Article Text

Abstract
Introduction Stroke is one of the leading causes of disability worldwide. Recent data support the possibility that person-centred, self-management interventions can reduce dependence after stroke. However, there is limited information on the generalisability and optimum dose of these interventions.
Methods The Taking Charge After Stroke (TaCAS) study is a multicentre, investigator-blinded, randomised controlled trial recruiting 400 participants following acute stroke from seven hospitals in New Zealand. All patients discharged to community living who have ongoing symptoms at time of discharge (modified Rankin scale>0) will be eligible. Participants will be randomly assigned to one Take Charge session, two Take Charge sessions 6 weeks apart or control.
Outcomes The primary outcome will be the Physical Component Summary score of the Short-Form 36 at 12 months post stroke. Secondary outcomes will include dependence (modified Rankin scale), performance in activities of daily living (Barthel Index) and carer strain (Caregiver Strain Index), at 6 and 12 months post stroke. All analyses will be conducted on an intention-to-treat basis.
Ethics and dissemination The TaCAS study is funded by a Health Research Council of New Zealand grant. It has been approved by the Central Health and Disability Ethics Committee (15/CEN/115). Results will be published and presented at relevant stroke meetings within New Zealand and internationally, informing the use of a self-management intervention after stroke.
Trial registration Australia and New Zealand Clinical Trials Registry ACTRN12615001163594. Date registered 02-11-2015. Medical Research Institute of New Zealand Registry TCS01. Universal trial number U1111-1171-4127.
- Stroke
- Rehabilitation
- Self-management
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a trial of a low-cost, practical intervention in the community phase of stroke with the potential to make a significant difference to important outcomes for people with stroke.
Few exclusion criteria and multicentre design with relatively large number of participants will provide good basis for generalisability of the results.
Our methodology has stringent safeguards for data quality including a centralised randomisation system, blinded outcomes assessment and an electronic database that tracks all entries and locks data.
Outcome measurements are obtained by an assessor blinded to allocation; however participants and research clinicians are unable to be blinded, potentially leading to bias.
The 12–month follow-up limits the study to shorter-term outcomes.
Introduction
Stroke is a sudden, devastating clinical event that affects 15 million people worldwide each year, leaving 5 million people permanently disabled.1 Some current therapies may modify the acute phase of stroke but their use is inappropriate for a large proportion of patients and their effectiveness is limited.2 3 Despite early interventions, a high proportion of people have substantial impairment, activity limitation and participation restriction after routine stroke care. At least half of stroke survivors remain dependent on others one year after the stroke.4 Currently, there is little evidence supporting the effectiveness and efficacy of community-based therapies after stroke. Family support workers and goal-setting strategies are examples of two particular interventions that have been tested in randomised controlled trials but shown no benefit.5 6 Systematic reviews of therapy-led interventions have shown a positive effect on activities of daily living although with a small effect size.7
Self-management intervention studies in stroke and other conditions suggest that there is a positive effect on patient outcomes.8–10 Self-management programmes differ from education or skills training because they emphasise enablement of individuals to take an active role in managing their condition. This includes management of psychosocial problems and lifestyle changes needed to enhance quality of life.
A successful self-management programme is the 'Take Charge Session' (TCS) intervention, which is a low-cost, person-centred intervention undertaken after discharge from an acute or rehabilitation hospital into the community following acute stroke. This was tested against a DVD-delivered educational intervention and control in the Māori and Pacific Stroke study (MaPSS).11 In New Zealand, 9000 people suffer stroke every year. Although a relatively small proportion (15%) of those in New Zealand who have a stroke are of Māori or Pacific ethnicity, compared with other ethnic groups in New Zealand, Māori and Pacific stroke patients are more likely to have stroke at a younger age and have poorer outcomes after 12 months, even when adjusted for case-mix.4
In more detail MaPSS was a multicentre, randomised controlled trial in which participants were randomised to one of four arms: a TCS (delivered by an ethnic-appropriate, trained layperson), a professionally produced DVD of Māori and Pacific stroke survivor stories, both the TCS and the DVD, or a control group who received written stroke educational material. Outcomes were assessed after 12 months for 80% of the 172 participants. The TCS improved physical health-related quality of life, dependence and caregiver strain. Those who received the TCS session had a Physical Component Score of the Short-Form 36 (PCS) of 6.0 (95% CI 2.0 to 10.0, p=0.004) higher than those who did not. The TCS also reduced dependence on others (modified Rankin scale (mRS) >2) for activities of daily living, OR 0.42 (95% CI 0.2 to 0.89), p=0.023. The number needed to treat to prevent one person becoming dependent was 10.
We hypothesise that the TCS could improve physical outcomes in New Zealand stroke survivors of all ethnicities, and that two exposures to TCS may be more effective than one. This target population for the intervention includes all stroke survivors discharged to community living after inpatient hospital care. This represents about 60% of all patients with acute stroke in New Zealand, which is >5000 people per year. To test this hypothesis, the present study (TaCAS) will determine whether the TCS session improves outcomes in New Zealand stroke survivors who are non-Māori and non-Pacific, and whether two TCS episodes are more effective than one. This paper outlines the study protocol for the TaCAS study and follows the SPIRIT guidelines see online supplementary table.12
Methods
TaCAS is proposed to be a prospective, single-country, multicentre, parallel-group, blinded outcome assessed, randomised controlled trial of 400 patients with a new diagnosis of acute stroke. Patients will be screened for eligibility by local researchers in seven New Zealand hospitals using the inclusion and exclusion criteria listed in box 1. The screening researcher will be either the stroke nurse or doctors of the stroke team, or the principal investigator depending on the centre. In hospital, this researcher will explain the study and provide a participant information sheet to eligible patients and determine their stroke severity using Barthel Index (BI) at days 3–5 after stroke. In the presence of conditions such as aphasia or cognitive impairment, the patient’s ability to understand the study—and therefore to consent—will be determined by the screening researcher. The hospitals are geographically dispersed and range from semirural (secondary) to regional (quaternary) units. The trial study sites are listed in table 1. Māori and Pacific stroke patients have been excluded from TaCAS as it would be unethical to randomise these patients to a control arm when MaPSS demonstrated that they benefit from the intervention.
Inclusion and exclusion criteria
Inclusion criteria
Non-Māori, non-Pacific adults>16 years of age with acute ischaemic stroke or intracerebral haemorrhage (WHO definition)
Discharged from hospital to non-institutional, community living situation
Modified Rankin score >0
Exclusion criteria
Inability to provide informed consent
Unlikely to survive beyond 12 months
Trial sites
Patients will receive diagnostic procedures, treatment and rehabilitation as per local practice, not influenced in any way by the study. Patients who express interest in participating will be followed until their date of discharge. Those discharged into community living (not rest home or hospital-level care) will be telephoned within two weeks to arrange a baseline home visit with a research clinician. This research clinician may be a nurse, physiotherapist or occupational therapist, who is trained in the delivery of the TCS. The research clinician must complete this visit within a 16-week window from date of stroke, which allows for time spent in inpatient rehabilitation.
Randomisation
At the baseline home visit, the research clinician will explain the study to the participant. Informed consent will be obtained based on the International Conference on Harmonisation Good Clinical Practices guidelines prior to randomisation. No one will consent on behalf of participants in TaCAS, that is, proxy consent is not permitted. Once consented, the research clinician randomises the participant to one of the two interventions or to control by opening a sealed, opaque envelope containing allocation. An independent statistician (MW) is responsible for the computer-generated allocation sequence used to create the envelopes, which are consecutively numbered and delivered to each site in blocks of 18.
Prior to randomisation, all participants undergo a baseline assessment, which includes patient demographics, poststroke dependence measured by the mRS,13 activities of daily living by the BI,14 extended activities of daily living by the Frenchay Activities Index (FAI),15 health-related quality of life by the Short-Form 12 (SF-12v2)16 and EuroQOL EQ-5D (EQ-5D),17 depression by the Patient Health Questionnaire-2 (PHQ-2),18 activation by the Patient Activation Measure (PAM),19 as well as stroke-related risk factors and medications. Current support, outpatient rehabilitation service involvement and work situation will all be recorded.
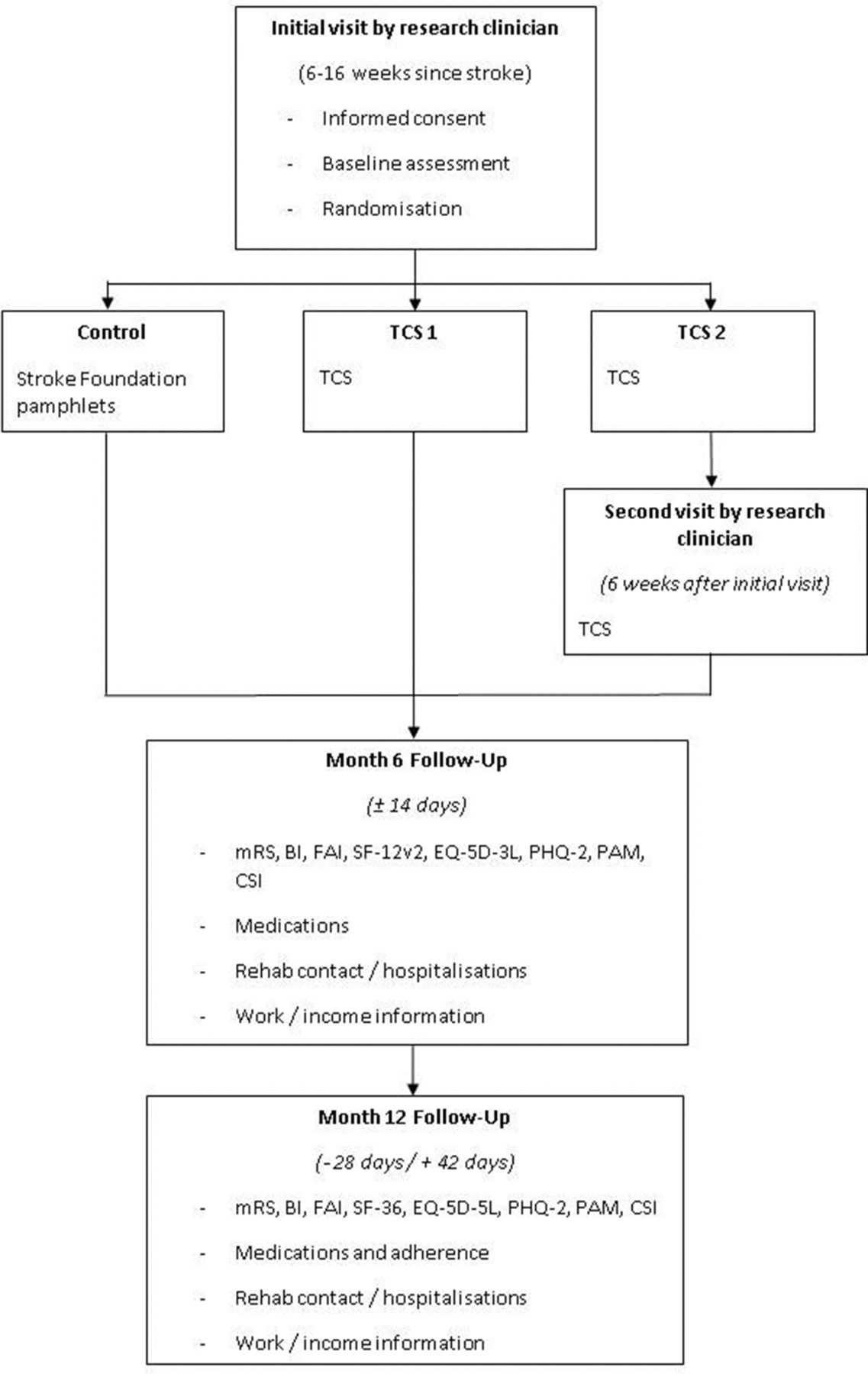
After the baseline assessment, but at the same visit, participants receive their allocated intervention: either a TCS or control. The study flow chart is presented in figure 1.

{kind=link}
TaCAS study flow chart depicting interventions and outcome measurements. BI, Barthel Index; CSI, Caregiver Strain Index; EQ-5D-5L, EuroQol 5-Dimensional, 5 Levels; FAI, Frenchay Activities Index; mRS, modified Rankin scale; PAM, Patient Activation Measure; PHQ-2, Patient Health Questionnaire 2; SF-12v2, Short Form 12 version 2; SF-36, Short Form 36; TCS, Take Charge Session.
Intervention arms
Prior to their involvement in TaCAS, all research clinicians undergo training focused on the rationale and delivery of the TCS. Research clinicians are trained to encourage participants to ask and answer their own questions, and to form their own ideas. Time spent listening to participants is emphasised, in particular allowing them to consider and express their hopes, fears and priorities. By gently reflecting the participant’s own thoughts, the TCS attempts to avoid shaping the patient’s goals, a process that can occur in therapist-led goal-setting.20 Research clinicians are discouraged from suggesting goals so that the focus remains on what the participant wants, rather than what is perceived to be doable. Using a structured workbook allows participants to write down any forthcoming goals and intermediate steps, and to see this as an ongoing process that they can review in their own time; in essence, ‘Taking Charge’ of their own recovery. The intervention takes between 60 and 80 min to complete. The headings within the workbook include Who I Really Am, Hopes and Aspirations, Main Fears, My Best Day, Physical Needs, Communication, Emotional Issues, Information Needs, Financial Issues, My Support Network and Stroke Prevention. The two intervention arms are distinguished in box 2.
Interventions
1 TCS
A person-centred, self-directed session designed to engage the participant in the process of recovery, guided by a workbook. The research clinician is trained to facilitate the process by listening and supporting any forthcoming ideas.
2 TCS second arm
The initial TCS will be undertaken, followed by a second TCS approximately six weeks after. The second ‘dose’ of the session allows time for the participant to express new, interim ideas that may have formed, and to reflect upon their progress.
Control arm
After the baseline assessment, these participants will receive educational pamphlets produced by the Stroke Foundation of New Zealand. All aspects of routine stroke care, in particular contact with rehabilitation services, will be unchanged by participation.
Outcomes
The primary outcome is physical functioning as determined by the PCS of SF-36 at 12 months after stroke.21 Participants will be followed 6 months after stroke with a questionnaire which will be delivered by telephone, post or by the internet. A blinded outcomes assessor, who will attempt to confirm incomplete responses by a telephone call, will gather all the questionnaire information. At 12 months after stroke, the blinded outcomes assessor will visit participants in person to complete follow-up. Box 3 describes the primary and secondary outcomes as well as the predefined subgroup analyses.
Primary and secondary outcomes and proposed subgroup analyses for the Taking Charge After Stroke study
Primary outcome
Physical Component Summary score of Short-Form 36 at 12 months after stroke
Secondary outcomes
At 6 months after stroke
Telephone-based, written postal or internet-administered questionnaire assessment of
Physical Component Summary score of the Short-Form 12 version 2 (PCS of SF-12v2)
Activities of daily living: Barthel Index (BI)
Instrumental activities of daily living: Frenchay Activities Index (FAI)
Level of function: modified Rankin scale (mRS)
Depression: Patient Health Questionnaire-2 (PHQ-2)
Level of activation: Patient Activation Measure (PAM)
Health-Related Quality of Life: WHO Quality of Life Assessment and euroQol Five-Dimensional scores (EuroQOL EQ-5D)
Carer strain: Caregiver Strain Index (CSI)
Contact with rehabilitation service
Hospitalisations
At 12 months after stroke
Face-to-face assessment of
BI, FAI, mRS, PHQ-2, PAM, EuroQOL EQ-5D, CSI, rehabilitation contact or hospitalisations
Predefined subgroups
Stroke severity: patients with BI at 3–5 days after stroke grouped severe (0–7), moderate (8–13) and mild (14–20)
Sites (all centres and tertiary centre vs not)
Age (<75 years vs 75+ years)
Patients taking fluoxetine at baseline
Patients with significant communication disorder (vs none/mild)
Patients with significant cognitive disorder (vs none/mild)
Self-reported purpose/autonomy/mastery/connectedness level
Patients with different levels of patient activation based on PAM
The SF-36 is a psychometrically robust self-reported measure of health status that is validated in multiple conditions, including stroke. The PCS assigns weights to responses about physical ability, the impact of physical health, pain and general health perceptions to give a composite score. The PCS score has an observed mean of between 38 and 39, 12 months after stroke in Australasian stroke studies.22 It was responsive to the TCS in the MaPSS study, in which the difference between mean-adjusted 12-month PCS scores exceeded the Minimal Clinically Important Difference of 5 points.
Table 2 summarises timing of the assessments. Research clinicians will write data from their visits onto paper forms, which are then scanned and sent to the data management team for entry onto a secure, online database. Each participant is identified by a unique identifier with only the central site at the Medical Research Institute of New Zealand (MRINZ) holding the master log of names.
Timing of assessments
Attempts will be made to obtain mRS and SF-36 data at 12 months by telephone from participants who discontinue or deviate from the intervention protocol. If this is not possible, data about living situation and level of disability (mRS) will be obtained from the participant’s general practitioner.
Risks to internal validity
The main risks to internal validity are threats to the fidelity of the intervention and unblinding. Site initiation and subsequent site training visits by the Coordinating Investigator, as well as 6-monthly teleconferences between research clinicians and the study team, will allow monitoring of the fidelity of the TCS. Research clinicians are encouraged to document specific problems encountered during the TCS although the participant keeps the TCS workbook as part of the intervention. Due to the personal nature of its contents, the workbook will not be collected or analysed. A central email account is checked daily for questions from research clinicians, and the principal investigator will answer urgent questions immediately by telephone. These queries form a Frequently Asked Questions section in a monthly newsletter to all the sites.
Blinding is maintained by employing a single-blinded outcomes assessor who will visit participants at each site. The blinded outcomes assessor will have an office that is physically separate from the office of the local research clinicians, and the specific online database user profile allows access only to demographic and outcomes data. Participants are asked not to disclose details of home visits to the blinded outcomes assessor, and intervention participants are asked to hide the TCS workbook when the blinded outcomes assessor visits.
Sample size calculation and statistical analysis
In MaPSS, the root mean square error for the PCS was 10.8. The clinically significant difference for PCS is five. A total sample size of 360, 120 in each of three arms, has 90% power to detect this difference. With provision for 10% drop out, we plan to recruit 400 participants. Experience in MaPSS has allowed prediction that TaCAS will complete recruitment in mid-2017.
All outcomes will be analysed using the intention-to-treat principle. Our primary analysis of the difference in mean PCS (between both Take Charge groups and control, and between high-dose Take Charge and low-dose Take charge) will be by analysis of variance. We will use analysis of covariance (ANCOVA) to analyse the Take Charge dose response as a continuous predictor. A further analysis will adjust for baseline variables including baseline PCS, age and gender. We will use also ANCOVA for our prespecified subgroup analyses using an interaction term between randomised treatment and each of stroke severity, site, age, gender, living situation, type of stroke, thrombolysis and fluoxetine use. The mRS will be analysed as dichotomous (0–2 compared with 3–5) and by ordinal logistic regression.
We plan to undertake a meta-analysis of individual patient data from TaCAS and the MaPSS study to compare the TCS against control, using PCS at 12 months after stroke in a linear mixed model meta-analysis. We will also assess combined dependency based on mRS in a generalised linear mixed model.
Finally, we will undertake a cost-utility analysis of the TCS using employment and earning information, cost to the carer and health-related quality of life.
Data collection and study management
The baseline data will be collected on paper forms by research clinicians at the initial home visits. These forms are scanned and sent to the data management team based at MRINZ for entry into a secure, online database. This database is designed to maintain complete blinding of the outcomes assessor. The data management team at MRINZ performs double data entry of the baseline visit data. Participants undertaking the 6-month questionnaire online will enter their data directly onto this database. The blinded outcomes assessor will enter the 6-month data obtained by telephone or posted questionnaire. The blinded outcomes assessor will also enter the 12-month data onto the database by an electronic tablet at the final home visit. This web-based data management system allows allocation concealment, locking of completed entries and ad hoc consistency checks by study monitors.
The TCS has no known harms associated. We plan to report the following serious adverse events (SAEs): death, life-threatening event, permanently disabling or incapacitating event, hospitalisation and any significant medical event considered serious by the study investigator. All SAEs will be reported to the New Zealand Central Health and Disability Ethics Committee of New Zealand (HDEC) in accordance with current guidelines, as well as to the MRINZ within 24 hours of the study investigators becoming aware of the event. AE data are collected at each follow-up and during the study period if the participant or their next-of-kin notify the research team. No interim analysis, for either effectiveness or harm, is planned prior to completion of the study. There are no current data available for data sharing.
There are no specific plans for independent auditing of this study; however, MRINZ research staff and online database will ensure there is a complete audit trail for external auditing, in the event this is required.
Ethics and dissemination
TaCAS will be conducted in compliance with relevant New Zealand legislation including the Health Information Privacy Code, the Health and Disability Code and the New Zealand Bill of Rights Act. Ethics approval has been provided by the HDEC, reference 15/CEN/115 and at the research office at each local site. Protocol amendments will first be approved by the HDEC and then by local ethics committees before implementation. The current approved protocol version is version 9.1, dated 20 February 2017.
Research clinicians will obtain informed consent from the participant when understanding of the study’s undertakings has been demonstrated. The participant ‘making a mark’ on the consent form will be accepted. Proxy consent by a surrogate will not be accepted.
To maintain confidentiality, participant information will be kept in the locked, central data office at MRINZ as well as at each local site in locked offices. The online database is password-protected and located on an encrypted server belonging to REDCap. Source data from TaCAS will be kept in secure premises for 15 years after completion of the study, then it will be destroyed.
The day-to-day management of the trial is undertaken by a management committee comprised of the principal investigator, Dr Harry McNaughton, the study coordinator, Dr Vivian Fu, project manager, Tanya Baker, and a team of researchers based at MRINZ. These individuals, as well as our statistician, Dr Mark Weatherall, will have access to the final trial dataset. The TaCAS Study Group meets on an ‘as-required’ basis with regular updates via newsletters and email. The majority of members meet regularly for national stroke and rehabilitation working groups, study days and conferences where progress and issues with the trial are discussed. Neither the principal investigator nor site investigators have competing interests.
All members of the TaCAS Study Group will contribute to, and be acknowledged in, the primary trial manuscript. The HRC funding will be acknowledged in all publications. Results will also be presented at national and international stroke meetings, including the National Stroke Rehabilitation Working Group and National Stroke Clinical Working Group meetings. Those participants who have indicated their desire to receive results of the study will have these sent to them.
Trial status
The first patient was randomised on 24 October 2015 and recruitment is expected to complete by June 2017. Study recruitment is continuing as planned.
References
Footnotes
Contributors HM conceived the study. HM, VF and MW contributed to the study design. VF collected the data. HM, VF and MW will be responsible for data analysis and interpretation. VF drafted this protocol, and HM and MW contributed equally to its critical review. VF, MW and HM have given final approval of this version to be published.
Funding This work was supported by the Health Research Council (HRC) of New Zealand (grant 15/297). The HRC had no role in the preparation or decision to publish of this protocol.
Competing interests None declared.
Ethics approval New Zealand Health and Disability Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.