Article Text

Abstract
Background Improving access to paediatric HIV treatment requires both large-scale treatment programmes and medication that is adapted to infants and children's needs. The WHO recommends lopinavir/ritonavir as first-line antiretroviral therapy for all HIV-infected children younger than 3 years. There is currently little evidence on the acceptability of, and adherence to, a formulation of this combination treatment if given in the form of pellets. This protocol presents how we will carry a realist evaluation to assess the factors that contribute to the acceptability and adherence to the new pellets formulation in 3 hospitals in Kenya.
Methods We structured the protocol along the realist evaluation cycle following 4 steps: (1) the initial programme theory, (2) the study design, (3) the data collection methods and (4) the data analysis plan. Theories of behavioural sciences were reviewed for frames that could provide insights into how using such new formulations may contribute to better acceptability and adherence.
Ethics and dissemination This study was approved by the Institutional Review Board of the Institute of Tropical Medicine, the Ethical Committee of the University Hospital Antwerp and the Kenyatta National Hospital/University of Nairobi Ethics and Research Committee. We aim to disseminate the findings through international conferences and peer-reviewed journals and to share them with Drugs for Neglected Diseases initiative's (DNDi) programme managers and with the Kenyan healthcare providers.
Discussion In developing this study, we encountered some challenges. First, methods to measure the acceptability of any formulation and adherence to it are not standardised. The second challenge is common in realist evaluation and relates to how to choose from different potentially interesting theoretical frameworks. We identified relevant and empirically tested theories from behavioural science that may be helpful in our study. We will test them in 3 settings by exploring the multilevel factors that influence acceptability and adherence of this new paediatric Antiretroviral (ARV) formulation.
- Paediatric antiretroviral treatment
- realist evaluation
- adherence
- acceptability
- Kenya
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Considering that there are no standardised methods to measure the acceptability and the adherence of any formulation, the proposal to adopt the realist evaluation approach for unpacking the black box between prescription of the drug and the actual long-term adherence is a major strength of this study.
The lack of standardised methods to measure acceptability and adherence may be seen as a limitation of our study.
Given the time constraints of a 1-year study, a complete literature review and full testing of partially contradicting hypotheses was not possible.
Observations at home may suffer from selection bias.
Background
The introduction of antiretroviral therapy (ART) in children has substantially reduced the risk of mortality and morbidity and has transformed the prognosis of HIV infection from a fatal disease into a manageable chronic illness.1–4 However, children living with HIV continue to experience persistent diagnostic challenges and treatment gaps. Globally, there are 2.6 million children under 15 years of age living with HIV and only one in three are on treatment. During 2014 alone, 220 000 children were newly infected with HIV (almost 90% of them in sub-Saharan Africa). Another 150 000 children died worldwide because of HIV, the vast majority before the age of 2, and many without having been diagnosed.5 Most of these deaths could have been avoided if the diagnosis had been made in the first weeks of infection and immediate access to treatment was ensured.6
The 2010 WHO guidelines recommended immediate initiation of ART in all children under 2 years of age regardless of immune or clinical status.7 In 2013, the WHO guidelines re-emphasised the immediate initiation of ART and recommended it for all children below 5 years.8 The WHO recognised the challenge related to the limited availability of drugs in appropriate formulations for infants and toddlers, the long-term toxicities of ARV drugs, and the difficulty with adherence. It is estimated that about half of the 1.2 million children who are exposed to HIV were tested before the age of 2 months, a proportion that is stable since 2014. More progress was made with treatment. Almost half of the HIV-infected children under 15 years of age are now on treatment, more than double the number compared with 2009.9 In Kenya, according to the UNAIDS database, 41% of children (aged 0–14 years) living with HIV had access to ART.10
Improving access to paediatric HIV treatment requires both large-scale treatment programmes and medication that is adapted to the needs of infants and children. Existing paediatric ART typically combines nevirapine (NVP), a non-nucleoside reverse transcriptase inhibitor (NNRTI), with two other nucleoside reverse transcriptase inhibitors (NRTIs): lamivudine (3TC) plus either abacavir (ABC) or zidovudine or stavudine (d4T). Young children with HIV who are exposed to NNRTIs used for prevention of mother to child transmission (PMTCT) may have demonstrable viral resistance in more than half of the cases,11 which compromises the response to NVP-containing first-line ART.12 ,13 For this reason, the revised 2013 WHO guidelines recommend the use of lopinavir/ritonavir (LPV/r) as first-line ART for all children infected with HIV younger than 3 years (36 months) of age, regardless of NNRTI exposure.14
While accumulated evidence demonstrates its superior clinical efficacy over NVP, regardless of the child's prior exposure to ART for PMTCT,15 ,16 LPV/r is still not widely used because of its liquid pharmaceutical formulation. The LPV/r syrup has a high alcohol and solvent content, and a bitter taste; it is therefore difficult to administer. Furthermore, it requires cold chain storage and is prohibitively expensive for many countries. In order to improve the administration of LPV/r as well as its acceptability, Cipla Pharmaceuticals developed mini ‘melt’ tablets in the form of oral pellets. This formulation has clear advantages to syrup in logistical terms (easy storage and transport) and acceptability (it can be administered to children who cannot swallow tablets and has a better taste).13 The LPV/r pellets received tentative approval by the US Food and Drug Administration (FDA) in 2015.
In 2011, the Drugs for Neglected Diseases initiative (DNDi) created a paediatric HIV programme with the commitment to make the LPV/r pellets immediately available for treatment of children infected with HIV in resource-poor settings, while working with Cipla to improve the formulation, assembling in a single-unit LPV/r taste-masked granules and dual NRTI powder.
A randomised controlled trial, the LIVING study,i has been set up in three hospitals in Kenya (Nairobi and Kisumu) with the primary objective of evaluating the effectiveness of LPV/r pellets in addition to the ABC/3TC or AZT/3TC paediatric fixed dose combination tablet under routine treatment conditions in HIV-infected infants and young children who cannot swallow tablets. The study's secondary objectives are to document the safety of LPV/r pellets and associated dual NRTIs, to assess the population pharmacokinetics of LPV/r and dual NRTIs in pellet form, to measure the adherence and to evaluate the acceptability of the pellets and their ease of use by the caregiver and healthcare workers. Initial observations by LIVING researchers indicated a differential uptake of the new formulation by the caregivers and differences in adherence to the treatment.17
Adherence to ART is an important determinant of treatment outcome. It could be argued that effective antiretroviral treatment made HIV a chronic disease, and therefore issues affecting children living with HIV are in essence similar to those affecting children with chronic diseases in general, in terms of ‘living with the disease for always' and requiring a chronic treatment. However, HIV is quite different compared with other chronic diseases in that it is multigenerational, affects primarily vulnerable populations, and has a unique social stigma attached to its transmission modes.18 HIV also requires almost perfect levels of adherence to achieve long-lasting viral suppression, and suboptimal adherence to ART is the most common cause of virological failure.19
Non-adherence to ART, which can take many different forms, can have important public health implications, such as treatment failure, promoting viral mutations and drug resistance.20 Acceptability of drug formulations by caregivers and children is an important determinant of long-term adherence. Acceptability may be viewed as a precondition for adherence, but since many intertwined contextual factors may interfere, it does not lead automatically to adherence.
These unique HIV-related characteristics make adherence behaviour in infants and children quite complex. To unpack the black box between prescription of the drug and the actual long-term adherence, we developed a protocol for a study that adopts the realist evaluation (RE) approach. The study is a substudy to the LIVING study, and conducted in collaboration between DNDi, the Institute of Tropical Medicine (ITM), Antwerp and the Institute of Anthropology, Gender and African Studies in Nairobi (IAGAS), University of Nairobi.
In this paper, we present the protocol of the RE study, labelled ‘RE-LIVING’, which aims at better understanding the factors that contribute to the acceptability and adherence to the new paediatric ART formulation (LPV/r 40/10 mg, oral pellets) in the three Kenyan settings where the LIVING study is currently enrolling study participants.
As mentioned before, acceptability may be perceived as a precondition for adherence but it does not lead automatically to adherence. In addition, adherence to ART is an important determinant of treatment outcome. Therefore, the RE-LIVING main findings may contribute, in the short term, to better understand the factors influencing the adherence to oral pellets introduced by the LIVING study and in the Kenyan-specific context. In the long term, these findings can contribute to better manage some of the adherence-related issues and therefore to have better acceptability to the paediatric treatment as well as to get better treatment outcomes.
Methods
The objective of the RE-LIVING study is to assess the factors that contribute to the acceptability of and adherence to the new paediatric ART formulation LPV/r 40/10 mg pellets in real-life settings. The study sets out to develop a good understanding of the acceptability of the new formulation, to assess the factors that contribute to correctly administering the new formulation when starting the treatment (ie, initiation to adherence) and to assess the factors and the conditions that enable caregivers to maintain adherence to the treatment over time.
For this substudy, we adopted the RE approach, which was developed by Pawson and Tilley21 and based on scientific realism.22 ,23 RE belongs to the school of theory-driven inquiry. Pawson and Tilley argue that evaluation and research need to answer the questions ‘What works in which conditions for whom?’, rather than merely ‘Does it work?’ in order to gather useful data for decision-makers. RE considers that interventions work (or do not) because actors take up what is provided by the intervention (or not). The interaction between ‘intervention’ and ‘actors’ in specific ‘contexts’ triggers ‘mechanisms’ that cause ‘outcomes’ to occur.
RE is theory-guided, starting and ending with middle range theory, often called ‘programme theory’.24 The latter should be considered as a detailed hypothesis that describes how the intervention is expected to lead to its effect and in which conditions. This hypothesis is then tested through empirical research. An RE ends by refining the initial programme theory, setting the scene for a new round of research.21–23 ,25 Figure 1 presents the realist research cycle, along which we structured our protocol.
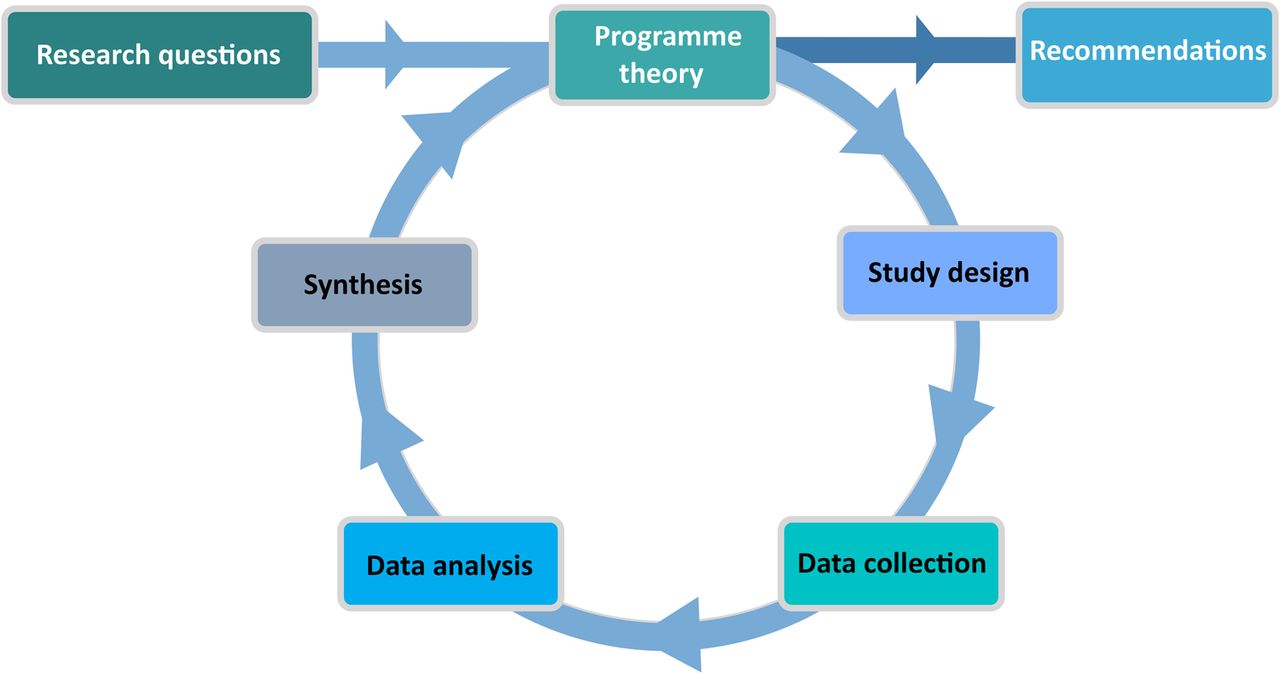
The realist cycle.
Initial observations by LIVING researchers indicated a differential uptake of the new formulation by the caregivers and differences in adherence to the treatment among the three Kenyan settings where the study was implemented. RE will allow us to identify explanations in the form of context-mechanism-outcome (CMO) configurations that explain these differences.
Step 1: formulating the initial programme theory
An RE starts with eliciting the initial programme theory, which will guide further choices of design, and data collection and data analysis methods. A number of sources can be used to elicit the programme theory (figure 2).

Eliciting the programme theory.
The first source of information includes the programme documents, plans and logical frameworks of the intervention under study. In our case, we have reviewed the protocol of the ongoing LIVING study in order to identify the assumptions of the designers on how the new formulation would lead to better adherence.
A second source of information consists of interviews and discussions with designers, funders and/or implementers of the programme and on-site observations can be used to obtain additional information. In our case, we engaged with DNDi staff at the Geneva headquarters and researchers involved in the LIVING study. DNDi staff identified a number of hypothetical factors influencing adherence to the new formulation. These included easier transport and storage and reduced conspicuousness of pellets compared with syrup formulation, less problems with swallowing because of the less bitter taste, etc.
Reviewing the literature is the third way to develop the initial programme theory, aiming at assessing findings of previous evaluations or research studies, and the state of the art in general. First, we examined papers presenting clinical trials that looked at the effectiveness and acceptability of the new formulation (for instance, the Cher trial in South Africa,26 the Promote paediatric trial in Uganda27 or the Chapas-2 study).13 Second, we explored theories of behavioural sciences for concepts and frameworks that could provide insights into how using such new formulations may contribute to better acceptability and adherence.
While we did not carry out any exploratory empirical research to elicit the initial programme theory, reviewing the available evidence shows that a complex set of psychosocial, sociocultural and economic factors, which are often intertwined and mutually influencing each other, determine whether a new medication or treatment will be accepted and adhered to. This has been shown, for instance, with areas in early infant testing for HIV and uptake of HIV care.28 This resulted in a categorisation of factors that influence adherence, including caregiver-related factors, health services and system factors, and sociocultural and community-related factors (box 1).
Multilevel factors related to adherence to treatment
Caregiver-related factors
We identified a number of studies investigating the role and impact of the caregiver on children's adherence. There is evidence that the quality of the caregiver–child relationships, including family functioning,29 influences adherence. This relationship has been shown to be moderated through emotional bonding and the ability to fully care for a child.30 There is no clear evidence if and how a parent's biological relationship affects adherence. Having one person who feels responsible to oversee the child's treatment is likely to result in better adherence than having multiple caregivers.31
Whoever the caregiver, it has been shown that caregivers' personal beliefs about HIV and the treatment, caregivers' education and antiretroviral therapy (ART) comprehension as well as their psychosocial functioning29 are crucial for motivation to support the child. Caregivers who accepted the child's infection were more likely to internalise the information given and developed a stronger motivation for adherence support.32 In the case of vertical transmission, how mothers deal with their own HIV infection may have an influence, especially if they have feelings of guilt or emotional and mental health problems.
Caregivers who are HIV positive and on ART may draw on their own experience when supporting the adherence of their children. A systematic review of 38 quantitative studies found substantial empirical evidence on the relationship between perceived HIV-related stigma and HIV medication adherence. Proposed mechanisms included enhanced vulnerability to mental health conditions, reduction in levels of self-efficacy due to exposure to stigma and concerns about unintended HIV disclosure.33
We found that one of the most widely used behavioural theories to predict adherence outcomes is the information-motivation-behavioural skills (IMB) model.34 It has been applied to various health promotion behaviours, including HIV prevention,35–38 antiretroviral medication adherence39–41 and self-breast examinations.42 It has been validated in resource-rich and resource-limited settings.43–45 While originally developed to predict HIV prevention behaviour, this model can serve as an explanatory framework to explain the caregivers' individual motivation to adhere to the treatment guidelines.
In a nutshell, the IMB model stipulates that individuals who have correct information, sufficient motivation and behavioural skills will be more likely to achieve good adherence. It has been shown that information and motivation influence both directly and indirectly the behavioural outcome and that behavioural skills are an important mediator towards this goal. One central psychological construct in this theory is self-efficacy, that is, the belief to be able to perform the specific behaviour. Self-efficacy has been shown to have great predictive value for behaviour change. Introducing skills as a behavioural construct is important because it constitutes, contrary to personality factors or societal macrofactors, an immediately modifiable factor in interventions that can be addressed through, for instance, patient education and counselling.
Health services and system factors
Easy geographic and financial access to health services may lead to a better ART adherence outcome. The lack of coordination across services has been identified in previous studies as a barrier to timely paediatric ART initiation in low-income and middle-income countries.46 ,47 Failure to diagnose HIV in pregnancy, to provide prevention of mother to child transmission (PMTCT) services or to follow-up the HIV-exposed infant represent missed chances for prevention of HIV transmission, infant diagnosis and linkage to care. Previous research has shown that integrating antenatal services, PMTCT, early infant diagnosis and paediatric HIV care greatly improve outcomes for HIV-infected infants in resource-limited settings.48–50 Finally, good performance of health services may have a positive impact on the user's confidence in the services and trust in their personnel.
Sociocultural factors
Individual-level theories intrinsically focus on microlevel factors, with no specific linkage to macrolevel factors on the structural level.51 However, resources, cultural and social factors like HIV-related stigma, social control and community health beliefs, as well as structural factors such as food shortage and poverty,29 may affect adherence behaviour directly or indirectly. Food insecurity can contribute to enhanced HIV transmission, as well as to antiretroviral therapy non-adherence, treatment interruptions and missed clinic visits, all of which are strong determinants of worse HIV health outcomes.52 The exacerbation of hunger or ART side effects in the absence of adequate food and competing resource demands are potential mechanisms that explain the relationship between food shortage and adherence.53
Individual-level factors are shaped by social and community norms. Research has shown that relevant community perceptions explain why women may be unwilling to take ART including HIV-related stigma, guilt, lack of knowledge, denial, stress and despair or futility. Maternal depression and internalisation of HIV-related stigma, while situated at the individual level, have been shown to further decrease uptake of treatment.54 A literature review18 highlights that while much has been written about how child-specific factors (eg, psychosocial function, neurological development, development stage) and regimen characteristics (eg, drug formulation, changes to treatment plans) may affect children's ART adherence, little is known about social factors impacting children's ART adherence.55
Social support has been shown to enhance adherence to HIV medication, with practical support bearing the highest correlation. Certain factors such as family functioning act as a mediator between social support and adherence.55 Research in Zimbabwe, for instance, has highlighted that despite poverty, social disruption and limited health infrastructure, social support networks creating a social atmosphere of empowerment can be facilitating factors for improving children's adherence.56
We summarised the findings of the review of the programme documents, the discussions with the designers and the literature review in the form of an initial programme theory, which shows how the intervention (ART in the form of pellets, combined with adherence support given by health providers) influences the choice of the caregiver to initiate and maintain treatment (or not). It shows how the context in terms of caregiver–provider relation, health service and system, and sociocultural factors influence the caregiver–infant dyad in the different stages of the adherence pathway (initiation, implementation and/or discontinuation). This programme theory will serve as a hypothesis that will be tested subsequently through qualitative research (figure 3).

{kind=link}
{kind=link}
{kind=link}
The initial programme theory. ART, antiretroviral therapy.
Step 2: study design
RE is design neutral: the design should allow adequate testing of the key elements of the initial programme theory. It is thus the research question and not any methodological or design preference that steers the design of the study. We will adopt the multiple embedded case study design.57 This design is often used in realist research in health.58
Case definition
We define the case in this study as the caregiver–infant couple or the extended family setting in which paediatric HIV care takes place. We will study them as they are embedded in the three facilities in which the LIVING study is being implemented and in their sociocultural context. Having three sites provides us with contrasting cases, as they present different service provision and management modalities, as well as cultural contexts.
Case selection
The cases will be purposively selected. We will include caregiver–infant couples who are enrolled in the LIVING study and who have transitioned from syrup to the new pellet formulation. This group may include dyads who (1) just recently initiated the new treatment, (2) are maintaining the treatment, and (3) initiated and maintain treatment but, because of encountering different problems, have not achieve a long-term adherence to the treatment. In addition, purposive selection criteria will include age, sociodemographic background and other user characteristics (according to the sociodemographic profiles of the LIVING study participants) aiming to achieve a maximum variation sampling.
Step 3: data collection methods, tools and procedures
In terms of data collection methods, RE is method-neutral. In health policy and systems research, often both quantitative and qualitative data are gathered in order to allow rigorous ‘testing’ of the initial programme theory.59
In this study, we will use complementary data collection techniques. First, we will describe the actual implementation of the ART intervention in the three sites. To achieve that, we will collect and analyse intervention guidelines and implementation reports. This document review will allow us to assess the LIVING study outcomes (treatment refusal, treatment initiation, treatment maintenance or implementation and discontinuation).
Second, we will carry out in-depth interviews with caregivers of HIV+ infants and with healthcare providers and, if needed, with health service managers. Here, we expect to explore the personal experiences with the new formula and issues like the perception of adherence support, the role of provider–patient relationships and of communication skills. Candidates will be selected purposively (see Case selection section above) to capture a wide range of opinions, meanings and interpretations concerning the new formulation. We estimate to do at least 15 interviews in each site with caregivers and 5 with providers and managers until data saturation is reached. Interviews will be held in suitable locations and we will use a topic guide that uses open-ended questions.
Third, in each site, one to two focus group discussions (FGDs) will be held with healthcare providers. FGD is an appropriate data collection tool, given its potential for identifying barriers and facilitators to adherence, adherence maintenance and perceived support strategies. We will aim at achieving homogeneous group composition, balancing power issues that may arise (for instance, between nurses and physicians due to their different professional functions and roles, linked to hierarchical positions). The FGDs will be moderated by a social scientist experienced in qualitative research and observed by another social science researcher who will function as a note taker. FGDs will be conducted at convenient locations (eg, meeting room of the clinic). They will last about 1½–2 hours. The FGDs will be recorded, using two recorders and notes will be taken as a backup. After each FGD, the moderator, researchers and the note taker will hold a debriefing meeting. This serves to identify most salient and emerging issues, which will inform the following FGDs to account for an iterative data collection approach.
Finally, to further explore the barriers and facilitators to adherence of the new formula at the level of family/kinship and the service provision, we will conduct observations at the clinic and in study participants' home environments, focusing on but not restricted to the infant's response to the drugs as well as the caregivers' and other family members' reactions. This means that home visits will be planned to coincide with treatment administration. This ethnographic method allows for an in-depth insight into relevant contexts, relationships and behaviours that cannot be assessed through personal inquiry. In this study, we use observations as an overt and complementary method to validate participants' subjective reporting of what they believe and do. In this sense, observation is used for data triangulation and to increase the validity of the overall study findings.
Data collection through observation has two objectives. Observations in the clinic setting aim at observing healthcare provider and study participants' interaction and communication patterns. Items include healthcare provider relationship (active–passive role), responsiveness to patient needs, timing and time constraints, ease of communication and addressing specific (sensitive) topics such as adherence, adherence support strategies and handling of confidentiality. Observations in the home setting aim at observing how study participants practically handle the administration of the pellets, and to get insights into the family-related and contextual factors that may influence this action. They will include ease versus difficulties of administering the pellets, timing and integration in daily routine (meals, etc), support for adherence received through family members, HIV-related stigma and other social predictors of child adherence (for instance, partner conflict, blame for infant's HIV infection, etc).
Kenyan anthropologists will observe the patient–provider interaction (ie, provider attitudes, communication style, supportive motivational strategies), as well as interaction in the home environment. In total, we aim at carrying out five observations in each setting in each of the three study sites. To ensure neutrality, the researcher conducting the participant observation will not contribute to any of the practical aspects of the study (eg, signing ICs, interviewing, etc).
Given the study settings, we apply observation in a moderate way, meaning that the researchers will maintain balance between ‘insider’ and ‘outsider’ roles, allowing for a sufficient degree of involvement while observing in a non-intrusive manner, and keeping the necessary detachment. Observations will be conducted in a systematic way using checklists with the main topics presented above. The researchers will assemble detailed field notes, interview summaries and memos, which form the raw data to be analysed (see below).
Step 4: data analysis
Since the RE is method neutral, we will use appropriate data analysis methods following the best practices of the disciplines from which it borrows the methods.21 In general, the analysis is guided by the CMO configuration, to which we add intervention and actors.
Qualitative data analysis
All recorded interviews and FGDs will be transcribed verbatim and translated where necessary. Interview transcripts and relevant documents will be entered in an N-Vivo database. In line with realist principles, a thematic coding approach will be used based on the core elements of the initial programme theory. We adopt ‘Framework’ analysis,60 which suits the realist approach. For each case belonging to the different clinical settings, we will identify key themes. To do so, the data will be categorised in a first round of analysis using the themes ‘intervention’, ‘actor’, ‘context’, ‘mechanism’ and ‘outcome’.
In essence, realists use retroduction.61 In retroduction, the analysis starts from the observed outcomes and with exploring the context conditions and the mechanisms through which the outcomes can be explained. They use the initial programme theory to guide them in the analysis, but are open to new explanations that emerge from the data. Questions at this stage include:
Identifying outcomes: What are the observed outcomes?
Identifying current intervention: What is the actually implemented intervention?
Identifying the process to reach this outcome: How was it carried out (duration, intensity)?
Identifying actors: Who delivered the intervention? Who are the actors involved in this programme? How did the intervention reach them and to what degree (coverage)?
Identifying links (mechanisms) between intervention and outcome: Can the observed results be linked to the actual intervention?
Once we have intervention-actors-outcomes identified, new interpretations will emerge in subsequent rounds of coding, leading to a refined analysis. At this stage, we will use the following guiding questions:
Identifying context features: Which context conditions facilitated the uptake of the intervention by the actors? Which conditions constrained the actors in taking up the intervention? Are there alternative explanations (ie, other interventions that took place and which may have contributed to the observed outcomes)?
Identifying links (mechanisms) between intervention and outcome: What explains the link between the actual intervention and the actual outcomes?
Typically, the following questions guide this phase: What are the observed outcomes? What is the actually implemented intervention? How was it carried out (duration, intensity)? Who delivered the intervention? Who are the actors involved in this programme? How did the intervention reach them and to what degree (coverage)? Can the observed results be linked to the actual intervention?
Interpretations of how these themes are linked will emerge in subsequent rounds of coding. At this stage, guiding questions include: What explains the link between the actual intervention and the actual outcomes? Which context conditions facilitated the uptake of the intervention by the actors? Which conditions constrained the actors in taking up the intervention? Are there alternative explanations (ie, other interventions that took place and which may have contributed to the observed outcomes)?
We will use methodological triangulation by combining the different qualitative data collection techniques, drawing on data from different source types (interviews, FDGs, observations and document reviews). This will increase the validity of the study's findings. Findings will first be summarised in case research reports and in a second step, a comparison of the findings of the three sites will be carried out.
Documentation of the data collection
Each day, the field research team members will write field notes and a research diary will be kept. This will be kept as a qualitative data log file, identifying the different sources of data collection. Contact summary sheets will be written after each interview to allow recording of impressions and ideas emerging form the interviews. Analytical memos will be written to allow for an iterative approach in data analysis. Case analysis meetings will be held regularly in the form of feedback and discussion meetings of all study collaborators. These will allow for a critical review of observations and preliminary findings and conclusions, as well as an internal peer review.
Monitoring and quality control
The timelines and study milestones will be monitored by the principal investigators at ITM. All digital study materials will be stored in password-protected folders and continuously backed up. All data collectors will receive individual training on conducting qualitative data using the study-specific data collection tools. All transcripts and the translations will be checked for quality and accuracy, and will be adapted if necessary. All digital study material will be stored in password-protected folders and continuously backed up.
Discussion
This paper describes a protocol of an RE that uses a multiple embedded case study design to understand the acceptability and adherence to a new paediatric ART formulation and to identify the factors that contribute to adherence.
While developing this study, we encountered a number of challenges. First, methods to measure the acceptability of any formulation and adherence to it are not standardised.52 Acceptability of the formulation may be assessed on the basis of a caretaker’s report of his/her child’s behaviour when given the medication. Direct observation may also provide insights. For this reason, we decided to both interview the caregivers and carry out observations of the administration of the new formulation in the clinic or at home (provided that the caregiver agrees, see section on ethical issues).
RE is a relatively new methodology. Guidance on how to carry out RE studies is limited and researchers with a broad knowledge of the approach are scarce in the health policy and research community, even more so in low-income and middle-income countries.58 Furthermore, RE requires good insights into the different dimensions of the context that are relevant to the issue under study. In our case, cultural and social context factors are likely to play an important role and, for these reasons, we set up a consortium with experienced social scientists and clinical researchers from Kenya.
A third challenge is common in RE and relates to how to adjudicate between different potentially interesting theoretical frameworks.24 ,62 Especially in case of short project duration, as in our 1-year project, a thorough literature review and full testing of partially contradicting hypotheses will not be possible. We relied on expert opinion to identify a few relevant theories from behavioural science that may be helpful in explaining adherence.
In conclusion, this study will allow for an initial testing of the programme theory as outlined above, and will deliver an in-depth exploration of the multilevel factors that influence acceptability and adherence of this new paediatric ARV formulation. At the same time, this study's findings will add new insights to adherence research in general and we hope that further studies will take off from our results.
Acknowledgments
The authors wish to acknowledge the Drugs for Neglected Diseases initiative (DNDi) for its commitment to and funding of this realist evaluation study.
References
Footnotes
Contributors ANG, CN, BM, JL, ML, OO and IN conceived the study proposal. ANG, CN, BM, JL, OS, ML, OO and IN developed the study proposal. ANG and BM led the writing of this paper. CN, JL, OS, ML, OO and IN contributed to the manuscript. All authors read and approved the final version of the manuscript.
Funding The study protocol reported in this paper has been funded by the Drugs for Neglected Diseases initiative in line with the research collaboration agreement signed between DNDi and ITM.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol has been reviewed and approved by the Institutional Review Board of the ITM (ref. 1088/16), and by the Ethical Committee of the University Hospital Antwerp (Belgian registration number B300201628563). In addition, the protocol has been approved by the Kenyatta National Hospital/University of Nairobi Ethics and Research Committee (reference KNH-ERC/A/293). The study will be carried out according to the principles stated in the Declaration of Helsinki, all related applicable regulations and established international scientific standards. The authors will follow the Code of Ethics of the American Anthropological Association (AAA) and distribute to each participant (before the data collection) an information sheet and an informed consent form.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors aim to disseminate the findings through international conferences and international peer-reviewed journals. The authors aim to share these findings with DNDi's programme managers in the field and in the headquarters as well as with the Kenyan healthcare providers.
↵i Implementation study protocol—protocol number: DNDIPedHIV002. More details on http://www.dndi.org/2016/clinical-trials/clinical-trials-hiv/