Article Text

Abstract
Introduction The current practice of service delivery in Germany for people with complex communication needs (CCN) who are in need of augmentative and alternative communication (AAC) is characterised by diverse problems, including a lack of clarity in the responsibilities of the service providers involved. To address these issues a new service delivery model has been put in place, implemented in three AAC counselling centres for patients with a particular health insurance across Germany. The implementation of a new service delivery model aims to improve individualised service delivery. The model goes beyond standard care by adding case management, counselling, AAC training and, if needed, AAC therapy. This study aims to evaluate the effectiveness of this complex intervention.
Methods and analysis In consideration of the complexity of the new service delivery model, formative and summative evaluation will be conducted. The formative evaluation will provide data based on qualitative and quantitative assessments of the competences and perspectives of all involved stakeholders, including a proxy measurement of persons with CCN. The summative evaluation will include a controlled study design as the new service delivery model will be compared against the service delivery in an existing contract and against data gathered from caregivers of AAC users provided with standard care. With the exception of the individual interviews the data will be collected from proxies—that is, informal and formal caregivers.
Ethics and dissemination Data collection, storage and evaluation meet the currently valid data protection regulations. Consultation by the responsible data protection officer of the Oldenburg Medical School and a positive vote from its Ethics Committee were obtained prior to the start of the study. Dissemination strategies include the presentation of the obtained data and results in the form of publications and at conferences.
Trial registration number DRKS00013628.
- augmentative and alternative communication
- complex intervention
- mixed methods
- health services research
- evaluation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- augmentative and alternative communication
- complex intervention
- mixed methods
- health services research
- evaluation
Strengths and limitations of this study
To date, case studies have been the main method used to evaluate augmentative and alternative communication (AAC) services. Therefore, the design of this interventional study, a controlled trial with follow-up, is an important step towards developing evidence-based practice in AAC.
A mixed-methods study design is used with focus group interviews, individual interviews with persons involved in AAC care and AAC users themselves as well as longitudinal surveys of formal and informal caregivers.
Both proxy assessments of outcomes by survey and by focus group data through informal and formal caregivers can be a source of bias.
The opportunity to involve AAC users in the study design, implementation and data collection was limited through resources available.
Due to the high degree of heterogeneity of the sample, sensitivity and robustness of measures across the full cohort are unclear.
Introduction
Augmentative and alternative communication (AAC) is a communication therapy concept for people who are unable to speak due to congenital or acquired disabilities. Their ability to communicate is either severely impaired or progressively worsens as a result of neurodegenerative processes.1 Furthermore, there are acquired conditions that result in AAC needs that are not progressive (eg, traumatic brain injuries).2 The most common nine medical conditions which lead to complex communication needs (CCN) are dementia, Parkinson’s disease, autism, learning disability, stroke, cerebral palsy, head injury, multiple sclerosis (MS) and motor neuron disease.3 Frequently, people with CCN receive support from speech and language therapists, who has in some cases already initiated AAC measures. In Germany, however, not all speech and language therapists specialise in AAC, so clients are often not adequately supplied.4 It is also important to note that AAC includes both aided systems (eg, communication boards or devices with voice output) and unaided systems (eg, gestures).5 Additionally, caregivers often find using some forms of AAC harder than others, and this is a significant factor in whether an AAC method is used or not.6 No comprehensive information is available on the prevalence of AAC needs in Germany. Data from Australia show that approximately 0.2% of the Australian population have CCN.7 Considered in detail, approximately 25% of people with cerebral palsy and 17%–25% of children with autism spectrum disorders fail to develop functional speech and have CCN.8–10 In addition, surveys from the USA show that among students receiving special education services, 3%–12% have CCN.11 12 Data from the UK show that approximately 0.5% of the population could benefit from AAC.3
Previous studies have identified the following six core problems in the AAC supply chain in Germany: (1) lack of legally binding regulations, (2) lack of qualifications in different occupational groups involved in the AAC care process, (3) poor quality of care (eg, inappropriate prescription and use of AAC systems), (4) missing aftercare after delivery of the aid, (5) lack of supply standards/guidelines for the care process, and (6) large regional differences in service delivery.13–17 So far, the evidence base on effective AAC interventions and models in Germany is sparse. Studies from the UK also show that the provision of AAC interventions was highly variable and that the provision of AAC devices was inconsistent and inequitable.18 19 Existing studies are limited to observational studies and often case studies without rigorous evaluation designs due to challenges with data collection from people with CCN.20–22 By German law, the service delivery model for AAC services involves a physician prescribing, that is, a certain speech generating device. Afterwards the healthcare insurance decides—sometimes with the Medical Service of the Health Insurance Companies involved—whether or not the device (or another one) will be funded (§ 33 SGB V). If funded the device will be provided, adapted and introduced by an AAC device company. This service delivery model lacks the involvement of AAC experts or speech and language therapists. Therefore, in 2011, a contract was signed by one of the leading health insurances in Germany with a pioneering AAC research and counselling centre, which allows the funding of AAC assessment and intervention planning provided by AAC experts to provide better recommendations for physicians and their prescriptions. Since the AAC care in the existing contract stops after AAC device delivery there is still insufficient support in learning to use the AAC system. For this reason, AAC systems are often not used in everyday life in Germany. Furthermore, there is often a lack of communication and cooperation between different occupational groups involved in the AAC care process. To close these gaps in the AAC supply chain and support the process of learning to use the AAC system a new service delivery (nSD) model was developed, which adds the following components: case management, training and, if necessary, intervention therapy in using AAC. As part of the nSD, patients may receive aided AAC systems (eg, voice output devices or paper-based communication books) or non-aided AAC systems (gestures). For detailed information see figure 1.

Augmentative and alternative communication (AAC) care structures in Germany.
Aims of the study
The overarching aim of the intervention study is to improve AAC care and fill the gaps in the AAC supply chain in order to achieve a functional use of resources and, as a result, significantly improved communication of persons with CCN. Primarily, the study aims to analyse whether the nSD correlates with an increase in communication skills, quality of life and participation for AAC users. Furthermore, the aim is to study any potential impact on AAC users’ and caregivers’ utilisation competence, acceptance, use of the AAC system, therapy compliance and satisfaction with the use of the AAC device. The following logic model (figure 2) illustrates the suggested relationships between the intervention processes and the indicators to be measured.23

Logic model. Bold denotes indicators to be measured (formative and summative evaluation). AAC, augmentative and alternative communication.
Methods and analysis
Study design
The research questions will be examined in the form of an interventional mixed-methods study to satisfy the requirements of the heterogeneous target group and the complexity of the intervention. A formative and summative evaluation of AAC care will be undertaken.23–25 The development of the intervention (nSD) started in March 2018 and the recruitment of participants and the intervention (nSD) started in June 2018 and will end in November 2019. The project will run until the end of November 2020.
Summative evaluation
The summative evaluation involves a controlled trial with follow-up measurements examining a primary outcome (pragmatic communication skills) and secondary outcomes (quality of life, participation and satisfaction with the AAC device). For each AAC user, outcomes will be assessed by a formal caregiver (eg, teacher, speech and language therapist or educator) and an informal caregiver (eg, parent, relative or friend) in proxy surveys. The outcomes of the nSD in the intervention group will be compared with two comparison groups (figure 3). By means of a quasiexperiment, it will be determined whether patients receiving the nSD reach better outcomes, compared prospectively with patients receiving service delivery under the existing contract (SDeC) and compared retrospectively with patients having received standard AAC care. The longitudinal measurements in patients receiving the nSD, with a baseline and two follow-up measurements, also provide valuable information on AAC care processes and mechanisms. The data will be collected by means of a standardised postal survey of informal and formal caregivers after the initial consultation (T0), 4 weeks after AAC system receipt (T1) and 4 months after AAC system receipt (T2). Two reminders will be sent out for every survey.26 The retrospective survey of informal caregivers is a cross-sectional survey with one reminder (figure 3).
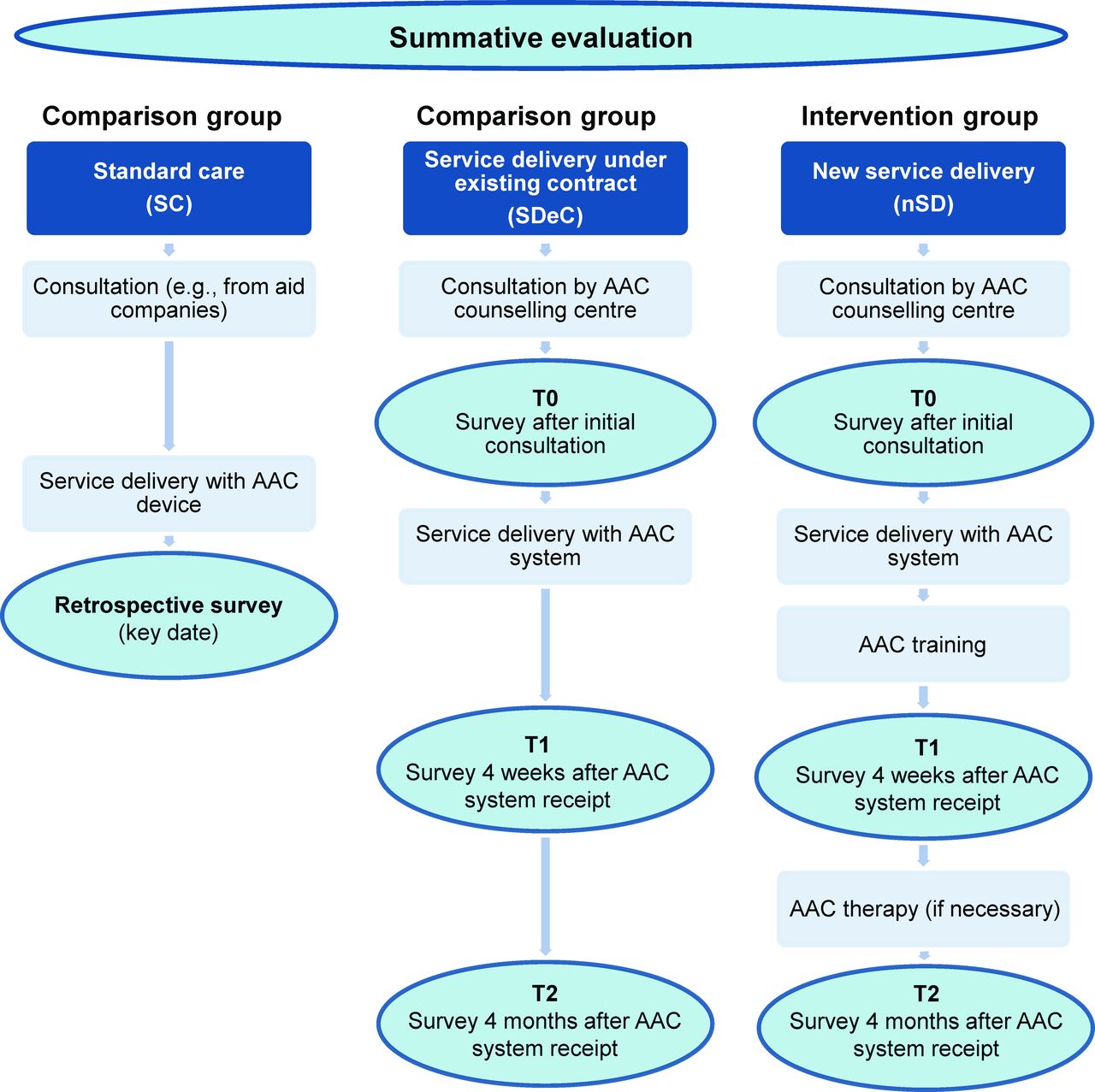
Study design of the summative evaluation. AAC, augmentative and alternative communication.
The controlled trial will investigate primarily the following questions:
Are AAC users receiving the nSD reported by caregivers as having better pragmatic communication skills than AAC users in the comparison groups?
Are AAC users receiving the nSD reported by caregivers as having a higher quality of life than AAC users in the comparison groups?
Are AAC users receiving the nSD reported as having a higher level of participation than AAC users in the comparison groups?
Are caregivers of AAC users using aided AAC systems who receive the nSD more satisfied with the AAC systems than caregivers of AAC users in the comparison groups?
Formative evaluation
The focus of the formative evaluation is on the different components of the complex intervention and its implementation characteristics.27 The formative evaluation supplements the prospective study with a cross-sectional observational study, in which the perspectives of the study participants (AAC users, informal and formal caregivers) on the nSD and its implementation will be elicited by means of qualitative and quantitative methods.28
On the one hand, the quantitative surveys (T0–T2) from the summative evaluation contain instruments for the formative purpose. On the other hand, five to six qualitative focus group interviews with four to eight people will be conducted at two points in time, before and during the nSD, with formal and informal caregivers involved in care (figure 4). In the first focus group interviews the AAC care in Germany in general as well as the care network and the interaction of the stakeholders will be discussed. Thus, they will be conducted before the intervention starts (preformative). The second focus group interviews focus on the caregivers’ and AAC counselling staff’s perception of the nSD implementation. These focus groups will be conducted in the middle of the project to ensure a process evaluation and, if necessary, changes can still be made. The focus groups will be led by two researchers using a semistructured interview guideline and will last up to 90 min.29 30 The development of the topic guide for focus group interviews followed the existing standards,29 31 32 objectives and research questions of the project.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Study design of the formative evaluation. AAC, augmentative and alternative communication.
Furthermore, AAC users with sufficient communication skills who participate in the nSD will be interviewed using individual, semistructured interviews about the care process (figure 4). The individual interviews are conducted with the first participants who have completed the nSD in the middle of the project duration to be able to provide feedback for intervention improvement. The topic guide for the individual interviews will be developed in close consultation with the cooperating counselling centres, as they have expertise in working with AAC users. In the topic guide development, the fact that the interviewees use AAC and may have multiple learning disabilities will be considered.33 A total of 9–12 interviews, each lasting about 60 min, will be conducted.34 35 The following questions will be answered during the formative evaluation and refer to the quantitative data of the survey as well as the qualitative data of the focus groups and individual interviews concerning the nSD:
Utilisation competence, acceptance and effective and regular use: How competent are the patients and caregivers in using the AAC system? Is the AAC system accepted and regularly used by patients and caregivers?
How do caregivers and AAC users rate the training and therapy?
How do the caregivers and AAC users assess and perceive the nSD? How is their acceptance for the new AAC system affected by the nSD? How satisfied are caregivers and AAC users with the nSD?
How well supported by case management do caregivers and AAC users feel?
Sample
People with CCN of all ages can participate in the study. Due to this and the fact that people with CCN with various diseases and disabilities can participate the study sample is very heterogeneous in order to represent AAC users in the general population. Patients in the intervention group (nSD, n=240) and in the prospective comparison group (SDeC, n=200) will be prospectively recruited for the study over 18 months, and each patient will be observed over 6 months. The essential distinction between the intervention and the comparison group is the health insurance fund (AOK Rheinland/Hamburg=nSD, other funds=SDeC).
The historical comparison group consists of patients who received an AAC device in standard care (SC) outside the two models and who were covered by the health insurance fund AOK Lower Saxony between 2014 and 2018 (n=400). The reason for the recruitment of AOK Lower Saxony’s insured persons for SC is that AAC care is still largely unregulated as there are hardly any AAC counselling centres in the state of Lower Saxony.
Apart from the care model and the health insurance fund, inclusion criteria for the patients in the three study groups are the existence of a congenital or acquired severe disability that is associated with the absence or loss of speech and/or speech skills. Patients in particular include children, adolescents and adults with congenital disabilities and complex communication disorders (eg, International Classification of Diseases Tenth Revision (ICD-10) diagnosis codes F07, F84, G40, G80, I60, Q75, Q87.2, Q90 and Q93.5) and adults having experienced apoplexy, craniocerebral trauma or in the final stages of neurodegenerative disorders with effects on spoken language, such as amyotrophic lateral sclerosis (ALS), multiple sclerosis (MS) and Parkinson's disease (eg, ICD-10 diagnosis codes G10, G20.9, G35 and R47).
The power calculation is based on the comparison between the intervention group and the prospective comparison group within the existing contract with regard to the primary outcome of pragmatic communication ability. Equal variances are assumed in both groups. Based on the mean expected increase in pragmatic communication skills of 10 scale points and referring to the estimated standard deviation (SD) from the US standard sample,36 the expected effect size measured in Cohen’s d equals 0.44. At a significance level of 5%, a required power of 80% and using an independent two-sided t-test, a sample size of 81 participants per group is required.37 Since the power calculation only relates to the primary endpoint of pragmatic communication skills and the target group has a high level of heterogeneity, it seems appropriate to aim for a larger sample size than 81 participants. To reach a sufficient sample size, a complete survey of all patients in the nSD and SDeC and their formal and informal caregivers must be conducted via the counselling centres. Based on the previous utilisation of the three counselling centres, a sample of 240 nSD patients and 200 SDeC patients can potentially be recruited over this period; for the retrospective analysis of SC patients, a sample of approximately n=400 patients can be contacted. The assumed sample size after considering non-participants, non-responders and dropouts is n=175 nSD patients, n=146 SDeC patients and n=280 SC patients.
Recruitment
The recruitment in the nSD and the SDeC will take place via the three participating counselling centres, where patients and caregivers receive initial counselling. The caregivers usually contact the AAC counselling centres by telephone. During this telephone call the healthcare insurance will be inquired and clarified whether they can participate in the nSD or in the SDeC (nSD: only insured persons of the AOK Rheinland/Hamburg). The caregivers receive the first information about the study orally and together with the patients they are invited to the initial consultation in the counselling centre without obligation. The initial consultation is carried out by the AAC counselling centre staff. In the initial consultation the caregivers receive all information about the study in written form and can decide whether they want to participate in the study. In the event that they do not want to participate in the nSD they would receive the SDeC instead. In case of participation, two caregivers (formal and informal) have to be named to whom the questionnaires will be addressed. These caregivers must provide their written consent which will be sent to the evaluators. If AAC users and caregivers participate in the nSD intervention they participate in the evaluation study at the same time.
Patients who received SC between 2014 and 2018 will be identified by the health insurance AOK Lower Saxony based on claims data. AOK Lower Saxony will contact the patients’ informal caregivers by mail in order to invite them to participate in the study. All potential study participants will be informed in written form about the study and asked to complete the survey.
The recruitment for all focus group interviews (before and during the intervention) is carried out by purposeful sampling38 and all participants are formal or informal caregivers and/or counselling staff of the three AAC counselling centres involved in the study. The focus group interviews performed before the project start will be heterogeneously composed to capture the different perspectives of those involved in AAC care. The participants of these focus group interviews will be selected out of four groups: (1) AAC speech and language therapists, (2) consultants from the AAC counselling centres, (3) educators, teachers, employees of a sheltered workshop, employees of homes for disabled persons, and so on, who are in contact with AAC, and (4) parents and relatives of persons who use AAC systems. For privacy reasons, the AAC counselling centres recruit the participants from their patient base.
The content of the second focus groups is the implementation of the nSD. In this round two types of focus groups will be performed: (1) On the one hand, there will be heterogeneous focus groups with formal and informal caregivers who participate in the nSD. In this context it will be ensured that formal and informal caregivers from the same AAC user will not participate in the same focus group. (2) In addition, a homogeneous focus group will be conducted with the AAC counselling staff working on the nSD. These two types of focus groups ensure that different views of the nSD will be collected and that the participants feel free to express themselves. Here, recruitment will be conducted by the evaluators, since written consents and contact details are present.
For the individual interviews, AAC users from the intervention group will be interviewed if they have sufficient communication skills. Sufficient communication skills mean that the AAC users are able to participate in an interview. That means, for example, they are able to answer questions with Talking Mats. AAC users aged 18 and older are allowed to participate in the individual interviews. Experienced employees from the counselling centres will provide support in the assessment of the AAC users’ abilities. The use of AAC methods like Talking Mats in interviews aims at involving AAC users in the interviews. Talking Mats is an internationally used communication tool which can be successfully used in research and clinical practice.39 Duration and procedure of the individual interviews will be adapted to the needs of the interviewees.
Measures
As part of the summative evaluation, three questionnaires will be developed to measure the outcomes of AAC care in a proxy survey of formal and informal caregivers of AAC users. The questionnaires include already validated scales, if available, as well as scales adapted to the target group and self-developed questions. The primary outcome of pragmatic communication skills is defined as the ability to communicate in everyday situations (such as greeting, agreeing and rejecting). AAC users often have difficulties acquiring pragmatic communication skills and are more likely to take a passive role in discussions.40–44 Pragmatic skills play a key role in the successful integration of people with disabilities.45 46 Studies show that good social skills are the key to school and work integration and that social skills have a significant impact on quality of life.47–49 The questionnaires at all three timepoints (nSD, SDeC) as well as the questionnaire for the retrospective survey (SC) include identical instruments with respect to the primary outcomes.
The high heterogeneity of the target group with regard to age and severity of the speech impairment as well as the use of various AAC systems (aided and unaided) and the proxy survey did not allow to rely solely on existing validated scales for measuring pragmatic communication skills. For this reason, a target group-specific new proxy scale has been developed. The items are based on the proxy survey instrument Pragmatics Profile, which is validated to reflect the development of language abilities of students aged 5–21 years and is part of the diagnostic tool ‘The Clinical Evaluation Language Fundamentals—CELF-5’.36 The initial idea of using the original version of the scale Pragmatics Profile was rejected as it has proved to be too difficult for proxy assessment by caregivers in pretests. In addition, this scale is not suitable for answering the items without a skilled person explaining the items. Furthermore, the developed items are based on the communication functions checklist from the programme ‘Communicative Development of nonspeaking children and their Communication Partners’ which is a generic programme developed for all age groups of AAC users and their families to enhance 16 communication functions.50 To measure the secondary outcome of quality of life, the German short version of the quality of life questionnaires for children with chronic conditions (DISABKIDS), a validated tool for measuring the quality of life of children with chronic diseases, is used.51 The items of the tool were adapted to our target group as well as to the proxy survey design. To measure the participation of AAC users, the German short version of the validated proxy instrument WHO Disability Assessment Schedule 2.0 will be used. The long version of this instrument contains items on six domains (cognition, mobility, self-care, getting along, life activities and participation). The short version explains 81% of the variance of the long version. This instrument is validated for assessing health and disability levels in the general population by self-report and for measuring the clinical effectiveness and productivity gains from interventions.52 53 Satisfaction of caregivers with the AAC system (in cases of aided AAC systems) will be measured as another secondary outcome using the German version of the instrument The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) which is validated for measuring user satisfaction with assistive technology.54 55 Both sections of the instrument (device, eg, size, comfort and service, eg, repair and information services) will be used. As part of the summative evaluation, the following sociodemographic information will be collected in order to control for them during the comparisons as potential confounders: (1) data about caregivers: technical affinity, gender, age group, mother tongue, German language skills, highest educational attainment, employment situation, housing situation, relationship to the AAC user; (2) data about AAC users: gender, age group, housing situation, employment situation, family language(s), duration of contact with the German language, cause of disability (acquired or congenital), severity of the disability and degree of the disability.
As part of the formative evaluation caregivers rate the AAC training and the AAC therapy in the nSD. The used instrument is based on the Training Satisfaction Questionnaire.56 Utilisation competence, acceptance and use of the AAC system are measured by a scale, which is based on the AAC Acceptance Scale.57
Quality assurance during study execution will be guaranteed by the standards of questionnaire development,58 59 pretesting,60 the total design method to increase response rates26 and data processing with the Teleform software.
The methods of summative and formative evaluation and the corresponding measurement instruments have been summarised in tables 1 and 2.
Data collection methods of the summative evaluation
Data collection methods of the formative evaluation (nSD)
Data analysis
With reference to the summative evaluation, the collected data of the intervention group will be compared with the comparison groups’ data by using descriptive statistics and multivariable regression analysis. Within this framework, possible confounders (eg, technology readiness, burden on private caregivers or sociodemographics) will be controlled. The collected survey data of the formative evaluation that only refers to the intervention group will be analysed with descriptive statistics and tests for mean differences in dependent samples between the three survey measurements to detect differences over time. After testing psychometric properties, reliabilities and performing a factor analysis we will form composite scores based on the scale manuals. Moreover, multivariable regression models will be employed to identify associations with independent variables (eg, sociodemographics, disability type and severity). All derived effects will be calculated with 95% CIs and corrected for multiple testing.
The data from the focus group interviews and the individual interviews will be analysed in the form of a structured qualitative content analysis according to Kuckartz.61 For this purpose, the audio recordings will be first transcribed verbatim and pseudonymised according to standards of transcription.62 Structuring qualitative content analysis is a multistage process in which first, a priori main categories derived from the interview guideline will be developed. During the coding process, subcategories will be inductively formed. The computer-aided coding of the text segments into the categories will be performed using the program MAXQDA. The entire coding process will be performed by two persons independently. The details of the evaluation are summarised in tables 1 and 2.
Patient and public involvement
Practice partners from the cooperating counselling centres with a lot of experience working with AAC users are involved in the planning, recruitment and instrument development of the study via regular meetings. An AAC user is part of the team in one cooperating counselling centre and has also provided advice. AAC users and their caregivers who participate within the study will be recruited for interviews to assess their preferences, expectations and experiences. Despite these aspects patient involvement in the study design is limited through resources available.
Ethics and dissemination
Ethical considerations
Before the beginning of the study, the study protocol was submitted to the Ethics Committee of the Oldenburg Medical School for professional consultation, and it received a positive vote. The investigation will be conducted in accordance with the Helsinki Declaration as amended and the underlying data protection regulation (EU GDPR). All study participants will submit written consent based on the current data protection regulations. Audio recordings of study information and consent forms in appropriate symbolised format will be produced for AAC users. All personal identifiers will be pseudonymised. The planned processing of personal data is legally permissible and the security measures to be taken are suitable and appropriate for controlling the existing risks. The evaluation study is entirely the responsibility of the research team of the Department of Organizational Health Services Research of Carl von Ossietzky University Oldenburg. The identifying data and the research data will be stored independently. Participation in the study is voluntary.
Dissemination plan
The results of the evaluation will be finalised in an evaluation report. Based on the report, it will be decided to what extent the care practice can be influenced and whether the evaluated new AAC service delivery model can help develop a new nationwide AAC care concept. The results will be disseminated in the scientific community via publications and congress contributions. The aim of this funding was to be able to decide on the larger implementation of these interventions, after evaluations have proven their effectiveness. Since this is a rather new national funding instrument, it is currently unclear on the basis of which criteria the Innovation Fund will decide which care models will be included in the SC in Germany and which not.
References
Footnotes
AZ and SAKU are joint first authors.
Contributors All members designed the study. AZ and SAKU drafted all sections of the paper. LA revised all sections of the paper and is the guarantor. JB, SKS and TB revised the paper. AZ, SAKU and LA designed the data collection tools, defined the sampling criteria and revised the paper.
Funding The study is funded by the Innovation Fund of the Federal Joint Committee (Grant No 01NVF17019). Both the new service delivery (counselling, AAC training and AAC therapy) and the evaluation of the intervention are financed by the Innovation Fund.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval A consultation by and a positive vote from the Ethics Committee and the responsible data protection officer of Oldenburg Medical School was obtained prior to the start of the study.
Provenance and peer review Not commissioned; externally peer reviewed.