Article Text

Abstract
Introduction Haemorrhagic stroke is of significant healthcare concern due to its association with high mortality and lasting impact on the survivors’ quality of life. Treatment decisions and clinical outcomes depend strongly on the size, spread and location of the haematoma. Non-contrast CT (NCCT) is the primary neuroimaging modality for haematoma assessment in haemorrhagic stroke diagnosis. Current procedures do not allow convenient NCCT-based haemorrhage volume calculation in clinical settings, while research-based approaches are yet to be tested for clinical utility; there is a demonstrated need for developing effective solutions. The project under review investigates the development of an automatic NCCT-based haematoma computation tool in support of accurate quantification of haematoma volumes.
Methods and analysis Several existing research methods for haematoma volume estimation are studied. Selected methods are tested using NCCT images of patients diagnosed with acute haemorrhagic stroke. For inter-rater and intrarater reliability evaluation, different raters will analyse haemorrhage volumes independently. The efficiency with respect to time of haematoma volume assessments will be examined to compare with the results from routine clinical evaluations and planimetry assessment that are known to be more accurate. The project will target the development of an enhanced solution by adapting existing methods and integrating machine learning algorithms. NCCT-based information of brain haemorrhage (eg, size, volume, location) and other relevant information (eg, age, sex, risk factor, comorbidities) will be used in relation to clinical outcomes with future project development. Validity and reliability of the solution will be examined for potential clinical utility.
Ethics and dissemination The project including procedures for deidentification of NCCT data has been ethically approved. The study involves secondary use of existing data and does not require new consent of participation. The team consists of clinical neuroimaging scientists, computing scientists and clinical professionals in neurology and neuroradiology and includes patient representatives. Research outputs will be disseminated following knowledge translation plans towards improving stroke patient care. Significant findings will be published in scientific journals. Anticipated deliverables include computer solutions for improved clinical assessment of haematoma using NCCT.
- computer aided diagnosis
- stroke
- computer algorithm
- hematoma volume
- non-contrast CT (NCCT)
- neuroimaging
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The paper introduced a study that taps into a well-defined clinical need to extract three-dimensional information from CT scans.
Outputs of the study can potentially assist with more effective clinical decision-making, potentially reducing risk of mortality and other adverse events.
Prospective algorithms from the project can be extended to improved management of other pathologies (eg, dementia, ventricle size in hydrocephalus and ischaemic stroke).
The study demonstrates an example of integration of multidisciplinary expertise for patient-centred clinical research.
This is not a systematic review and may have used information that is scoped to the protocol and study design. Nevertheless, the development of the protocol is rooted from a thorough literature search and review and thus is built on the current literature.
For now the project has been focused on acute haematoma stroke with clear clinical significance and not yet covered other conditions for more generalised stroke assessment. Building on the success of the project development, future research can extend the research outcomes to other conditions.
Introduction
Stroke overview
Stroke is the third leading cause of disability and the second leading cause of death worldwide.1 2 Globally, there are over 33 million people living with stroke with over 12 million of them left with permanent disabilities.3 Haemorrhagic stroke refers to a sudden loss of brain function due to lack of perfusion to the brain when an artery or other blood vessel in the brain ruptures leading to blood accumulation in the brain.4 5 Blood can either pool in the brain parenchyma (intracerebral haemorrhage) or spread into the subcortical areas and the ventricles (subarachnoid and intraventricular haemorrhages).5 6 About 15%–20% of all stroke types are haemorrhagic.5 In 2010, 62.8 million disability-adjusted life years (a measure of the disease burden that indicates how many years of healthy life are lost to sickness and disability) were lost due to haemorrhagic stroke worldwide in low/middle-income countries.7 An effective clinical decision-making tool in haemorrhagic stroke management is in pressing demand but presents a significant challenge in practice.
Over a third of deaths occur within 30 days with half of that number occurring in the first 48 hours in haemorrhagic stroke.6 8 This is explained by the fact that blood accumulation in the brain can lead to fast neurological deterioration due to an increasing cerebral oedema and intraparenchymal haemorrhage expansion of bleeding into ventricles and subarachnoid space in the acute phase.9 The volume of intracerebral haemorrhage is one of the strongest determinants of mortality in a 30-day period following the stroke event.10 Treatment decisions for haemorrhagic stroke (eg, procoagulant administration, drainage, surgery) are made, taking into account volume of the bleed.11–13 Therefore, the volume of the bleed needs to be accessed as quickly as possible on presentation of the patient to the hospital to improve patient outcomes.
CT imaging in acute haemorrhagic stroke
Once a patient presents to the hospital with symptoms of stroke, the first imaging needs to be done quickly and is typically the non-contrast CT (NCCT), as strongly recommended by the best practices for acute stroke. NCCT involves series of X-rays in thin two-dimensional (2D) axial slices of the brain tissue, without an injection of contrast media,11 14 and is fast, readily available and has good resolution for acute haemorrhages because of the high contrast it shows between blood and cerebrospinal fluid (CSF). In the acute phase, the bleed appears very bright, while the surrounding CSF remains dark.15 However, the initial emergency NCCT does not routinely include calculation of volume of bleeding. Effective methods of obtaining volume information from the NCCT once a haemorrhagic stroke has been confirmed are of significant clinical value.
Clinical haematoma evaluation
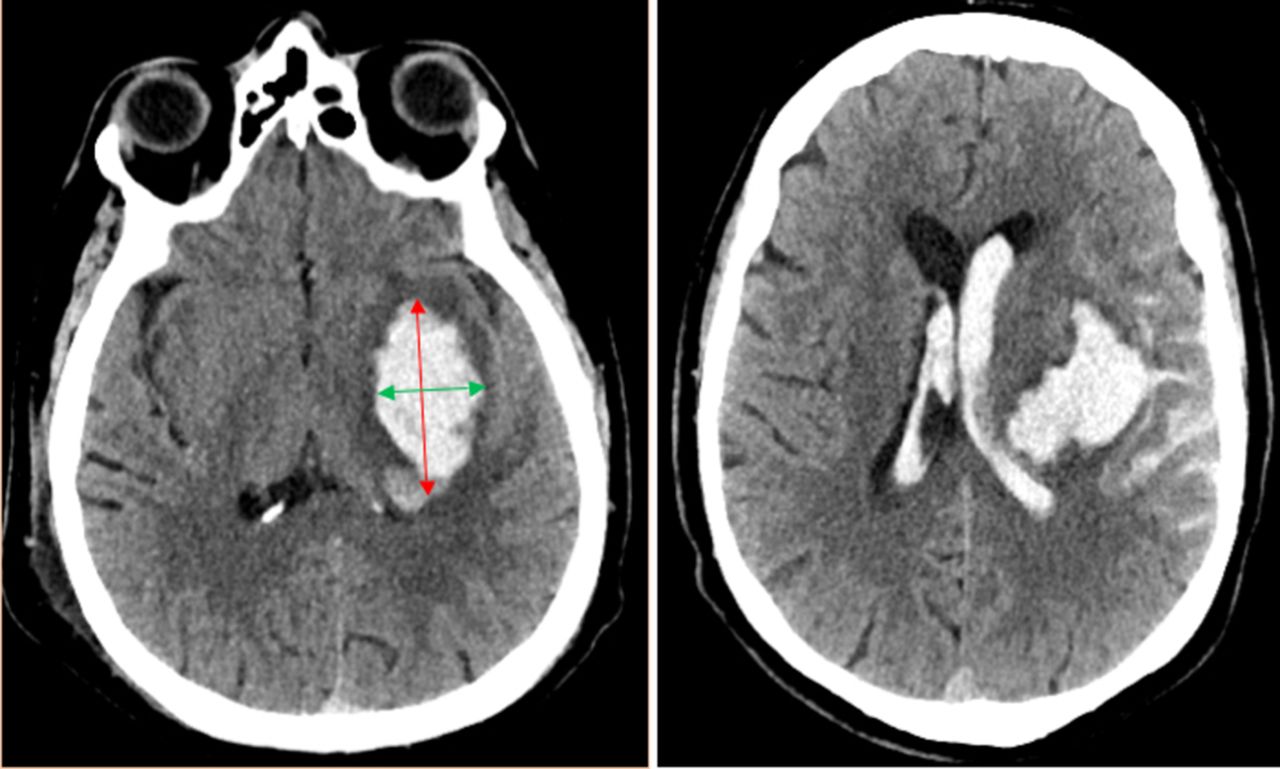
The so-called ABC/2 method is commonly used clinically to estimate haemorrhage volume, using bleed dimensions obtained from the NCCT. In the ABC/2 formula, measurement A is the largest haematoma diameter, B is the diameter 90° (or perpendicular) to A and C is the number of CT slices with bleed (eg,~30 to cover the brain) multiplied by standard CT thickness.9 16 These three numbers are multiplied and divided by 2 to get the average haematoma volume from the NCCT (figure 1). The ABC/2 method suffers from several major drawbacks, chiefly arising from the fact that the ABC/2 formula assumes an ellipse shape and thus would be appropriate only for elliptical-shaped haematomas.9 16 17 The accuracy of the method is poor for irregular lobar and ventricle-penetrating haematomas that are most common and life threatening.16 17 For estimating acute bleeds (<24 hours), the ABC/2 method has worse inter-rater reliability given the difficulty of defining infarct margins less than 3 hours on CT scan.18 Also, manual calculations are typically time consuming, expert knowledge demanding and prone to subjective variability errors. Therefore, solutions for automated haemorrhage volume estimation on NCCT scans are needed.

CT scans showing different shapes of haematoma. The regions of hyperintensities (bright) indicate the bleeding. Left panel shows it in an elliptical shape. The volume of the haematoma can be estimated using the ABC/2 method. The red arrow indicates the ‘A’ dimension, while the green arrow is the ‘B’ dimension. Right panel shows the haematoma in a non-elliptical (irregular) shape that has encroached into the lateral ventricles. The ABC/2 method cannot be applied to this case.
Computer-aided diagnosis
Computer-aided diagnosis (CAD) represents diagnosis made by the physician using computer output derived from quantitative analysis of diagnostic images as a guiding opinion.19 CAD improves diagnostic accuracy and consistency of radiologists’ image interpretation as well as reduction of intrarater and inter-rater variations.19 Potential gain in CAD often comes from synergistic combination of the radiologist’s competence and the computer’s capability.20
Our work in the preparation of the present project has identified a number of CAD programmes for computing haematoma volume in research. These include three-dimensional (3D) Slicer, Analyse, Osirix, Quantomo, MiStar and Leornado V.21–25 While none of these has been validated for clinical use, these methods also adopted a semiautomated solution and often rely on manually drawing regions of interests and haematoma islands based on which segmentation is performed and thus can be flawed by subjectivity errors and the requisite of additional expertise. A recent method by Scherer et al 26 has involved full automation, yet the algorithm has so far been validated only in intracerebral haemorrhage in research.26 The existing methods also have difficulties estimating intraventricular haemorrhage due to diminished distinction between blood and CSF and/or overestimating the haemorrhage volume (ie, by automatically classifying all the ambiguous pixels as haematoma) especially with irregular haemorrhages.21–25 In addition, when limited by lack of a 3D display option, such a method may not permit a thorough overview of the haematoma status. These signify a significant clinical need for novel effective software solutions that can estimate both regular and irregular shaped haematoma, handle different types of haemorrhages and support use in clinical settings with 3D presentation. Our project was designed to address this need. The present project aims to improve the accuracy of haematoma volume estimation and increase the speed in clinical decision-making, with an anticipation to integrate the automation solution in further research to help improve treatment decision.
Objectives
The objectives of the project are: (1) to develop a completely automated software tool for clinical use, with evaluation of haematoma volume regardless of shape; (2) to establish the reliability, validity and efficacy of the automation solution against results from using clinical expertise, planimetry and current CAD evaluations.
Methods and analysis
Study design and settings
The proposed project involves development of a fully automated software tool and secondary use of existing neuroimaging data in validating the tool under development. Currently available volume estimation automation software will be tested and compared with our proposed tool. New software solutions will be explored and novel machine learning algorithms developed. Reliability and validation will be established for potential clinical use. The study will take place at the Simon Fraser University (SFU) ImageTech Lab situated in Surrey Memorial Hospital of Fraser Health Authority (FHA) and at various affiliated study centres at SFU and FHA.
Participants and data source
The study will use existing CT imaging data. No new patients will be recruited specifically for the study. We will use non-probability sampling of whole brain CT scans of patients with acute stroke who were admitted to the neurological department at several FHA sites (eg, Royal Columbian Hospital, Surrey Memorial Hospital, Jim Pattison Outpatient Centre).
Inclusion
Patients (men or women) admitted to FH between 1 January 2011 and 31 December 2017 with acute haemorrhagic stroke as primary diagnosis.
Exclusion
Patients with multiple haematomas, haemorrhage as a result of tissue plasminogen activator administration for treatment of ischaemic stroke. We will retrieve a random sample of 200 patients from the pool of available CT scans using Fraser Health Picture Archiving and Communication System. Data manipulations are described in detail in the study procedures section.
Sample size
We estimate that a set of 200 full-head CT scans from patients with acute haemorrhagic stroke will be adequate sample size for the study based on power analysis (figure 2).27 28 This number will allow a sufficiently large sample to assess the concurrent validity and comparison between different automation approaches (eg, with high correlation ~0.7 and to detect a difference using two-tailed t-test with α=0.05 (type 1 error rate) and β=0.20 (type 2 error rate). In the literature review, similar comparisons have employed 30–290 independent data points (ie, scans from individual participants) to achieve a medium effect size (Cohen’s d=0.5) at 95% significance level. We have conducted a preliminary survey, which confirmed the feasibility of obtaining the required sample size based on an admission rate of >400 patients with the targeted condition per year at multiple sites in the FH region. It is feasible to achieve the proposed sample size.

Power analysis calculation graphically displayed justifying the choice of the chosen sample size for examining correlation (A) and group difference (B).
Determining the sample size of training set needed for machine learning algorithms can largely depend on the complexity of the targeted problem and the learning algorithm. For developing the new automated tool, we studied projects on voxel-wise brain imaging processing employing machine learning algorithms29 30 and decided that the proposed sample size in the training set would allow the identification of the features representing haematoma in contrast to normal brain tissue. In addition, our preliminary result using a pilot dataset of 30 CT scans has shown clear differentiation for haematoma using the software under development. However, more data are clearly needed to train the programme for more fine-tuned execution. Given that the study makes use of existing data, ensuring a sample size that is greater than the minimum required will allow the capture of the important features during the training phase, so that during the validation phase, new individual cases can be accurately evaluated.
Study procedures
To achieve objective 1 (ie, automation software development), existing methods that are used in segmentation of CT images will be studied to yield a solution building on top of algorithms.
To segment the haematoma volume, in the first step, the non-cerebrum tissues are removed. Then for each voxel, a set of predictors are calculated which have been shown to be useful to discriminate haemorrhage voxels from non-haemorrhage voxels. Apart from the raw intensity of the voxels, mean, SD, skew and kurtosis of the neighbouring voxels are included in the predictors set. Other features to be used are distance of voxels to the centre of the image and the intensity difference between contralateral voxels to take advantage of symmetry of non-haemorrhage voxels. Based on the training data, set of annotated images by radiologists, the thresholds for these predictors are calculated automatically using a random forest classifier. Segmenting CSF requires a similar method; however, in addition to the mentioned predictors, the result of another CSF segmentation method will be used as predictors. The initial segmentation is obtained through a 3D convolutional neural network which produces a probability for each voxel indicating how probable the voxel is haemorrhagic. Although the methods under investigation may have a relatively good performance in terms of segmentation accuracy, combining that with other mentioned features can yield a better result.
Segmentation, including differentiating between different types of haemorrhages, will be based on the Hounsfield Units of the CT images and not number of voxels. The method under development will classify each voxel as haemorrhagic or non-haemorrhagic brain tissues or CSF. To address errors from segmentation (eg, from region of skull-haemorrhage confusion as bone is very dense like blood), a method for extracting out the skull and leaving just the brain parenchyma will be employed.
To increase the capacity of the software, the solution will incorporate a function (with user-friendly interface) for expert input that may be activated when encountering areas where the infarct margin is ambiguous (figure 3). The segmentation thresholds will be determined using clinical CT data as well as experts on the research team (eg, clinical neuroradiologists).

An example showing haematoma with no clear bleed-parenchyma boundary; the volume of which cannot be correctly calculated using existing automation software and demonstrating the need for improved algorithms.
To achieve objective 2 (ie, test the reliability and validity of the new software solution), we will test the proposed software solution for reliability, accuracy and timeliness using sampling of CT scans (which are stripped of any identifying information and assigned a random study identification (ID) before use). Intrarater and inter-rater reliability will be examined using the novel software tool and comparisons will be made with other techniques such as ABC/2, Quantomo and planimetry to establish concurrent validity. As they have been considered to provide ‘gold standard’ outputs31 (even though it can be extremely time consuming and expertise demanding32), planimetric analyses will be employed in our study as the ‘comparator’ to test the construct validity of the intended software solution. Computer-assisted planimetric analyses, which calculate the area of haematoma on individual 2D slices will be performed to generate a total volume.31–35 Planimetric methods have been applied in validating Quantomo and ABC/2 in the past,23 32 36 justifying use in the current study to validate the novel solution (which is aimed to perform effective volumetric analysis, that is, a volumetric approach leading to significantly reduced processing time and expert input).
After development and validation of the software, the tool will be packaged into an easy-to-operate application with user-friendly interface in future implementation that can be installed in information systems in hospitals in the future to allow easy use clinically.
Timeline and milestones
Ethics and other approvals have been obtained mid-2017 and are up to date. Initial validation and data handling procedures is to be completed by the end of 2017. The prototype software will be developed, followed by the refinement and optimisation in 2018. Validation procedures developed in testing reference software will take place in 2019 towards the completion of the study goals.
Statistical analysis
Standard descriptive statistics will be conducted to understand the frequency and distribution of haematoma and its severity. Inter-rater and intra-rater reliability testing and analysis on volume measurements will be performed for absolute inter-rater agreement rate based on intraclass correlation coefficient (ICC) using two-way random effects model. The 95% Confidence Interval will be computed for ICC population values. Differences in the means of the calculation results among various methods will be examined and compared for accuracy. Efficiency of the various software tools will be examined by obtaining time data and comparisons made to see how quickly these methods can estimate volume.
Preliminary results and discussions
A set of random CT scans has been used in a preliminary test for reliability of Quantomo (figure 4) which is being used also as a comparator to test for concurrent validity of our tool. Nearly 80% of these CT scans were lobar strokes while 20% encroached into the subcortical regions. Two raters completed the haematoma volume estimation of the 10 patient scans, and the scores were used in computing the reliability testing. The calculations were made using the 2D option and CT images were analysed slice by slice.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A screenshot of the Quantomo software beaning used for comparison to validity testing. The top toolbar shows options for selection and estimation of haematoma; the left tool bar shows the measurement panel where the total volume is displayed. The most accurate way of estimating the volume is by going slice by slice in 2D, which can be time consuming, whereas the 3D estimate tends to miss classified normal tissues surrounding the haematoma.
High agreement rates were observed for the total score (table 1).
Intrarater and inter-rater agreement rates for Quantomo volume analyses using preliminary data
While the preliminary result has suggested high reliability of certain existing programme, the result should be interpreted with caution due to a small sample size. Also, most of the strokes were elliptical and lobar which is easier to estimate with even the ABC/2 method. These concerns will be addressed in the proposed study that will involve an estimated sample size of 200 cases.
Ethics and dissemination
A harmonized ethics approval has been obtained for this research from Fraser Health and Simon Fraser University Research Ethics Boards (FHREB2016-113). Additional approval was obtained for each of the software and patient data deidentification procedures. The deidentifying software, DicomCleaner, has been cleared for use by the participating Fraser Health Research Ethics Board Privacy, Confidentility and DAta Security Office. The CT images are given a randomly assigned study ID, while the original paperwork with patient information is only available to one principal investigator stored on a password protected file on secure FH network. In that way, there is no unauthorised access to personal details of the patients by members of the research team.
The protocol will not involve recruitment of any actual participants or alteration of the standard patient care in any aspect, and no informed consent from patients will be required. The research team has also included patient representatives to help ensure that the result presentations and other research documentations are meaningful and easily understood by lay persons.
Results from this research will be disseminated chiefly through acute stroke care and clinical neuroimaging conferences, and significant findings will be submitted for publication in peer-reviewed journals. The end result for potential clinical utility of the software will be disseminated first at FH sites.
Conclusion
Lack of accurate automated calculation of haematoma volume has limited the effective clinical use of NCCT-based information in guidance of care decisions and prediction of clinical outcomes in patients with acute haematoma. Development of such automated solution is important because increased precision of a clinical judgement is achieved through greater validity and reproducibility of intracerebral haemorrhage volume calculations. Preliminary investigations show that existing automation methods have good reliability for regular-shaped lobar bleeds. However, the existing research tools for volume automation make errors during segmentation of irregular, subcortical and ventricle-encroaching haemorrhages due to miss-setting the thresholds between haematoma and brain tissue for ambiguous regions. Research has shown that these kinds of haemorrhages are most fatal; 30-day mortality rate was 43% for patients with intraventricular haemorrhage compared with 9% in patients with only intraparenchymal blood.8 Hence, there is need for improved approach for these patients. The purpose of the proposed research project is to develop a fully automated measurement tool for the accurate clinical evaluation of brain haematoma volume in patients with acute haemorrhagic stroke, regardless of shape or location of the bleed. The intended solution will improve on current automation methods in accuracy while remaining superior over manual programmes regarding time and expert input requirements. The solution will be able to retrieve volume information from NCCT automatically and will allow for expert input for location-specific haematoma threshold settings where ambiguity may arise.
The clinical utility of a completely automated tool in managing intracerebral haemorrhage are numerous. Accurate and reliable haematoma volume automation speeds up the treatment decision-making (eg, surgery to evacuate bleed, procoagulant administration) which can translate into improved patient chances of survival and recovery. It is anticipated that the outcomes of the project will allow further investigation of the utility of the software tool in combination with relevant clinical and demographic data for the development of prognostication tools with application of machine learning techniques. Results of the project will also help to explore the potential of the proposed software tool in application to image analyses in other conditions such as ischaemic stroke, brain neoplasms and hydrocephalus to name a few.
Acknowledgments
The authors would sincerely acknowledge Dr J Kosior, Q Gao, B Strain, R Nagra and B Selema for critical discussions with the development of the research, implementation of the imaging analytical approaches, assistance with data access and processing and manuscript proofreading.
References
Footnotes
Contributors Conceptual construction of research and design: GM, WS, RCND’A, XS. Literature search and review: BC, AA, XS. First draft of the manuscript: BC, XS. Data access: GM, WS, XS. Image evaluation: BC, WS, TG. Research supervision: ME, SM, RCND’A, XS. Result interpretation and manuscript editing: All authors. All authors have approved the final version of the manuscript for submission for publication.
Funding This work has received funding support from Fraser Health Surrey Hospitals and Outpatient Centre Foundation and the Royal Columbian Hospital Foundation (FHREB 2016-113). Additional scholarship support was from Simon Fraser University Community Trust Endowment Fund and Fellowship Award from Beijing Hospital.
Competing interests None declared.
Patient consent Not required.
Ethics approval Research protocol has been approved by the Fraser Health and Simon Fraser University Research Ethic Boards. The study has involved a patient representative team member who provides input at various stages of the research development from the perspective of a patient.
Provenance and peer review Not commissioned; externally peer reviewed.