Article Text

Abstract
Objective To determine whether an educational leaflet had any effect on seat belt use, seat preference and motor vehicle accidents rate during pregnancy in Japan.
Design Prospective, non-randomised control trial with a questionnaire survey.
Setting Eight obstetric hospitals in Sapporo, Japan.
Participants 2216 pregnant women, of whom 1105 received the leaflet (intervention group) and 1111 did not (control group).
Interventions Distribution of an educational leaflet on seat belt use to women in the intervention group.
Primary outcome measures The effect of an educational leaflet on seat belt use, each pregnant woman’s seat preference and the women’s rates of motor vehicle accidents rate during their pregnancies. To evaluate the effects, the intervention group’s responses to the questionnaires were compared with those of the control group.
Results The proportion of subjects who always used seat belts during pregnancy was significantly higher in the intervention group (91.3%) than in the control group (86.7%; p=0.0005). Among all subjects, the percentage of women who preferred the driver’s seat was lower during pregnancy (27.0%) than before pregnancy (38.7%), and the percentage of women who preferred the rear seat was higher during pregnancy (28.8%) than before pregnancy (21.0%). These two rates did not differ between two groups. Seventy-one women (3.2%) reported experiencing a motor vehicle accident during pregnancy. The motor vehicle accident rate for the intervention group (3.3%) was similar to that for the control group (3.2%).
Conclusions An educational seat belt leaflet was effective in raising the rate of consistent seat belt use during pregnancy, but it did not decrease the rate of motor vehicle accidents. The wearing of seat belts should be promoted more extensively among pregnant women to decrease rates of pregnancy-related morbidity and mortality from motor vehicle accidents.
- leaflet
- seatbelt
- pregnancy
- traffic accidents
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This was a multicentre study including eight hospitals; almost all of which had neonatal intensive care units, with emergency rooms for pregnant women and emergency rooms for traffic accident victims in Sapporo city and the surrounding area.
This study was less biased than the study conducted at only higher facilities due to inclusion of primary facilities.
In this study, the intervention group was compared with the control group, and the current data could be compared with data obtained from the 2013 study including eight hospitals that we had performed in Sapporo.
The results might be influenced by both information bias and selection bias in the participants’ answers, since the study was based on a questionnaire survey.
The leaflet distributed to women in the intervention group did not refer to seat position or motor vehicle accidents during pregnancy, and indirect effects of the leaflet were not observed in this study.
Introduction
The acute traumatic injury included motor vehicle accidents during a pregnancy is a significant contributor to maternal and fetal morbidity and mortality. The motor vehicle accidents have been the leading cause of injury-related maternal death, followed by violence and assault in many countries. The motor vehicle accidents were reported to be the most common causes of trauma during pregnancy (approximately 50%).1–5 In addition, the pregnant woman involved in a motor vehicle accident while driving was associated with elevated rates of adverse the preterm birth, placental abruption and premature rupture of the membranes6 and their infants’ subsequent cerebral palsy.7
According to the study including a total of 507 262 women who gave birth during the study period in Canada, the incidence rate of motor vehicle crashes with pregnant women as drivers during the second trimester was 1.42-fold significantly higher than that during the 3-year baseline interval before pregnancy (p<0.001). Thus, the authors concluded that ‘pregnancy is associated with a substantial risk of a serious motor-vehicle crash during the second trimester, and this risk merits attention for prenatal care’.8 Using a multicentre questionnaire survey targeting pregnant Japanese women in 2013, we have previously demonstrated that the incidence of motor vehicle accidents during pregnancy was 2.9%.9
In a previous report from Sweden, motor vehicle crashes during pregnancy caused 1.4 maternal fatalities per 100 000 pregnancies and a fetus/neonate mortality rate of least 3.7 per 100 000 pregnancies. The incidence of major maternal injury was 23 per 100 000 pregnancies, and crash involvement was 207 per 100 000 pregnancies.10 Based on these data, it is estimated that the number of annual pregnancy-related traffic accident injuries in Japan with approximately 1 million deliveries per year would be approximately 2000–2500, the number of maternal deaths due to pregnancy would be approximately 10–15 and the number of fetal/early neonatal death would be approximately 35–40. Furthermore, in previous report including 57 pregnant women involved in motor vehicle crashes, proper maternal belt-restraint use (with or without airbag deployment) was associated with acceptable fetal outcome (OR 4.5, p=0.033), approximately half of fetal losses in motor vehicle crashes could be prevented if all pregnant women properly wore seat belts.11
The wearing of seat belts reduces the risk of adverse maternal and fetal outcomes from motor vehicle accidents,12 13 and many clinical guidelines recommend proper seat belt use during pregnancy.14–16 According to the ‘Guidelines for Obstetrical Practice in Japan’ of the Japan Society of Obstetrics and Gynecology (JSOG)/Japan Association of Obstetricians and Gynaecologists (JAOG), ‘Damage from car accidents is reduced if seat belts are applied in an appropriate manner. The chest belt should pass between the breasts, and the waist belt should pass below the pubic bone; neither belt should cross the protruding abdomen’.16
According to Japan’s National Police Agency, the rate of fatalities from motor vehicle accidents in 2012 among seat belt users and non-users were 0.14% and 7.9%, respectively, of people in the driver’s seat, 0.17% and 2.9%, respectively, of those in the front passenger seat and 0.15% and 0.49%, respectively, of those in the rear seat.17
In Japan, the rate of using the seat belts among non-pregnant people has been very high (the driver’s seat: 98.8%; the front passenger seat: 95.9%; the rear seat: 38.0% of general roads and the driver’s seat: 99.6%; the front passenger seat: 98.5%; the rear seat: 74.2% of turnpike/expressway in 2018), and those had been increasing during a decade.18 However, the rate of using the seat belts for each sitting position among pregnant women remains unknown.
Despite guideline recommendations and clear evidence of the efficacy of seat belt use, the rate of seat belt use by women decreases after confirmation of pregnancy in Japan, probably because of the inappropriate concern that seat belt use might be harmful to the fetus if the pregnant woman is in a motor vehicle accident.9 In a questionnaire survey examining the driving habits of 135 pregnant women in France, between 90% and 100% of pregnant women wore their seat belts irrespective of their stage of pregnancy, although nearly one-third of subjects considered that the seat belt was dangerous for their unborn child.19
The rate of intrauterine fetal deaths in the seat belt non-users was significantly higher than the seat belt non-users in a motor vehicle accident; therefore, the lack of seat belt use during pregnancy is associated with an increased risk of fxetal death.6 20 However, in some case reports, the fetal death occurred due to seat belt injury of pregnant women involved in an motor vehicle accident.21 22 Thus, educating the women about the ‘correct’ method of using the seat belt during pregnancy is important.4 9
In the previous report from the USA, 2% of women were hurt in a motor vehicle accident during their pregnancy and only 57% of them had received counselling on seat belt use.23 In another previous report from Kuwait, the prenatal care provider counselling for seat belt use occurred in 44.8% women during prenatal visit, and only 21% of pregnant women were using seat belt during the motor vehicle accident.24 Thus, only current counselling on seat belt use would be insufficient to reduce morbidity and mortality rates among pregnant women and fotuses involved motor vehicle accidents.
Furthermore, a campaign to promote seat belt wearing during pregnancy is, therefore, needed. However, large-scale systematic campaigns for this purpose have not been waged in recent years in Japan. The Japan Traffic Safety Association, the National Police Agency, JSOG and JAOG collaboratively published a poster for pregnant women about the correct method of wearing seat belts during pregnancy with the message, ‘The correct method of seat belt wearing saves both maternal and foetal life’.25 This educational poster was accessible on the website,25 but many pregnant women are unaware of it.
To reduce morbidity and mortality rates among pregnant women and fetuses from motor vehicle accidents, more pregnant women must use seat belts. We administered a multicentre questionnaire survey to pregnant Japanese women to evaluate the short-term effect of an educational leaflet to increase the rate of seat belt use during pregnancy.
Methods
Study design
This study was conducted by the eight participating hospitals (Sapporo Maternity Women’s Hospital, Sapporo Toho Hospital, NTT East Japan Sapporo General Hospital, Teine Keijinkai Hospital, Sapporo City Hospital, JCHO Hokkaido Hospital, Sapporo Medical University Hospital and Hokkaido University Hospital) in Sapporo city, whose population was approximately 1.9 million and number of deliveries was approximately 10 000 per year.
During the 8-month study period between 1 January 2018 and 31 August 2018, women in the 35th–37th weeks of pregnancy seeking antenatal care at eight hospital’s outpatient clinics were asked to respond to anonymous questionnaires (box 1).
Questionnaire given to pregnant women at weeks 35–37 of pregnancy
Q1. Did you get the leaflet about the correct method of seat belt use during your current pregnancy?
□ Yes □ No
Q2. How old are you?
□≤19 years □ 20–29 years □ 30–34 years □ 35–39 years □≥40 years
Q3. Have you experienced childbirth previously?
□ Yes □ No
Q4. Do you have your driver’s licence?
□ Yes □ No
Q5-1. Were you an ‘always seat belt user’ before your current pregnancy?
□ Yes □ No
Q5-2. Have you been an ‘always seat belt user’ during your current pregnancy?
□ Yes □ No
Q6-1. Which seat did you prefer before your current pregnancy?
□ Driver’s seat □ Front seat (passenger seat) □ Rear seat
Q6-2. Which seat have you preferred during the current pregnancy?
□ Driver’s seat □ Front seat (passenger seat) □ Rear seat
Q7. Did you always carry Boshi Techo** while going out by motor vehicle?
□ Yes □ No
Q8. Did you have a motor vehicle accident when travelling by motor vehicle during your current pregnancy?
□ Yes □ No
The following questions are for women answering ‘Yes’ in response to Q8.
Q9-1. Which seat were you occupying when you had the motor vehicle accident?
□ Driver’s seat □ Front seat (passenger seat) □ Rear seat
Q9-2. Were you wearing a seat belt when you had the motor vehicle accident?
□ Yes □ No
*Boshi Techo is the Mother and Child Health Handbook provided by the local municipal office for maintenance of medical and welfare records
On the top of the anonymous questionnaires, the note as ‘Even if you cannot cooperate with this research (questionnaire), medical treatment available is the same as those who cooperated, and there is no disadvantage’ was written.
The eight hospitals had 4315 maternity patients during the study period. Women who reported always using a seat belt were classified as ‘always seat belt users’.
An educational leaflet was created from a poster24 (online supplementary figure 1) that recommended seat belt use and showed how to wear a seat belt properly during pregnancy: ‘1) The chest belt should pass between the breasts, 2) the waist belt should pass below the pubic bone, 3) neither belt should cross the protruding abdomen’.
Supplemental material
The women participating during the first half of the study (approximately between 1 January and 30 April) did not receive this educational leaflet and were classified as the control group. The women participating during the second half (approximately between 1 May and 31 August) received the leaflet between weeks 8 and 12 or between weeks 24 and 28 of pregnancy, or both, and were classified as the intervention group.
The leaflets were given to all pregnant women by the midwives (or nurses) or the medical clacks. Then, our medical clacks requested that they read the leaflets at home, but they did not give the announcements to all pregnant women that all pregnant women had to answer the questionnaires at 35–37 weeks of pregnancy. When the pregnant women asked doctors or midwives the questions about using seat belts during their pregnancy, doctors answered them according to the ‘Guidelines for Obstetrical Practice in Japan’ of JSOG/JAOG.16 Furthermore, the questionnaires were given to pregnant women by the midwives (or nurses) or the medical clacks. Then, they requested to all pregnant women that they answered the questionnaires and submitted them to the medical clacks before they went home. Thus, the physicians (medical doctors) did not give the bias to all pregnant women in this study.
To evaluate the educational leaflet’s effect on seat belt use, seat preference and motor vehicle accident rate during the participants’ pregnancies, we compared the two groups’ responses to the questionnaires.
Participants
A total of 2216 pregnant women responded and were enrolled in this study, which corresponded to approximately 51.4% of the 4315 pregnant women in the participating institutions during the study period. Of the women in this study, 1105 women (49.9%) received the leaflet (intervention group) and 1111 women (50.1%) did not (control group).
Statistical analysis
We used JMP Pro (V.14.0) to perform statistical analyses. Fisher’s exact test was used to compare categorical data. In all analyses, a p level of less than 0.05 indicated statistical significance.
Patient and public involvement
No patients were involved in devising the research questions, the outcome measures or the plans for recruitment, design or implementation of the study. No patients were asked to advice on interpretation or writing up of results. There are no plans to disseminate the research study results to study participants or the relevant patient community.
Results
Characteristics of women in intervention group and control group
There was no significant difference between the two groups in percentages of primiparous mothers, ages of mothers, percentage of mothers who possessed a driver’s licence, percentages of mothers who carried the Boshi Techo (the Mother and Child Health Handbook, provided by the local municipal office for maintenance of medical and welfare records) when going out, percentages of mothers who always used seat belts or seat preference before pregnancy (table 1).
Comparison between women in the intervention group to those in the control group
Women who always used seat belts before and during pregnancy
The percentages of women who always used seat belts before pregnancy in the intervention group were similar to that in control group (p=0.4254; table 1).
In the intervention group, the percentage of women who always used seat belts during pregnancy (91.3%) was similar to that of women who always used seat belts before pregnancy (91.0%; p=0.8808). However, in the control group, the percentage of women who always used seat belts during pregnancy (86.7%) was significantly lower than that of women who always used seat belts before pregnancy (90.0%; p=0.0005). Thus, the percentage of women who always used seat belts during pregnancy was significantly higher in the intervention group (91.3% (n=1009 of 1105)) than in the control group (86.7% (n=963 of 1111); p=0.0005; table 1).
In both groups, the number of subjects who always used seat belts and those who did not always use seat belts before and during the current pregnancy are shown in online supplementary figure 2. Of the 1000 women in the control group who had always used seat belts before pregnancy, 938 (93.8%) always used seat belts consistently during pregnancy, whereas of the 1006 in the intervention group who had always used seat belts before pregnancy, 965 (95.9%) always used seat belts consistently during pregnancy; this difference between the groups was significant (p=0.0421; figure 1A). Conversely, of the 111 women in the control group who had not always used seat belts before pregnancy, 25 (22.5%) became ‘always seat belt users’ during pregnancy; this number was significantly lower than that in the intervention group, in which 99 had not always used seat belts before pregnancy and 44 (44.4%) of them became ‘always seat belt users’ during pregnancy (p=0.0082; figure 1B).
Supplemental material

Comparison of the rates of ‘always seat belt use’ (ASU) and seat position preferred between intervention group and control group. Black bar: intervention group; white bar: control group. (A) Rate of non-ASU before pregnancy but ASU during pregnancy. (B) Rate of ASU before pregnancy but non-ASU during pregnancy. (C) Rate of changing preference for driver’s seat (DS) before pregnancy to non-DS (PS; front or rear passenger’ s seat) during pregnancy. (D) Rate of changing preference for non-DS (PS) before pregnancy to Ds during pregnancy. (E) Rate of changing preference for front seat (FS; DS or front passenger’s seat) before pregnancy to rear seat (RS) during pregnancy. (F) Rate of changing preference for RS before pregnancy to FS during pregnancy.
Seat preference before and during pregnancy
In both groups, the number of subjects who used the driver’s seat before pregnancy and those who did not use the driver’s seat before and during the current pregnancy are shown in online supplementary figure 3. The numbers of women who used the driver’s seat before pregnancy and changed to using a passenger seat (front or rear) during pregnancy (intervention: 35.4% (157/443); control: 33.2% (138/416); p=0.5178; figure 1C), and the numbers of women who changed from using passenger seats (front or rear) to using driver’s seats (intervention: 2.6% (17/662); control: 2.6% (18/695); p=1.000; figure 1D), did not differ significantly between the two groups. Similarly, the number of women whose preference for the driver’s seat or front passenger seat to the rear seat after pregnancy were almost the same in the two groups (figure 1E), as were the numbers whose preference changed from the rear seat changed to preference for the driver’s seat or front passenger seat (figure 1F).
Supplemental material
Motor vehicle accidents during pregnancy
Of all the women in this study, 71 (3.2%) reported having experienced a motor vehicle accident during their pregnancies. The incidence of motor vehicle accidents among women in the intervention group (n=36 (3.3%)) was similar to that among women in the control group (n=35 (3.2%); p=0.9045; see table 1).
Relationship between always using seat belts/seat preference and motor vehicle accidents during pregnancy
Among the 1972 pregnant women who always used seat belts, the rate of motor vehicle accidents (n=62 (3.1%)) was similar to that among the 244 who did not always use seat belts (n=9 (3.7%); p=0.5678; see online supplementary figure 2). The rate of motor vehicle accidents was significantly higher among the 599 pregnant women who used the driver’s seat (n=27 (4.5%)) than among the 1617 who used the (front or rear) passenger seat (n=44 (2.7%); p=0.0411; see online supplementary figure 3). Among the 638 who used a rear seat during pregnancy, the rate of motor vehicle accidents (n=15 (2.4%)) was similar to that among the 1578 who used the driver’s seat or front passenger seat (n=56 (35%); p=0.1822; see online supplementary figure 4).
Supplemental material
Discussion
The rate of seat belt use during pregnancy decreases from that before pregnancy in Japan.9 26 This decrease probably arises from misunderstandings about the safety of seat belt use for a fetus during motor vehicle accidents, despite reports that seat belt use is effective for lowering rates of mortality and morbidity in motor vehicle accidents.15 16 This irrational avoidance of the seat belt use during pregnancy was observed in this study, and our simple intervention providing a leaflet that recommended and gave instructions on the proper method of seat belt wearing was shown to help women continue using seat belts. To our knowledge, this is the first study of the effect of an educational leaflet on reducing avoidance of seat belt use during pregnancy.
This effect resulted from three factors observed in the intervention group: (1) a decrease in the number of women who had always used seat belts before pregnancy and used seat belts less frequently during pregnancy (control group: n=62 (5.6%); intervention group: n=41 (3.7%)); (2) an increase in the number of women who had not always used seat belts before pregnancy and became ‘always seat belt users’ during pregnancy (control group: n=25 (2.3%); intervention group: n=44 (4.0%)) and (3) a decrease in the number of women who did not always use seat belts before and during pregnancy (control group: n=86 (7.7%); intervention group: n=55 (5.0%)).
In the USA, the seat belt non-users were more likely to be younger (between 18 and 24 years)6 and primiparous.20 Among the 244 women who did not always use seat belts during pregnancy in the present study, the characteristics of women who, before pregnancy, had always worn seat belts may have differed from those of women who, before pregnancy, had not always worn seat belts. The 141 women who had not always worn seat belts both before and during pregnancy reported a significantly higher rate of multiparity (71.0% (n=93)) than did the 103 women who always wore seat belts before, but not during, pregnancy (47.6% (n=49); p=0.0004), used the driver’s seat significantly more during pregnancy (32.6% (n=46) vs 14.6% (n=15), respectively; p=0.0016) and carried Boshi Techo relatively less often (36.2% (n=51) vs 48.5% (n=50), respectively; p=0.0654). Thus, for multiparous pregnant women, pregnant women who use the driver’s seat and those who do not carry the Boshi Techo regularly, a strategy stronger than leaflet distribution might be necessary to change careless behaviour in Japan.
‘Boshi Techo’ is the Mother and Child Health Handbook, provided by the local municipal office for maintenance of medical and welfare records. In Japan, the classical first version of Boshi Techo was introduced in 1942, and all pregnant women have used its traditional version of Boshi Techo since 1965.27 Thus, many people would think that Boshi Techo was used in only Japan. However, the English version of Boshi Techo has been published since 1983 in Japan, so Boshi Techo has been used in some counties of Asia and Africa (Indonesia, Thailand, Mexico, Nepal, Guatemala, China, Vietnam, Palestine, Afghanistan, Tajikistan and so on) and France and Netherlands in Europe and in State of Utah of USA since 1990.28 In addition, Boshi Techo has been used in Rosia since November 2017.
In the previous report between 2001 and 2008 from the USA, 40% of pregnant women in motor vehicle accidents were drivers and the risk of being a driver in a motor vehicle accident was 12.6 per 1000 pregnant women.29 In the present study, the leaflet did not influence seat preference or incidence of motor vehicle accidents during participants’ pregnancy. The percentage of women in the intervention group who used the driver’s seat before pregnancy and stopped using it during pregnancy was similar to that in the control group. Similarly, among the women who had not used the driver’s seat before pregnancy but did so during pregnancy, women who had used the front passenger seat before pregnancy and the rear seat during pregnancy and the women who had used the rear seat before pregnancy and the front passenger seat, the rates of motor vehicle accidents during pregnancy did not differ from the corresponding rates in the control group. The leaflet did not refer to seat position or motor vehicle accidents during pregnancy, and indirect effects of the leaflet were not observed in this study. In the previous study between 2000 and 2012 from the USA, 65% of pregnant women were seated in the front left seat position (driver’s seat) and roughly the same percentage of pregnant women was wearing a seat belt (lap and shoulder belt).30
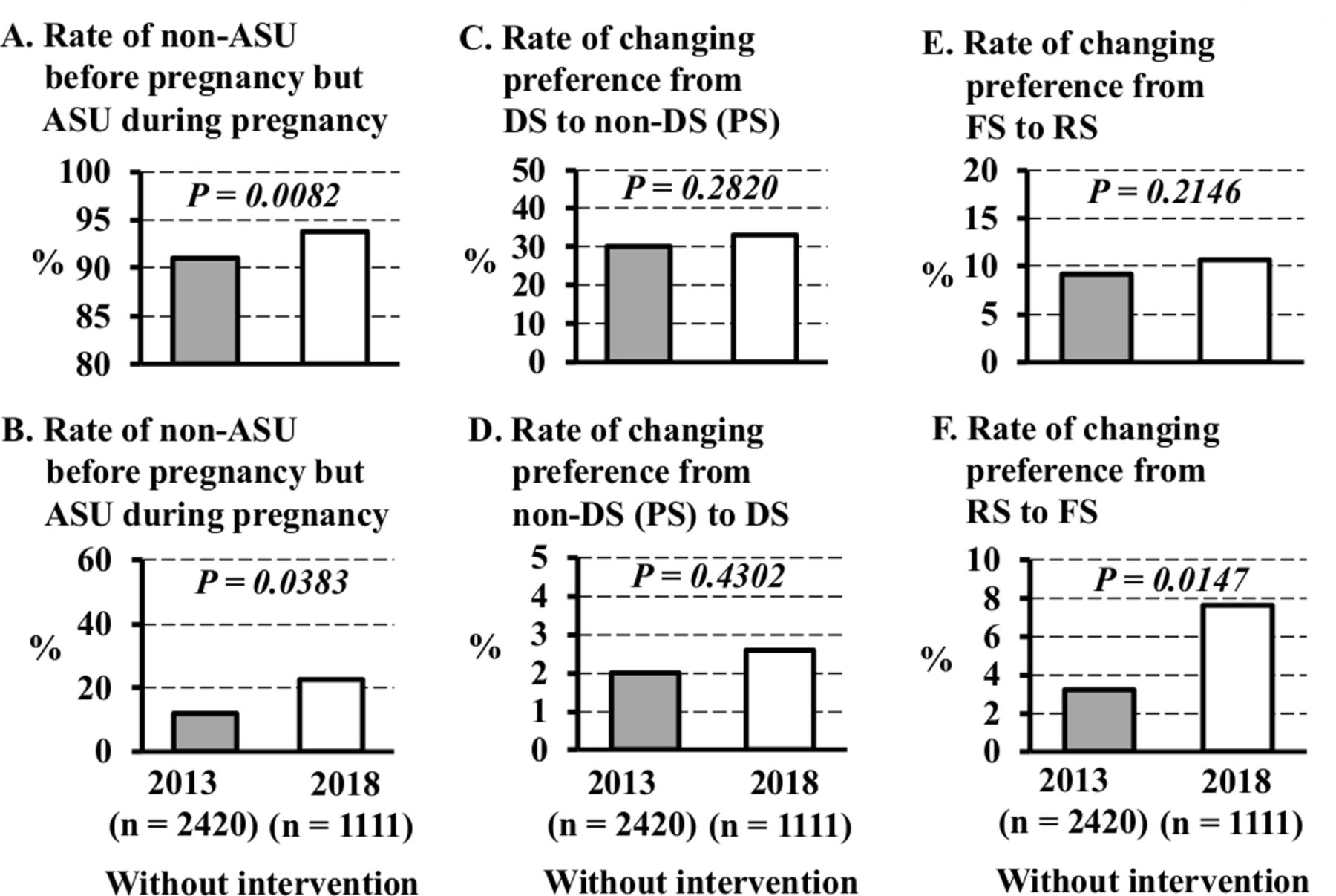
This study was conducted in almost the same hospitals as our previous study (study 2013) without the intervention.9 In comparison with data from the 2013 study, pregnant Japanese women without the intervention in this study (control group) exhibited behaviour changes (table 2 and figure 2).
Comparison between women in the control group to those in the 2013 study

{kind=link}
{kind=link}
Surprisingly, the percentage of women in the control group who had always worn seat belts before pregnancy was significantly lower in this study (90.0%) than in the 2013 study (94.5%; p<0.0001; table 2). In addition, the percentage of women in the control group who had preference for rear seat before pregnancy and during pregnancy were significantly higher in this study (22.4% and 29.0%, respectively) than in the 2013 study (16.6% and 23.8%; p=0.0001 and p=0.0010, respectively; table 2).
Furthermore, the percentage of women in the control group always carried Boshi Techo when going out was significantly higher in this study (51.5%) than in the 2013 study (43.0%; p<0.0001; table 2). Thus, the careful attitude of pregnant women towards driving safety would be significantly higher in this study than in the 2013 study.
However, the percentage of women in the control group who had always worn seat belts before and during pregnancy was significantly higher in this study (93.8%) than in the 2013 study (91.0% (n=2215); p=0.0082, figure 2A), and the percentage of women who had not always worn seat belts before pregnancy, but always used them during pregnancy, was significantly higher (22.5%) in this study than in the 2013 study (11.9% (n=16 of 134); p=0.0383; figure 2B). Thus, the number of women in the control group who always used seat belts during pregnancy was almost the same in this study as it was in the 2013 study.
The numbers of women who used the driver’s seat before pregnancy and changed to using a passenger seat (front or rear) during pregnancy (figure 2C), and the numbers of women who changed from using passenger seats (front or rear) to using driver’s seats (figure 2D), did not differ significantly between the two groups. Similarly, the number whose preference changed from the driver’s seat or front passenger seat to the rear seat was almost the same in the two groups (figure 2E); however, the number of women whose preference for the rear seat changed to preference for the driver’s seat or front passenger seat after pregnancy was significantly higher (7.6%) in this study than those in the 2013 study (3.2%; p=0.0147, figure 2F). To decrease rates of morbidity and mortality from motor vehicle accidents during pregnancy, a more extensive and systematic campaign to promote rear seat sitting during pregnancy may be necessary. Furthermore, we should know the information that the seat belt systems for rear seats might need to be developed to improve passenger safety, especially for pregnant women because of short height and late term of pregnancy with protrusion of the abdomen, the shoulder belt deviates to the right or left, avoiding the protruded uterus, and subsequently makes the contact with the neck.31
More preferable behaviour changes were observed in the intervention group in this study: the percentage of women who always used seat belts during pregnancy (91.3%) was significantly higher than that in the 2013 study (86.7% (n=2097 of 2420); p<0.0001). Thus, the overall increase in always using seat belts during pregnancy in intervention group indicated effectiveness of the leaflet. The percentage of women who were in motor vehicle accidents during pregnancy in this study (3.2%) was similar to that in the 2013 study (2.9% (n=70 of 2350); p=0.5499).
We may have missed responses from pregnant women who died or were injured in motor vehicle accidents or who experienced fetal loss in association with motor vehicle accidents, even though none of the eight hospitals reported maternal deaths or fetal demise due to motor vehicle accidents during the study period. However, based on the above report from Sweden,10 it is estimated that the number of maternal deaths due to pregnancy would be approximately 0.03, the number of fetal/early neonatal death would be approximately 0.08 and the number of crash involvements would be approximately 49 in this study (n=2216). Thus, we would have not missed responses from pregnant women who died by motor vehicle accidents in this study with 71 crash involvements but no maternal and/or fetal/early neonatal deaths.
The current study had three major strengths. First, this was a multicentre study including eight hospitals, almost all of which had neonatal intensive care units, with emergency rooms for pregnant women and emergency rooms for traffic accident victims in Sapporo city and the surrounding area. Second, this study was less biased than the study conducted at only higher facilities due to inclusion of primary facilities. Third, the intervention group was compared with a control group in this study, and the current data could be compared with data from the 2013 study including eight hospitals performed in Sapporo.
This study had three limitations. First, the results might be influenced by both information bias and selection bias in the participants’ answers, since the study design was based on a questionnaire survey. Second, the leaflet that was distributed to the women in intervention group did not refer to seat position or motor vehicle accidents during pregnancy, and indirect effects of the leaflet were not observed in this study.
In conclusion, the simple intervention of providing a leaflet recommending and giving instructions for wearing seat belts during pregnancy was effective in maintaining the number of women who always used seat belts, but it was not associated with the frequency of motor vehicle accidents during pregnancy. To decrease rates of morbidity and mortality from motor vehicle accidents during pregnancy, a more extensive and systematic campaign to promote seat belt wearing during pregnancy may be necessary. In addition, the activity of direct advice by physicians (medical doctors) to promote seat belt wearing during pregnancy would be necessary.
References
Footnotes
Contributors MM and TY conceived and designed the study. MM, TY, HK, MS, AN, YF, EKH and SI accessed data at their participating hospitals. MM conducted the data analysis and drafted the initial version of the manuscript. TY provided important insight during the data analysis. All authors contributed to data interpretation, critically revised the manuscript, had full access to the data in the study and take responsibility for data integrity and data analysis accuracy. HW is the guarantor. The corresponding author attests that all listed authors meet authorship criteria, and that persons who did not meet the criteria have been omitted.
Funding This study was supported by a grant from The General Insurance Association of Japan (Tokyo, Japan). http://www.sonpo.or.jp/en/
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Institutional Review Board of Hokkaido University Hospital (017-0231).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.