Article Text

Abstract
Objectives This research aims to explore the association between serum osmolarity and mortality in patients who are critically ill with specific categories of disease.
Design A retrospective cohort study.
Setting and participants Data were extracted from an online database named ‘Multiparameter Intelligent Monitoring in Intensive Care II’. 16 598 patients were included.
Methods Patients were divided into six disease subgroups based on the diagnosis at admission: cardiac, cerebral, vascular, gastrointestinal, respiratory and non-respiratory. The association between maximum osmolarity (osmolaritymax) and hospital mortality in each subgroup was evaluated using osmolaritymax as a design variable (six levels).
Results Analysis of the 16 598 patients revealed a ‘U’-shaped relationship between osmolarity and mortality with a threshold of 300 mmoL/L. For patients with non-respiratory disease, both hypo-osmolarity and hyperosmolaritymax were associated with increased mortality, with the OR increasing from osmolaritymax level 3 (OR: 1.98, 95% CI 1.69 to 2.33, p<0.001) to level 6 (OR: 4.45, 95% CI 3.58 to 5.53, p<0.001), using level 2 (290–309 mmoL/L) as the reference group. For patients with respiratory disease, however, neither hypo-osmolarity nor hyperosmolaritymax was significantly associated with mortality (levels 1 to 5) except for extreme hyperosmolaritymax (≥340 mmoL/L, OR: 2.03, 95% CI 1.20 to 3.42, p=0.007). ORs of mortality in the other four subgroups (cardiac, cerebral, vascular, gastrointestinal) were similar, with OR progressively increasing from level 3 to 6. In all six subgroups, vasopressin use was consistently associated with increased mortality.
Conclusions Hyperosmolarity is associated with increased mortality in patients who are critically ill with cardiac, cerebral, vascular and gastrointestinal admission diagnoses, with thresholds at 300 mmoL/L. For patients with respiratory disease, however, no significant association was detected.
- serum osmolarity
- mortality
- respiratory disease
- vasopressin
- ICU
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The large sample size facilitated a robust modelling approach.
Subgroup analysis based on different admission diagnoses was performed to alleviate the heterogeneity of mixed intensive care unit.
The serum osmolarity was calculated in the current study which leads to certain bias despite an optimal equation was used.
Causal relationship could not been inferred due to the nature of retrospective study.
Introduction
Serum osmolarity plays an important role in extracellular and intracellular water distribution and mainly depends on the concentrations of Na+, K+, Cl–, glucose and urea. Perturbation of osmolarity is strongly associated with various body fluid imbalances,1 2 such as dehydration and hypernatraemia, leading to clinically adverse consequences such as increased risk of cardiovascular, respiratory and renal disorders3 4 and mortality.5 6
The predictive value of serum osmolarity has been studied in several specific patient populations, such as those with stroke, intracranial haemorrhage and acute coronary syndrome.7–9 Despite the consistency of results showing that hyperosmolarity is associated with increased mortality, this conclusion is still not applicable to patients in intensive care units (ICUs), mostly due to the heterogeneity of disease severity and classification. For instance, Rohla et al 8 reported a significant correlation between mortality and hyperosmolarity in patients with acute coronary syndrome. However, this correlation became insignificant after excluding the patients who are critically ill, which further reflects the heterogeneity of disease severity. Moreover, the impact of osmolarity on different diseases is also inconsistent, especially for patients with respiratory diseases. Experimental data suggested that hyperosmolarity may improve recovery from lung injury by inhibiting the production of cytokines,10 11 and a clinical investigation12 also confirmed that hypernatraemia was not associated with the mortality of patients with respiratory disease; however, osmolarity has not been studied in this group.
Despite all of these efforts, the prognostic and therapeutic value of serum osmolarity for specifically critically ill populations still has not been well established. Holtfreter et al 13 reported that serum osmolarity has moderate predictive value for mortality in unselected patients in ICU (area under the curve (AUC)=0.732), but two critical limitations should be noted. First, an ‘S’-shaped relationship was revealed between osmolarity and mortality based on the assumption that the mortality rate is near zero for patients with very low serum osmolarity, which is not consistent with clinical observations. Second, no subgroup analysis was performed, probably owing to the relatively small sample size, which made it difficult to apply this conclusion into practice.
Thus, it is of vital importance to re-evaluate the association between osmolarity and mortality in patients in ICU. In the present study, patients were stratified based on their ICU admission diagnoses, and subgroup analysis was performed. In particular, the respiratory and non-respiratory disease subgroups were compared.
Materials and methods
Database introduction
The Multiparameter Intelligent Monitoring in Intensive Care II (MIMIC II, V.2.6) database is maintained by the Laboratory for Computational Physiology at the Massachusetts Institute of Technology. It contains information from more than 30 000 patients in ICU at Beth Israel Deaconess Medical Center from 2001 to 2008.14 15 The database is accessible to researches who have completed a ‘protecting human subjects’ training. The institutional review boards of the Massachusetts Institute of Technology (Cambridge, MA) and Beth Israel Deaconess Medical Center (Boston, MA) approved the establishment of the database. Thus, the consent was obtained for the original data collection, but not specifically for this study. Data presented in this study were extracted by author Shen, who completed the online training course of the National Institutes of Health (certification number: 1564657). Data extraction was performed using PostgreSQL tools V.1.12.3.
Study population and stratification method
Patients who were pregnant or younger than 18 years old were excluded from this analysis. The following information was extracted: age, gender, weight, race, comorbidity, type of patients admitted to ICU, hospital length of stay (LOS), hospital mortality, sequential organ failure assessment score, vasopressin use, urine output and serum levels of Na+, K+, glucose, urea, creatinine and albumin.
Serum osmolarity was calculated using the equation (2 × Na+ + K+) + (glucose/18) + (urea/2.8).16 Only values of plasma sodium, potassium, glucose and urea measured at the same time were used in the calculations. Patients without sufficient data to calculate serum osmolarity were excluded. Plasma protein levels were omitted as they only contribute ~0.4% to serum osmolarity.17 Maximum osmolarity (osmolaritymax) was calculated using the maximum values of serum Na+, K+, glucose and urea measured at the same time during the ICU stay. Although 285–300 mmoL/L is typically considered the normal range of serum osmolarity, the MIMIC II database defines the normal osmolarity range as 290–309 mmoL/L. Thus, 290–309 mmoL/L was used as the normal range and reference group in the present study. Crude outcomes were compared among three groups: hypo-osmolarity (<289 mmoL/L), normal osmolarity (290–309 mmoL/L) and hyperosmolarity (≥310 mmoL/L). To further examine the effect of hyperosmolarity, osmolaritymax was further categorised into six levels for analysis with logistic regression models: level 1 (<289 mmoL/L), level 2 (290–309 mmoL/L), level 3 (310–319 mmoL/L), level 4 (320–329 mmoL/L), level 5 (330–339 mmoL/L) and level 6 (≥340 mmoL/L). The data were also analysed in terms of subgroups based on diagnosis at admission: cardiac, cerebral, vascular, gastrointestinal, respiratory and non-respiratory disease.
Definitions and outcomes
The primary endpoint was hospital mortality, defined as death during hospitalisation. Secondary endpoints included ICU mortality, hospital LOS, ICU LOS, development of acute kidney injury and maximum sequential organ failure assessment score during ICU stay. For patients with more than one ICU stay, only the first ICU stay was considered. An increase in serum creatinine level of more than 1.5 times above baseline was considered to reflect acute kidney injury according to the Kidney Disease Improving Global Outcome criteria.18 Vasopressin use was defined as any vasopressin use during ICU stay for any reason.
Statistical analysis
Continuous variables are presented in the tables as the mean with SD or median with interquartile ranges. The Student’s t-test, Wilcoxon rank-sum test or Kruskal–Wallis test was used as appropriate. Categorical variables are presented as a percentage and compared using the X2 test. The Lowess Smoothing technique was used to explore the crude relationship between osmolarity and mortality. A logistic regression model was built for each of the six subgroups using osmolarity as a design variable, with the normal range (290–309 mmoL/L) as the reference group. A stepwise backward elimination method with a significance level of 0.05 was used to build the final models. Potential multicollinearity was tested using a variance inflation factor, with a value of ≥5 indicating multicollinearity. Goodness of fit was assessed for all logistic regression models. Receiver operating characteristic curves were depicted to show the diagnostic performance. All statistical analyses were performed using the software Stata V.11.2 . All tests were two sided, and a significance level of 5% was used.
Results
Population and baseline characteristics
The MIMIC II database contains records for 32 425 admissions, of which 6973 were excluded because they were duplications. Of the remaining 25 452 admissions, 7932 were excluded because the patients were younger than 18 years old (7888) or pregnant (44), and 754 were excluded because of insufficient data. After excluding outliers (168 admissions), 16 598 admissions were included in this analysis, including 2055 non-survivors and 14 543 survivors, establishing an initial mortality rate of 12.4%. The mean age was 65.2±22.6 years, and 9491 patients were male (57.0%).
Demographic characteristics of the survivors and non-survivors are presented in table 1. Osmolarity0 and osmolaritymax were significantly lower for survivors (301.9±11.3 and 309.1±12.6, respectively) than non-survivors (305.8±14.8 and 321.5±16.8) (p<0.001). Vasopressin was used less often by survivors than non-survivors (2.50% vs 19.6%, p<0.001). The number of patients of each disease subgroup was as follows: cardiac group (5652, 34%), cerebral group (2531, 15.2%), vascular group (2092, 12.6%), gastrointestinal group (2020, 12.1%), respiratory group (1750, 10.5%) and non-respiratory group (14 848, 89.5%).
Comparisons of demographics between survivors and non–survivors
Figure 1 shows the relationship between osmolarity0/osmolaritymax and hospital mortality for patients in ICU with or without respiratory admission diagnosis determined using the Lowess Smoothing technique. Four models yielded non-linear relationships, with the lowest mortality rate at osmolarity of ~300 mmoL/L. Thus, the group with osmolarity of 290–309 mmoL/L was used as the reference in all comparisons and logistic regression models. A ‘U’-shaped relationship between osmolarity0 or osmolaritymax and mortality was found for patients admitted with non-respiratory disease (figure 1 A and B); for patients with respiratory disease, however, this relationship became less clear, especially for osmolarity0 (figure 1C and D).
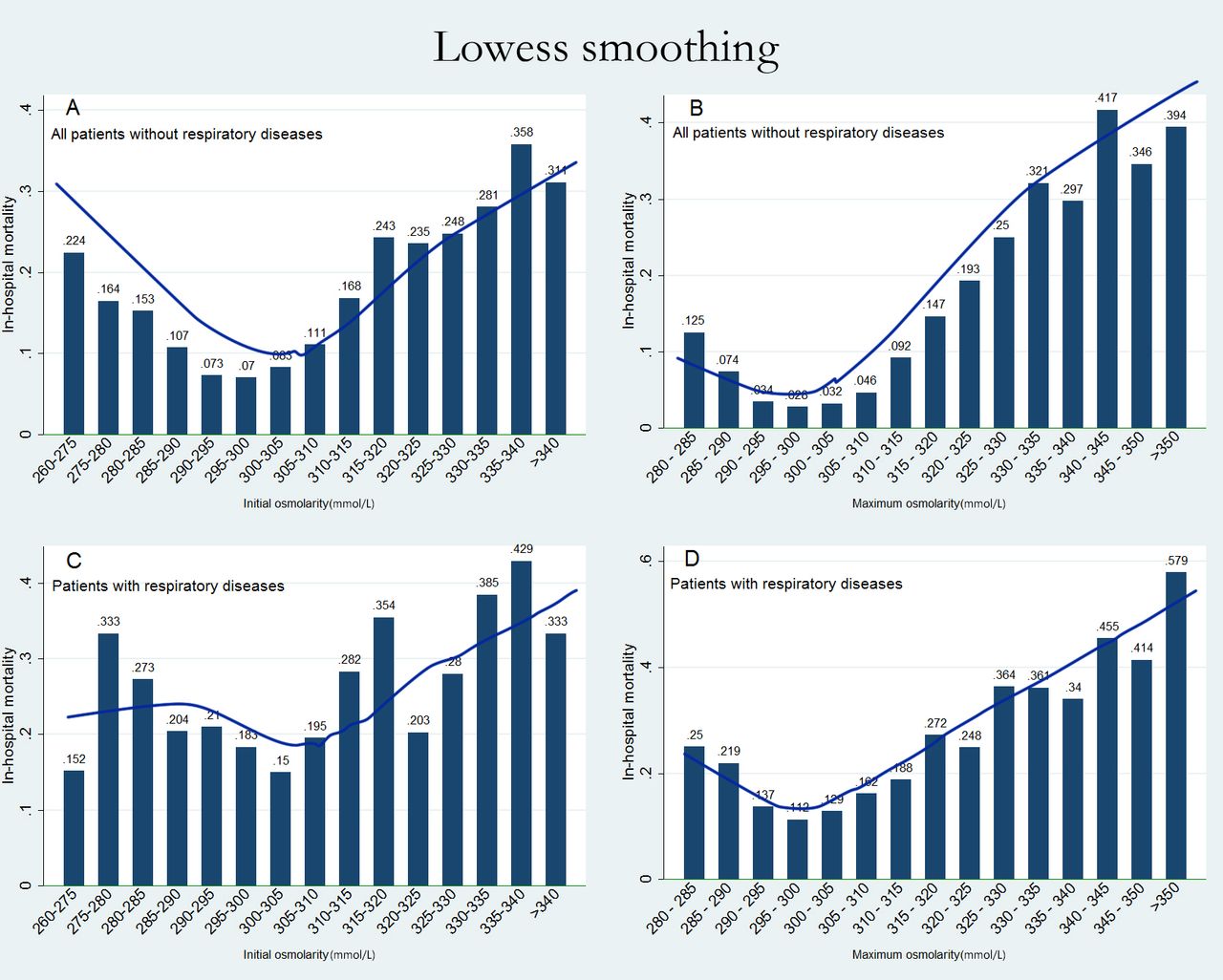
Association between osmolarity0 (left)/osmolaritymax (right) and mortality of patients with (C, D) or without (A, B) a respiratory admission diagnosis. Non-linear relationships are presented in this figure. The ‘U’-shaped curve revealed that the threshold of osmolarity was ~300 mmoL/L.
Crude outcomes are given in table 2 for the three osmolaritymax categories. Without adjusting for covariates, the outcomes were similar for patients with or without respiratory disease. Hyperosmolaritymax was associated with increased hospital and ICU mortality compared with normal osmolarity levels for patients with or without respiratory disease (p<0.001, all). In addition, hyperosmolaritymax was also associated with higher acute kidney injury rates in these two subgroups (p<0.001, both).
Unadjusted outcomes by maximum serum osmolarity categories in patients with or without respiratory admission diagnosis
To further explore the effect of hyperosmolarity, osmolaritymax was categorised into six groups (as described above), which were used as design variables in six regression models, with level 2 (290–309 mmoL/L) serving as the reference group. Table 3 shows that after adjusting for covariates, both hyposmolaritymax and hyperosmolaritymax were associated with increased hospital mortality in patients without respiratory admission disease, with the OR increasing stepwise from level 3 (OR: 1.98, 95% CI 1.69 to 2.33, p<0.001) to level 6 (OR: 4.45, 95% CI 3.58 to 5.53, p<0.001). For patients with respiratory admission disease, however, this trend no longer existed. Neither hyposmolaritymax nor hyperosmolaritymax was significantly associated with higher mortality (levels 1 to 5), but extreme hyperosmolaritymax (≥340 mmoL/L) was related to increased mortality (OR: 2.03, 95% CI 1.20 to 3.42, p=0.007). In both models, vasopressin use was positively associated with mortality (OR: 1.89, 2.05, p<0.001, p=0.011, respectively). Also, another four logistic regression models were built for analysis of the cardiac, cerebral, vascular and gastrointestinal disease subgroups. Figure 2 shows the OR and 95% CI for the other four subgroups. A similar trend was observed that OR progressively increased from levels 3 to 6, with the maximum OR observed in the vascular group. Vasopressin use was associated with increased mortality (see online supplementary table 1, which illustrates the logistic models of the other four subgroups).
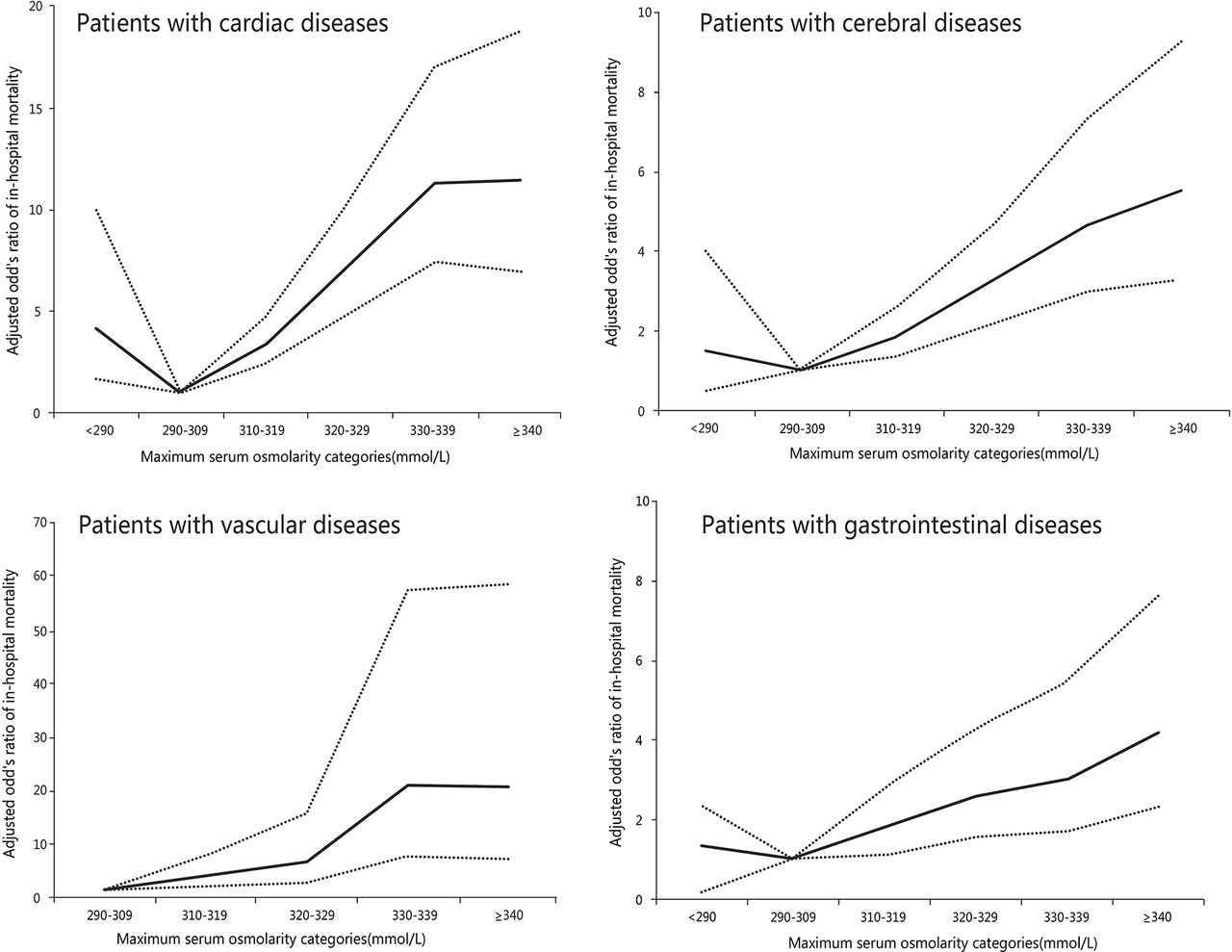
Adjusted OR of hospital mortality relative to 290–309 mmoL/L for different categories of osmolaritymax during ICU stay in the cardiac, cerebral, vascular and gastrointestinal subgroups. ICU, intensive care unit.
Adjusted ORs using osmolaritymax as the design variable in patients with or without respiratory admission diagnosis
The diagnostic value of osmolaritymax was examined for all six subgroups using receiver operating characteristic curves (figure 3). The results showed that the diagnostic performance was moderately good for the cardiac (AUC=0.795) and vascular groups (AUC=0.835), and the lowest AUC (0.651) was found for the respiratory group, as expected.

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curves for osmolaritymax in six subgroups.
Discussion
Our results reveal that hyperosmolarity is associated with increased hospital mortality of patients who are critically ill, presenting as a ‘U’-shaped association. However, this pattern was not observed for patients with respiratory admission disease, and only extreme hyperosmolarity was related to increased risk of death in this subgroup. In addition, vasopressin is strongly associated with a higher mortality rate in all six subgroups. To the best of our knowledge, this is the largest study using subgroup analysis to establish a link between osmolarity imbalance and mortality in patients in mixed ICU.
Water balance inside the body is of vital importance for patients who are critically ill , and serum osmolarity plays an important role in extracellular and intracellular water distribution. Perturbation of osmolarity is common in patients admitted to ICU, which is related to intracellular dehydration or oedema, potentially leading to adverse outcomes.17 Holtfreter et al recently examined the ability of osmolarity to predict mortality of patients admitted to the ICU13 (AUC=0.732) and revealed an ‘S’-shaped relationship between osmolarity and mortality which is quite different from our finding. Most importantly, the heterogeneity of patients in mixed ICU was ignored, which made it difficult to apply their conclusions in practice.
In the present study, a ‘U’-shaped relationship between osmolaritymax and mortality was found (figure 1), which was similar to Trevor Nicholson’s finding19 that both calculated hypo-osmolarity or hyperosmolarity on admission were associated with increased mortality in emergency patients. However, several differences should be noticed. First, the stratification method was different from ours and more importantly, unlike with patients admitted to emergency, those admitted to ICU were more likely to be unconscious, intubated or sedated,20 21 and insufficient ‘water intake’ commonly happened which lead to higher incidence of hypervolaemic hypernatraemia,20 22 thus, the peak of serum osmolarity may be more important for patients in ICU. Besides, it alleviates the heterogeneity of patients in mixed ICU, subgroup analysis based on admission diagnoses was also performed in our study.
For ICU patients with cardiac diseases, the impact of osmolarity on mortality has not been reported. However, several studies have investigated this association patients in general cardiac. Recently, Arevalo Lorido et al reported that, for patients with heart failure, hyperosmolarity was associated with increased mortality and readmission, but the impact of hypo-osmolarity was insignificant.23 However, the osmolarity categories were not evenly distributed in that study, which lead to the inadequately evaluation of hypo-omolarity. In the present study, the association between hyperosmolaritymax and increased mortality was also observed, with moderately good AUC of 0.7948. In addition, association between hypo-osmolaritymax and mortality was also confirmed in the current study, which is consistent with the findings of De Luca et al 24 Moreover, Rohla et al 8 reported that the significant correlation between hyperosmolarity and mortality for patients with acute coronary syndrome disappeared when the patients who are critically ill were excluded, which further confirms the heterogeneity between patients in general and patients in ICU.
Two aspects should be considered when interpreting the underlying mechanism. First, hyperosmolarity is always accompanied by the increase of its main components, such as hypernatraemia25 and hyperglycaemia,26 which have separately been reported as risk factors for patients with increased mortality of cardiac. Second, hyperosmolarity itself could cause redistribution of body fluids, such as mobilisation of fluid from the venous capacitance vessels to the effective circulatory volume, thereby increasing cardiac preload volume and leading to worse outcomes.
In clinical practice, hyperosmolarity is common in patients with cerebral diseases,7 partly owing to dehydration. Nag et al 9 reported that higher serum osmolarity at admission (≥310 mmoL/L) was associated with early death and worse outcomes, and this was also confirmed by Bhalla et al 7 This correlation was also found in the present study (figure 2), with an AUC of 0.7299. Besides, no correlation between hypo-osmolarity and mortality was found. However, whether treatment to decrease serum osmolarity would benefit these patients was unclear. Therapies such as haemodilution, related to low osmolarity, was adopted in patients with stroke, but the conclusion remains controversial.27–29 Further studies are needed to investigate the interactions among serum osmolarity, osmotherapy and mortality in this subgroup.
For patients with respiratory disease, findings have been contradictory. Experimental data suggested that a hyperosmolar environment (400 mmoL/L, in vitro) may suppress lung injury by upregulating the turnover of cytokine-encoding messenger RNAs10 and reducing neutrophils-human pulmonary microvascular endothelial cells (PMN-HMVEC) adhesion in human pulmonary cells.11 Clinical investigations have found that hypernatraemia, which to a certain degree reflects the effect of osmolarity, was not associated with ICU mortality of patients with respiratory disease.12 However, Yagi et al 30 reported that hyperosmolarity was associated with increased extravascular lung water in patients who are critically ill, which was strongly associated with increased mortality. In addition, one cross-sectional study also indicated that hyperosmolarity had a negative influence on ventilation,31 which may be due to the depressed ventilator response to metabolic acidosis in hyperosmolar conditions.32 Thus, a clear conclusion about the connection between hyperosmolarity and mortality is still lacking. In the present study, no protective effect of hypo-osmolaritymax or hyperosmolaritymax (levels 1 to 5) was detected, but extreme hyperosmolaritymax (≥340 mmoL/L) was related to increased mortality. We boldly speculated that unlike cardiac or kidney dysfunction, lung injury was less likely to cause electrolyte disorder such as water sodium homeostasis. Therefore, the association between serum osmolarity and severity of lung injury is not as strong as the other groups. As for the extreme hyperosmolarity, it may suggest severe disruption of homeostatic mechanisms, especially for sodium, glucose and urea, each of which had a substantial impact on survival independent of osmolarity.
As a vasopressin receptor agonist, vasopressin was used more often in the hyperosmolarity group (table 2), as expected, and a strong link between vasopressin use and mortality was detected for all six subgroups (OR: 1.89–5.57). Currently, the merit of using vasopressin in patients who are critically ill is still debatable. Vasopressin has been recommended to be added to norepinephrine33 for the treatment of septic shock because it has been found to decrease the levels of circulating cytokines, chemokines and growth factors,34 even though it has been reported to be associated with increased adverse events during septic shock.35 Owing to the nature of our observational study, whether vasopressin causes increased mortality or its use is simply a marker of sicker patients with higher risk of death needs to be further investigated.
The advantage of the present study is the large sample size, which allowed for subgroup analysis and adjustment for confounding factors, but it also has limitations. First, the osmolarity was calculated in the present study rather than being measured directly, which could cause deviation from actual osmolarity values despite careful consideration of the optimal equation.16 Second, because osmolaritymax was used as the independent variable, only 292 patients were included in the hypo-osmolarity group (level 1), leaving the effect of hypo-osmolarity unclear. Third, the grouping method was based on diagnosis at admission, and thus overlap within subgroups was unavoidable. Finally, owing to the nature of retrospective research, the association between osmolarity and mortality could only be directly inferred, but it also provided compelling evidence for further research to establish a definitive causal link. Whether treatment or correction of the hypo-osmolarity or hyperosmolarity could reduce mortality among these patients needs further investigation.
References
Footnotes
Contributors YS: Responsible for data analysis and writing of the manuscript.
XC: Responsible for data analysis.
MY: Responsible for study data extraction.
HC: Statistician, responsible for data analysis.
WZ: Responsible for data validation.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Laboratory for Computational Physiology at the Massachusetts Institute of Technology.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Full data set available from the corresponding author at jalmine@sina.com. However, reanalysis of the full data need to be approved by MIMIC II Institute.