Article Text

Abstract
Introduction In a context of constrained resources, the efficacy of interventions is a pivotal aim of healthcare systems worldwide. Efficacy of healthcare interventions is highly compromised if clinical reasoning (CR), the process that practitioners use to plan, direct, perform and reflect on client care, is not optimal. The CR process of health professionals is influenced by the institutional dimension (ie, legal, regulatory, administrative and organisational aspects) of their societal and practice contexts. Although several studies have been conducted with respect to the institutional dimension influencing health professionals’ CR, no clear integration of their results is yet available. The aim of this study is to synthesise and disseminate current knowledge on the influence of the institutional dimension of contexts on health professionals’ CR.
Methods and analysis A scoping study of the scientific literature from January 1980 to March 2013 will be undertaken to summarise and disseminate research findings about the influence of the institutional dimension on CR. Numerous databases (n=18) from three relevant fields (healthcare, health law and politics and management) will be searched. Extended search strategies will include the manual search of bibliographies, health-related websites, public registries and journals of interest. Data will be collected and analysed using a thematic chart and content analysis. A systematic multidisciplinary team approach will allow optimal identification of relevant studies, as well as effective and valid content analysis and dissemination of the results.
Discussion This scoping study will provide a rigorous, accurate and up-to-date synthesis of existing knowledge regarding: (1) those aspects of the institutional dimension of health professionals’ societal and practice contexts that impact their CR and (2) how these aspects influence health professionals’ CR. Through the synergy of a multidisciplinary research team from a wide range of expertise, clinical pertinence and an exhaustive dissemination of results to knowledge-users will be ensured.
- literature review
- research design
- evidence-based practice
- decision-making
- health services administration
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
- literature review
- research design
- evidence-based practice
- decision-making
- health services administration
Article summary
Article focus
-
This scoping study aims to synthesise and disseminate current knowledge on the influence of the institutional dimension of contexts on health professionals’ clinical reasoning.
Key messages
-
Clinicians are increasingly expected to successfully and systematically search for and synthesise scientific literature.
-
As the scoping studies’ framework is specifically designed to ‘…summarise and disseminate research findings’, it is a promising, clear and systematic procedure for clinicians. The seven stages are: (1) identifying the research questions; (2) identifying the relevant studies; (3) selecting the studies; (4) charting the data; (5) collating, summarising and reporting the results; (6) consulting and (7) disseminating the results.
-
A scoping study protocol could help clinicians, with the collaboration of colleagues, to successfully conduct a systematic and up-to-date synthesis of existing knowledge regarding any topic relevant to their practice.
Strengths and limitations of this study
-
This study will follow the rigorous scoping studies’ methodological framework, including the methodical retrieval of articles on aspects of the institutional dimension of societal and practice contexts, in numerous multidisciplinary databases. Enriched by the close collaboration of knowledge users from different levels (higher management and clinical practice) of varied institutions (rehabilitation centre and CSSS), results will provide an accurate and up-to-date synthesis of knowledge about: (1) particular aspects of the institutional dimension of societal and practice contexts and (2) their influence on health professionals’ CR. Moreover, aspects of the institutional dimension of societal and practice contexts that have not been covered by previous research will be identified and guide future interdisciplinary research. However, similar to other scoping research,54 this project will not appraise the quality of the evidence. Furthermore, as textbooks are not systematically included in electronic databases, information available in some textbooks might be missed. Nevertheless, the impact of this limitation is mitigated by the fact that textbooks are not a primary source for empirical results. Results obtained from this scoping study will permit a greater understanding of the aspects and influence of the institutional dimension of the societal and practice contexts on health professionals’ CR. This enhanced understanding will orient decision-makers regarding avenues of intervention to optimise the efficacy and effectiveness of healthcare services.
Introduction
In a context of constrained human and financial resources,1 the efficacy and effectiveness of interventions have become pivotal aims of contemporary healthcare systems worldwide.2 Indeed, effective interventions are essential in order to meet the increased demands for health services, which are largely attributable to: shifting societal demographics3; the increased range, sophistication and availability of technologies; the changing nature of consumer expectations and the costs of professional services rendered.4 ,5 The efficacy of health interventions depends on various factors related to: (1) the intervention, (2) the environment (place, time and context, resources of the professional and client, etc), (3) the health professional, (4) the client and (5) the interactions between the professional and the client.6 The efficacy of healthcare interventions is highly compromised if clinical reasoning (CR), a factor related to the health professional, is not optimal.7
Processes and content of CR: critical aspects of health professional interventions’ efficacy
Since CR, that is, “…the process that practitioners use to plan, direct, perform, and reflect on client care”,8 (p.314), leads to health professionals’ choice of interventions, it is a critical competence underpinning intervention efficacy.7 The importance of CR for health professionals is emphasised by, for example, the findings of a scoping study,9 in which the underlying cognitive processes and content of CR from numerous studies (n=652) were identified. Being influenced by both internal and external factors, two distinct but inter-related cognitive processes are involved in CR: problem-solving and decision-making10 (figure 1). Problem-solving refers to the way professionals combine formal theories with professional experiences to understand their client's situation.8 In turn, decision-making leads to professionals’ actions.11 ,12 During the problem-solving process leading to decision-making, two strategies are generally used, pattern recognition and hypothetico-deduction,13 as well as two tactics, heuristic and algorithmic.10 ,14 Cognitive tactics are influenced by the complexity of the problem to be solved.10 ,14 The cognitive strategies used are mainly related to the professionals’ level of expertise.13 ,15

Clinical reasoning processes and content. Inspired by Carrier, Levasseur, Bédard and Desrosiers, 2010.9
Expertise, which is one of the most important factors related to the health professional, exerts, through CR speed13 and richness of content,16 a pivotal influence on intervention efficacy. Experts can thus be flexible,8 fast, effective15 and creative17 in their interventions. Expertise level is reached through professional and personal experiences, and active reflection on those experiences,18 which is part of reflective practice19 and a critical skill for professionals.20 Experiences and reflective practice are both influenced by one powerful factor related to the environment: the societal and practice contexts (see table 1 for definitions of the concepts).
Concepts pertinent to the research project
Better understanding of the societal and practice contexts: towards a promising research intervention strategy to improve intervention efficacy
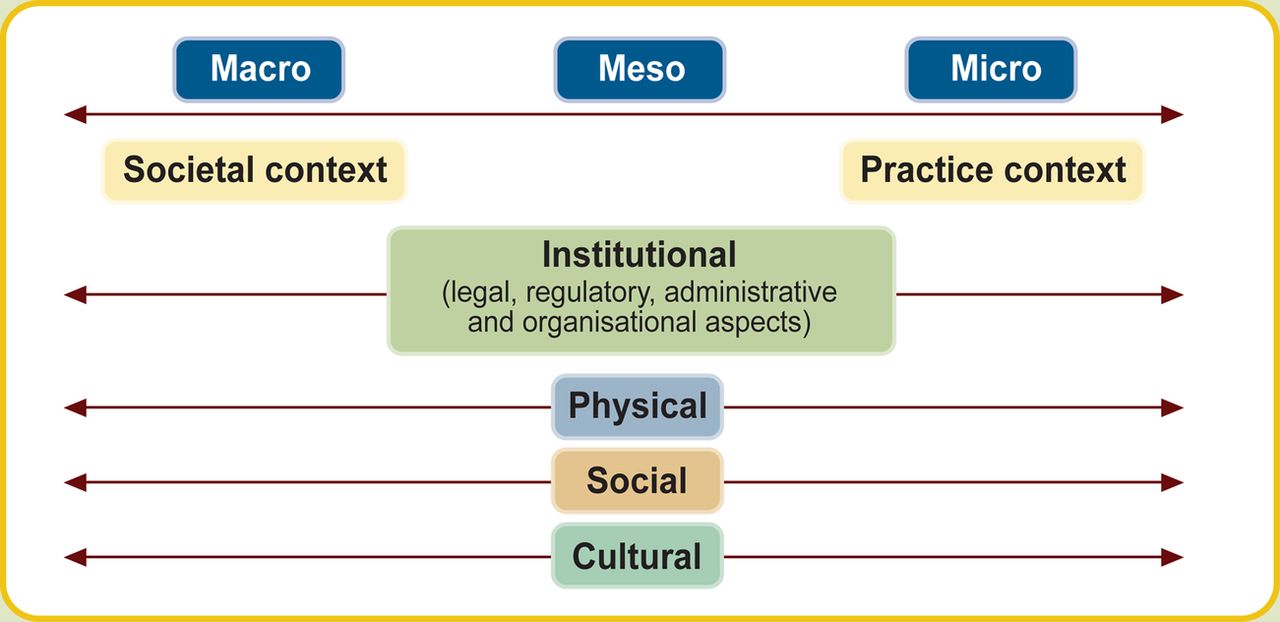
Situated on a continuum from a macro to micro level and consisting of four dimensions (physical, social, cultural and institutional; figure 2), societal and practice contexts mould professional and personal experiences. Pattern recognition, one of the two strategies involved in the CR problem-solving process (figure 1), relies on these professional and personal experiences and is indirectly affected by societal and practice contexts.24 Among the four dimensions of the context (figure 2), the institutional dimension includes the legal, regulatory, administrative and organisational aspects.21 ,22 These aspects influence the possibilities for improving CR and clinical competence. Indeed, organisational elements such as the time available25 and explicit administrative support26 (health institution internal policies) have been found to have an impact upon opportunities to reflect on practice. The societal and practice contexts affect the adoption of innovations and evidence-based practice guidelines,27 which can in turn influence the efficacy and quality of services.

{kind=link}
{kind=link}
Both the quality of services and access thereto, which are important outcomes of the organisational aspects (ie, relative to work organisation: schedule, waiting lists, etc) of the institutional dimension of both societal and practice contexts, are major global preoccupations.28–32 Indeed, quality and access to services are affected by the current discrepancy between healthcare demands and available resources,33 with potentially important personal and societal costs. Personal costs for clients and their caregivers may include diminished quality of life, incapacities and social participation restrictions and financial burden.28 ,34 Societal costs include, for example, workforce reductions35 ,36 and financial burden.37 In the light of these important consequences, considerable discussion regarding how to improve access, quality and continuity of care has taken place in the societal context38 which, as mentioned, can in turn influence the CR of health professionals.
One example of an intervention undertaken to improve access, quality and continuity of care is the 2003 legislative reforms enacted by the government of the province of Québec (Canada) that modified the institutional dimension of the societal and practice contexts. Among the changes to the societal context, the province was divided into 95 regions, the services in each of which are overseen respectively by a Centre de santé et de services sociaux (Health and Social Services Centre; CSSS).39 Each CSSS is now responsible for its respective population's health and must deliver services relating to three missions: hospital, residential and community care. This reform also impacted the institutional dimension of the practice context. The reform gave local institutions (the 95 CSSSs) increased responsibilities. Importantly, not only are these institutions and their health professionals required to deliver services, but also they have had to assume responsibility for the entire population in their territory without a proportional increase in their financial resources. They must identify people's healthcare needs, reach people in their environment and offer them the required services by contracting with other institutions.39 Furthermore, each CSSS and health professional is accountable to meet provincial or regional policy goals regarding the population served and services delivered.40 ,41 Changes in the institutional dimension of societal (eg, legislative reforms, healthcare policy modifications) and practice (eg, institutional goals) contexts are well documented. Studies have revealed the impact on health professionals of different aspects of the institutional dimension, for example, waiting lists (organisational aspect), institutional goals (administrative aspect) and ethical obligations (regulatory aspect). These significant impacts include: (1) pressure and ethical tensions affecting decision-making42 ,43; (2) fatigue and cognitive overload44 leading to interventions of suboptimal quality and increased risk of errors and (3) choice of interventions (CR) diverging from formal professional theories with a potential impact on quality.45 Importantly, although several studies have been conducted with respect to the institutional dimension and other aspects influencing health professionals’ CR, no clear integration of their results is yet available.
What is lacking from the literature?
Some advances have been made in regard to understanding the influence exerted by societal and practice contexts on elements linked to CR, for example: health professionals’ well-being46 and organisational commitment47; nature of services offered48; access to services49; interventions rendered50 and quality of interventions.51 Despite these advances and the acceptance regarding the importance of the institutional dimension of societal and practice contexts, a rigorous and integrated synthesis of the literature regarding which aspects influence health professionals’ CR and how they do so is lacking. Although various disciplines (health law and politics, management, cognitive psychology, health sciences) have studied the topic from different perspectives, to our knowledge, no attempt has been made to develop a comprehensive portrait rigorously integrating the results of the diverse empirical studies and the theoretical literature. In the light of the existing empirical studies and recent theoretical advances, it is now timely, innovative and advantageous to conduct a rigorous synthesis of the literature to provide a better understanding regarding how the institutional dimensions of societal and practice contexts influence CR.
Modifications to the societal context most certainly have an impact upon the practice context,21 ,52 influence health professionals’ CR and hence their interventions. However, the exact aspects of the institutional dimension of the societal and practice contexts and their impact on health professionals’ CR lack integration. Such understanding is essential with respect to their association with healthcare intervention efficacy and quality and, potentially, access. Indeed, because aspects of the institutional dimension influence interventions, their efficacy and quality, and CR leads to the choice of these interventions, a clear integration of the aspects of the institutional dimension that impact health professionals’ CR is pivotal to optimise interventions.
The overall objective of this scoping review was thus to synthesise and disseminate current knowledge on the influence of the institutional dimension of societal and practice contexts on health professionals’ CR. The specific objectives of this original contribution are to identify: (1) those aspects of the institutional dimension of health professionals’ societal and practice contexts that impact their CR; (2) how these aspects influence health professionals’ CR and (3) those aspects of the institutional dimension of the societal and practice contexts that have not been covered by previous research. Based on the Canadian Practice Process Framework21 and clear definition of concepts found in the CR literature (table 1), this research project will identify comprehensively those aspects having an influence on CR. This should help decision-makers and clinicians to enhance positive aspects while tempering negative ones, optimising efficacy, quality and, ultimately, access to services.
Methods and analysis
To synthesise and disseminate the current vast and diverse knowledge on the influence of the institutional dimension of the societal and practice contexts on health professionals’ CR, scoping studies’ methodological framework will be followed.53–55 Scoping studies are specifically designed to ‘…identify gaps in the evidence base where no research has been conducted’ and to ‘…summarise and disseminate research findings’54 (p.21). Seven stages are included in scoping studies’ framework (table 2). As the framework does not involve human participants, ethical approval is not requested.
Seven stages of the scoping study and implication of team members in the research project
Stage 1: identifying research questions
The research questions emerged from the clinical practice of three of the team members. Based on a comprehensive approach maximising the pertinence and probability of knowledge translation, these research questions were then refined by the research team (ie, authors of the manuscript, including experts and knowledge users and the research assistant). In order to optimally map current knowledge of the influence of the institutional dimension of societal and practice contexts on health professional CR, the research questions are broad and based on the Canadian Practice Process Framework21 and clear definitions of all pertinent concepts55: (1) What aspects of the institutional dimension of health professionals’ societal and practice contexts impact their CR? (2) How do these aspects influence health professionals’ CR? (3) What aspects of the institutional dimension of the societal and practice contexts have not been covered by previous research?
Stage 2: identifying relevant studies
Considering the multidisciplinary nature of the research questions, the planned research strategy is developed with the active contribution of experts, knowledge users (decision-maker and clinician) and information scientists from various fields. Identification of databases and keywords will be discussed by all research team members and validated by information scientists. Following this validation, an electronic search of numerous databases from three relevant fields (healthcare, health law and politics and management) will first be conducted by the research assistant with the supervision of the principal investigator and close support from the two information scientists. Specifically, the research assistant will report every 2 weeks to the principal investigator on the outcome of the search within each database and, when needed, will request technical support from the information scientists. The databases that will be included are detailed in table 3. The search will be limited to articles published in English, French and Italian (languages spoken by research team members), between January 1980 and March 2013. This timeline will allow: (1) retrieval of up-to-date articles considering major reforms worldwide in the organisation and delivery of healthcare services56 and (2) completion of the identification of the studies (stage 2) within the expected time schedule. To optimise search results, keywords will vary according to the specificity of each database and, when relevant, consider Medical Subject Headings (MeSH) (table 3).
Choice of databases and keywords
Stage 3: selecting the studies
A systematic team approach will be used to properly select the studies.55 First, articles will be screened for eligibility by title and, when available, by abstract, by the collaborator (CR content expert) and the research assistant. All articles (textbooks, empirical studies, opinion article, etc) that comprehensively inform aspects of institutional dimension of societal or practice contexts and their influence on health professionals’ CR will be retained. Extended search strategies will include the manual search of bibliographies, health-related websites (such as Health and social services department, agencies and institutions and health professionals’ regulatory boards), public registries (such as CUBIQ and Catalogue de la Bibliothèque Nationale du Québec) and journals of interest. Relevant literature proposed by experts in the field of health law and politics, management and CR will also be selected. Articles will be excluded if the aim is to: (1) validate an instrument to document the aspects of contexts, (2) offer practice guidelines regarding a specific intervention, (3) report only conference proceedings or (4) discuss the influence of contexts on other elements than CR. To discuss and resolve any ambiguity relating to study selection, the collaborator and the research assistant will meet with the principal researcher once a week. To ensure the clinical and managerial relevance of study selection, meetings of the whole team will also be held at the beginning (first focus group) and middle (second focus group) of this process. The final selection of all included articles will be made in agreement with both the collaborator and the research assistant. Any disagreement will be submitted to a third member of the team (practice context content expert). To ensure transparency and repeatability of the process55 and following PRISMA guidelines,57 a flow chart of the literature search will be developed and methodological choices will be documented.
Stage 4: charting the data
Through a preliminary reading, all included articles will be first categorised into detailed aspects of the institutional dimension of societal and practice contexts that influence CR. Such a detailed charting will permit identification not only of the specific aspects of the institutional dimension of both contexts that influence the processes, strategies, tactics or contents of CR, but also of the uncovered aspects. Emerging categories for each context will then be identified and lead to the collective development of the data charting form by the research team. Anticipated categories include: (1) aspects of the institutional dimension of societal and practice contexts: organisational; administrative; regulatory; legal characteristics and (2) cognitive processes (problem-solving or decision-making) and content of CR. As the link between formal evidence and current healthcare context is pivotal to knowledge translation, and because scoping studies must be related to a particular health service context,53 all emerging categories will be linked to the type of clinical setting (see description below). Development of the data charting form will be led by method and content experts, in collaboration with the rest of the team. Considering the iterative nature of scoping studies, the data charting form will evolve with the data collating process.55 Data will then be independently extracted and categorised by the collaborator and the research assistant. Validation of the process, including the data charting form, and its relevance to the research questions will be provided by research team discussion (table 2) after the first 10 articles and subsequently, as required.
Stage 5: collating, summarising and reporting results
This stage includes three steps: analysing data, reporting results and applying meaning to results.55
Step 1: analysing data
To characterise articles, contextual data will be first collected regarding the year of publication, country of origin, type of article (eg, empirical, theoretical, report, opinion, etc), type of study design (if applicable), health profession under study and type of clinical setting (eg, hospital, community-based, rehabilitation centre, etc). Contextual data will then be analysed through descriptive statistics (means and SDs or frequencies and percentages according to the number and type of variable; continuous or categorical, respectively).
Using content analysis,58 all data will be exhaustively analysed, organised and synthesised by both the collaborator and the research assistant. Analysis will also be discussed and one-third cocoded by part of the research team (table 2). More specifically, initial categories will be grouped by meaning, reduced and then classified into coherent, consistent, relevant, clearly defined, objectified and productive themes.58 Such qualitative methods to analyse documents ensure credibility of the results.55
Step 2: reporting results
The collaborator and the research assistant will numerically report data with graphs, tables and figures. Narrative data will be synthesised into relevant themes. Each theme will be contrasted to show similarities and differences relating to different clinical settings to increase applicability to knowledge users.
Step 3: applying meaning to results
Through discussion with content experts and knowledge users (third focus group), implications of results will be challenged and, when possible, broadened to include aspects of health governance, politics and finances. As their contribution provides direct relevance and feasibility input, the knowledge users’ implication is essential and will be significant for the current and the following stages of the project (table 2). Recommendations will thus consider clinical as well as managerial, political and financial implications.
Stage 6: consulting
In a process congruent with an integrated approach to knowledge translation and to ensure the clinical relevance of the results, knowledge users are an inherent part of the research project. Specifically, knowledge users will be consulted through a team meeting (at stage 2) and three focus groups (2 at stage 3 and 1 at stage 5) to optimise the methodology of the research project and to guide data collection and analysis. Furthermore, the implication of researchers and collaborators from different fields (health sciences, CR, public health, social sciences, health law and politics and management) will ensure a complementary and multidisciplinary project vision. Involving optimal collaboration, focus groups and meetings will permit the discussion and validation of the findings and inform future research. This collaborative process will involve preliminary findings from stage 5 (either in the form of a framework, themes or list of findings). Based on these results, knowledge users will then be able to support their decisions and interventions with the evidence and offer a higher level of meaning, content expertise and perspective to preliminary findings. This stage will also be considered as the beginning of knowledge transfer (dissemination strategies).
Stage 7: dissemination of results
Congruent with an integrated knowledge translation process, varied dissemination strategies targeting a wide audience (researchers, decision-makers and clinicians) will be used. Details as well as the expected impact of dissemination are provided in table 4.
Dissemination strategies of knowledge generated and expected outcomes
Discussion
First, the feasibility of this project will be discussed, followed by potential outcomes. Subsequently, strengths and limitations will be addressed.
Feasibility
The feasibility of the project is first insured by the quality of the experienced synergic research team. The researcher and collaborator team members have been selected based on their expertise and the required qualities to successfully carry out this project. Indeed, members include researchers from health sciences (n=2) and health law and politics (n=1), knowledge users from varied institutions (rehabilitation centre and CSSS), a collaborator specialising in CR and two information scientists, respectively, from health sciences and health law and politics. From a methodological perspective, two team members have already realised a total of seven scoping studies and have published and presented their results. Furthermore, the strong multidisciplinary perspective and clear definition of the contribution and role of every member will ensure optimal realisation and dissemination of the results. The specified contribution of researchers and collaborators in major decisions regarding project coordination, study selection and analysis of results (table 4) will also favour real involvement of team members. Second, the present project has been designed with specific and attainable objectives that can be carried out within the obtained grant's timeline and funding. The researcher and collaborator team members have already agreed to divide the work efficiently into stages (study identification and selection, data charting and analysis, dissemination of results), which will facilitate the overall completion of the project.
Outcomes
This scoping study will provide a rigorous, accurate and up-to-date synthesis of existing knowledge regarding: (1) what aspects of the institutional dimension of health professionals’ societal and practice contexts impact their CR and (2) how these aspects influence health professionals’ CR. Through the synergy of an exceptional research team from a wide range of expertise and multiple disciplines, clinical pertinence and exhaustive dissemination of results to knowledge-users will be ensured.
The knowledge generated will first be useful to decision-makers in the societal context (table 4). Indeed, results will allow them to better understand the impact of healthcare legislation and policies (societal context) on the clinicians’ choice of interventions (CR). In the current context of a discrepancy between the demands of services and the resources available, such an understanding could lead to modifications in the ways legislation and policies are used to optimise efficacy, quality and, ultimately, access to services. Finally, this understanding could also lead to the development of more comprehensive legislation and policies.
Second, because the project has been developed and will be realised with the participation of decision-makers in the practice context and clinicians, results will be useful to them (table 4). Knowledge about aspects of the institutional dimension of societal and practice contexts, in Québec, Canada and elsewhere, could offer a base for empirical comparison with the decision-makers and clinicians’ own institutional dimension. As the flexibility of the scoping review allows the description in sufficient detail of aspects identified in the literature as having an influence on CR, decision-makers and clinicians will be able to enhance positive aspects while mitigating negative ones. Results could also contribute to raising the optimal reflective practice of clinicians, enhancing their expertise and possibly improving the efficacy of their interventions. Educators and researchers will also benefit from the knowledge generated by the present project. On the one hand, the entry-level and continuing education of health professionals could be modified so as to better prepare students to the reality of clinical practice. On the other hand, researchers could use results to develop an assessment instrument of the institutional dimension of societal and practice contexts. In collaboration with decision-makers and clinicians, researchers will also be able to develop practice guidelines for decision-makers to optimise the positive influence of the institutional dimension of practice context on CR.
Finally, the present study will permit the identification of areas where insufficient evidence exists about the institutional dimension of the societal and practice contexts and where future interdisciplinary research is necessary (table 4). Initiation of contact with primary knowledge-users (clinicians and decision-makers) and coresearchers from multiple disciplines (health sciences, CR, public health, social sciences, health law and politics and management) of the present project will lead to the development and implementation of a high-quality, novel and inventive research programme on the influence of societal and practice contexts on health professionals’ CR.
Conclusion
The efficacy of interventions, a pivotal aim of healthcare systems worldwide, is highly compromised if health professionals’ CR is not optimal. One factor that influences their CR is the institutional dimension of health professionals’ societal and practice contexts. Although several studies have been conducted with respect to the institutional dimension influencing health professionals’ CR, no clear integration of their results is yet available. The aim of this study is thus to synthesise and disseminate current knowledge on the influence of the institutional dimension of societal and practice contexts on health professionals’ CR. In the current context of a discrepancy between the demands of services and the resources available, such a synthesis could lead to modifications in the ways legislation and policies are used to optimise efficacy, quality and, ultimately, access to services.
References
Footnotes
-
Contributors AC drafted the manuscript. ML and AF helped to draft and extensively revise the manuscript. MG and FL contributed to the identification of the database research strategies. All authors have approved the final manuscript and are willing to take the responsibility for appropriate portions of the content.
-
Funding This study is supported by the Canadian Institutes for Health Research (#250497). AC is a Canadian Institutes for Health Research (#250281), Fonds de recherche du Québec–Santé (#22754) and Canadian Occupational Therapy Foundation scholarship doctoral student.
-
Provenance and peer review Not commissioned; internally peer reviewed.