New Jersey, USA) Norman Lasser; (University of Miami, Miami, Florida, USA) Mary Jo O'Sullivan; (University of Minnesota, Minneapolis, Minnesota, USA) Karen Margolis; (University of Nevada, Reno, Nevada, USA) Robert Brunner; (University of North Carolina, Chapel Hill, North Carolina, USA) Gerardo Heiss; (University of Pittsburgh, Pittsburgh, Pennsylvania, USA) Lewis Kuller; (University of Tennessee Health Science Center, Memphis, Tennessee, USA) KCJ; (University of Texas Health Science Center, San Antonio, Texas, USA) Robert Brzyski; (University of Wisconsin, Madison, Wisconsin, USA) Gloria E Sarto; (Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA) Mara Vitolins; (Wayne State University School of Medicine/Hutzel Hospital, Detroit, Michigan, USA) Michael Simon. Women's Health Initiative Memory Study: (Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA) Sally Shumaker.
-
Contributors ES-B, JEM, CAA and KMH contributed to the conception and design of the study. KMH and CAA contributed to the acquisition of the data and did the statistical analysis. All authors contributed to the interpretation of the results. ES-B drafted the manuscript. All authors critically revised the manuscript for important intellectual content. KMH and CAA had full access to all of the study data and take responsibility for the integrity of the data and the accuracy of the data analysis. ES-B and JEM supervised the study. All the authors made a significant contribution to the research and the development of the manuscript and approved the final version for publication.
-
Funding The WHI program is funded by the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through contracts N01WH22110, 24152, 32100-2, 32105-6, 32108-9, 32111-13, 32115, 32118-32119, 32122, 42107-26, 42129-32, and 44221.
-
Competing interests JGR reports grants and personal fees from Amgen, grants from Amarin, grants from Astra-Zeneca, grants and personal fees from Merck, grants from Daiichi-Sankyo, grants and personal fees from Sanofi-Regeneron, grants and personal fees from LaRoche/Genetech, grants from Glaxo-Smith Kline and grants from Takeda.
-
Patient consent Obtained.
-
Ethics approval The WHI study was approved by the research ethics committees at each of the participating centres.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement: Technical appendix, statistical code, and data set available from the corresponding author at Brown University with prior written permission from the WHI P&P Committee.