Article Text

Abstract
Introduction As the early stage of coronary heart disease (CHD), borderline coronary lesion (BCL) is defined as a 30%–70% diameter stenosis. Previous studies have demonstrated that BCL may progress to acute coronary syndrome easily. However, routine medications available for the treatments of BCL have some limitations. Xuanbi antong granule (XAG) has been used for the treatment of BCL in China for many years. Previous studies have shown that XAG has effectiveness in improving clinical symptoms and quality of life in patients with CHD. This study aims to evaluate the effectiveness and safety of XAG in patients with BCL.
Methods and analysis This is a multicentre, randomised, double-blinded, placebo-controlled clinical trial. A total of 300 participants will be randomly assigned to the intervention group and the placebo group. Based on routine medications, the intervention group will be treated with XAG and the placebo group will be treated with XAG placebo. All participants will receive a 6-month treatment and then be followed-up for another 6 months. The primary outcomes are the changes of target plaque characteristics (including target plaque volume, degree of stenosis, CT value and calcification score) measured by dual source CT angiography. The secondary outcomes include blood lipid indicators, efficacy of angina symptoms, Seattle Angina Questionnaire, high-sensitivity C-reactive protein and occurrence of major adverse cardiac events. All the data will be recorded in electronic case report forms and analysed by SPSS V.20.0.
Ethics and dissemination This study has been approved by Research Ethics Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences in Beijing, China (No. 2017–083-KY-01). Written informed consent will be obtained from all participants. The results of this study will be disseminated to the public through academic conferences and peer-reviewed journals.
Trial registration number ChiCTR-IOR-17013189; Pre-results.
- Chinese herbal medicine
- borderline coronary lesions
- randomised controlled trial
- protocol
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This multicentre, randomised, double-blinded, placebo-controlled clinical trial is exploring the effectiveness and safety of xuanbi antong granule for the treatment of borderline coronary lesions.
We used a non-invasive test dual source CT angiography to evaluate the degree of coronary artery stenosis and plaque compositions, which is easy for investigators to operate and more acceptable to participants.
Participants are randomised in a 1:1 ratio using central randomisation system (CRS), and the blinding codes will be kept by the manufacturer of CRS, which effectively guarantees the implementation of blinding in clinical trials.
The data from all participating centres will be recorded in electronic case report forms and imported into public clinical trial management platform (www.medresman.org) within 6 months after the trial completes.
Our experiments will be conducted in three regions of China, and whether similar effects are available to other ethnic groups and regions remains uncertain.
Introduction
In China, cardiovascular disease(CVD) remains the leading cause of mortality, which accounts for 44.8% and 41.9% of deaths in rural and urban area, respectively. In Europe, CVD is still the most common cause of deaths, which accounts for 45% of all deaths. Among them, coronary heart disease (CHD) is the most common cause, which accounts for 20% of all death. The incidence of CHD is continuously increasing and the burden of CHD remains heavy, which has become a major public health issue.1 2 As the early stage of CHD, borderline coronary lesion (BCL), also called intermediate lesion, is defined as a 30%–70% diameter stenosis.3 Although the presence of severe coronary stenosis has been traditionally explained as indication of myocardial ischaemia, yet it has been reported that coronary occlusion and myocardial infarction most frequently evolve from mild to moderate stenosis.4 Some other studies have recently demonstrated that approximately 87% of lesions requiring subsequent percutaneous coronary intervention (PCI) were ≤60% in severity during original PCI, and 6% of patients with intermediate lesions needed PCI in 1 year because of acute coronary syndrome (ACS).5 There is evidence that BCL may become unstable and can be the starting point for ACS.6 Studies have shown that patients with BCL have a higher burden of mixed plaque (MP, 46%) and non-calcified plaques (NCPs, 33%), also known as vulnerable plaque.7 The number of deaths resulting from BCL continues to rise despite the use of currently recommended antiplatelet therapy, lipid-lowering therapy, revascularisation procedures as appropriate, and other evidence-based secondary preventive measures.8 It has been demonstrated that plaque regression was associated with a lower rate of major adverse cardiac events (MACEs).9 Therefore, it is necessary to develop multidisciplinary management method that can relay or reverse plaque progression and eventually reduce the occurrence of MACEs in patients with BCL.
Currently, the main treatment methods for BCL include lifestyle changes, medical treatment and coronary revascularisation. Among these treatments, revascularisation, including PCI and coronary artery bypass grafting (CABG), is recommended for patients with significant anatomic (≥50% Left Main or ≥70% Non-Left Main) coronary artery stenosis to improve survival and symptoms.3 In the era of drug-eluting stents, some might suggest that stenting all BCL is a suitable therapy. However, there are still some procedural complications related to revascularisation, such as in-stent restenosis and stent thrombosis.10 Moreover, research shows that revascularisation is not relevant to improved long-term survival which may not be warranted in patients with BCL.11 Among routine medications, antiplatelet and lipid-lowering therapy are mostly important in the treatment of BCL. Aspirin and clopidogrel are the most commonly used antiplatelet medications, which can reduce MACEs in patients with BCL. Whereas, studies have found that in patients with CHD, 5%–45% are aspirin-resistant, 4%–30% are clopidogrel-resistant and 10% are resistant to both.12 Previous study has demonstrated that aggressive lipid-lowering therapy using high-dose statins could reduce coronary plaque volume obviously and stabilise plaque to improve long-term progression.8 However, long-term statin therapy may cause symptomatic adverse events such as myopathy, defined as muscle pain or weakness with creatine kinase increasing in blood concentrations, and haemorrhagic stroke.13 In addition, many patients do not receive the conventional treatments because of the side effects, contraindications and unsatisfied relief of symptoms.14 It is therefore crucial to develop supplementary therapeutic approaches for the treatment of BCL.
Chinese herbal medicine (CHM), a popular type of supplementary and complementary medicine, plays a significant role in treating BCL in China. Within the framework of Traditional Chinese Medicine (TCM) theory, all the related symptoms at a certain stage of a disease are summarised as a syndrome (‘Zheng’ in TCM), which has been used in China for more than 3000 years.15 Patients with BCL can be divided into varied syndromes. In the diagnosis of BCL, ‘phlegm, blood stasis and heat syndrome’ is an important syndrome based on the viewpoint of TCM theory and our previous clinical practice.16 Therefore, the principle of ‘clearing away heat, resolving phlegm, promoting blood circulation and removing blood stasis’ is applied in the treatment of BCL. TCM practitioners always attach importance to preventing disease before it arises and controlling the development of existing disease. Therefore, there are some special advantages for TCM in controlling the plaque progression of BCL.
Xuanbi antong granule (XAG) is a commonly used CHM based on the TCM theory of ‘clearing up heat, resolving phlegm and promoting blood circulation’ for prevention of BCL in China. Clinical trials have found that XAG is effective in improving clinical symptoms and improving the quality of life in patients after PCI by protecting endothelial cells and regulating platelet function.17 Experimental studies have found that XAG can significantly improve the heart function of ventricular remodelling rats after myocardial infarction, by down-regulating inflammatory factors of TNF-a.18 XAG consists of eight herbal medicines (table 1), including salviae miltiorrhizae (Dan Shen), puerariae lobatae radix (Ge Gen), peaoniae radix rubra (Chi Shao), cistanches herba (Rou Cong Rong), pinellia rhizoma (Ban Xia), ginseng radix et rhizoma (Ren Shen), coptis chinensis (Huang Lian), panax notoginseng (San Qi). Among them, salvia miltiorrhiza, panax notoginseng and coptis chinensis are the principal pharmacologically active components. They have various pharmacological effects, including antioxidation, antiatherosclerotic, lipid-lowering, antiplatelet aggregation, protecting vascular endothelial cells, anti-inflammatory and so on.19–22 However, there is no evidence for XAG in the treatment of BCL. Therefore, we designed a central-randomised, double-blinded, multicentre trial aiming to evaluate effectiveness and safety of XAG for the treatment of BCL.
Components and dose of XAG.
Methods and design
Study design
This is a multicentre, randomised, double-blinded, placebo-controlled, parallel-group clinical trial. The study was registered at the Chinese Clinical Trial Registry on 31 October 2017 (ChiCTR-IOR-17013189). This study complies with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. We will rigorously follow the latest Consolidated Standards of Reporting Trials (CONSORT 2017) for CHM recommendations,23 Standard Protocol Items: Recommendations for Interventional Trials and 2013 statement24 for herbal interventions. Written informed consent will be acquired from all patients prior to their participation in this study. Totally 300 participants diagnosed BCL will be enrolled in the trial, which consists of a 1-week screening period, a 6-month treatment period and another 6-month follow-up period. The recruited patients will be randomised and allocated to either the intervention group or the placebo group in a 1:1 ratio using central randomisation system (CRS). In addition to routine medications, they will be given 7.72 g XAG or placebo in granule form two times per day for 6 months. The participants flowchart is briefly illustrated in figure 1.

CONSORT flow diagram for XAG clinical trial. XAG, xuanbi antong granules.
Patient and public involvement
This trial was designed to evaluate the effectiveness and safety of XAG in patients with BCL. In our previous clinical practice, early intervention of BCL may prevent the occurrence of MACEs and it is considered very important in BCL patients. XAG, a type of Chinese herbal medicine, is easily accepted by patients. Adding XAG to routine medications may increase the effectiveness in preventing the progression of BCL, thus significantly improve patients’ quality of life and reduce the occurrence of MACEs. The outcome measures used in this trial were considered as important endpoints in clinical practice. The participants of this trial will be recruited from three participating hospitals. However, patients were not directly involved in design, recruitment or conduct of the study. After the trial completes, the results of this study will be disseminated to the public through academic conferences and peer-reviewed journals. Once the manuscript is published, the results will be briefly summarised in a simple language and sent to all trial participants through e-mail and phone. The burden of intervention will not be assessed by trial participants.
Participant recruitment
Consecutive patients undergoing coronary dual source CT angiography (DSCTA) for a clinical indication will be evaluated for the entry into the study. Inpatients and outpatients at the three participating hospitals (table 2) will be screened according to the inclusion and exclusion criteria by two experienced cardiologists separately. When two cardiologists both confirm that patients conform to the criteria for recruitment, the participants will be enrolled in the trial. In addition, recruitment advertisements of the study will be posted on webpages and notice boards in three participating hospitals and resident communities. It includes a brief description of the subjects needed, the medicines, medical examinations and the ways to participate in this study. For those people who are ineligible or decline to participate, we will record the basic demographic information and reasons for non-participation. The trial began in December 2017 and will continue until December 2020.
The hospitals participating in this study
Diagnostic criteria of BCL
The diagnosis of BCL will refer to the criteria published in ‘ACC/AHA Guidelines for Coronary Angiography’, which is defined as 30%–70% diameter stenosis.3 The diameter stenosis of the main coronary, including left anterior descending (LAD), left circumflex (LCX) and right coronary artery (RCA), is between 30% and 70% measured by DSCTA.
Diagnostic criteria of CHD
Two types of CHD will be recruited, including stable angina and unstable angina. The diagnostic criteria will refer to the ‘Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease’25 (2012 edition) and the ‘Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes’26 (2014 edition).
Diagnostic criteria of TCM syndrome
Diagnostic criteria of ‘phlegm, blood stasis and heat’ syndrome in TCM will refer to the ‘Syndrome Elements Diagnostic Criteria of Coronary Heart Disease of Angina’ published by Chinese Society of Traditional Chinese Medicine Cardiovascular Disease Branch on March 2018.27 Syndrome elements are the smallest diagnostic unit for the diagnosis of TCM syndromes. ‘Phlegm, blood stasis and heat’ syndrome is the combination of ‘phlegm’, ‘blood stasis’ and ‘heat’ syndrome elements. TCM syndrome of each participant will be estimated by two TCM experts blindly. The consistency will be checked on by kappa test.
Inclusion criteria
Provision of written informed consent by participants or surrogates voluntarily.
Patients aged 30 to 75 years at the time of their consent.
Demonstration of at least one obstruction with 30%–70% diameter narrowing with NCP or MP (target plaque) in at least one main coronary artery (the diameter of the target vessel is ≥2.5 mm) determined by DSCTA.
Exclusion criteria
Chest pain caused by severe left main coronary artery lesions, severe valvular heart disease (aortic stenosis), severe psychoneurosis, climacteric syndrome, hyperthyroidism, cervical spondylosis, gallbladder heart syndrome, gastro-oesophageal reflux disease.
Uncontrolled hypertension with Systolic Blood Pressure≥160 mm Hg or Diastolic Blood Pressure≥100 mm Hg, severe cardiac insufficiency with Ejection Fraction<35%, severe arrhythmia (fast atrial fibrillation, atrial flutter, paroxysmal ventricular tachycardia, atrioventricular block higher than second degree subtype II, complete bundle branch block).
Patients with severe primary diseases like heart, brain, liver, kidney, haemopoietic system related diseases and patients whose Alanine Aminotransferase or Aspartate Transaminase is higher than 1.5 times of the upper limit, patients with abnormal renal function or insulin dependent diabetes mellitus.
Reference vessel diameter of the target vessel <2.5 mm, or there is no NCP or MP in the main coronary artery, or severe tortuosity of the target vessel or any other anatomical reasons that the investigator deems inappropriate for DSCTA procedure.
Patients have undergone revascularisation including PCI or CABG.
Patients with depression or anxiety.
Stroke or resuscitated sudden death in the past 6 months.
Hyperthyroidism with TSH levels more than 1.5 times upper limit of normal.
Patients with malignant tumour.
Pregnant women or breast feeding women.
Chronic disease requiring treatment with oral, intravenous, or intra-articular corticosteroids (use of topical, inhaled, or nasal corticosteroids is permissible).
Patients with allergic constitution or are allergic to many kinds of TCM herbs and iodine.
Patients with low compliance, who might miss the follow-up.
Participation in other clinical trials in last 1 month.
Removal, dropout and termination criteria
During the course of the study, a participant may be removed if one was not taken medication after inclusion, occurrence of myocardial infarction, revascularisation (PCI or CABG) or sudden cardiac death during the treatment period. Participants can voluntarily drop out at any time during the trial. Eligible subjects failing to complete the observation period presented in the trial will be considered as dropout cases regardless of the time and reason. Reasons for dropout will be recorded in eCRFs, and the last data recorded for these participants will be included in the data analysis. The trial will be suspended in a specific participant if (1) serious adverse events (AEs) relevant to the XAG occur; (2) the participant decides to join in another clinical research project in terms of cardiovascular diseases; (3) the participant demonstrates hypersensitivity towards XAG, such as abnormal thirsty, stomach ache and diarrhoea; (4) the participant suffers from acute life-threatening disease. The whole research would be terminated in the following circumstances: (1) masking of the randomisation fails; (2) unblinding rate exceeds 20% of the sample size; (3) assessments of all follow-up are completed.
Randomisation and blinding
Participants are randomised in a 1:1 ratio using CRS for Clinical Research (Web Edition) to achieve computerised randomisation in blocks of 4, stratified by centre. CRS could not only avoid factitious randomisation mistake but also promote the real-time track for the progress of the participant enrolment, which is successfully developed and widely applied to multicentre clinical trials.28 The CRS achieved the functions of subject screening, randomisation, emergency exposure, drug delivery and drug supply management. It has the advantage of shortening the clinical trial cycle, improving the efficiency of clinical trials and saving drug use. The researcher uses the screening module to input some basic information of the subject such as date of birth, sex and answer tests to identify the subject and then obtain the subject’s unique identification number. After the subjects pass the screening period, subjects are randomised into either XAG or placebo group by using a randomisation module. In addition, CRS effectively guarantees the implementation of blinding in clinical trials. In order to ensure that the blinding method in randomised controlled clinical trials is effectively guaranteed, the random number and the drug number are separated in the system. The researcher uses the drug designation module to obtain the drug number for the subject. All patients, laboratory and inspection staff, attending physicians and statisticians will be blinded to treatment assignment until the entire research is completed. Emergency unblinding process should only occur when the knowledge of intervention allocation is essential to guide the clinical magenement. The blinding codes will be kept by the manufacturer of CRS (Clinical Evaluation Center of China Academy of Chinese Medical Sciences). All the participants and investigators in this trial will be asked to complete a questionnaire about which treatment the patents received to evaluate the success of blinding at the last visit.
Target plaque selection and analysis by DSCTA
The target plaque to be monitored will be determined in NCP or MP on the main coronary vessel (diameter of the target vessel is ≥2.5 mm such as LAD, CX and/or RCA), and the diameter stenosis is between 30% and 70%. The distance from the target plaque to the coronary opening will be measured as a reproducible fiduciary index to guarantee the accuracy of the after-treatment measurement. The target plaque will be selected in each subject according to the standard operating procedures illustrated in the figure 2, which will be evaluated as representative effect of XAG. Investigators will be required to use the same DSCTA operating system (SOMATOM Definition Flash, Siemens Healthineers, Erlangen, Germany) for both the baseline and after-treatment DSCTA image acquisition in order to make sure that each centre can keep in same standard level in terms of data collection for DSCTA parameters. The DSCTA images of target plaque characteristics include plaque volume, CT values, degree of stenosis and calcification scores by using the same workstation (Syngo.via VB10B). The images will be logged, and quantitative analysis of DSCTA will be performed by two independent blinded experienced investigators who are blinded to the patient group allocation in the Radiology Department of Guang’anmen Hospital of China Academy of Chinese Medical Sciences so that the data assessment for DACTA parameters could be conducted within the same standard for each centre. We will use kappa test to evaluate the consistency of the results of the two investigators.

Flow chart of target plaque selection.
Interventions
Eligible patients will be allocated to receive XAG or placebo granules for 6 months randomly using CRS, based on routine medications including lipid-lowering, antiplatelet, antihypertensive or antidiabetic therapy.3 Eligible participants are prohibited from using other TCM therapies for treating BCL. The XAG and placebo granules (7.72 g/bag, one bag at a time, two times per day, 6 months) will be provided by Sichuan New Green Pharmaceutical Technology Development Co. Ltd. (Peng Zhou, China). Both XAG and placebo have the same outer packaging, colour, shape and flavour, so that neither the participant nor the investigator could recognise which group of intervention the participants are receiving before unblinding. After the treatment, the packaging will be returned to the investigators.
Data collection
Background information
Background information includes demographic data and general clinical data, which will be recorded during the 1-week screening period. Demographic data consists of gender, age, height, weight and so on. General clinical data consists of medical history, course of disease, treatment history, combined diseases, concomitant medications and so on. The participants’ information and privacy will be strictly protected and forbidden to the public.
Safety outcomes
Safety is assessed by vital signs, laboratory examinations and AEs. Vital signs include body temperature, breathing, blood pressure and heart rate. Laboratory examinations include blood, urine and stool routine, liver and kidney function. AEs will be recorded all the time during the treatment. The development of AEs will also be observed until the adverse reactions disappear.
Primary and secondary outcomes
The primary outcome measures of the study are plaque characteristics including target plaque volume, degree of stenosis, CT value and calcification score measured by DSCTA, which will be measured at baseline and 6 months after randomisation. Secondary outcomes include the efficacy of angina symptoms, Seattle Angina Questionnaire (SAQ), which will be recorded at baseline and every month during the treatment period (1 to 6 months after randomisation), blood lipid indicators, including cholesterol, triglycerides, low-density lipoprotein and high-density lipoprotein, and high-sensitivity C-reactive protein (hs-CRP) which will be recorded at baseline, 3 months and 6 months after randomisation. At the same time, the trial also observes the occurrence of MACEs defined as the composites of deaths from any cardiac causes, myocardial infarction and revascularisation (PCI or CABG) at 9 months and 12 months after randomisation. Items to be measured and the time window of data collection are shown in table 3.
Schedule of data collection
Sample size calculation
The formula used to calculate the sample size is as follows, which is based on superiority clinical trial interval hypothesis test sample size estimation29. The sample size was calculated on the basis of expected reduction in plaque volume. One previous study suggested that the reducing value for plaque volume after interventional treatment is 1 mm3, and the combined SD is 2.75 mm3. Therefore, we assume the reduction in plaque volume as 1 mm3 in this study. In the following formula, c is the ratio between two sample cases.  , so c=1. σ is the combined SD and δ is the expected effect size, so σ=2.75, δ=1. Given a type I error rate of α = 0.05, a power of 90 % (type II error rate of β = 0.1), so
, so c=1. σ is the combined SD and δ is the expected effect size, so σ=2.75, δ=1. Given a type I error rate of α = 0.05, a power of 90 % (type II error rate of β = 0.1), so  =1.64,
=1.64,  =1.28. n1=n2≈128, the sample size for one group needs to be 128, resulting n=2×128=256 patients. Considering the maximum possible dropout rate is 15%, a total of 294 patients need to be allocated to reach the required number of patients for the efficacy analysis. For convenience of randomisation, we decided to recruit 300 patients.
=1.28. n1=n2≈128, the sample size for one group needs to be 128, resulting n=2×128=256 patients. Considering the maximum possible dropout rate is 15%, a total of 294 patients need to be allocated to reach the required number of patients for the efficacy analysis. For convenience of randomisation, we decided to recruit 300 patients.


Adverse events
AEs are defined as negative or unintended clinical manifestations following the treatment. Patients will be asked to report to the investigators any abnormal reactions occurring at any time during the trial. In addition, investigators will collect information about abnormal reactions monthly. All details of related and unexpected AEs, such as time of occurrence, degree and duration of AEs, suspected causes and the effective measures and outcomes will be recorded on eCRFs. Any AEs, such as subjective discomfort and laboratory abnormalities, should be taken seriously. Careful analysis and immediate measures are taken to protect the safety of the subjects until the adverse events disappeared. There is also a data safety monitoring board to oversee the trial.
Quality control of data
eCRFs will be used for data collection, and data from all participating centres will be imported into public clinical trial management platform (www.medresman.org) within 6 months after the trial completes. To maintain the quality of the data, we will adopt valid measures to ensure information accuracy, integrity and authenticity. First, all investigators will receive pretrial training on patients screening, data filling, medication use, AEs reporting and other matters. Second, a trial inspector will visit each site regularly to check the electronic database and ensure the trial is strictly following the protocol. Third, the Data Coordination Center will be in charge of data validation. Fourth, the researchers should take measures to control the incidence rate of drop-out within 15%.
Planned analysis
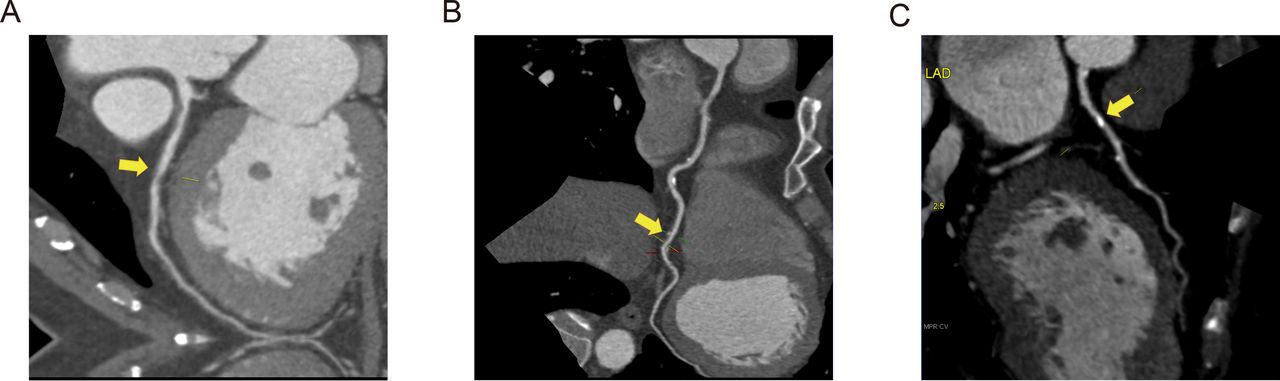
All the efficacy and safety analyses will be conducted within the full analysis set (FAS) according to the intention-to-treat principle, with all randomly assigned participants included. Furthermore, we will also conduct the per-protocol set (PPS) analysis to compare the results from FAS and PPS. The data from all participating centres will be combined for statistical analysis of the primary and secondary outcomes as well as AEs. Demographic and laboratory characteristics will be calculated at baseline and after-treatment period for all patients. The primary endpoint will be analysed by the absolute change in DSCTA-defined total plaque volume and degree of stenosis within the target segment, CT value and calcification score measured by DSCTA workstation from baseline to follow-up. A safety analysis will be performed in all patients. The analysis will be done at Guang’anmen Hospital, China Academy of Chinese Medical Sciences in Beijing. Continuous variables will be expressed by mean ±SD; categorical variables will be shown as counts and percentages. Whether the hypothesis of superiority is available will be judged by comparing the 95% CI of the difference in intergroup efficacy. The comparability of the characteristics between the two study groups will be assessed by using t-test for continuous variables with normal distribution, while the non-parametric Mann-Whitney-Wilcoxon test will be used for the comparison of data with non-normal distribution. Specifically, the paired t-test will be used to compare the difference of the outcome between preintervention and postintervention in each group and independent t-test will be used to compare the difference between the two groups. Categorical variables will be compared using Χ2 statistics, while the Fisher exact test will be used when the theoretical frequency is less than 5 in more than 25% of the cells. In order to control the centre and baseline effects, covariance analysis will be applied for the intergroup comparison with continuous variables and Cochran-Mantel-Haenszel test for categorical variables. We will also use the Bonferroni test for multiplicity correction of the change in each of four parameters (total plaque volume, degree of stenosis, CT value and calcification score). We will also conduct the subgroup analyses stratified by whether or not the participant is receiving statin therapy at the time of randomisation and by subtypes of the target segment of coronary plaque determined by DSCTA. The subtypes include NCP, calcified plaque (CP) and MP, as shown in figure 3. All statistical tests are unilateral test, p<0.05 will be considered as statistically significant. All statistical analyses will be performed using SPSS V.20.0.
{kind=link}
{kind=link}
{kind=link}
Subtypes of coronary plaques determined by dual source CT angiography A reflects non-calcified plaque, B reflects mixed plaque, C reflects calcified plaque.
Ethics and dissemination
This trial has been registered at Chinese Clinical Trial Registry http://www.chictr.org.cn/. The data of this trial will be managed by ResMan at http://www.medresman.org/ and posted on Chinese Clinical Trial Registry. The results of this study will be disseminated to the public through academic conferences and peer-reviewed journals.
Discussion
Most of the plaques in BCL are thin-cap fibroatheromas or characterised by a large plaque burden, also called vulnerable plaques,4 which may progress to ACS easily. The main pathogenesis of myocardial infarction is the rupture of vulnerable plaques and thrombosis.30 31 Coronary atherosclerotic plaque assessment provides improved discrimination of ischaemia compared with stenosis assessment alone.32 Coronary artery angiography is considered as the gold standard for diagnosis of coronary artery stenosis.33 However, it cannot observe the characteristics of plaque. DSCTA, a non-invasive testing, is widely used in clinical practice, which can not only measure the degree of coronary artery stenosis but also measure plaque compositions. As the primary outcome indicators, target plaque volume, degree of stenosis, CT value and calcification score can not only reflect the size of the plaque but also reflect the stability of the plaque. CT value demonstrates the density of the plaque. The vulnerable lesions demonstrate low-attenuation plaques and NCP with <30 HU (CT value) density identified by multislice CT.34 35 In this study, we will investigate whether XAG has the effect on relaying or reversing plaque progression by reducing plaque volume and stabilising plaque via turning NCP and MP into calcified plaque (figure 3).
Integrative medicine, combined TCM with routine medicine, emerges as an optimal approach for achieving better effectiveness in patients with BCL. As a supplementary and complementary medicine, TCM is attracting our attention. With lifestyle and dietary changes, the number of patients with obesity and abnormal lipid metabolism increase significantly. In TCM studies, the level of low-density lipoprotein cholesterol was obviously increased in BCL patients with ‘intermingled phlegm and blood stasis’ syndrome.36 People are getting more and more anxious under increasing pressure, which is related to ‘heat’ syndrome in TCM theory. ‘Phlegm, blood stasis and heat syndrome’ is the core pathogenesis in patients with BCL. XAG has the effect of ‘clear up heat, resolve phlegm and promoting blood circulation’. As the principal active components, pharmacological studies have shown that salvia miltiorrhiza could perform the function of antioxidation, adjusting lipid metabolism, inhibiting thrombosis and expanding the coronary artery.19 20 Panax notoginseng is reported to protect vascular endothelial cells against hypoxia and have the antiatherosclerotic, lipid-lowering, antiplatelet aggregation and antithrombosis effects.21 Previous studies have shown that coptis chinensis can stabilise plaque by anti-inflammatory therapy.22 However, whether XAG is effective in the patients with BCL still requires confirmation by large-sample, multicentre and randomised controlled clinical trials. This study is a multicentre, central-randomised, double-blinded, placebo-controlled clinical trial with the objective of determining the effectiveness and safety of XAG for treating BCL.
There are also some limitations in this study. First, DSCTA is easy for investigators to operate and more acceptable to participants, but plaques with diffuse irregular calcification always produce the image artefacts of DSCTA, which might cause deviation in the degree of stenosis of CP. It is recommended that the use of Intravascular Ultrasound on the evaluation of plaque characteristics of coronary lesions would enhance the accuracy of the plaque evaluation. Second, our experiments will be conducted in three regions of China. Whether similar effects are available to other ethnic groups and regions remains uncertain.
References
Footnotes
MiH and GC contributed equally.
Contributors JW is the principal investigator of this study. MiH and GC contributed equally to the article, who conceptualised the study design and wrote the manuscript. JW, KY and JL modified the manuscript. X-jX, CL, QG and HH participated in the establishment of the eCRF. QZ, FL and XH participated in the recruitment of patients. YZ and MeH designed the method for statistic analysis. YoL, ZZ and YiL will participate in the data collection and analysis. All authors read and approved the final manuscript.
Funding This study is supported by the China Academy of Chinese Medical Sciences, and is funded by the Fundamental Research Funds for the Central public welfare research institutes (Z210-013) and National Chinese Medicine Clinical Research Foundation Construction Program of State Administration of Traditional Chinese Medicine of the People’s Republic of China (No.JDZX2015248).
Competing interests None declared.
Ethics approval This study has been approved by Research Ethics Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences in Beijing, China (No. 2017-083-KY-01).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.