Article Text

Abstract
Introduction Social communication difficulties (SCDs) occur frequently after an acquired brain injury (ABI) and have disabling consequences, but effective interventions are scant. Group Interactive Structured Treatment (GIST) is a holistic group treatment targeting SCD that has received empirical support.
Objective To determine the efficacy of two GIST protocols, standard GIST and a newly developed intensive GIST, comparing standard GIST results to a wait-list control group (WL), as well as to intensive GIST received by participants following WL. The within subject results for WL and intensive GIST will also be examined.
Methods and analysis Sixty adults (18–75 years) with SCD after ABI will be recruited for this randomised controlled trial. Standard GIST (n=30) will be delivered via outpatient sessions for 2.5 hours once per week for 12 weeks, plus one initial orientation session. Participants will be assessed at preintervention and postintervention and at 3-month and 6-month follow-ups (T1-T4). Intensive GIST (n=30) participants will be admitted to an inpatient rehabilitation unit for 4 weeks (two times 3 days/week, two times 4 days/week) and receive full-day sessions each week. Those participants will complete four assessments (T1-T4) in 12-week intervals as part of WL, assessments preintensive and postintensive GIST and at 3-month and 6-month follow-ups (T4-T7). The primary outcome measure is the La Trobe Questionnaire (self-report). Secondary outcome measures include the Profile of Pragmatic Impairment in Communication, a test of emotion recognition, the Goal Attainment Scale and questionnaires addressing social, emotional and cognitive functions, self-efficacy and quality of life.
Ethics and dissemination Results will be communicated through international, peer-reviewed and popular science journals and presentations at scientific conferences. The study is approved by the Regional Committees for Medical and Health Research Ethics Norway (2017/1360). The trial will be conducted in accordance with the Declaration of Helsinki and reported in accordance with the Consolidated Standards of Reporting Trials 2010 statement and Standard Protocol Items: Recommendations for Interventional Trials recommendations.
Trial registration number NCT03636399.
- brain injury
- social competence
- GIST
- cognitive rehabilitation
- group treatment
- evidence-based
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The sample size, well-defined outcome measures and the inclusion of two follow-up sessions (at 3 and 6 months) are the strengths of the study.
The effects of an intensive Group Interactive Structured Treatment protocol for inpatients will be explored for the first time.
A robust randomised controlled design, including an active control group with all participants receiving treatment, may enhance study adherence and also address the ethical challenges of using control groups.
The active involvement and commitment from a close family member/friend for home assignments is a major strength of the study because this support may increase the likelihood of participants achieving their social communication goals and may also improve the return to everyday life.
Limitations include the risk of bias due to lack of sample stratification, non-adherence to the interventions and dropout due to a long waiting period and the comprehensive and time-consuming interventions.
INTRODUCTION
A number of patients with an acquired brain injury (ABI) experience cognitive difficulties that affect the way they communicate.1–3 Indeed, cognitive processes, such as memory, attention and executive functions, are important in social communication and may affect the ability to remember information, to avoid making inappropriate statements4 and to attribute mental states (ie, beliefs, goals, intentions, emotions) to oneself or others (eg, theory of mind; ToM).5–7 Social communication deficits following ABI are often referred to as social communication difficulties (SCD),3 4 cognitive communication disorders8 or pragmatic language disorders.9 In this paper, the term SCD is used.
SCD represent one of the most prevalent and persistent problems following ABI.3 10 Some studies have indicated that 34% to 70% of persons with traumatic brain injury (TBI),11 12 and 50%–94% of persons with right hemisphere stroke13 14 experience difficulties in at least one aspect of social communication, including long-term difficulties with emotional recognition, ToM and general behaviour issues.15 A lack of successful social skills can lead to conflicts, isolation and limited access to social and vocational opportunities.16 In fact, impaired management of communication exchange represents a major barrier to social reintegration for persons with ABI.12 17 Despite these major barriers, few studies have investigated the efficacy of treatments for persons with SCD.
According to the cognitive rehabilitation recommendations (2012–2014) provided by the American Congress of Rehabilitation Medicine (ACRM), the main goal in the treatment of SCD should be to develop skills in assertiveness, communicating needs and thoughts using and interpreting nonverbal messages and regulating emotions.4 18 This is further supported by Cicerone et al in their most recent systematic review including five studies from 2009 to 2014 recommending interventions focusing on pragmatic conversational skills and recognition of emotions for people with SCD.19 In a similar vein, the work by Togher et al highlight two main approaches of group treatments for SCD: standardised social skills training and conversational skills training.20 Of the two, conversational skills training that included training close family members and communication partners, demonstrated more immediate generalised effects of trained behaviour as well as several months after treatment.20
A systematic review conducted by Finch et al, including trials through October 2013, concludes that the evidence supports a context-sensitive approach to treatment for adults with SCD delivered in a group setting.3 Individual goal-setting, group-based activities with or without an individual component, homework and feedback were described as key components of context-sensitive approaches.3 Of note, Group Interactive Structured Treatment (GIST) is one of the key approaches that incorporate these components.3 18 21 To the authors’ knowledge, these are the most recent systematic reviews describing SCD interventions, and a search of Ovid MEDLINE in April 2019 indicated that only four studies have been conducted since 2013. These four studies22–25 provide further evidence for the efficacy of SCD interventions.
The latest study, a multicentre randomised controlled trial (RCT) conducted by Harrison-Felix et al, compared two methods of GIST: an interactive group format versus a classroom lecture.25 They found that social competence skills improved in both treatment groups and the interactive format was not found to be superior to the classroom treatment using the same curriculum.25 This study provides evidence for the efficacy of GIST across different delivery formats.
Still, GIST is one of the best-validated context-sensitive group interventions for SCD,21 25 26 and the treatment emphasises self-assessment, individual goal setting and facilitates generalisation through homework and family or friend involvement.18 The efficacy of GIST has been demonstrated in several systematic reviews and guidelines,1 3 19 20 and findings have suggested improved social communication and overall satisfaction with life in various TBI populations, with results also maintained at follow-up.21 25 26 Hence, application to broader patient groups seems feasible. In fact, our group developed an intensive version of GIST (intensive GIST) for ABI inpatients (including right hemisphere stroke) in the chronic phase and conducted a pilot study (n=6) exploring its feasibility and acceptability.27 This newly developed GIST protocol integrates intensive rehabilitation in the chronic phase, which is associated with better functional communication outcomes in other ABI populations (eg, aphasia).28–30 The intervention included the same sessions as the standard GIST protocol for outpatients, but was presented in a more condensed timeframe, in addition to being delivered in an inpatient setting. Feedback from the participants indicated that the protocol included sufficient time and opportunities to work on individual social communication goals. As the present study will examine the efficacy of intensive GIST, the results will contribute to increased knowledge of SCD treatment dosage.
STUDY AIMS AND HYPOTHESES
The main objective of the study is to determine the efficacy of GIST for persons with ABI and SCD. Hence, the aims include the following:
To determine the efficacy of two GIST protocols (standard GIST and intensive GIST) by comparing (1) standard GIST to intensive GIST, (2) standard GIST to a wait-list control group (WL) and (3) the within subject results between the WL and the intensive GIST.
Examine close family member/friends’ experiences of change in the participant’s SCDs following the standard GIST and intensive GIST.
It is hypothesised that there will be a greater reduction in SCD following GIST (both protocols) when compared with the results from WL. It is also hypothesised that intensive GIST will be equally effective as standard GIST. Finally, it is expected that close family member/friends will report positive changes in the participants’ social communication skills following both standard GIST and intensive GIST assessed at 6-month follow-up.
METHODS AND ANALYSIS
Study design
The proposed study is an RCT comparing two different GIST versions, standard GIST (n=30) and intensive GIST (n=30). Additionally, the results from both treatments will be compared with the results from persons in the WL group, who will later receive intensive GIST. The WL design is based on previous studies.21 31 A repeated-measures design will be employed across four time points for the standard GIST group (preintervention and postintervention, and 3-month and 6-month follow-ups) and seven time points for the WL/intensive GIST group (see figure 1). This will allow us to make comparisons between the standard GIST and intensive GIST, between the standard GIST and WL, and within subjects for the WL and intensive GIST.

CONSORT 2010 flow diagram. CONSORT, Consolidated Standards of Reporting Trials; GIST, Group Interactive Structured Treatment.
The trial will be conducted and reported according to Consolidated Standards of Reporting Trials (CONSORT) guidelines32 and good clinical practice.33 The flow diagram is depicted in figure 1. The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist will be used, as recommended, as the protocol closely mirrors the CONSORT statement and ethical considerations.34 In addition, the Template for Intervention Description and Replication (TIDieR) checklist and guide35 will be used. The SPIRIT checklist is applied in figure 1, and provided in online supplementary file 1. The CONSORT and TIDieR checklists are provided in online supplementary files 2 and 3.
Supplemental material
Study setting
Sixty participants with ABI and SCD and 60 of their close family members/friends will be recruited through several channels in order to cover health institutions, rehabilitation settings and arenas where eligible participants in the chronic stage are typically found: (1) Participants will be invited to participate in the study based on discharge diagnosis and hospital record information from Sunnaas Rehabilitation Hospital (SRH) in Norway. (2) Participants will also be recruited from speech-language pathologists (SLP) in south-eastern Norway and (3) by directly advertising on social media such as Facebook and through user organisations. The recruitment of patients began in September 2018 and is planned to be completed by autumn 2019.
Participants
Eligibility criteria
The study population consists of adults (18–75 years) diagnosed with ABI resulting from both TBI and non-traumatic brain injuries (eg, cerebrovascular accidents (CVA), brain tumours, anoxic incidents). The patient journal at SRH will be screened for patients who have undergone rehabilitation from 2014 to 2017 as a result of either TBI or non-traumatic brain injuries and who have documented cognitive deficits, such as difficulties with memory, attention and/or executive function. Participants will also be recruited by advertising at user organisations and through local SLP. The inclusion criteria are: (1) TBI or non-traumatic brain injuries, a minimum of 12 months post-injury with no upper limit; (2) SCD, as assessed by both self-reports and a family member; (3) motivation for treatment, including an expressed desire to change communication behaviour; (4) one close family member/friend able to participate as a support person during home assignments throughout the treatment; (5) adequate Norwegian language proficiency to participate; (6) communication difficulties reported for a minimum three questions (ie, ‘often’ or ‘always’) on the La Trobe Communication Questionnaire (LCQ)35; and (7) a minimum level of intellectual insight into communication difficulties, as assessed with the Awareness Questionnaire (>20 in the discrepancy score).36 37 Patients will be excluded from the study if they meet any of the following criteria: (1) major psychiatric disorder or reported ongoing alcohol or substance abuse; (2) concomitant neurological diseases; (3) severe cognitive, sensory, physical or language impairment affecting the capacity to complete the intervention; or (4) communication difficulties primarily associated with aphasia (as assessed by an SLP).
Procedure
Information about the study, including a written consent form, will be sent to eligible participants at recruitment. Verbal consent will be required before conducting a more thorough telephone screening interview and before participants are summoned to an inclusion assessment meeting at the hospital. The inclusion assessment will be conducted with both the participant and close family member/friend present to provide information regarding the two treatment conditions and to assess willingness to participate prior to enrolment. If some of the participants express a preference to one of the treatments, the assessor will clarify that group allocation is decided through randomisation. However, any preferences will be reported for possible data analysis. During the inclusion assessment meeting, written informed consent will be obtained. Once the participants are approved for inclusion, they will complete a baseline assessment (T1) before they are randomly assigned to either standard GIST or WL/intensive GIST.
Randomisation
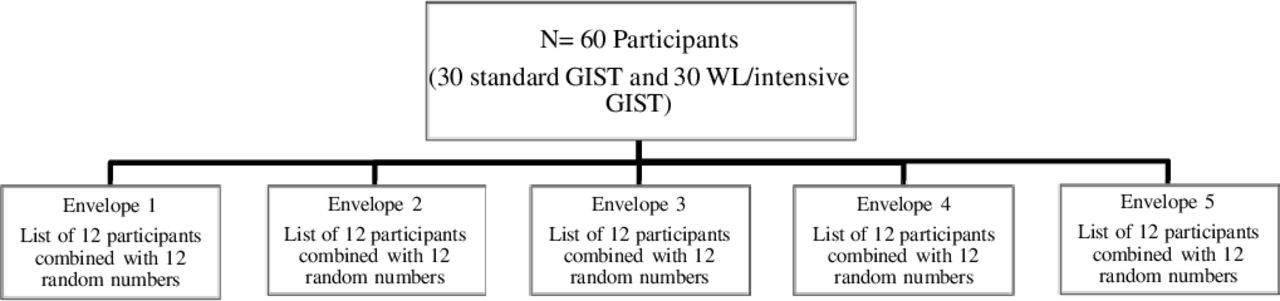
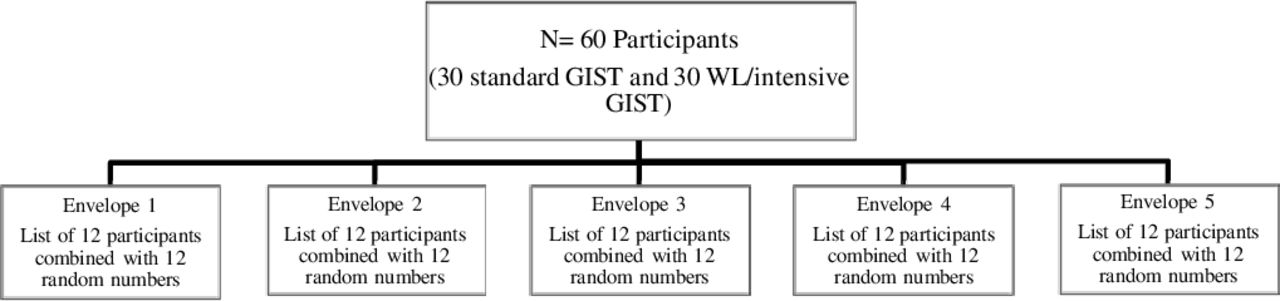
The participants will be randomly assigned to either standard GIST or WL/intensive GIST with a 1:1 ratio (see figure 2). All participants included in the study will be in the chronic phase with a minimum of 12 months since an ABI. The randomisation sequence list will be created in advance by a researcher who is not a member of the research team, using an online list randomiser.38 The list for each of the five subgroups will be placed in sealed envelopes, and the envelopes will then be randomly numbered 1–5. The condition will be set in advance to allocate even numbers to standard GIST and odd numbers to WL/intensive GIST. Once the randomisation is completed, participants will be informed of the group to which they have been allocated. This process will continue until all 12 participants in subgroup 1 have been allocated, at which point the randomisation from the second envelope will begin. The entire process will be repeated five times until all participants are allocated to treatment groups of six. The group size is based on the recommendations of GIST developers.18
{kind=link}
{kind=link}
Overview of the randomisation process. GIST, Group Interactive Structured Treatment; WL. wait-list control group.
Measures
In addition to the demographic interview, a variety of neuropsychological tests and questionnaires will be administered at T1, T2, T3 and T4 as well as T5–T7 for the WL/intensive GIST group (see table 1).
Measures used in the study at different assessment points
Primary outcome measures
The LCQ35 (self-report) will be employed as the primary outcome measure in the present RCT. Both Braden et al26 and Harrison-Felix et al,25 found the LCQ to be sensitive to change in social communication skills, and comparable with changes found in Social Communication Skills Questionnaire–Adapted (SCSQ-A) used as primary outcome measures in other GIST trials.26 The LCQ has been psychometrically evaluated with excellent results in the TBI population,35 39 40 and it has been translated into Norwegian. Also, based on the multiple causes of SCD, the LCQ-developer39 anticipates that the LCQ will provide useful information across the ABI populations. The LCQ is a 30-item self-report and other-report questionnaire assessing communication ability. Various communication behaviours are rated on a four-point scale: never or rarely (1), sometimes (2), often (3) and usually or always (4). Higher scores reflect greater perceived communicative difficulty. This LCQ is self-completed at each assessment point by participants with ABI, with the assessor present to clarify items if needed.
Secondary outcome measures
A conversation between the participant and a close family member/friend will be videotaped at each assessment point as part of the clinical assessment. In the cases, where the assessments will be conducted over the telephone, the participant and close family member/friend will also be instructed to conduct the video recording at home. Before each recording, the assessor will instruct the participant and the close family member/friend to have a conversation about a self-chosen topic for 10 minutes. The videos will be analysed by a trained research assistant who is blinded to group allocation, by using the observation form Profile of Pragmatic Impairment in Communication (PPIC).41 The PPIC is an objective measure of social communication skills designed specifically for people with ABI. It includes 10 feature summary scales that assess communication skills on a six-point scale from normative (0) to very severely impaired (5), with lower scores indicating better performance. Author SMH will analyse 25% of the video clips, randomly chosen, to ensure inter-rater reliability.
Another secondary outcome measure is the SCSQ-A21 42 which is a 37-item self and informant questionnaire including various communication behaviours that are rated on a five-point Likert scale. The SCSQ-A contains additional questions added by Dahlberg et al21 that are designed to capture all topics covered in GIST. Self-report forms regarding emotional and cognitive function, self-efficacy and quality of life will also be included along with a test of emotion recognition ability (see table 1). To assess self-efficacy during treatment, a process measure has been developed for the participants to complete after sessions 2, 7, 10 and 12. The process measure contains 10 statements regarding social communication skills, and participants are instructed to consider their own social communication skills in relation to these statements on a ten-point scale ranging from 1 (‘I completely disagree’) to 10 (‘I completely agree’). Goal Attainment Scaling43 will also be employed to assess goal achievement after treatment.
The administration of the Mind in the Eyes test6 following intervention will be completed by an assessor not blinded to treatment allocation; however, this test does not require the assessor to interpret the answers. The participants and close family members/friends will complete the secondary outcome measures following intervention at home without influence from the assessor. The assessment points will be audio-recorded so that test scoring of the tests will be conducted by a trained research assistant blinded to group allocation to ensure inter-rater reliability.
Interventions
Arm 1—standard GIST: The treatment comprises 12 modules, plus one initial group orientation session, over a period of 12 weeks (weekly outpatient sessions). In previous studies,21 26 standard GIST has been carried out in 1.5-hour sessions; however, based on observations from our pilot study (eg, fatigue), this has been extended to 2.5 hours (32.5 contact/treatment hours in total including the initial group orientation session), allowing for more breaks. There will be two follow-up treatment sessions after 3 and 6 months.18 In all group modules, a new topic will be presented, discussed and practised with group exercises. The participants will be asked to focus on their social communication skill goals, defined early in treatment, and to work on home assignments with their close family member/friends between the sessions.
Arm 2—WL (control)/intensive GIST: Following a WL period (9 months) the WL group will receive intensive GIST. Participants will be admitted to an inpatient treatment for 4 weeks in addition to two follow-up sessions after 3 and 6 months. Intensive GIST consists of the same 12 modules as arm 1 (ie, manualised) in an inpatient setting (2x 3 days/week, 2x 4 days/week). Due to the intensive time schedule, participants do not have the same number of weeks available for home practise and to work on their individual social communication goals (4 weeks compared with 12 weeks for the standard GIST group). Therefore, the time spent on each GIST-session is expanded to allow additional practice for the participants, discussion and interaction within the treatment session. When compared with standard GIST, the intervention is more intensive and extensive with a total of 44 contact/treatment hours over 4 weeks. Furthermore, informal group activities (eg, cooking or garden groups) are added to the participant’s weekly schedule (2 hours/week, total of 8 hours). In addition, the participants are encouraged to participate during social activities in the morning/evening offered at the hospital (eg, morning walks, quiz or ceramics) or initiated by the participants themselves (eg, shuffle-board or café/restaurant visits). The 4 weeks also include time for assessments preintervention and postintervention. The participants will have extended leave each weekend (3/4 days/week) to practise and to complete home assignments with their family members/friends.
Both GIST protocols have been adapted (eg, more structured workbooks) based on the pilot study.27 The family members who participated in the pilot study reported the need for a more thorough explanation of their role prior to treatment. Therefore, the close family member/friend attends the first inclusion assessment meeting. If a participant misses one session, the amount of repetition in GIST allows him/her to continue directly to the next session. However, if more than one session is missed consecutively, an individual session will be delivered. Both GIST protocols are manualised, ensuring the consistency in which the intervention content is delivered.
Sample size
Based on previous studies, the estimated annual incidence of adult TBI in Norway is 12 000,44 and approximately 15 000 for CVA.45 Therefore, the sample size of 60 is considered attainable in the context of the total eligible population. The small number of intervention studies on SCD represents a challenge in estimating the required sample size for this project to document moderate effects of GIST for the primary outcome measure (LCQ). A power analysis, based on the LCQ and prior research on the effect of GIST in ABI where moderate to large effect sizes were reported,21 26 46 indicates that a sample size of 30 participants in each group, with an expected effect size of d=0.65 provides a statistical power of 0.80.
Data analysis plan
Data analysis will follow the intention-to-treat principle. The long waiting period for the WL group may affect adherence and drop-out rates. However, all participants enrolled and randomly allocated to the two treatment groups will be included in the analyses.
Analyses will be performed using the Statistical Package for the Social Sciences V.25, with p<0.05 as the level of significance. Frequency distributions, means and SD will be calculated for the demographics, neuropsychological performance variables and questionnaires. Differences between groups will be analysed using t-tests for continuous variables, a regression analysis will be used for estimating the relationships among variables and χ2 will be used for dichotomous variables.
A general linear model with repeated-measures analysis of variance (ANOVA) will be used to examine group-related treatment effects.47 We are planning to run three analyses comparing: (1) standard GIST and intensive GIST: the between-subjects factor and time (baseline T1/T4), postintervention (T2/T5), 3-month follow-up (T3/T6) and 6-month follow-up (T4/T7)); (2) standard GIST and WL: the between-subjects factor and time (baseline (T1/T1), postintervention/WL (T2/T2), 3-month follow-up/WL (T3/T3) and 6-month follow-up/WL (T4/T4)) and (3) intensive GIST and WL: t-tests will be used to explore the within-subjects factors change of scores (baseline–postintervention (T4–T5), baseline–3-month follow-up (T4–T6), baseline–6-month follow-up (T4–T7)) and accordingly also for the WL ((T1–T2), (T1–T3), (T1–T4)). To adjust for multiple comparisons the Holm-Bonferroni procedure will be applied. The strength of experimental effects will be interpreted with effect-size statistics, including partial eta-squared (ƞ2) for ANOVA results and for t-tests. Partial ƞ2 allows us to compare the effect of variables in different studies. According to Cohen,48 thresholds for interpreting ƞ2 are <0.06 (small), 0.06–0.14 (medium) and >0.14 (large). A description of patient characteristics and baseline data will be compiled once all groups have completed the baseline assessment (T1), which is anticipated to occur during the autumn of 2019. The final analysis of the RCT will be conducted following the 6-month follow-up, which is anticipated to be completed during the autumn of 2020.
ETHICS AND DISSEMINATION
Data management and monitoring
Only data relevant to the study will be collected. Participants will be allocated a unique identification number prior to assessment. The collected data will be anonymised, marked with the participant’s number and confidentially stored. The coupling key will be stored separately from person-identifiable information on a secure server at the University of Oslo. Consent forms and documents containing personal information will be kept in a locked file in a locked office at the University of Oslo. This article presents the research protocol of this RCT. There is no data available at this point; however, the data will be made available as soon as the results are published.
Ethics and safety aspects
The study will be conducted in accordance with the Declaration of Helsinki. Furthermore, the methods employed for the study are not contrary to legislation, norms or values of Norwegian society. The trial will be reported in accordance with the CONSORT 2010 statement.
Dissemination and user involvement
Research findings from the study will be disseminated through peer-reviewed journals, national and international conferences and patient organisations.
Patient and public involvement
User involvement will be incorporated in all study phases. Members of the project group have conferred with previous ABI patients and user representatives; they have also executed a pilot study before commencing this RCT. Study design and choice of outcome measures have been informed by patients’ priorities and experience. However, the patients will not be involved in the recruitment or conduction of the study. User representatives will be involved in the remaining phases of the study, including the dissemination. Finally, the main findings will be made available to the participants at the end of the study along with an offer of receiving feedback regarding individual results.
DISCUSSION
The present study focuses on exploring the efficacy of GIST (standard and intensive) for people with SCD. Furthermore, limitations of previous studies will be addressed by a robust study design and method, adequate and broad outcome measures and long-term follow-up. As such, it is expected that the present study will contribute to more knowledge on the effects of standard GIST and intensive GIST in various ABI populations (ie, TBI, CVA, anoxic incidents and tumours). Also, the proposed study requires a substantial amount of involvement from family/friends which is expected to enhance study adherence and intervention gains. However, this requirement may also exclude potential participants without social network. In the present study, data regarding family/friend relation and cooperation during treatment is collected and evaluated. A general challenge for future studies is, however, to make social interventions more accessible to persons experiencing social isolation. There are some limitations that should be noted for the present study. The use of a WL design has been criticised for overestimating treatment effects.49 50 In our study, the WL-group will have contact with health personnel every 12th week during the waiting period (ie, assessment points) in addition to other possible treatment. However, a no-treatment comparison does not control for variables such as participants’ expectancy to improve or the therapeutic relationship.51 Furthermore, the use of broader outcome measures is considered a strength in SCD research, and thus applied in this protocol. Nevertheless, a large outcome battery may also be considered a participant burden due to time and fatigue. The use of self-report forms with good psychometric quality give valuable insight into how participants perceive their communication behaviour.46 However, there are limitation factors regarding the accuracy and validity of self-report such as participant awareness, demand characteristics, social desirability bias, acquiescent and/or extreme responding.52 53
Still, the proposed study is unique in the field of cognitive rehabilitation, as standard outpatient GIST will be compared with intensive inpatient GIST for the first time. Hence, the study is expected to have a direct impact on rehabilitation practice. If intensive GIST is proven acceptable and equally effective as standard GIST, the latter may facilitate access to treatment across municipal borders and geographical distances. Thereby, people with limited social networks may have the opportunity to work on their social communication skills in a social environment at the hospital. From a socioeconomic perspective, intensive inpatient training is more expensive than outpatient training; however, some research indicates that intensive treatment has significant effects for persons in the chronic phase after ABI.28 There may be drawbacks to completing an intensive outpatient GIST because completing three or more sessions per week may limit participants’ time to practice their social skills and homework between sessions. This has been addressed for inpatients by reinforcing opportunities for practice as the group receives full-day treatment and by living in an environment with exposure to different social settings and activities throughout the day and in the evenings. In future studies, we recommend exploring designs with stratification to ensure a higher degree of group homogeneity, in addition to larger sample sizes, and the inclusion of different ABI populations.
Supplemental material
Supplemental material
Acknowledgments
The authors thank the patient advisors, Anne Katherine Hvistendahl and Lena Hartelius for their contributions.
References
Footnotes
Contributors SMH is a doctoral fellow for the project and wrote the first draft of the present paper. Authors SMH, JS and MK planned the study, and authors SMH and MH will be conducting the interventions. All authors contributed to the final manuscript, including final approval of the version published.
Funding This study was funded by Department of Special Needs Education, University of Oslo, Norway and Sunnaas Rehabilitation Hospital, Norway.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study has been approved by the Norwegian Regional Committee South East for Medical and Health Research Ethics (2017/1360).
Provenance and peer review Not commissioned; externally peer reviewed.