Article Text

Abstract
Objective Musculoskeletal care pathways are variable and inconsistent. The aim of this systematic review was to evaluate the evidence for the clinical and/or cost effectiveness of current care pathways for adults with hip and/or knee pain referred for specialist opinion.
Design Systematic review.
Data sources Electronic database searches were carried out in MEDLINE, MEDLINE In-Process, Cumulative Index of Nursing and Allied Health Literature, Embase, PEDro, PubMed, Web of Science, Cochrane Central and Health Management Information Consortium without language restriction from 1990 onwards. Websites were reviewed for grey literature.
Eligibility criteria All study designs and documents that considered care pathways for adults with musculoskeletal hip and/or knee pain referred for specialist opinion were screened by two reviewers. Risk of bias was assessed using The Critical Appraisal Skills Programme checklist for randomised controlled trials and the Joanna Briggs Institute checklists.
Data extraction and synthesis Data extraction and quality assessment were performed by one reviewer and checked by a second. Findings are reported narratively.
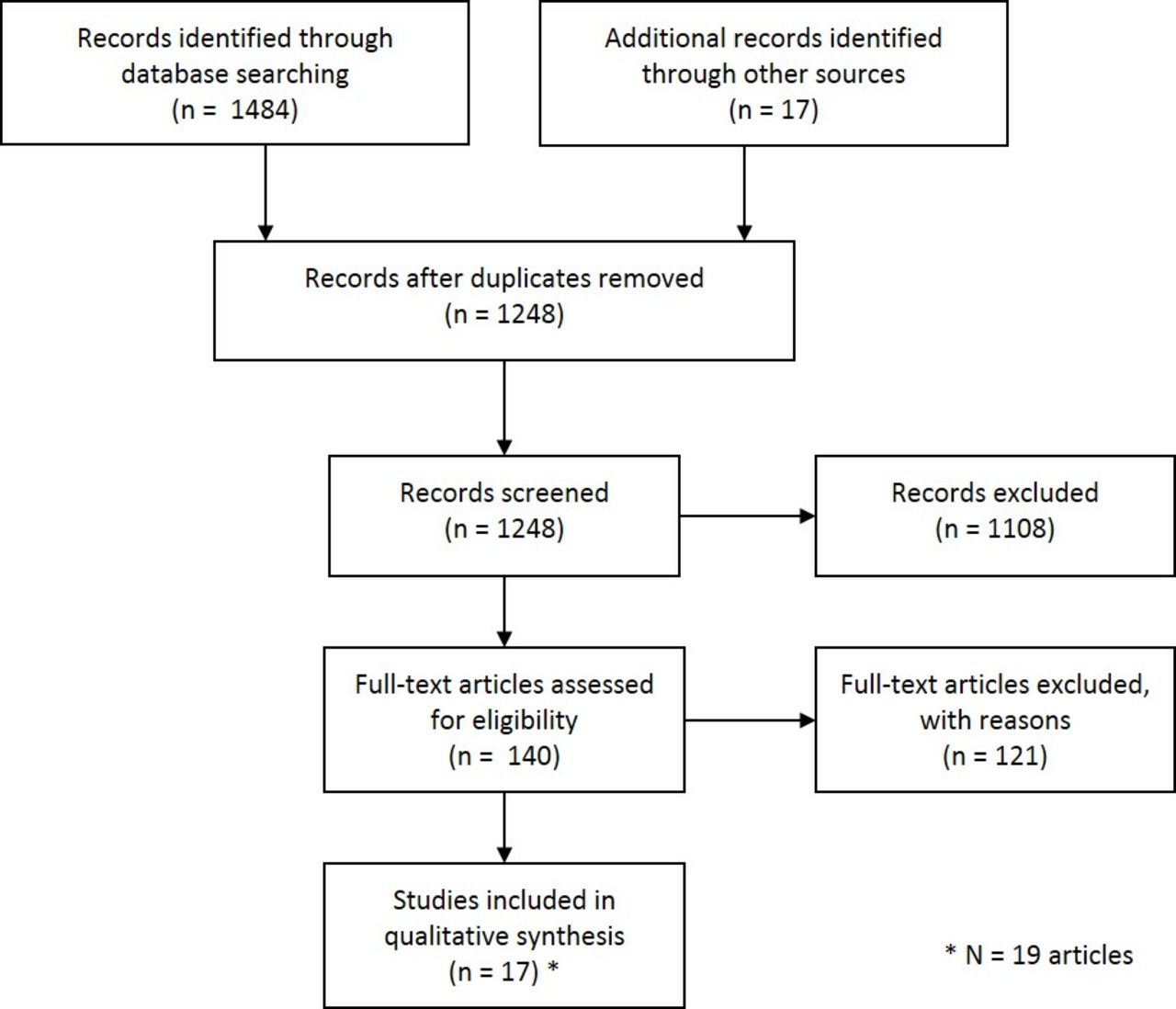
Results The titles and abstracts of 1248 articles were screened and 140 full-text articles retrieved. 19 papers reporting 17 studies met the study inclusion criteria. Quality was low due to study design and methodological flaws. Most of the outcomes relate to organisational process at the ‘meso’ level of a whole systems approach.
Conclusion It can be concluded that the pathway is not linear, containing variations and activity loops. The available evidence suggests that, from the point of referral for specialist opinion, a model is required that integrates the skills of all the different healthcare professionals and streamlining is required to ensure that individuals are seen by the healthcare professional that best meets their needs. There is very limited evidence of patient experience informing knee and hip care pathways.
PROSPERO registration number CRD42016035510.
- musculoskeletal
- hip pain
- knee pain
- care pathway
- service delivery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Designed and reported using Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Robust search strategy designed by the Specialist Unit for Review Evidence.
Two reviewers checked eligibility of manuscripts.
Two reviewers checked study quality.
Insufficient randomised control trials for a meta-analysis .
Introduction
The incidence of musculoskeletal pain is known to be high globally, and to be a significant factor in causing disability through reduced functioning and lower levels of general well-being. In 2016, musculoskeletal problems were the second most common cause of work-related absence in the UK, with an estimated 30.8 million days lost.1 The impact on concurrently existing long-term conditions, health resource utilisation and societal impacts such as work disability are considerable.2–4 Worldwide, musculoskeletal conditions account for 21.3% of the total years lived with disability within the general population,5 but this is even higher in older populations; reaching a high point of 28.5% in the 50–69-year-old age group and 23.4% in the 70-year plus age group.6 As a result, individuals may not be able to be physically active with a possible knock-on effect on the prevention and treatment of other non-communicable diseases.7
Hip and knee osteoarthritis (OA) is one of the most common musculoskeletal conditions and causes chronic joint pain after non-specific low back pain. It has a prevalence of 3.7% in the population, affecting approximately 268 million individuals worldwide. This increases to 14% in individuals over 65 years.6 8 A number of evidence-based guidelines exist detailing what treatment should be delivered. These centre on the delivery of self-management, education, exercise and joint replacement surgery when needed or at the end stage of OA.9–11
What is less frequently considered in both research and guidelines is the organisation of care: where it is carried out, how it is done and the complex inter-relationships between these factors and the type of treatment given. For example, the first point of contact for most individuals seeking help for a musculoskeletal condition is usually a general practitioner (GP) in a primary care setting.9 12–14 If treatment fails or assessment for surgery is required, then a ‘specialist’ opinion will be sought, which may occur in primary or secondary care.9 The ‘specialist’ could be from any one of several healthcare professionals: a physiotherapist, a GP with a specialist interest in musculoskeletal conditions, an advanced nurse practitioner or an orthopaedic surgeon.15 16 Understanding the variation and interrelationships between how and where treatment is delivered is required in order6 12 17 18 to optimise care around patient outcomes and efficiency in a multilevel whole systems approach.6 At a macro level, there needs to be consideration of the scope and functionality of healthcare policy, healthcare systems and socioeconomic factors. At a ‘meso’ level, considerations relate to health services, clinical workforce, competencies, education and infrastructure. Finally, at a ‘micro’ level, considerations relate to the involvement of an individual in their own care.6 Applying this to care pathway research helps to identify where the evidence already exists and enables more effective research planning.
This review will focus on the care pathway for chronic hip and knee pain for adults referred for specialist opinion. The joint-specific focus at this point in the care pathway recognises the rising demand for both care and joint replacement surgery in this group, which is associated rising healthcare costs.19 Thus, the following are the aims of this review:
to understand the evidence for the clinical and/or cost effectiveness of current care pathways for adults with chronic hip/knee pain patients accessing care for specialist opinion.
to identify the key information required to inform effective referral decisions for specialist opinion.
Methods
This systematic review is reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance.20 A protocol with full details of the methodology for this systematic review, including the search terms used has been published, so only a brief overview is provided here.21
Search strategy
Searches were undertaken without language restrictions for both published and grey literature that considered models of service delivery and care pathways. All sources were searched for evidence published between 1 January 1990 and 20 December 2017. The following databases were searched: Medline, Medline in Process, Cumulative Index of Nursing and Allied Health Literature, Embase, Pedro, PubMed, Web of Science, Cochrane Central Register of Controlled Trials and Health Management Information Consortium. In addition, websites were searched for grey literature, care pathways and policy documents. Finally, reference lists were checked and citations tracked for included evidence. Full details of the search, including the Medline search strategy are provided in the published protocol.21 Details of searches for other databases are available on request from the authors.
Eligibility
All study designs and documents that considered care pathways for musculoskeletal hip and/or knee pain for adults from the point of referral for specialist opinion meeting the European Pathway Association definition of a care pathway22 were included. No diagnostic criteria were specified as musculoskeletal pathways accept all hip/knee pain without such criteria. Publications were excluded if their primary focus was generalised inflammatory arthropathy, stroke, postsurgical care or musculoskeletal care pathways that did not include hip and knee joint-specific data.
Data selection
After duplicate results were removed, two reviewers (KB and Cheryl Cleary, FM) independently considered citations against inclusion/exclusion criteria. At both title/abstract and full-text stages, disagreement was resolved by discussion with a third reviewer.
Quality assessment
Studies were appraised using validated checklists for specific research designs: The Critical Appraisal Skills Programme checklist for randomised controlled trials (RCTs)23 and the Joanna Briggs Institute checklists for qualitative studies, cross-sectional surveys, longitudinal studies and case series.24 After a sample of studies had been piloted to ensure a baseline of understanding and agreement between reviewers, papers were assessed by one reviewer (KB) and checked by a second (FM).
Data extraction and synthesis
Data were extracted into a standardised form. After piloting, data extraction was completed by one reviewer (KB) and checked for accuracy by another (FM). The protocol21 specified the utilisation of a mixed-methods approach to data synthesis. However, only one qualitative study was identified. This combined with the low quality and heterogeneity of the evidence precluded any mixed-methods synthesis or meta-analysis. Consequently, the results are presented narratively by primary outcome type reported. These categories were identified inductively from the data: patient flow (the movement of patients between healthcare professionals, services and organisations),25 professional competency (the level of agreement in diagnosis and treatment between Advanced Physiotherapy Practitioners and orthopaedic surgeon or expert physicians), resource use including clinical and cost effectiveness, time (changes in patient waiting times experienced as a direct result of the way the pathway was delivered), patient satisfaction and patient experience. These outcomes are organised according to where they apply in a multilevel, whole systems approach, that is, macro, meso or micro level.6
Patient and public involvement
A patient representative was involved at the planning stages and helped to formulate the aims of this systematic review.
Results
Pathways for the delivery of care for hip and knee pain after referral for specialist opinion have not been widely researched. Although 1248 citations were identified, most of the primary research in this area has looked at generalised pathways for musculoskeletal conditions that are not specific to body regions. In most instances, findings were not disaggregated and therefore were excluded. Thus, of the 140 full-text articles assessed for eligibility, 121 were excluded and only 19 articles reporting the results of 17 studies were included in the analysis (see figure 1).

Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols flow chart for study selection.
All the included studies were from high income, developed countries: eight from the UK,16 26–32 five from Canada,33–37 two from New Zealand15 38 and one each from Australia39 and the Netherlands.40 There were some differences in the patient population being evaluated across the studies: seven studies included patients with a knee condition only,26 27 30–33 37 two studies with a hip condition only16 29 and eight studies had patients with hip or knee pain.15 28 34–36 38–40 Specific characteristics of each study are described in table 1.
Characteristics of included studies
Thirteen of the studies were based on healthcare activity in hospitals within secondary care,27–39 with consultation led by a physiotherapist in three studies,15 30 34 physiotherapist and orthopaedic surgeon/expert physician in seven,27 28 31 33 35 37 39 orthopaedic surgeon-led in two29 38 and GP led care in the remaining studies.16 26 32 40 Only three studies had a clinic that was located in primary care.32 35 38 Each of these also had a subset of patients that were assessed in a hospital-based secondary care clinic. These studies were not set up to allow comparison between the primary and secondary care clinics.
The study designs of the articles in the analysis included: one RCT,26 41 42 four cohort studies,16 28 38 40 one qualitative interview study,32 one case report,39 five cross-sectional designs,15 27 33 35 36 two case series,29 34 one prospective diagnostic study37 and two audits.30 31 Using the hierarchy of evidence proposed by the Oxford Centre for Research Evidence,43 the overall level of evidence from the included studies is low. The limitations of the studies included in this systematic review are described in table 2. The most common weaknesses in the study designs related to incomplete reporting of the outcomes for cost and resources use16 34 and clinical outcomes16 30 31; low external validity and generalisability due to sample size,33 population studied36 38 or number of assessors28 37; insufficient length of follow-up34 35; reporting bias29 32 34 36 38 39; selection bias due to sampling.16 27 34 Overall, the RCT was reasonably well designed, but there was no blinding and allocation to group was not concealed.26 41 42
Key findings from the reviewed papers
The outcome types and study-specific outcomes are described in table 2 along with the numerical data reported. Variations in care pathways in terms of where and who delivers the different pathways are displayed in figure 2 along with the types of outcome that have been evaluated in each study and the study reference. If there were two arms to the pathway, then the associated outcome types are aligned between the arms.

{kind=link}
{kind=link}
Care pathway and outcome types evaluated in the included studies. APP, advanced physiotherapy practitioner; MCAS, multidisciplinary team assessment clinic.
Meso level: patient flow
Johnson et al 29 evaluated an orthopaedic-led fast-tracking pathway for hip replacement. Physiotherapists assessed patients on the orthopaedic waiting list that an orthopaedic surgeon had screened off for physiotherapist management. The fast-track pathway resulted in 23/25 patients being given a total hip replacement, but a further 15 patients from the routine route were also listed for joint replacement surgery.
A study by Pearse et al 30 benchmarked the ability of advanced practice physiotherapists to independently assess 85% of patients on an orthopaedic waiting list, following strict criteria set out by a surgeon. Fifty patients with knee pain had been screened by a surgeon and deemed appropriate for physiotherapy assessment and non-surgical management. Physiotherapists failed to meet the benchmark; only independently assessing 66% of patients. Of the patients they were not able to manage, 17 (34%) were referred to a consultant, with only 11 being listed for surgery. The authors concluded that physiotherapists did not efficiently manage patients on the orthopaedic waiting list. However, the benchmark set was not underpinned by research.
The Damask Study Group26 41 42 conducted a RCT to assess the effectiveness and cost effectiveness of GP referral to MRI and provisional orthopaedic appointment, compared with referral to an orthopaedic specialist only, for knee problems. The study found that having an MRI did not change the diagnosis or the treatment plan, but there was greater treatment and diagnostic confidence among GPs in the MRI group. Patients in this group also reported a statistically significant improvement in their physical functioning and quality of life.
Gwynne-Jones et al 15 evaluated the effectiveness of a prioritisation service for assessment of hip and knee OA. A physiotherapist and a nurse assessed patients referred into a joint clinic and surgeons only assessed those identified at referral as requiring specialist opinion, or who were subsequently rereferred from the joint clinic. Of the 339 patients included, 54 were referred directly to the surgeon and a further 89 were referred after the initial assessment. Of the 143 referred to the specialist clinic, 115 were listed for or underwent surgery. The authors concluded that this service freed up valuable surgeon time.
Only one study by Inglis et al 38 reported outcomes that can be applied at a macro level within a complex multilevel system. This evaluated the effectiveness of consultant-led triage of referrals for patients requiring a fast-track specialist surgical opinion. Of the patients referred, 57% of those with hip pain and 46% of those with knee pain were assessed or directly listed. Others were sent elsewhere because of insufficient clinic capacity, or they were deemed lower prioritisation based on referral information, or their referral was incomplete.
Meso level: professional competency
Overall, agreement in diagnosis between the professional groups was reported to be high for three studies, with kappa values ranging from 0.80 to 89 agreement,33 35 37 where 1.0 represents perfect agreement. The study by MacKay et al 36 reported agreement between physiotherapists and orthopaedic surgeons in 69% of cases. Compared with arthroscopy, physiotherapists were found to identify the correct diagnosis in 80%–84% of cases.27 Agreement on treatment type (surgical vs non-surgical) between physiotherapists and physicians was found to be 77% in one study35 and Decary et al 37 reported a kappa value of 0.73.
Macro level: resource use
The implementation of a stepped care pathway in primary care was described by Smink et al.40 The pathway resulted in the increased use of non-surgical treatments for hip and knee OA over 2 years. Dietary interventions were less well used. Of the patients 21% were referred for orthopaedic opinion in the first 6 months and at 2 years, this had risen to 45%.
Meso level: resource use
A number of studies described the resources used at the point of referral for a specialist opinion but there were differences in the type or structure of the pathway being reported on.
Farrar et al 28 evaluated a multidisciplinary team assessment clinic (MCAS), compared with direct referral to an orthopaedic service. Referral to the MCAS clinic resulted in more appointments before a working diagnosis was achieved compared with the orthopaedic route (p<0.001). However, there was a greater use of non-surgical treatments and lower surgical referrals in the MCAS service (16% vs 36%; p<0.001).
In a study by Rabey et al, 31 9% of new referrals seen by an Advanced Physiotherapy Practitioner were referred for surgical opinion. Of these, 42% were for knee conditions. Of the patients referred with knee conditions, 84% went on to have surgery.
Only one study16 described a potential cost saving by using advanced physiotherapy practitioners to directly list patients for total hip replacement surgery rather than going via an orthopaedic clinic. This saving was calculated to be £145 per patient. MacKay et al 36 found that for ongoing treatment in a clinic, physiotherapists were more likely to give exercise and education at the time of consultation while a surgeon was more likely to refer to rehabilitation services (which would include exercise and education), adding a further step and potential delay in the patient receiving the correct care.
Desmeules et al 35 did not find any difference in the referral rates for imaging between orthopaedic surgeons and Advanced Practitioners. Conversely, an MCAS service was reported to result in a greater use of imaging (p=0.04).28 In terms of numbers of imaging referrals made by Advanced Physiotherapy Practitioners, Rabey et al 31 reported that 36% were referred for a knee X-ray and 23% for an MRI.
Meso level: time
Physiotherapy-led triage resulted in a reduced wait for surgery from 140 to 40 days.34 Using physiotherapists to directly list patients for total hip replacement, rather than going via an orthopaedic appointment resulted in a shorter wait for surgery (21.4 weeks vs 24.7 weeks).16 Conversely an MCAS service resulted in a longer waiting time from referral to diagnosis (p=0.05).28 Doerr et al 39 described a new referral process and found a reduced patient wait for an initial specialist appointment but the time is not specified. Desmeules et al 35 found that advanced physiotherapist practitioners had longer consultation times than orthopaedic surgeons.
Micro level: patient satisfaction and patient experience
Two studies34 35 evaluated patient satisfaction using questionnaires. Both found a high level of satisfaction with the physiotherapy triage. One35 reported greater patient satisfaction with the care by the physiotherapists than the surgeon and the other34 reported that no patients requested a subsequent appointment with the orthopaedic surgeon.
Only one interview study evaluated patient experience.32 This related to being on a waiting list for specialist diagnosis and surgery. Four themes were identified; inadequate information, the social and psychosocial cost of waiting, coping strategies and the varying effectiveness and support provided by clinicians. The recommendation was to improve information provision to improve patient well-being.
Discussion
This review first aimed to understand the evidence for the effectiveness of current care pathways for adults with chronic hip/knee pain patients accessing care for specialist opinion. The second aim was to identify the key information required to inform effective referral decisions for a ‘specialist’ assessment.
The complexity and variation of the patient pathway from primary care referral to receiving a specialist opinion is clearly highlighted. Subtle variances were found in the pathway, such as different referral prioritisation,15 38 41 fast-tracking systems,29 different models of care40 and a varying role for different professional groups.16 27 28 31 35–37 Also, despite musculoskeletal conditions being a rising global health concern,8 all the research identified was conducted in high-income countries, limiting the generalisability of the findings.
Only a limited number of studies were eligible to be included as most studies did not disaggregate their findings to report hip-specific and knee-specific data. More joint-specific research is therefore required, as when an individual is referred for a specialist opinion, this is the point in the care pathway where an individual is moving from generalist to a specialist approach. Only one RCT was identified that evaluated the effectiveness of referral pathways for specialist opinion, which means there is insufficient evidence to draw solid conclusions on the effectiveness of current care pathways or the key information required to inform effective referral decisions. However, the findings demonstrate complexity in the care pathway around referral for a specialist opinion and are informative about pathway and organisational processes. Discussion of the findings around a multilevel whole systems approach assists with understanding where the evidence is located and what research needs to happen next.
Macro level
The findings from only one study were relevant at the level of healthcare systems and policy. Smink et al,40 described healthcare utilisation after the implementation of a stepped care strategy in the treatment of hip and knee OA. The authors reported that the pathway resulted in a higher percentage of patients being managed with non-surgical treatment before referral for specialist opinion, but that referral to a dietician for weight management was underutilised. However, the usefulness of this research is limited by the lack of baseline data to compare healthcare utilisation premodel and postmodel implementation. The acceptability of this model to GPs and patients also needs to be questioned. While 157 GPs were recruited from eight practices, healthcare utilisation data were only available for 313 patients. Two patients per GP is a very low number considering how many individuals present with joint pain. Second, patient experience of the pathway does not appear to have been considered. Further research on the effectiveness of the pathway for GPs and patients, along with greater integration of dietician referrals should provide additional answers.
Meso level
Most of the studies included in this systematic review looked at patient flow (fast-track models, referral prioritisation and advanced practice triage) and resource use. The findings suggest that advanced practice physiotherapists are comparable to orthopaedic surgeons in their diagnosis of knee and hip pain27 33–37 and triage to surgical or non-surgical treatment. This would suggest that physiotherapists have the skills required to triage patients referred for a specialist opinion about their hip or knee pain.
Despite this finding, there appears to be less consistency in treatment allocation and healthcare resource use when applied in practice across different care pathways. This may be due to differences in staff skill mix, triaging processes and patient referrals. For example, in one study higher conversion rates to surgery are reported from an orthopaedic clinic, while advanced physiotherapy practitioners have higher referral rates to non-surgical treatment options.28 In addition, practice within orthopaedic clinics can vary with physiotherapists providing more exercise and advice and surgeons having higher referral rates to rehabilitation services.36 Surprisingly, considering the importance of weight management in the treatment of joint pain and OA, no studies have specifically evaluated referral rates to dietician services by these different professional groups.9 44 45
In terms of imaging referrals (X-ray and MRI), there is inconsistency in the referral rates across different clinics or professional groups.28 35 A RCT evaluating the clinical and cost effectiveness of GP referral for specialist opinion26 41 42 found that clinicians had more diagnostic and treatment confidence when referring for an MRI and that patients on this pathway had a better level of functioning. The concern about the study is that it only considered GPs as the primary referrers. It also failed to take into consideration other treatments recommended within the primary care pathway.9
From the evidence, it is clear that, regardless of nuances in the care pathways considered, there will be a proportion of patients assessed in a physiotherapy clinic who will require a surgical opinion and also patients referred to an orthopaedic clinic who will require conservative management.15 16 30 38 This occurred despite triaging and referral systems implemented to fast track or direct patients to the most appropriate service.15 29 38 Additionally, both the fast-tracking criteria29 and surgeon screening of referrals,30 seem to lack sensitivity and specificity as individuals move between surgical and conservative pathways. The quality of the research means that insufficient evidence exists regarding predictor variables to identify the key variables to inform specialist referral. Thus, the current evidence suggests that an innovative workforce model is required that integrates the skills of the different professionals to meet individual patient needs and tackle these complexities. This would give patients access to clinicians with expert knowledge of both conservative and surgical treatments at the same locality. In addition, better streamlining is required so that only those individuals requiring specialist opinion are referred. Taken together, this may help avoid delays in care, interruptions of patient flow and suboptimal use of resources.25 46
Several studies found pathway steps that reduced waiting times from referral to diagnosis and the number of surgeries.16 28 34 39 Unfortunately, they did not evaluate the cost, sustainability or resource implications of these steps. No studies evaluated the demand for the care pathway and the capacity available or needed to meet this demand and achieve target waiting times. Thus, no conclusions can be drawn about the potential cost–benefit or effectiveness of care, regardless of the pathway.
The majority of the available evidence is based on outcomes around professional competency for clinics containing a mixture of professional groups. A better understanding of the roles, learning, communication and expertise within this clinic structure is required, along with a robust assessment of pathway effectiveness. Although physiotherapists have been found to have high diagnostic accuracy, the complexities and diversity of the pathways presented means that future decisions on pathway design are unlikely to be as simple as replacing a surgeon with a physiotherapist.
Micro level
Measuring patient experience and using this to inform care is a key component of healthcare quality.47 Only two papers were identified that considered patient satisfaction34 35 and methodological flaws make it difficult to draw meaningful conclusions. There is limited research evidence on patient expectation and experience of hip and knee pain pathways as only one qualitative study was identified.32 The study recommended the development of a pathway with better information provision. This is an important consideration given the potential complexities and variations in care pathways that patients may experience and needs to be addressed in future studies. None of the studies evaluated differences in experience according to the location of the specialist clinic. This is a key area for patient involvement for future pathway design research.
There are some limitations of the review. First, our search for qualitative studies should also have included patient needs regarding the pathway. Second, our interpretation of clinical and cost effectiveness has been limited by a lack of randomised control trials in this area.
Conclusion
The evidence base as exists is fragmentary and of low methodological quality. While several pathways have been developed and implemented,13 48 the evidence base underpinning them is limited. Only one RCT was identified, so there is insufficient evidence of the clinical and cost effectiveness of the care pathway for individuals accessing care for specialist opinion. What is clear is that the pathway is not linear: there are variations and potential activity loops. Most of the studies report organisational process outcomes, at the ‘meso’ level of a multisystems model, which focus on the skills and treatment decisions of the different professions. Based on the evidence presented, it is suggested that when an individual is referred for a specialist opinion, a pathway which integrates the skills of all the different professions is required. Additionally, individuals need to be referred to the professional who is most likely to be able to help them address their joint-related problems, for example, a physiotherapist or specialist GP for non-surgical treatment. No key predictor variables were identified in the literature to inform when an individual should be referred for specialist opinion. There is an urgent need for further research that is designed with the involvement of patients to develop and determine effective and cost-effective pathway(s).
Acknowledgments
Cheryl Cleary (CC) for her work reviewing abstracts and titles.
References
Footnotes
Twitter @k8button
Contributors KB is the guarantor. KB, FM, ALW and SJ designed the protocol. ALW conducted the searches. KB and FM selected studies, undertook data extraction and critical appraisal. KB, FM and SJ were responsible for writing this publication. All authors read and approved the final manuscript.
Funding This work was funded by Health and Care Research Wales, Research for patient and public benefit, grant number 1114.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The findings of the search strategy are available to any readers if they contact the corresponding author by email.
Patient consent for publication Not required.