Article Text

Abstract
Objectives To describe the perspectives of clinicians and researchers on identifying, establishing and implementing core outcomes in haemodialysis and their expected impact.
Design Face-to-face, semistructured interviews; thematic analysis.
Stetting Twenty-seven centres across nine countries.
Participants Fifty-eight nephrologists (42 (72%) who were also triallists).
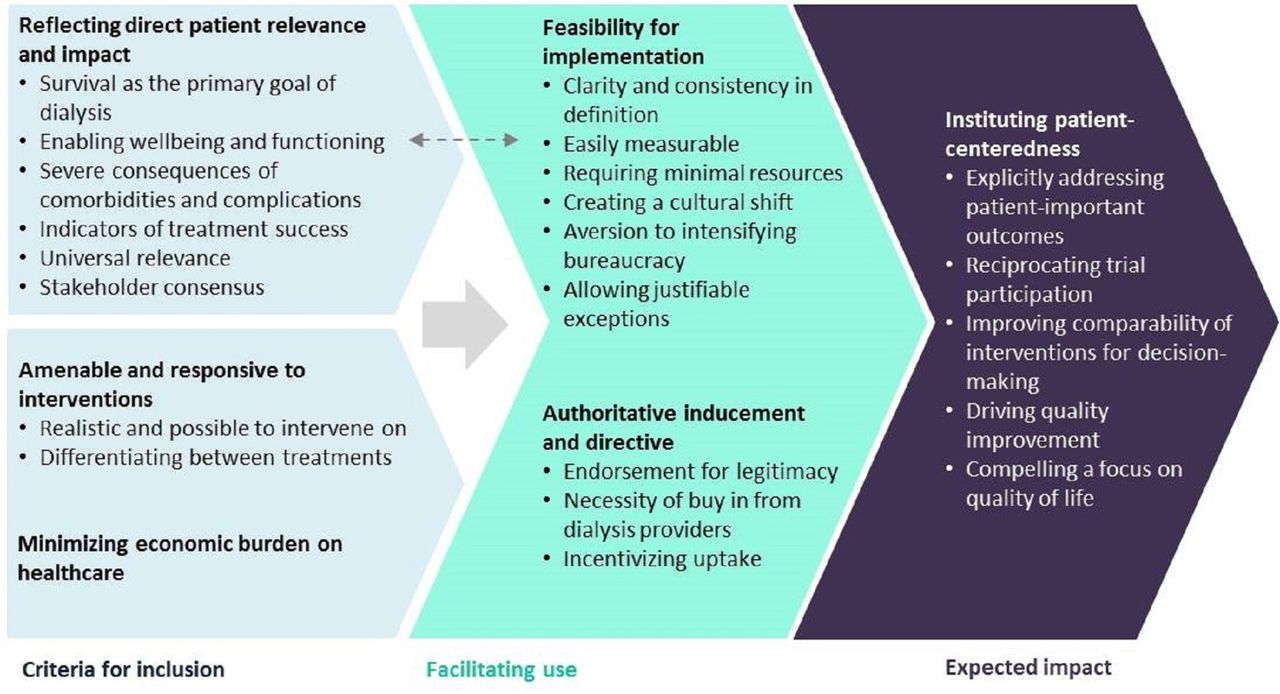
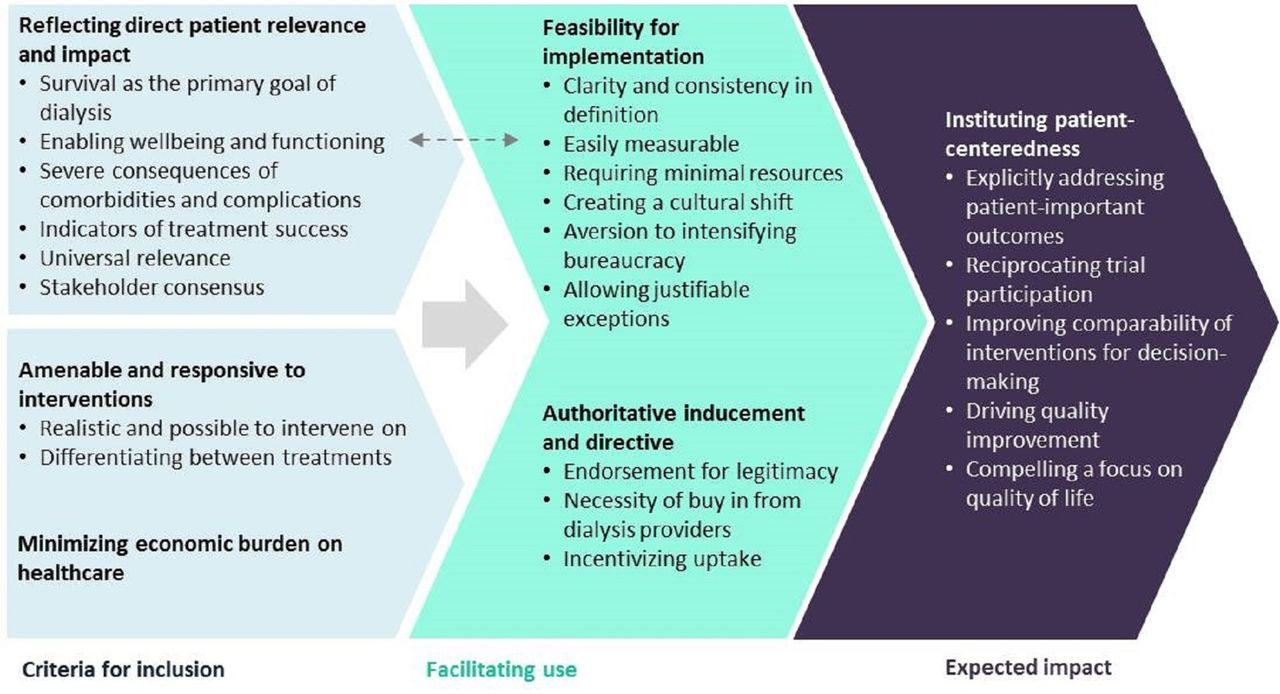
Results We identified six themes: reflecting direct patient relevance and impact (survival as the primary goal of dialysis, enabling well-being and functioning, severe consequences of comorbidities and complications, indicators of treatment success, universal relevance, stakeholder consensus); amenable and responsive to interventions (realistic and possible to intervene on, differentiating between treatments); reflective of economic burden on healthcare; feasibility of implementation (clarity and consistency in definition, easily measurable, requiring minimal resources, creating a cultural shift, aversion to intensifying bureaucracy, allowing justifiable exceptions); authoritative inducement and directive (endorsement for legitimacy, necessity of buy-in from dialysis providers, incentivising uptake); instituting patient-centredness (explicitly addressing patient-important outcomes, reciprocating trial participation, improving comparability of interventions for decision-making, driving quality improvement and compelling a focus on quality of life).
Conclusions Nephrologists emphasised that core outcomes should be relevant to patients, amenable to change, feasible to implement and supported by stakeholder organisations. They expected core outcomes would improve patient-centred care and outcomes.
- nephrology
- dialysis
- trials
- chronic renal failure
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Face-to-face, semistructured interviews were conducted with nephrologists purposively sampled across nine countries to obtain in-depth and diverse data on their perspectives on establishing core outcomes for trials in patients on haemodialysis.
The range of perspectives and challenges obtained will inform the development and implementation of core outcomes to be used in all trials in haemodialysis.
Nephrologists were all interviewed in English language and we focused on haemodialysis, which may potentially limit transferability of the findings.
Introduction
The value of randomised trials for informing practice and policy is currently limited by the inconsistency of outcomes that are reported, which can prevent meaningful assessment of the comparative effectiveness of interventions across trials. There is a tendency to measure and report outcomes that are expected to be responsive to the intervention and those that are easy to measure rather than what is important to decision making.1–3 Biochemical or surrogate endpoints, which are usually easier and feasible to measure, are frequently reported instead of ‘patient-important’ outcomes such as mortality and quality of life that are directly relevant to patients and clinicians for shared decision-making.4 5 Without standardised outcomes, outcome reporting may be biased, whereby researchers selectively report outcomes that show positive results and may lead to patient harm.6 7
The problems with outcome reporting in trials have been increasingly recognised and resulted in concerted efforts to establish core outcome sets.2 8 A core outcome set is defined as an agreed standardised set of outcomes that should be measured and reported, as a minimum, in all clinical trials in specific areas of health or healthcare.3 To date, more than 900 core outcomes studies have been registered in the Core Outcome Measures in Effectiveness Trials (COMET) database.9 Although specific core outcome sets in rheumatology (such as tender joints, swollen joins, pain, physician and patient global assessment and physical disability for rheumatoid arthritis) developed through the long-established Outcome Measures in Rheumatology (OMERACT) initiative have been shown to be increasingly used in trials,10 evaluations of the uptake of core outcomes are few in number and show variable results.10–14
The implementation of core outcomes requires extensive stakeholder engagement, and specifically, end-users (eg, triallists who use them and clinicians who apply the results) need to be involved in the process of establishing core outcomes.15 In recent studies, developers of core outcome sets have been interviewed to inform guidance for the conduct of core outcomes studies.2 15 However, the perspectives of end-users on the concept, identification and expected impact of core outcomes remain largely unknown. For example, the clinicians’ acceptance and role in advocating for core outcomes in clinical trials may impact on the implementation of core outcomes.
In the context of dialysis, for example, nephrologists can provide relevant insights on establishing and implementing core outcomes because of their direct role in patient care and involvement in trials. The aim of this study was to describe the attitudes and perspectives of nephrologists on outcomes that should be included in a core outcome set for haemodialysis, the implementation of core outcomes in trials in haemodialysis and their expected impact. This may inform strategies and mechanisms for implementing core outcomes in trials in haemodialysis and potentially in other settings.
Methods
Context
The international Standardised Outcomes in Nephrology (SONG) Initiative commenced in November 2014 to establish core outcomes across the spectrum of chronic kidney disease, with an initial focus on haemodialysis.16–19 As part of the SONG Initiative and prior to establishing the final core outcome set for haemodialysis (which included mortality, cardiovascular disease, fatigue and vascular access), interviews were conducted with nephrologists and this article focuses on the attitudes, expectations and opinions of nephrologists on establishing and implementing core outcomes in haemodialysis. Of note, core outcomes are to be reported in all trials within a given area because they have been explicitly identified by patients, caregivers and health professionals to be critically important for decision-making. The outcome is of importance to patients, even if the results of a particular trial show no difference in the outcome.’ We used the Consolidated Criteria for Reporting Qualitative Health Research (COREQ) to report this study20 (online supplementary file 1).
Supplementary file 1
Participant selection
Nephrologists involved in providing care for adults on haemodialysis were eligible to participate. We identified potential participants via our collegial and professional networks and asked a nominated nephrologist at each city internationally (London, Oxford, Cambridge, UK; Brussels, Belgium; Vienna, Austria; Berlin, Germany; Calgary, Canada; Houston, USA) to identify potential participants at their institution. Using a purposive sampling strategy, we selected participants to include a diverse range of demographic characteristics (age, gender, location), clinical experience (years of clinical experience in nephrology, size of haemodialysis unit) and research experience (involvement as an investigator in clinical trials and systematic reviews). All participants provided written informed and voluntary consent to participate.
Data collection
The interview guide was developed based on a literature review on core outcomes and discussion among the investigators (online supplementary file 2). Participants were asked what outcomes they believed were important to include in all trials in haemodialysis and their attitudes and beliefs about establishing and implementing core outcomes for haemodialysis. We defined a core outcome set as an agreed minimum set of outcomes to be measured and reported in all trials in a specific area,3 that is, in patients on haemodialysis. The first author (AT) conducted face-to-face semistructured interviews at office and conference venues during May to October 2015 until data saturation across all interview topics was reached. All interviews conducted in English, audio-recorded and transcribed verbatim.
Supplementary file 2
Data analysis
The transcripts were imported into HyperRESEARCH software V.3.3 (ResearchWare, USA). Thematic analysis involves identifying, examining, coding, comparing and grouping concepts to develop themes that describe the phenomenon being investigated and addresses the research question.21 Using thematic analysis, AT coded the transcripts line-by-line and inductively coded concepts relevant to the participant perspectives on establishing and implementing core outcomes in haemodialysis. The preliminary codes were reviewed by authors (TG, EO’L, AJ, AV) who independently read the transcripts and discussed any feedback with AT. This form of investigator triangulation can enhance the analytical framework and ensure that the full range and depth of data were captured in the initial analysis. We grouped similar concepts into themes and identified patterns, broader overarching concepts and links among the concepts and mapped these into a thematic schema. Preliminary findings were sent to participants for feedback (member-checking).
Patient and public involvement
Author TH is a patient who is one the SONG-HD Executive Committee and was involved in developing the research question, the design of this study and the data analysis. Patients were not involved in the recruitment and data collection as this was an interview study conducted with nephrologists.
Results
Participant characteristics
Of the 60 approached, 58 (97%) nephrologists from 27 dialysis units across nine countries were interviewed (table 1). Two did not participate because of conflicting schedules. Most participants (n=42, 72%) had conducted at least one clinical trial of whom 11 (19%) had been an investigator on more than 10 trials and 17 (29%) participants had published a systematic review. The mean duration of the interviews was 40 min. Fifty (86%) were conducted at a hospital (office or meeting room) and 8 (14%) at conference venues.
Participant demographic characteristics (n=58)
Themes
We identified six main themes: reflecting direct patient relevance and impact; amenable and responsive to interventions; burden on healthcare; feasibility for implementation; authoritative inducement and directive and instituting patient-centredness. The subthemes are described below and a thematic schema depicting how the themes relate to each other is provided in figure 1. Supporting quotations are provided in table 2.
{kind=link}
Thematic schema. Participants believed that core outcomes for haemodialysis should be directly relevant to patients and encompass mortality, indicators of well-being and functioning, serious comorbidities and treatment complication; those that consumed healthcare resources and could be potentially impacted by interventions. They emphasised that core outcomes should be applicable across healthcare contexts and populations. For implementation, the outcomes had to be clearly defined, valid and feasible though some were uncertain about whether quality of life outcomes were easily measurable. A cultural shift to focus on patient-important outcomes with support from external agencies was thought to facilitate uptake of core outcomes. The use of core outcomes was expected to strengthen patient-centred care and outcomes by compelling researchers and clinicians to give explicit attention to and address patient-centred outcomes.
Selected participant quotations for each theme
Reflecting direct patient relevance and impact
Survival as the primary goal of dialysis
The inclusion of mortality in a core outcome set was undisputed with participants defining this as a ‘classic hard endpoint’ that was ‘most important’ because of the ‘20% 1 year’ mortality rates in haemodialysis. As nephrologists, they felt primarily responsible for patient survival and discussed treatments with their patients in terms of its risk of mortality. Dialysis was intended ‘to keep patients alive’ and participants asserted that they would not ‘do a therapy that makes people feel better but kills them faster’. Some suggested that, with such a high event rate, a difference in mortality in trials could be reasonably expected. Others argued that a long follow-up and a large sample size would be required for a trial to show a difference in mortality because of the lack of powerful potential interventions and noted the paucity of positive trials for this outcome to date. Although mortality was a critically important outcome for participants, they emphasised that patient survival should be considered in conjunction with quality of life outcomes and comorbidities.
Enabling well-being and functioning
In recognising the severely impaired quality of life in patients on haemodialysis undergoing ‘an intensive, time-consuming, life-altering intervention’, participants felt that a core outcome set must capture the impact of treatment on ‘physical and social functioning’ to evaluate the patients’ capacity to maintain independence and be rehabilitated. This could encompass anxiety, depression, stress, fatigue and pain that limited a patient’s ability to ‘lead a normal life’, ‘do the things they want to’ and achieve life goals such as sustaining gainful employment, reaching educational milestones and having a family. Some participants, however, felt that these concepts were difficult to measure or may not be relevant to specific trials that did not target quality of life outcomes.
Severe consequences of comorbidities and complications
The very high prevalence of life-threatening comorbidities in the haemodialysis population was viewed by participants as strong justification for their inclusion as core outcomes. They consistently emphasised cardiovascular disease as the ‘greatest threat to haemodialysis patients … the number one reason that patients die’ and a key driver for hospitalisations. Some explained that the risk of cardiovascular disease could be ‘diffuse, non-concrete’ to patients and thus trials needed to report cardiovascular disease so nephrologists could ‘communicate better to patients of the various adverse consequences’. Other complications suggested included infection, cancer and bone disease based on severity and need for hospitalisation.
Indicators of treatment success
Participants also suggested that core outcomes could be those that defined the success of therapy including vascular access function, dialysis adequacy and treatment failure (eg, requiring change in dialysis modality). This would enable them to ‘understand the treatment better by looking at the outcomes in different ways’.
Universal relevance
Core outcomes had to be relevant, valid and acceptable across patient populations and healthcare contexts and measurable in different jurisdictions given the variability in access to technology and other resources. Participants suggested that core outcomes required cross-cultural relevance as ‘there are different beliefs about what happens with death and the sanctity of life’ or differences in how they may respond to symptoms—‘in some cultures people would exaggerate pain’.
Stakeholder consensus
Some participants acknowledged they were uncertain which outcomes would be of highest priority from the patient perspective and they were currently thinking about important outcomes ‘in a nebulous sort of way’. Thus, they supported systematic consensus among a broad range of stakeholders, including patients, physicians and policy makers, to identify important outcomes—‘the benefit of measuring it will outweigh the cost of measuring it, if there’s consensus around that, then that’s going to make the case for the benefits to measure it’.
Amenable and responsive to interventions
Realistic and possible to intervene on
For participants, a core outcome ‘should be something that we [nephrologists] could intervene upon’ because there was ‘not much point in worrying about things that we can’t do anything about’. For example, one participant doubted the feasibility of delivering an intervention that would alleviate financial impact, though some remarked that whether an outcome was ‘alterable’ (ie, potentially responsive to an intervention), could be difficult to determine without having been assessed in the first place. It was also contended that large trials were often trying to answer questions that were too ‘black and white’ and thus consistently showed no difference in mortality and morbidity, and some suggested that a ‘marked difference in patient experience’ may be more likely to be seen and relevant to report as an outcome in a trial.
Differentiating between treatments
Some thought core outcomes had to be potentially responsive to the intervention to detect existing differences and were uncertain about ‘mandating [specific outcomes] necessarily, unless the intervention was interested in it’.
Reflective of economic burden on healthcare
Participants considered outcomes that imposed substantial economic burdens on patients and the health system, such as hospitalisation and vascular access complications should be included as core outcomes.
Feasibility for implementation
Clarity and consistency in definition and interpretation
Developing standardised definitions for core outcomes was expected to be challenging and require detailed thought as the core outcome would have to ‘mean something to doctors, professionals and to mean something impactful to patients’ and ‘hold true across all studies and centres’.
Easily measurable
Participants emphasised that core outcomes should be relatively easy to measure in a ‘valid, meaningful way with minimal bias’ so that it could be assessed in ‘multiple settings across the world.’ For dimensions of quality of life such as fatigue, they suggested that patients should be able to report it but also expressed uncertainty about what measures were appropriate and validated for use in this setting.
Requiring minimal resources
Some participants were wary about mandating core outcomes that would require added cost and burden on researchers and patients—‘if for some reason you don’t have the budget or the time or the resources to do it, I don’t think we should put a black mark on that trial’.
Creating a culture shift
Participants believed that the uptake of core outcomes should be inspired by ‘real genuine interest’ and should happen ‘organically’ through a change in culture. They suggested coordinated and targeted funding towards studies that address the core outcomes and to shift the mindset of clinicians from numbers and blood results that are easy to measure, to focusing on outcomes that patients are interested in.
Aversion to intensifying bureaucracy
There was some concern and hesitation about enforcing the use of core outcomes as it was perceived to add bureaucratic pressure on investigators and may ‘deflate and deter them [ie, residents and fellows] from pursuing research’ as they had other pressing priorities to contend with.
Allowing justifiable exceptions
Some advocated that using core outcomes should come with a ‘proviso’ as a ‘trial may not be designed to measure them [the core outcomes], but if they still have to report them, it may not be received as well’.
Authoritative inducement and directive
Endorsement for legitimacy
Providing endorsed measures for outcomes was anticipated to be an effective strategy for facilitating the acceptance and use of core outcomes in trials.
Necessity of buy-in from dialysis providers
Dialysis providers (ie, industry) were identified as gatekeepers to the implementation of core outcomes—‘if you come up with a bunch of core outcomes that industry says we cannot deliver these, you might as well go home’. At the same time, some predicted that the dialysis industry would be unlikely to object to outcomes that reflected what patients and physicians considered important in order to avoid ‘terrible publicity’.
Incentivising uptake
In principle, ‘tying payment’ to core outcomes would be effective and incentives could be given to exemplary units. Another participant suggested that core outcomes should be able to be commissioned—‘you could commission around renal failure and hospitalization, and vascular utilization…I could commission for how much travel the patients have done and I would put in inducements to support travel for people on haemodialysis’.
Instituting patient-centredness
Explicitly addressing patient-important outcomes
Some expected that implementing core outcomes would shift current clinical practice towards an explicit focus on patient-centred care—‘the most obvious reason to have a set of core outcomes is that we should enforce or at least try to provide care to all of our patients such that all of these core outcomes are met. I’m glad that somebody’s going to do trials about them, but more importantly, I want our patients to realise, or notice that, we are listening to what they think is important to them’.
Reciprocating trial participation
Reporting core outcomes was seen to align with ethics of research conduct—‘patients give us their time and effort to participate in the trial, they need to get something out of that, that is valuable to them’.
Improving comparability of interventions for decision-making
Participants were aware of the heterogeneity of outcomes that prevented their ability to assess the comparative effect of interventions—‘we need to be comparing apples with apples; we’re talking about meta-analyses and getting a fruit salad’. Having standardised outcomes that were consistently reported would allow them to make informed decisions based on the totality of the available trial evidence.
Driving quality improvement
Although core outcomes would be primarily established for trials, some participants believed it would support quality improvement initiatives and inform ways to modify approaches to clinical care and address outcomes that matter to patients and clinicians.
Compelling a focus on quality of life
Participants expected that a core quality of life outcome would translate into routine clinical practice and prompt nephrologists to undertake explicit and systematic assessment of patient concerns and priorities. It provided an opportunity to align goals as ‘physicians and scientists look at the world differently than the patient does’. Some participants remarked that this would ‘force a lot of providers who see their patients like cattle, a way of making money…a sort of billing code’ to address patient-centred outcomes.
Conclusion
Nephrologists supported the need for a consensus-based core outcome set to be reported in every trial in haemodialysis to enable treatment decisions based on outcomes that were regarded as important to patients and clinicians. They agreed that core outcomes should have direct relevance and impact on patients, which necessitated the inclusion of mortality, well-being and functioning, serious comorbidities (namely cardiovascular disease) and other indicators of treatment success. The implications to healthcare resource of including the outcomes in trials were considered, as was the plausibility of the outcome being able to measure the benefits and harms (effectiveness) of an intervention. Nephrologists emphasised that core outcomes must be broadly applicable across healthcare jurisdictions and patient populations, particularly in low-income and non-English speaking countries.
To ensure feasibility for implementing core outcomes, nephrologists suggested providing clear and consistent definitions for the outcome, making available valid and simple measures that can be used across all trials, creating a cultural shift through targeted funding schemes for research that address core outcomes and minimising bureaucratic burden on researchers. They believed endorsement, buy-in from gatekeeper stakeholders (eg, dialysis providers) and incentivisation would support implementation. Nephrologists perceived core outcomes as an opportunity to strengthen patient-provider communication, shared decision making education and patient-focused research by providing a mechanism for researchers and clinicians to explicitly address the patients’ well-being, defining targets for quality improvement and improving the consistency and relevance of evidence to inform shared decision about treatment.
Broadly, the types of outcomes suggested by nephrologists are similar to the OMERACT core areas of death, life impact (how a patient feels or functions), pathophysiological manifestations (disease-specific clinical and psychological signs, biomarkers and potential surrogate outcome measures) and resource use (financial and other costs of the health condition and interventions).22 However, establishing a core outcome set was perceived by nephrologists as an endeavour to focus much needed attention towards patient-reported outcomes, clinical outcomes (eg, cardiovascular disease) and treatment complications (eg, vascular access problems), rather than biochemical parameters such as serum phosphate, calcium and parathyroid hormone. This may reflect concerns about the widespread use of non-validated biochemical outcomes in trials and clinical practice in nephrology.23 24 In relation to the core area of ‘resource use’, nephrologists considered the burden of comorbidities and treatment complications on healthcare consumption (eg, hospitalisation) but did not explicitly suggest including economic evaluations as a core outcome.
Nephrologists also raised principles that reflect components of the OMERACT Filter for the development and validation of outcome measures: truth (measures what is intended and is unbiased and relevant), discrimination (reliability and sensitivity to change) and feasibility1 as well as items in the recent COMET-Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) guidelines.8 A challenge raised by nephrologists was the lack of validated and appropriate patient-reported outcome measures for use in patients on haemodialysis.25–27 Some also argued that interventions may not be targeted at improving quality of life outcomes. This highlights a tension between responsiveness to an intervention and importance as the basis for identifying a core outcome. While responsiveness to an intervention may be important to triallists, patients and caregivers want to know about the impact of outcomes that matter to them—even if the trial shows no difference.28
The COSMIN-COMET guideline stipulates ‘regulatory agency’s requirement for approval’ as a feasibility aspect8 and while this may have helped to improve the uptake of the OMERACT core outcomes for rheumatoid arthritis,10 some nephrologists were concerned about the potential burden on researchers. In addition to COSMIN-COMET feasibility items, nephrologists suggested that advocacy or endorsement by external agencies or setting up targeted funding calls to address core outcomes may promote a cultural shift to support the uptake of core outcomes. Of note, the UK National Institute for Health Research guidance for grant applications advises researchers to include core outcomes in their proposal.29 Similarly, the UK Marie Curie Research Grants scheme (total US$2 million) recently sought proposals for research priorities identified by a research priority partnership with patients and health professionals in palliative and end-of-life care.30 We suggest that targeted or prioritised funding for trials or research proposals that address core outcomes would be conceivable and effective for implementation.
Our study provides novel empiric data about the perspectives of nephrologists on core outcomes: what they, in principle, believe should be included as core outcomes, considerations for feasibility for implementation and the expected impact of core outcomes. We used purposive sampling and obtained a diverse range of demographic characteristics and clinical and research experience. However, our study has some potential limitations. The transferability of the findings to low-income settings is uncertain as the participants were from high-income countries. However, they emphasised cross-cultural applicability and validity as a key consideration in establishing core outcomes. We acknowledge that these data were collected prior to establishing the core outcome set for haemodialysis. Therefore, perspectives on implementing the specific cores outcomes for haemodialysis that have since been established (eg, cardiovascular disease, fatigue, mortality, vascular access function) may not have been specifically discussed. However, clinician’s perspectives on implementing the specific core outcomes have been detailed in subsequent workshop reports.17 31 32 Also, we only included nephrologists in the study, though the similarities with broader frameworks1 3 8 22 for establishing and implementing core outcomes suggest that the findings may be relevant to other populations and disease and healthcare settings. Other healthcare providers, policy makers and service users will be involved in other phases of SONG-HD.17 31 32
In recent years, there have been calls to establish core outcomes in nephrology.33 34 Using the COMET and OMERACT methodology framework for establishing core outcomes (ie, systematic review, nominal group technique, stakeholder interviews Delphi surveys and consensus workshops),3 35 the SONG-HD Initiative has engaged over 1300 stakeholders (including patients/caregivers and health professionals) from more than 70 countries to establish core outcome domains for trials in haemodialysis: mortality, cardiovascular disease, fatigue and vascular access.16–19 36 These echo the outcomes nephrologists expected to be included in the core outcome set, though the SONG-HD process identified fatigue as a critically important specific patient-reported outcome because of its profound impact on patients’ well-being and functioning.16 17 Establishing feasible and valid core outcome measures are now in progress.28 Moreover, actions to facilitate implementation are underway. We are inviting endorsement by professional organisations, guideline groups and trial networks and convening implementation workshops involving a broader range of stakeholders including representatives from regulatory and policy agencies, industry, patient organisations, professional societies, research organisations, registries, trial networks and funding bodies.28
Ensuring a parsimonious set of simple, consistent and valid core outcome measures and creating a cultural shift such as through targeted funding to address the outcomes may facilitate the use of outcomes. Also, garnering buy-in and support from regulatory agencies, ‘gatekeepers’ and other key stakeholder organisations were recommended by nephrologists to enable and promote widespread implementation of core outcomes. Integrating these in the implementation strategy and action plan for core outcomes will improve the consistency of reporting critically important outcomes across trials. This may ultimately improve the contribution of trial-based evidence to advance patient-centred care and outcomes.
Acknowledgments
We thank all participants for sharing their interesting and thoughtful perspectives in this study. With permission, we acknowledge by name in alphabetical order: Aine Burns, Annemie Dhondt, Balaji Hiremagular, Biruh Workeneh, Bruno Watschinger, Chris Pugh, Chris Wenearls, Cormac Breen, Damien Ashby, Daniel Cejka, David Goldsmith, David Harris, Donal O’Donaghue, Edwina Brown, Evi Nagler, Francis Verbeke, George Mangos, Gregor Bond, Hamish Dobbie, Helen Alston, Jennifer MacRae, Jill Vanmassenhove, John Agar, Jose Perez, Katrien Blanckaert, Kevan Polkinghorne, Klemens Budde, Lina Choon Hui Lin, Manfred Hecking, Mark Brown, Matthew James, Matthew Jose, Matthew Roberts, Medha Airy, Neil Ashman, Nigel Toussaint, Norbert Lameire, Oliver Staeck, Paramit Chowdhury, Pascale Bernaert, Paul Lawton, Peter Kerr, Pietro Ravani, Prabir Roy-Chaudhury, Rainer Oberbauer, Rajeev Raghavan, Raymond Vanholder, Rob Quinn, Rosemary Masterson, Sai Kaumudi Saridey, Sajeda Youssouf, Sandip Mitra, Sreedhar Mandayam, Steve Holt, Suetonia Palmer, Sufi Suhail, Susanne Kron, Torsten Slowinski.
References
Footnotes
Contributors AT participated in the design of the study, conducted the interviews, analysed the data and drafted the manuscript. SC, JSG, TH, BRH, BM, RP-F, PT, WvB, AYMW, DCW, WCW, TG, AJ, EO’L, BS, AV and JCC participated in the design of the study, contributed to the analysis and provided critical intellectual input on the manuscript revisions. All authors approved the manuscript.
Funding This work was supported by a National Health and Medical Research Council (NHMRC) Project Grant (APP1098815). AT is supported by a NHMRC Career Development Fellowship (APP1106716). AV receives grant support from the NHMRC Medical Postgraduate Scholarship (APP1114539) and the Royal Australasian College of Physicians (Jacquot NHMRC Award for Excellence). EO’L receives grant support from the NHMRC Medical Postgraduate Scholarship (APP1114539).
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved by The University of Sydney Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.