Article Text

Abstract
Introduction After a stroke, 55% of survivors do not regain the ability to completely use their arm in daily life functioning. Currently, evidence-based guidelines recommend functional training for improving the affected hand after stroke. However, promoting an optimal quantity and quality of functional training is influenced by personal and environmental contextual factors. Studies that comprehensively target multiple factors regulating arm use are limited. This study compares the effects of functional training to multifactorial context-enhancing functional training program for improving functional arm use and recovery after stroke.
Methods and analysis This is a protocol for an observer-blinded, two parallel groups, randomised controlled trial. A total of 126 community-dwelling subacute and chronic stroke survivors will be included in the study. A tailor-made multifactorial context-enhancing intervention-incorporating education, environmental enrichment and behaviour change techniques to reinforce functional training will be provided to the experimental group. The functional training group will be provided with functional exercises. The intervention will be delivered for 2 months. The primary outcomes of functional arm use and recovery will be measured using Motor Activity Log, Goal Attainment Scale and Rating of Everyday Arm-use in the Community and Home scale. The secondary outcomes of arm motor impairment and function will be measured using Fugl-Meyer upper limb score, Action Research Arm Test, ABILHAND questionnaire and Stroke Impact Scale. These will be measured at three points in time: before, after 2 months and after 1-month follow-up. The outcome measures will be analysed using one-way analysis of variance and regression analysis will be performed to identify factors limiting optimal task practice.
Ethics and dissemination The study has been approved by the Institutional Ethics Committee of Kasturba Hospital, Manipal, India. Participants will sign a written informed consent prior to participation. The results will be published on completion of the trial and communicated to community-dwelling stroke survivors.
Trial registration number CTRI/2017/10/010108
- stroke
- rehabilitation medicine
- adult neurology
- protocol
- upper extremity
- behaviour change
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This protocol tests a multifactorial intervention to facilitate behaviour change in arm-use level of stroke survivors.
The experimental intervention is tailored to address contextual barriers preventing arm use of each participant.
The experimental group will be compared against functional exercises.
Study will provide insight on factors limiting arm use and recovery after stroke.
Social influences on arm use are not addressed in this study.
Introduction
Stroke affects a large proportion of people living in developing countries.1 In developing countries, they lose 12 083 000 disability-adjusted life years due to stroke.2 Many stroke survivors remain dependent for performing daily life activities even years after the event. Recovery of functional arm use after stroke is a major contributor to regaining independence in performing functional activities.3 Yet, 55%–75% of survivors do not regain functional ability of their arm after stroke and one-third do not use their affected arm for accomplishing day-to-day activities despite regaining functional ability.4–6
To regain functional ability of the paretic arm, stroke rehabilitation guidelines recommend optimal quality and quantity of functional task practice to be sustained for a few months.7 8 To gain substantial improvements, the patient must actively engage in the practice of salient tasks at a challenging intensity. Each task so practiced has to be repeated numerous times per day, progressed gradually until a cumulative dose of 2000–3000 repetitions are achieved.9 10 However, the amount of practice provided within and outside rehabilitation is far less than the requirement.11 Further, implementing these recommendations in developing countries is even more challenging.
During the treatment session, a majority of time is spent on leg exercises and preparatory activities. Furthermore, many participants living in semi-urban and rural regions do not have continued access to active rehabilitation programmes.12 In lieu of such limitations, given the inadequacy of suboptimal quantity of exercises to produce functional gains, promoting self-driven practice becomes essential to bring about recovery. However, undertaking such practice is challenging for the patients and their caregivers.13
Many contextual factors unique to individuals influence physical activity in stroke survivors.14 Perceived need to engage in a high amount of practice15; awareness, understanding and procedural knowledge of right exercises16; opportunity to practice desired tasks with limited functional abilities17 and motivation to sustain such practice can all limit attaining threshold practice levels among survivors.18
Physiotherapy interventions implementing task-oriented training have attempted overcoming some of these challenges.19 However, despite delivering a high amount of practice and providing motivational support, they have not targeted specific contextual barriers to promote task practice and its sustenance. Many studies enforce task practice in the clinic or home and have found that the benefits do carry over; however, degree of uptake of self-driven practice beyond the study period is unknown.20 21
Hence, the primary objective of this study is to compare a functional task training programme with a tailor-made multifactorial context-enhancing functional task practice promotion programme among subacute and chronic stroke survivors living in semi-urban and rural regions.
The multifactorial contexts include factors that act as barriers to the amount of arm use. These can be personal factors, such as awareness, physical capability and motivation, or environmental contextual factors, which include the physical objects that commonly are used by stroke survivors and their family members support to promote arm use. Context enhancement refers to planned changes made to each of the four above-mentioned domains.
We intend to attain this by using behaviour change techniques (BCTs) to optimise the behaviour of interest. In this study, we intend to optimise the amount of use of the paretic arm of the stroke survivors for functional task practice and deliberate use during the performance of daily functions. BCTs are strategies used to help an individual to change their behaviour to promote better health. They contain a group of different techniques, such as sensitising the individual to health risks of not performing the behaviour, setting goals and providing action plans, environmental restructuring to facilitate the behaviour and so on, to promote the behaviour of interest.
We will assess and intervene personal and environmental barriers preventing uptake of functional task practice, such as physical barriers, lack of knowledge and motivational limitations, to enhance optimal functional task practice behaviour.
The secondary objective will be to compare gains in arm function and quality of life between the two interventions. Information gained from this programme could help us to identify behavioural support methods for designing efficient yet cost-effective intervention delivery models.
Methods
Research design
The study is a two parallel-group, outcome measurer blinded, exploratory randomised controlled trial with 1:1 allocation ratio.
Population and setting
The study will be conducted among subacute and chronic stroke survivors living in rural andurban regions of Udupi and Bangalore, India. The intervention will be provided in the patient’s home. Community-dwelling participants who meet the selection criteria (table 1) will be identified and contacted by phone from hospital records and directly from the community by the primary researcher. On obtaining permission, the primary investigator will visit and explain about the study. If they agree, they will be screened for eligibility. This will be done every week to identify participants and the participants will be contacted 10 days after discharge.
Selection criteria
Sampling procedure and group allocation
Sample size calculation
The sample size for the intervention study was calculated based on Cohen’s d effect size with mean 1.37 and SD 1.17 on Motor Activity Log (MAL) between the two groups based on a previous study of similar characters.22 To achieve 80% power for the Kruskal-Wallis test at 5% level of significance, the required sample size is 63 per group. This also accommodated the sample size for a 1-point change in Rating of Everyday Arm-use in the Community and Home (REACH) score.
Random group allocation
Participants will be randomly assigned to experimental and control groups. Block randomisation with variable block sizes of 8–12 will be done using Random Allocation Software, which uses computer-generated random numbers. An independent staff will generate the randomisation sequence and maintain randomisation sequence in sealed opaque envelopes and will communicate to the therapist delivering intervention after obtaining the informed consent on evaluation of selection criteria and collection of pre-test baseline data.
Procedure
Signed written informed consent will be obtained from each participant by the study therapist responsible for delivering intervention. Participant’s safety will be upheld during the intervention delivery and any adverse events will be immediately reported to the ethics committee and further follow-up action will be initiated. On completion of the trial, each participant will be provided instructions on how to further maximise their recovery. If treatment is required, they will be guided to the nearest physiotherapy centre. All data will be monitored by an institutional review board that works independent of the study team.
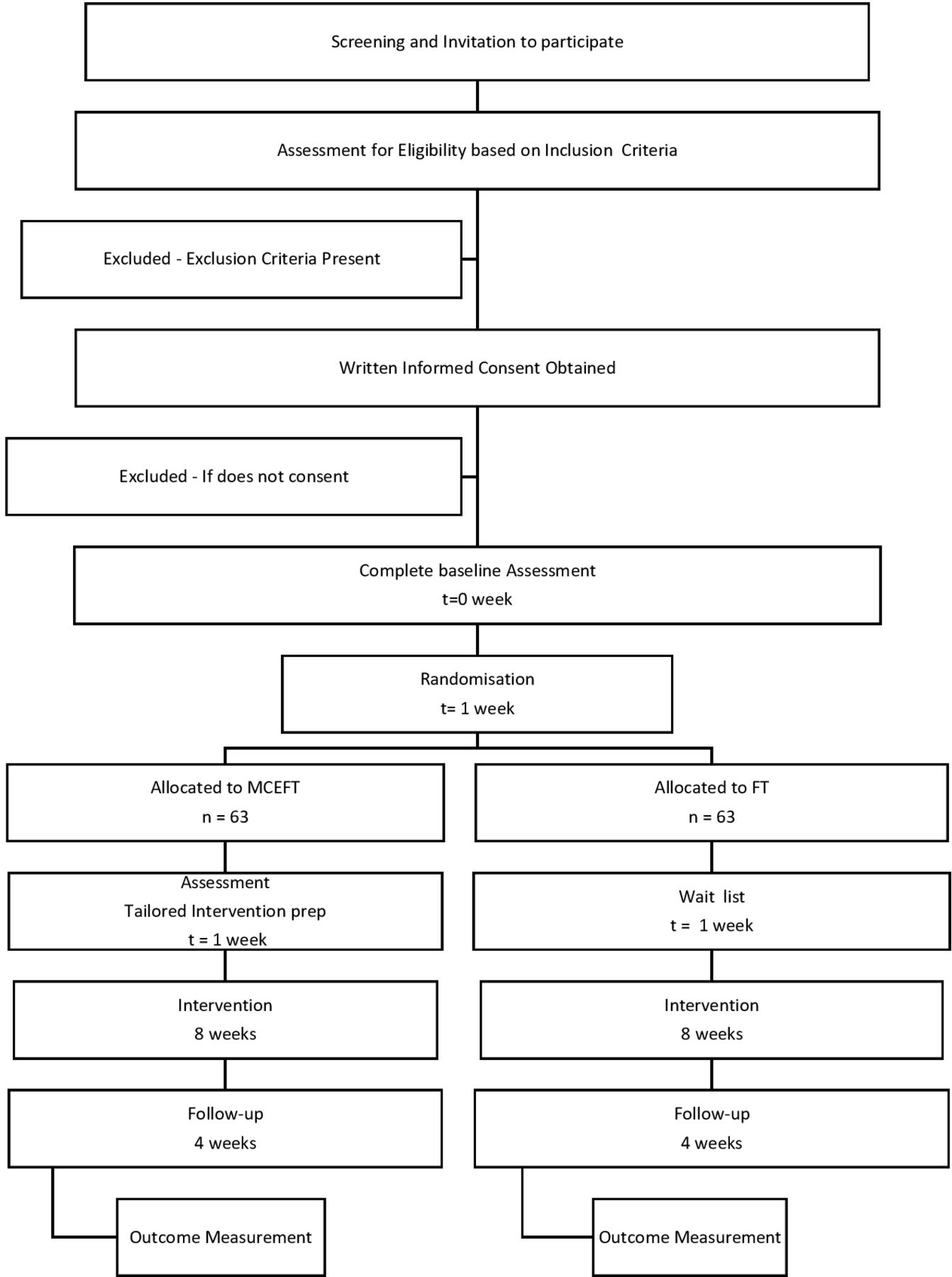
The CONSORT flow diagram (figure 1) provides the flow of participants within the study. The primary target of the intervention will be to attain and sustain optimal levels of functional task practice with affected arm (table 2).8 23 The trial team was responsible for monitoring and implementation of the trial (table 3). The schedule of the implementation of various steps of the trial is provided in the participant timeline (table 4).
Target behavioural criterion for optimal levels of functional task practice to promote arm use
MCEFT clinical trial committee
Participant timeline

CONSORT flow diagram. FT, functional therapy; MCEFT, multifactorial context-enhancing FT.
Control group (functional therapy programme)
A research therapist will instruct and train the patient to practice their preferred functional activities based on exercise principles outlined and found effective in clinical trials.23–25 An active comparator was chosen based on current best evidence recommendation. They would be prompted to select activities that are most important but unable to complete using the affected upper extremity.
We will videotape the activity performed in the home to select tasks and task parameters to be improved during training. Each week, the therapist will set the goals for the patient’s to achieve. Exercises will be progressed if active functional task practice is performed at the challenging intensity and optimal practice quantity. Task selection and training for a sample programme to improve eating activity are described in table 5A,B.
Task and progression parameter selection for functional therapy group
Functional task specific training programme
The participants will be instructed to practice each selected tasks for 5 days in a week. A therapist with knowledge on functional task training will visit the patient two times in a week to provide training, monitor their functional task practice and provide feedback on improvement. General educational sessions on stroke prevention will be provided and each participant will be taught about the benefit of exercise and encouraged to practice as much as possible.
Experimental group (multifactiorial context-enhancing functional therapy programme)
We identified factors mediating physical activity in stroke survivors through a qualitative interview and literature review. After ascertaining the nature of the contextual barriers, we enlisted evidence recommended BCTs that can address those modifiable mediators.26–28 Next, we used multiple theoretical constructs of action-based behaviour change theories alongside motor learning exercise principles that promote neuroplasticity for designing the intervention along with its overall delivery model23 (table 6).
Theory incorporation in MCEFT intervention
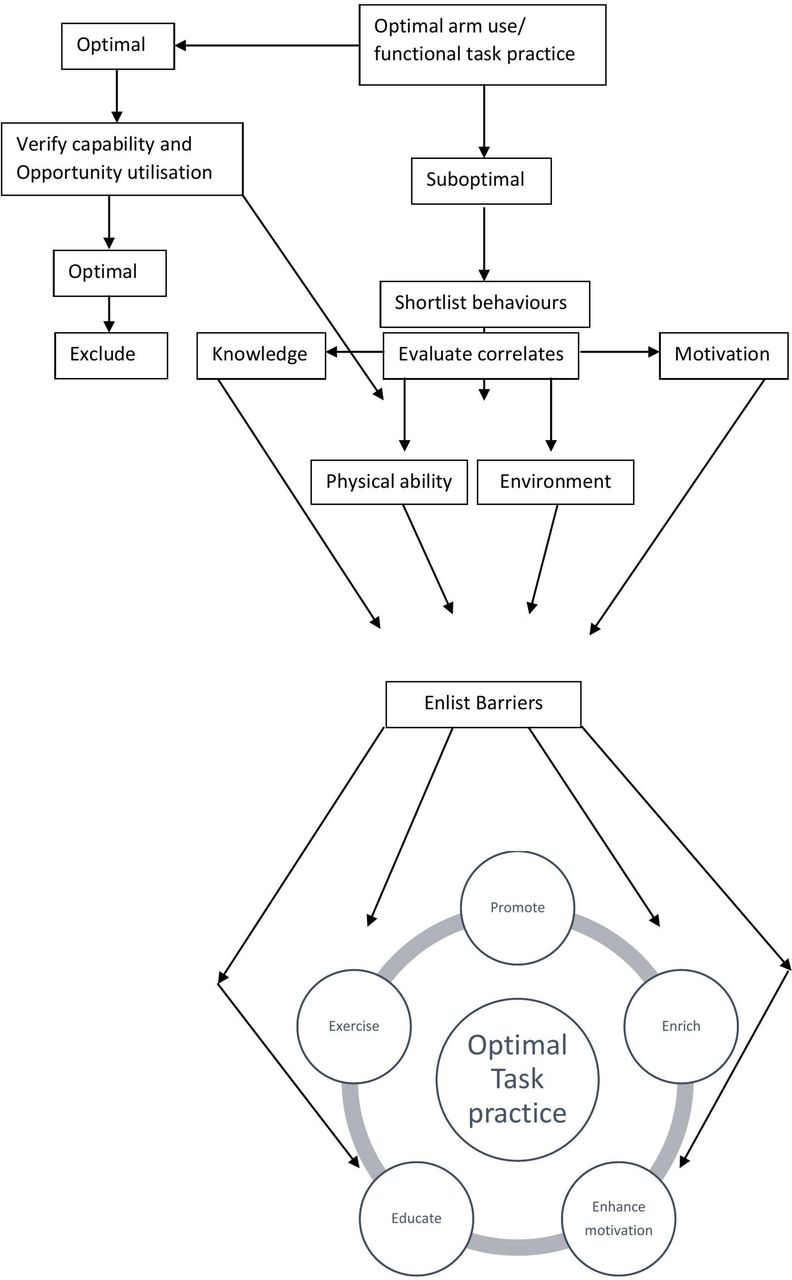
The overall intervention delivery model is depicted in figure 2. In brief, this intervention is a two-staged tailored intervention programme. Participant-perceived and therapist-observable contextual barriers will be separately identified for initiation and sustenance of arm use during functional tasks. On identifying the barriers, we will intervene using BCTs elaborated in multifactorial context-enhancing functional therapy intervention manual specifically designed for promoting upper extremity functional task practice in stroke survivors based on a behaviour change wheel approach.29

{kind=link}
{kind=link}
MCEFT intervention delivery model. MCEFT, multifactorial context-enhancing functional therapy.
The intervention manual provides a decision algorithm for choice of BCT to address each contextual barrier and details the procedure to be followed for implementation of each technique. One psychologist with experience in behaviour change and two physiotherapists verified the face validity of the intervention manual. The manual will be published online on completion of the last data collection point to prevent possible contamination in participants who might gain access to the manual.
We will evaluate deficiencies in participants’ knowledge through an open-ended questionnaire. The questionnaire consists of 20 open-ended questions addressing four domains of knowledge, namely rationale for affection of the arm, interventions undertaken to improve arm, procedural knowledge about exercises and knowledge of functional recovery potential. The domains and the underlying questions were based on qualitative findings and theoretical domains framework constructs that influence behaviour.
We will then screen the individual constructs of theoretical domains that prevent arm use using the determinants of a physical activity questionnaire (DPAQ). The DPAQ identifies 14 self-perceived theoretical domain determinants that encompass awareness, physical and psychological capability, physical and social opportunity, and reflective and automatic motivation.30 We will then ascertain actual physical opportunity to perform the desired functional task by video-recording their performance of the selected tasks in their home environment.
The experimental group participants will, based on their needs, undergo a specific set of behaviour change interventions designed to train the patients to initiate and sustain functional task practice. This set of interventions, depending on the need, may include the following. Educational sessions on what entails optimal practice and the need for such practice for people who are unaware. Providing objects matched to their abilities for people who are having limited capabilities to use existing objects in their home and training them on how to perform and providing feedback on their optimal performance. Once they understand and initiate task practice, they will be attempting to reach the optimal practice amount. Followed by this, we will ask them their perceived barriers to sustain such practices. Behavioural goals to sustain practice will be prepared along with the participants and their practice will be reinforced by appropriate BCTs as presented in table 7.
Behaviour change techniques for MCEFT group
Where caregivers are available, they will be trained to monitor the activity performed by the stroke survivors. They would be asked to provide procedural and practical support for functional task practice in the home. This will be verified by the treating therapist.
Patient and public involvement
This protocol was developed after completion of a qualitative study that helped in identifying the reasons for non-use of arm of stroke survivors. This qualitative study helped to identify limitations to real-life translation of physical therapy directed to improve arm function of stroke survivors.31 Once limited arm use was established as problem behaviour by the investigators, we identified the contextual barriers and their underlying reasons from an extensive literature review. Additionally, a systematic review of the effect of prior BCTs was undertaken to evaluate their efficacy. The systematic review has been registered in PROSPERO (CRD42015025713). Next, we piloted the protocol on a set of five stroke survivors for establishing the patient’s perspective of the intervention and feasibility of its delivery. Based on the participant’s ability to uptake the intervention, the delivery schedule and the dose of the interventions were modified.
Intervention delivery
The experimental group will be encouraged to self-sustain optimal functional task practice until they attain functional ability in the desired task. The functional task practice content will be similar to the control group. However, the method of intervention delivery will be integrated with behavioural support techniques to facilitate contextual enhancement.
We will educate, train and enable using predetermined BCTs on how to use the arm during their preferred daily activities or practice within their ability to promote initiation of optimal practice. They will be trained for 1 month. Next, we will use intervention modes, such as training, persuasion, enablement and/or incentivisation, to promote sustenance of arm use during a further period in the second month. The overall model of BCT intervention is shown in figure 2. The components will be specific to each individual’s contextual barrier. The specific behaviour change components for each intervention function incorporated in the programme for behavioural initiation and sustenance are provided in table 7.
The intervention will be delivered by a therapist with over 10 years of experience who has undergone training in delivering the behavioural support intervention enlisted in the manual. Each individual component BCT will range from 1 to 3 sessions, with a maximum of 12 sessions during the first month and 10 sessions in the following month.
Fidelity monitoring
Treatment will be delivered according to a pre-validated treatment manual. The content and dose of overall intervention components delivered will be documented using a checklist based on the intervention manual selected for each participant. A total cut-off of >70% adherence to enlisted content will be an acceptable fidelity in the delivery of the intervention. This will be monitored by the project supervisor weekly using a modified fidelity monitoring checklist.32
Participant’s uptake and enactment of the intervention will be documented. For the experimental group, education component will be evaluated using a knowledge scoring sheet. Physical enrichment will be documented by their use of the enriched object or environment during practice in over 50% of the post-enrichment session and documented as present or absent from participant’s self-report. Skill training component will be evaluated by analysing the recorded video of the task trained. All the three components will be documented at the end of the first month. Enablement components, such as behavioural goal setting and action planning, will be documented by their adherence to plans and goals at two equally spaced time points after delivery of the intervention. The quantity of practice will be documented by a weekly activity log.
For the control group, a weekly record of their exercise performance will be documented. Co-interventions to the planned intervention will be documented by the therapist providing intervention. The participants will not be prevented from taking any other intervention during the trial period. However, these will be documented and analysed for the dose of arm use. We used the SPIRIT checklist to guide the writing of this protocol.33
Pre-test and post-test outcome measurement
An outcome assessor blinded to the participant assignment will be pre-trained on five patients and evaluated for consistency of measurements. The participants will be interviewed at baseline for the amount of real-world arm use and patient goals and tested for the capacity to perform arm function by a therapist blinded to intervention allocation. This will be repeated by the same therapist once the intervention is completed by treating therapist and after an additional 1-month follow-up. If there are dropouts who have completed at least a month of intervention, they will be requested to undergo post-test and follow-up assessment.
Outcome measures
Primary outcomes
Motor Activity Log
The MAL—Amount of Arm Use and Quality of Movement subscales will be used to quantify the actual amount of arm use by the participants. The scale has been proven valid and reliable.34
The REACH scale
The REACH scale will be used to measure the nature of real-world arm use. The activities identified by the scale will incorporate the patient preferred tasks and this scale is proved valid and reliable.35We will elicit responses for activities that were selected for practice by the participants in this study.
The two primary measures are intended to capture how and how much the participants use the arm across a range of upper extremity activities.
Secondary outcome measures
Activity-specific MAL
The participant selected tasks will be measured using the scoring method used in section Motor Activity Log.
Goal Attainment Scale
The Goal Attainment Scale (GAS) is a patient-driven outcome measure and it will be used to identify how an individual goal set by the patient is achieved. The items chosen by the patient will be scored in a standardised manner. It is a sensitive patient-centric measure.36
The activity-specific MAL and GAS are intended to capture how and how much arm use increases in the specific activities trained in the study.
Action Research Arm Test
The patients will be evaluated for their functional capability using Action Research Arm Test. The participant’s performance will be videotaped and scored according to the standard format. The measure has been proven valid and reliable.37
ABILHAND
This measure will be used to evaluate the patient-perceived capability of arm function on 23 common daily life tasks that require bilateral involvement. It’s validity and reliability has been established among stroke survivors.38
Fugl-Meyer scale
The upper extremity motor performance will be evaluated using Fugl-Meyer scale. It’s validity and reliability have been established on subacute and chronic stroke survivors.39
Measurement of functional task practice
An activity log including the amount of functional task practice of goals set by the participants in each week will be documented for both the groups. This will be categorised as optimal, suboptimal or none. Optimal quantity includes the performance of independent functional task practice for at least 1 hour in a day at a moderately challenging intensity.
We will document the baseline characteristics of all participants, such as demographic details, disease characteristics and severity of stroke.
Time points of measurement
All outcomes will be measured before starting the intervention, post-intervention and at follow-up of 1 month.
Study integrity check
Compliance, co-interventions, crossover and contamination to the planned intervention will be documented. Patient adherence to trial will be reinforced by providing self-actualisation contingencies, such as reminders, event greetings and appreciation of follow-up.
Harms assessment
Adverse events are untoward medical complications in a participant that does not necessarily have a causal connection to the intervention will be prospectively solicited from the participants weekly by the therapist providing the intervention. It will be communicated through the study coordinator to the institutional review board. The reasons will be discussed among the study team and supportive actions initiated. We will document the adverse events in adverse event reporting form and submit to the institutional review board. The review board on evaluation will initiate the necessary actions. In case of second stroke, falls and all other serious adverse events, we will provide intervention until needed. In case of deaths, as they are unlikely due to the intervention, they will not be compensated as per the regulatory rules.
Trial audit
The study coordinator will monitor the progress of the intervention delivery and all trial documents every week throughout the trial period until the closure form for individual patients is signed and submitted to the committee. Amendments relating to the study design by the study team will be informed to the institutional review board. Once approval is obtained, it will be updated in the clinical trial registry. The steering committee (table 3) will monitor the overall progress of the trial.
Analysis
Data management
The basic participant details will be separated and a unique identifier allotted on inclusion decision. These will be communicated to the study coordinator and outcome measurer. Questionnaire survey will be conducted using electronic survey forms and physical performance measures will be video-recorded. The data will be additionally entered in physical form and maintained securely. The video data will be stored in a computer and a hard drive. The cumulative scores will be provided to the study statistician for data analysis. All other study data will be maintained in the primary computer and a hard drive with the study coordinator and therapist providing intervention and made accessible to the study team at the end of the trial unless needed for scrutiny.
On obtaining the data, we will assign codes to the sheet and separately store the sheets with identifiers. The information collected through interview, audio-recording and video-recording, will contain personal identity of participants. On obtaining consent for recording, we will request removal of or drape personal identifications before video-recording; focus video camera to not capture the facial identity and code individual participant’s name in all data. We will store data with password protection in a storage device not connected to the Internet.
The researcher will provide three data analysts short-term access via secure means after signing a written confidentiality agreement. We will not share information with anyone else. We will not use individual participant’s data for the education of future participants. We will conceal individual participant identity and merge individual patient data after data analysis in academic publications. The data will be stored in one computer hard disk that will be retained with the principal investigator.
Analysis of change in outcome
The group difference between the two groups will be calculated using repeated measure Kruskal-Wallis analysis of variance for change in MAL, REACH score, GAS score, ABILHAND, Fugl-Meyer score and Action Research Arm Test score. The test will be performed at 5% level of significance. A score above established minimal clinically significant score will be considered as a positive. A score on MAL above 1.1 and GAS score of 1 will be considered as clinically meaningful improvement.40 A complier average causal analysis will be conducted to find the comparative efficacy of control and experimental interventions.
Analysis of reason for the change in the amount of arm use
The following candidate variables will be evaluated by regression analysis to identify the explanatory variable for change in the amount of arm use:
Presence of change in functional task practice.
Increase in functional capacity of arm as measured by Action Research Arm Test.
Participant demographics, such as age×gender interaction, and confounding variables mentioned.
Presence of prior exercise behaviour.
Differential duration of contact between the groups.
Discussion
The primary aim of this trial is to translate theoretically guided, evidence-supported BCTs commonly used by health behaviour interventionists to improve arm use behaviour after stroke. This translation is necessary since attaining and maintaining optimal arm use for multiple activities is challenging.41
This protocol, unlike prior upper extremity studies that have employed behaviour change interventions, defines the behaviour of interest; provides theoretical basis for tailoring and selection of target factors influencing behaviour; and incorporates evidence-based BCTs to promote arm use. This is in line with the current standards of developing and implementing complex interventions.42 This would help us to understand not only the effectiveness of the intervention but also the reasons for behaviour change if one occurs. Additionally, implementing the intervention in rural and semi-urban regions of a developing country where learning of behaviour may be influenced by the cultural context and community awareness can help us glean novel insights on barriers amenable or resistant to change as compared with programmes tested elsewhere. In addition to identifying their effects in improving the arm use behaviour, the study’s findings will provide us insights on the degree of enhancement of personal and environmental context achievable in the study participants.
Currently, we have tried addressing prevalent factors influencing physical activity behaviour identified among stroke survivors. However, there is a paucity of studies exploring determinants specific to arm use. A better targeting of the factors will become possible in future trials when such factors are identified. Nevertheless, this study will help us to identify methods of how regular physiotherapy can additionally be reinforced by addressing known potentially modifiable contextual determinants as a comprehensive entity. If found effective, this tailoring algorithm has the potential to reduce the amount of resources necessary for achieving the target behaviour as compared with generic programmes. The results will also help us to elicit unique contextual determinants in this region. Since how the contexts interact to modulate arm use may vary between cultures, the different factors can provide preliminary clues on how to address these issues elsewhere.
Ethics and dissemination of findings
Participants will sign a written informed consent prior to participation. The trial started on November 2017 and will be completed by November 2019. On completion, the trial results will be communicated to the trial participants. Further suggestions appropriate to their stage of recovery will be provided. The study results will be communicated through publication in a journal. The summary of the results will be presented to the staff of physiotherapy department of the institution. The authorship will be accorded as guided by the institutional policy.
Acknowledgments
We would like to acknowledge Dr Vasudeva Gudatta, Associate Professor at Department of Statistics, Manipal Academy of Higher Education, India, for providing statistical consultancy; Dr Steve Bellomy, Assistant Professor, Clarke University, USA, for proofreading and language corrections; and K Hariohm, Spring Physiotherapy Centre, India, and Prakash, Associate Professor, Ashok and Rita Patel College of Physiotherapy, India, for providing comments on an earlier version of the article.
References
Footnotes
Contributors VR conceived the study, and participated in the design and preparation of the manuscript. JMS contributed to the concept, design and preparing the manuscript. MN, SPG and SP contributed to the concept, design and reviewing the manuscript. VR is currently pursuing PhD in the Department of Physiotherapy, Manipal College of Health Professions, Manipal Academy of Higher Education, India. JMS and MN are associate professors in the Department of Physiotherapy, Manipal College of Health Professions, Manipal Academy of Higher Education, India. SP is the Head of the Department of Psychology, Manipal College of Health Professions, Manipal Academy of Higher Education, India, and SPG is the Head of the Department of Neurology, Kasturba Medical College, Manipal Academy of Higher Education, India.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Written informed consent obtained.
Ethics approval The study has been approved by the Institutional Ethics Committee of Kasturba Hospital (IEC 431/2016), Manipal, India.
Provenance and peer review Not commissioned; externally peer reviewed.