Article Text

Abstract
Introduction Survivors of critical illness frequently exhibit acute and chronic neurological complications. The underlying aetiology of this dysfunction remains unknown but may be associated with cerebral ischaemia. This study will use near-infrared spectroscopy to non-invasively quantify regional cerebral oxygenation (rSO2) to assess the association between poor rSO2 during the first 72 hours of critical illness with delirium severity, as well as long-term sensorimotor and cognitive impairment among intensive care unit (ICU) survivors. Further, the physiological determinants of rSO2 will be examined.
Methods and analysis This multicentre prospective observational study will consider adult patients (≥18 years old) eligible for enrolment if within 24 hours of ICU admission, they require mechanical ventilation and/or vasopressor support. For 72 hours, rSO2 will be continuously recorded, while vital signs (eg, heart rate) and peripheral oxygenation saturation will be concurrently captured with data monitoring software. Arterial and central venous gases will be sampled every 12 hours for the 72 hours recording period and will include: pH, PaO2, PaCO2, and haemoglobin concentration. Participants will be screened daily for delirium with the confusion assessment method (CAM)-ICU, whereas the brief-CAM will be used on the ward. At 3 and 12 months post-ICU discharge, neurological function will be assessed with the Repeatable Battery for the Assessment of Neuropsychological Status and KINARM sensorimotor and cognitive robot-based behavioural tasks.
Ethics and dissemination The study protocol has been approved in Ontario by a central research ethics board (Clinical Trials Ontario); non-Ontario sites will obtain local ethics approval. The study will be conducted under the guidance of the Canadian Critical Care Trials Group (CCCTG) and the results of this study will be presented at national meetings of the CCCTG for internal peer review. Results will also be presented at national/international scientific conferences. On completion, the study findings will be submitted for publication in peer-reviewed journals.
Trial registration number NCT03141619
- near-infrared spectroscopy
- cerebral autoregulation
- kinarm
- delirium
- post-intensive care syndrome
- rbans
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Our study will further assess the association between poor regional cerebral oxygenation (rSO2) and delirium, as well as long-term cognitive outcomes among survivors.
Although this study is observational in nature, which limits causal inferences, broad inclusion criteria and a representative sample size will increase external validity of our findings.
This study closely resembles routine clinical practice with only minor methodological differences (eg, rSO2 monitoring) and results will have the potential to directly translate into clinical practice.
Introduction
Medical advancements in the intensive care unit (ICU) has led to a substantial reduction in mortality rates.1 2 However, survivors frequently experience postintensive care syndrome, which is characterised by cognitive, psychiatric and physical impairments.3 These complications have profound effects, including long-term cognitive impairments affecting between 25% and 75% of survivors,3 and an approximately 50% decrease in full-time employment.4 Therefore, modern critical care research should improve our understanding of, and the prevention of, long-term impairments in the growing number of ICU survivors.
A recent systematic review identified prolonged delirium as the most consistent and potentially modifiable risk factor for long-term cognitive impairment.5 Patients with delirium experience persistent deficits in various domains, including: memory, executive function, verbal fluency and attention.6–8 Furthermore, robotic technology, known as the KINARM, which uses the participant’s upper limbs to asses sensorimotor and cognitive function, has indicated that ICU survivors also develop visuospatial and motor deficits.9 Importantly, when assessed using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS), many critical illness survivors had performance scores similar to patients with moderate traumatic brain injury or mild Alzheimer’s disease, with a duration-dependent effect of delirium on impairments in global cognition and executive function.6
Delirium is characterised by reduced awareness, emotional disturbances, restlessness and incoherence with a 60%–87% ICU incidence rate.10 While risk factors associated with delirium include mechanical ventilation, age and frailty,10 the underlying aetiology of delirium is poorly understood. Cerebral ischaemia is thought to play a central role in delirium development; however, understanding this relationship presents several challenges due to the difficulty of continuously measuring cerebral perfusion in the ICU.
Therefore, there is a paucity of studies investigating the influence of cerebral perfusion on delirium in critically ill patients (Reviewed in11). Near-infrared spectroscopy (NIRS) is a non-invasive technology that measures regional cerebral oxygenation (rSO2) as a surrogate marker of cerebral perfusion,12 13 as rSO2 values correlate with other markers of cerebral perfusion, including CT perfusion, jugular venous bulb oxygen saturation and brain tissue oxygen tension.12–14 Therefore, NIRS is an ideal candidate for both ICU research and clinical practice.
Feasibility and single-centre prospective ICU studies have been performed with NIRS, discovering that low rSO2 is an independent risk factor for the development of delirium.15 16 A nested cohort in this study demonstrated that impaired cerebral autoregulation (ie, the ability to maintain stabilised and adequate cerebral perfusion) is also associated with the development and duration of delirium.17 18 While these findings were statistically significant, a multicentre observational study is necessary for external validation and the study of long-term outcomes.
Our overarching hypothesis is that decreased rSO2 in the early stages of critical illness leads to the development of delirium, as well as long-term cognitive impairment among survivors. The primary objective is to further establish an association between poor cerebral perfusion and delirium severity. Secondary objectives include assessing the haemodynamic and physiological determinants of rSO2, as well as to identify potential risk factors (eg, poor rSO2) associated with delirium and long-term cognitive deficits. Overall, elucidating the mechanisms of acute and chronic neurological impairment will allow for the development of preventative treatments to improve outcomes among ICU survivors.
Methods and analysis
Patient and public involvement: At Kingston Health Sciences Centre (KHSC), our staff includes a patient experience advisor who is a critical care nurse that has been previously admitted with respiratory failure and shock. This experience as a front-line healthcare professional, as well as an ICU patient, will be invaluable to both patient and public involvement. In addition to the scientific community, patients and their families will also be central to the dissemination of our findings. Participants that selected to be informed of the results will be mailed/emailed the published findings on study completion.
Study locations and participants: An overall visual schematic of the study design is shown in figure 1. This prospective observational study will take place at five sites within Ontario, Canada. KHSC will serve as the coordinating centre, as the ICU has a history of coordinating academic and industry funded studies and the staff are familiar with the Cerebral Oxygenation and Neurological outcomes FOllowing CriticAL illness (CONFOCAL) protocol, as the pilot study16 was conducted at this site. Patients are considered eligible if they are ≥18 years old, have been admitted to the ICU >24 hours and have respiratory failure requiring invasive mechanical ventilation with an expected duration >24 hours, and/or have shock of any aetiology. Shock will be defined by the need for one of the following vasopressors/inotropes: dopamine ≥7.5 μg/kg/min, dobutamine ≥5 μg/kg/min, norepinephrine ≥5 μg/min, phenylephrine ≥75 μg/min, epinephrine at any dose, milrinone at any dose (if used in conjunction with another agent), vasopressin ≥0.03 U/min (if used in conjunction with another agent), which is adapted from the BRAIN-ICU inclusion criteria.6 The exclusion criteria are admission to the ICU >24 hours, a life expectancy <24 hours, a primary central nervous system admitting diagnosis (eg, traumatic brain injury, stroke, subarachnoid haemorrhage), and/or any reason that the subject may not be able to participate in the follow-up assessments (eg, limb amputation, paresis, neuromuscular disorders). Postcardiac arrest patients are also excluded from this study. Additional study sites will include the following: London Health Sciences Centre-Victoria Hospital (London, ON; Site PIIan Ball, with co-PIs Dr. Marat Slesserev and Niamh O’Reagan), Ottawa General Hospital (Site PI Shane English), and Ottawa Civic Hospital (Site PI Shane English). KHSC is responsible for developing and maintaining the electronic case report forms (eCRFs), data management and analysis.

A visual representation of the CONFOCAL2 study design from enrolment to 3 and 12 months follow-up assessments. APACHE II, Acute Physiology and Chronic Health Evaluation II; Hb, haemoglobin; ICU, intensive care unit; NIRS, near-infrared spectroscopy; pCO2, partial arterial pressure of carbon dioxide; pO2, partial arterial pressure of oxygen; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status.
Potential non-Ontario site expansion: We are anticipating an enrolment rate of 1–2 patients per site/month. Should our enrolment rates be slower than anticipated, additional sites have already agreed to participate in this study, including: Toronto Western Hospital (Site PI Victoria McCredie, Université de Montreal (Montreal, QC; Site PI Michael Chasse) and Vancouver General Hospital (Site PI Donald Griesdale). Local ethics approval would be sought prior to enrolment in this study.
Recruitment and consent: All patients admitted to the ICU will be screened daily for eligibility. The participant will be approached by a member of the research staff. If the participant is unable to provide consent, the research staff will approach the substitute decision-maker (SDM). The research coordinator or trained study staff will obtain informed consent and documentation of the consent process will be noted in the patient’s medical chart. As patients meeting eligibility criteria are unlikely to be able to give informed consent at the time of enrolment due to their critical condition, we will employ a deferred consent model when appropriate (eg, SDMs are frequently in an emotional state and may not be available to be contacted), which has already been granted local research ethics board approval. When an SDM is not available to approach, we will enrol the patient and begin trial procedures until the SDM is available for a consent encounter, targeted to be within 72 hours of enrolment. However, we will encourage an a priori informed consent whenever possible. The SDM response will be used to continue all trial procedures or any further data collection. If the patient or SDM declines enrolment, then the patient will be excluded, and all data obtained using deferred consent will be confidentially destroyed. In addition, once the patient has regained capacity according to the medical team, the patient will be approached to affirm or withdraw consent. Each site will be provided with patient identification numbers, which will be assigned sequentially when a patient is enrolled and will be used in all study documentation to ensure patient confidentially and anonymity. All eligible patients will be recorded on a screening log, which will include their study ID, date of consent or reason the patient could not be enrolled. The de-identified screening log will be forwarded to the lead project coordinator on a monthly basis. The individual site research coordinators and investigators will be responsible for ensuring the ethical conduct of this trial, screening patients, obtaining consent and training of staff as needed. The principal investigators and coinvestigators will review monthly compliance with the study protocol and recruitment rates.
Confidentiality: To ensure patient confidentiality, identifying information will not be collected on the CRF. Patients will be identified to the coordinating centre only by their unique study identification number. The site study coordinator will maintain a participant master list including the participant name and linked study ID. At the end of the study, this master list will be destroyed. In accordance with current requirements, we will store the de-identified data for a minimum of 10 years.
Data collection
rSO2, haemodynamics, medications and clinical characteristics: Patients will be enrolled within the first 24 hours of their ICU admission. Immediately following enrolment, the patient will undergo rSO2 monitoring. A sensor will be placed in the centre of the patient’s forehead, which is attached to the FORESIGHT ELITE oximeter (CASMED, Caster Medical, Canada). This device will provide continuous quantification of rSO2, every 2 s, for 72 hours. To assess the association between haemodynamics and rSO2 recordings, we will use a commercially available system (Bedmaster, Excel Medical Electronics, Florida, USA; or site equivalent) to capture the following vital signs from enrolled patients: heart rate (HR), systolic blood pressure, diastolic blood pressure , mean arterial pressure (MAP) and peripheral oxygen saturation (SpO2). These data are captured locally and uploaded to the eCRF Research Electronic Data Capture (REDCap). Throughout this 72 hours period of recording, we will document administered continuous infusion and intermittent bolus doses of vasoactive and sedative/analgesic medications, which will be converted to either ‘fentanyl equivalents’ for narcotics or ‘midazolam equivalents’ for benzodiazepine medications. These conversion formulas have been previously described.19 Severity of illness will be measured during the first 24 hours of ICU admission using the Acute Physiology and Chronic Health Evaluation II score (APACHE II). Trained research staff will approach whomever provided informed consent (ie, either the patient or the SDM) to ascertain the enrolled patient’s pre-existing frailty (ie, prior to ICU admission) using the clinical frailty scale,20 which is 9-point scale (eg, 1=very fit to 9=terminally ill). All clinical data will be captured on the eCRF.
Central venous and arterial blood collection: Both arterial and central venous gases will be sampled every 12 hours during the 72 hours period of rSO2 recording and will include: pH, pO2, pCO2 and haemoglobin (Hb) concentration. These blood samples will be collected only if a central line (peripherally inserted central catheter, internal jugular, subclavian) and arterial line are already in place.
Delirium screening: Patients will be assessed once daily for delirium throughout their entire hospital stay (ICU and ward; up to day 30) using validated screening tools; the confusion assessment method (CAM)-ICU,21 as well as the brief CAM22 which will be administered on the ward. Both delirium screening tools will be administered by trained research staff at a time that is convenient for the patient, their family and the medical team directing their care.
From the CAM-ICU, the CAM-ICU 7 (ie, 7-point delirium severity scale) will also be documented (ie, 0–2: no delirium, 3–5: mild to moderate delirium and 6–7: severe delirium).23 The ICU discharge day will be considered to be the day that the attending writes orders to discharge, in order to avoid the influence of delayed discharge.
Determination of pre-existing cognitive impairment: Our pilot study16 excluded 10% of patients with a documented history of cognitive impairment in their medical chart, which may limit external validity. Importantly, individuals may have substantial cognitive impairment prior to enrolment but did not receive any formal diagnosis. To address this potential confound, all patients will be assessed, on enrolment, using the Clinical Dementia Rating (CDR) scale.24 The CDR is a scale from 0 (normal) to 3 (severe dementia) that is calculated from a standardised scoring sheet completed by interviewing a patient or their caregiver. All staff completing the interview and scoring sheet will undergo rigorous online training and pass a certification exam. A diagnosis of pre-existing cognitive impairment will be defined as a CDR >1.
3 and 12 months follow-up
Neuropsychological assessment:RBANS: Participants will complete a 3 and 12 months follow-up assessment in which the RBANS will be administered by a trained researcher. The RBANS assesses global cognition, as well as several subdomains (ie, immediate and delayed memory, visuospatial/constructional, language and attention). These indices have been described previously,25 and survivors will be compared with age-matched controls. To improve follow-up rates, in home/hospital testing will be performed for individuals not able to return for laboratory assessment. Participant scores are converted to standardised values in which the normative range will be considered a mean of 100±24.75 (1.65 SD). Participants that score >75 will not be considered impaired, as these subjects are performing within or above the normative range. The RBANS assessment requires ~20–30 min to complete.
KINARM assessment: Participants (from the Kingston region only) will complete a 3 and 12 months follow-up assessment using the End-Point bimanual KINARM robot (BKIN Technologies, Kingston). With each hand, the seated subject grasps a handle attached to a planar robotic device that permits movements in the horizontal plane with an integrated virtual reality system that presents objects in the horizontal plane (figure 2). Subjects will perform a behavioural battery to quantify a broad range of sensorimotor, and cognitive function using their upper limbs. A trained operator selects a task from the software menu, reads the standardised instructions, and then monitors performance in real time. We will administer eight tasks from the KINARM Standard Tests including: object hit,26 object hit and avoid,27 ball on bar,28 visually guided reaching (VGR),29 reverse VGR,30 spatial span, trail making A and B, and arm position matching.31 Each task has been previously described,32 and quantifies subject performance using approximately 6–12 metrics per task. Each metric is converted into normalised units based on healthy subject performance, considering the influence of sex, age and handedness (0 is mean performance and ±1 is a SD from the mean). For each task, a task score will also be generated to provide a global performance measure with values that are equivalent to SD units with zero specifying best possible performance, and higher values indicating worse performance. Therefore, performance will be considered abnormal if the task score is outside the +1.96 range (ie, 5th percentile). The task score has been previously described.33 The KINARM assessment takes ~45 min to complete.

Three-dimensional animated representation of the KINARM endpoint robotic set-up used at 3 and 12 months follow-up assessments.
Statistical plan
Quantification of disturbed cerebral autoregulation: Cerebral autoregulation will be evaluated by computing customised algorithms (MATLAB, MathWorks, Massachusetts, USA) of the time-varying Spearman’s correlation coefficients between rSO2 and MAP (ie, Cerebral Oximetry Index, COx) with a moving time window advanced in 1 min steps over the 72 hours period of recording. This cerebral autoregulation assessment has been previously described18 and a visual representation can be observed in figure 3. In addition, we will perform the COx across varying window lengths to further assess the optimal window length of recording (eg, 5, 10, 30, 60, 120, 240, 300 min windows). Positive COx values (ie, MAP and rSO2 move in the same direction) reflect dysfunctional cerebral autoregulation, whereas negative (ie, MAP and rSO2 move in the opposite direction) and near zero (<0.3) indicate intact cerebral autoregulation. However, we will define cerebral autoregulation dysfunction by using a statistical significance threshold for positive COx correlation values (p<0.0001). Cumulative duration of disturbed autoregulation will be given by the duration of time spent with a significant positive correlation throughout the period of neuromonitoring. Computer algorithms for COx will be developed and implemented blind to the neurological status of enrolled patients.
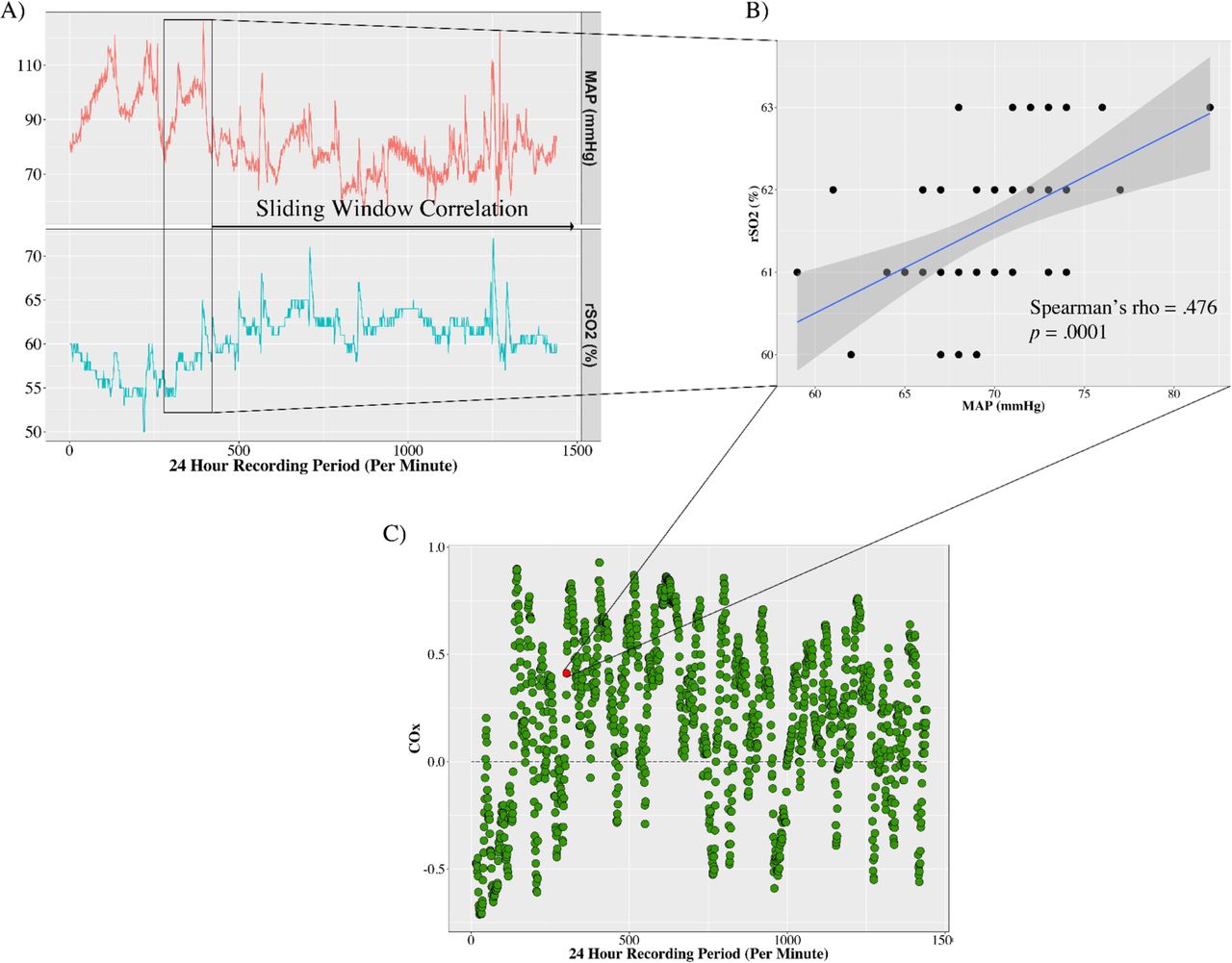
(A) Simplified line graph (24 hours instead of the full 72 hours recording period) illustrating the sliding window correlation between mean arterial pressure (MAP) and regional cerebral oxygenation (rSO2) for an individual patient over a 24 period of recording. The black rectangle represents a 60 min window that moves forward 1 min at a time until the recording period is completed. (B) Scatter plot illustrating a time dependent positive association between MAP and rSO2. Black dots represent data collected for an individual patient over 24 hours, with the blue line representing a linear model fit to the data, and the grey shaded region representing the 95% CI. (C) Scatter plot indicating the time varying association between MAP and rSO2 represented as the Cerebral Oximetry Index (COx) over an individual patient’s 24 hours recording period. Statistically significant (p<0.0001) positive COx values represent dysfunctional cerebral autoregulation, with negative or near zero values indicating intact cerebral autoregulation.
Estimating optimal MAP (MAPOPT): To calculate the individualised MAPOPT, the computed COx values will be binned by the average MAP value in their respective moving windows in 5 mm Hg bins.34 An alternative strategy will also be implemented. We will invert the MAPOPT binning procedure by binning MAP values by their corresponding COx values in sequential 0.05 bins of Spearman correlation coefficients ranging from −1 to +1. This procedure has been previously described.18
Assessment of primary outcome: Multivariate linear regression will be used to characterise the association between adequate cerebral perfusion (as measured using duration of time (minutes) outside of MAPOPT, mean rSO2 and duration of disturbed cerebral autoregulation) and delirium severity throughout a patient’s ICU stay to determine if poor cerebral oxygenation is an independent predictor of delirium. We will estimate the unadjusted effect of each individual predictor on delirium severity (ie, cumulative CAM-7 scores per patient). The simultaneous multivariate regression model will adjust for the following covariates due to their potential associations with delirium: a history of hypertension, a history of alcohol abuse, total sedative dose (in midazolam equivalents), total narcotic dose (in fentanyl equivalents), severity of illness (APACHE II scores), pre-existing cognitive impairment (CDR score), length of ICU stay, frailty, (clinical frailty scale) and blood urea nitrogen. The multivariable model will provide the adjusted regression coefficients after controlling for all predictors included in the model. All covariates included in regression modelling have been chosen a priori based on clinical judgement and previous research.16 35 Model diagnostics will be conducted to assess the underlying assumptions of linear regression (ie, linearity, normally distributed residuals, equal variances and lack of multicollinearity) for all models. Multiple imputation strategies will be applied at the time of the regression modelling to account for any missing data and reduce bias associated with excluding patients due to partially collected data.
Secondary outcomes
Determinants of rSO2 : To assess the haemodynamic and physiological determinants of rSO2 at the patient level, multiple linear regression will be performed using the patient average of each variable over the 72 hours data collection period. The following predictors will be included in the regression model: HR, SpO2, MAP, arterial and venous blood gas data (ie, pH, pO2 and pCO2), central venous oxygen saturation and Hb concentration. In addition, the multivariate model will control for the following covariates associated with cerebral perfusion: age,36 as well as total sedative, narcotic and vasopressor dosing. Simultaneous multiple linear regression with adjustment for all aforementioned covariates will be implemented. As stated for the primary outcome regression analysis, model diagnostics will be performed. Furthermore, the relationship between the determinants of the NIRS-derived rSO2 signal may vary over time (see figure 4 and online supplementary movie 1). Therefore, a repeated measures analysis will also be performed by using multilevel modelling with six observations reflecting each 12-hour period during the 72 hours data collection period (with time coded as 0–5, so the intercept equals baseline/time of enrolment) nested within each subject. The predictors will be the same as the regression model but allowed to be time varying across the six observation points. This analysis will assess if within patient changes in the predictors correlate with changes in rSO2, and if these associations are modified by fixed patient characteristics, such as age.
Supplemental material

Line graph of the high frequency vital sign recordings indicates the highly variable relationships with regional cerebral oxygenation over the 72 hours period of recording. The figure represents a single patient’s ICU recording. artMAP, mean arterial pressure from an arterial line; HR, heart rate; ICU, intensive care unit; rSO2, regional cerebral oxygenation; SpO2, peripheral oxygen saturation.
Assessing if poor cerebral perfusion during critical illness is a significant predictor of long-term neurological dysfunction among ICU survivors: Multiple linear regression analysis will be used to assess if impaired cerebral perfusion (ie, time below MAPOPT, mean rSO2 and duration of disturbed cerebral autoregulation) is associated with RBANS global cognition scores at 3 and 12 months post-ICU discharge. We will use the following clinical covariates collected on admission (ie, pre-existing cognitive impairment, age, severity of illness, frailty) and data collected within the first 72 hours of the patients’ ICU stay (ie, narcotic dosing and benzodiazepine dosing). All covariates will be adjusted for in separate regression models for the cognitive outcomes at 3 and 12 months post-ICU discharge. If global cognition is significantly predicted by the time below MAPOPT, we will conduct an exploratory analysis of the RBANS subdomains of cognition (ie, delay and immediate memory, language, attention, visuospatial/constructional) adjusting for the aforementioned covariates to further explore specific areas of impairment observed among survivors of critical illness. Due to the limited availability of the KINARM robot across sites, only patients assessed at KHSC will undergo KINARM testing.This data will be assessed with descriptive statistics only to avoid any potential bias introduced by this design.
Sample size calculation
Primary outcome: Our overall hypothesis is that poor cerebral perfusion contributes to delirium and long-term cognitive impairment. For study purposes, we define poor cerebral perfusion as the composite of (1) low mean rSO2, (2) duration of impaired cerebral autoregulation and (3) time outside individualised optimal MAP MAPOPT, which will be discussed in more detail in the statistical plan section. We acknowledge that this is an imperfect measure of cerebral perfusion. However, this is a comprehensive, continuous and non-invasive assessment of cerebral perfusion. For our primary outcome (CAM-7 delirium severity score), we will enrol a total of 500 patients, as our prior work has demonstrated that ~20% of patients remain comatose (RASS=−4 or −5) during their entire ICU stay,16 and cannot be assessed for delirium. Therefore, using our pilot data, we estimate that ~100 patients will be remain comatose resulting in approximately 400 patients to assess our primary outcome, which will allow for 10 df for our 3 measures of perfusion (ie, mean rSO2, duration of disturbed cerebral autoregulation, duration outside MAPOPT) and controlling for the nine covariates (see below). The 10 df will allow us to model non-linear relationships between the 3 measures of cerebral perfusion and delirium severity. This sample size achieves 90% power to detect an R2 of 0.050 collectively among these measures of cerebral perfusion and using an F-test with a significance level (alpha) of 0.050 (see figure 5).

{kind=link}
{kind=link}
{kind=link}
![[bmjopen-2019-029189supp001.jpg]](https://bmjopen.bmj.com/content/bmjopen/9/6/e029189/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
A power curve indicating the study sample size, and the respective statistical power, to asses the primary study outcome. Red dots represent the sample size needed for a given statistical power. The primary sample size was calculated using the following multivariate regression model parameters: 10 independent variables tested, controlling for 9 additional covariates, power=0.90, R2=0.050, α=0.05, which would require a sample size of 400.
Secondary outcomes: physiological determinants of rSO2 and neurological outcomes
For evaluating the determinants of the rSO2 signal during critical illness, we will assess the association between each of the nine prespecified candidate predictors of rSO2 after controlling for the four covariates (see below for covariates). We will use a Bonferroni correction (0.05/9=0.0056) to control for multiple testing. With the total 500 patients recruited, and a multivariate regression model that includes 13 independent variables, this testing strategy will provide 90% power to identify any predictor that explains an additional 3.2% of the variance of rSO2 after controlling for the other variables in the model. This sample size is sufficient to identify independent significant predictors that account for a small-moderate degree of variance in the overall rSO2 signal. However, our pilot data indicated a 30% mortality rate. Given our overall sample size of 500 patients recruited, we are anticipating ~350 ICU survivors (ie, 500–150) to return for follow-up assessment. This cohort will provide sufficient power to detect important predictors of long-term neurological outcomes. However, these predictors have been intentionally not specified a priori, as this analysis will be dependent on our findings related to cerebral perfusion and delirium.
All sample size calculations were conducted using Power Analysis and Sample Size Software (V.15).37
The actual start date at KHSC began on 26 January 2018 and our estimated primary completion data is June 2022. Due to our 12-month follow-up, we expect the study to be completed June 2023.
Discussion
This multicentre observational study will extend our preliminary findings of reduced rSO2 as an independent risk factor for the development of delirium during critical illness. With the proposed larger sample size, we will not only be able to replicate and validate this completely novel finding, but we will also be able to further characterise the physiological determinants of rSO2 in a representative cohort. Furthermore, this study will have the potential to identify novel pathophysiological mechanism associated with the development of delirium and long-term neurological dysfunction among ICU survivors. These findings will inform the next phase of this research programme: a proof-of-principal study, aimed at devising strategies to optimise rSO2. It will lay the foundation for a larger interventional study designed to assess whether optimisation of rSO2 can reduce delirium and improve long-term neurological outcomes for patients.
Ethics and dissemination
Risks/ethical considerations: Ethics approval will be obtained prior to the commencement of screening and enrolment at each site. There are no assumed risks associated with the proposed assessment procedures, as this study only involves a small amount of blood work, which will only be collected if a central line and arterial line are already in place. Furthermore, results from our pilot study demonstrated that non-invasive monitoring of cerebral oxygenation, while using a deferred consent model, does not interfere with patient care or management.15 Research participants and their SDMs will be informed that enrolment in this study will not affect their care in any way, and that they have the right to refuse participation or withdraw at any time.
Dissemination of results: The results of this study will be presented at national meetings of the Canadian Critical Care Trials Group. Prior to submitting any manuscript for publication, it will undergo rigorous internal peer review by this group of critical care experts. Our study group has a long track record of presenting our data at national and international critical care conferences. We anticipate the preliminary results of this research programme will also be presented at these conferences (eg, American Delirium Society). The final study results will be submitted for publication to high-impact journals.
Acknowledgments
The authors would like to thank the study coordinators, MH, Ilinca Georgescu and Tracy Boyd, as well as the entire KHSC ICU staff for their continued support of our clinical research. This manuscript underwent an internal peer-review process with the Canadian Critical Care Trials Group, and we are greatly appreciative of the helpful contributions made by both Dr. Lisa Burry and Dr. Pierre Cardinal. We would also like to thank the KINARM technologists, Simone Appaqaq, Kim Moore and Helen Bretzke.
References
Footnotes
Contributors MDW participated in study design, statistical planning and drafting of the manuscript. JK participated in study design and drafting of the manuscript. KFHL participated in study design and drafting of the manuscript. DMM participated in study design and drafting of the manuscript. JM participated in study design and drafting of the manuscript. MH participated in study design and drafting of the manuscript. SHS participated in study design and drafting of the manuscript. AD participated in sample size calculations and finalising of the statistical plan. JAJ participated in statistical planning and drafting of the manuscript. IB participated in study design and drafting of the manuscript. MS participated in study design and drafting of the manuscript. NO participated in study design and drafting of the manuscript. SWE participated in study design and drafting of the manuscript. VM participated in study design and drafting of the manuscript. MC participated in study design and drafting of the manuscript. DG participated in study design and drafting of the manuscript. JGB is the primary investigator. He participated in study design and drafting of the manuscript.
Funding This work was supported by the Physician Services Incorporated and the Southeastern Ontario Academic Medical Organization New Clinician Scientist Program for which JGB was the recipient.
Disclaimer The funding agencies had no role in the design of this study, data collection or data analysis.
Competing interests JM is the scientific director of the Canadian Frailty Network. SHS is the cofounder of BKIN Technologies, the manufacturer of the KINARM device. IB receives a stipend from the Trillium Gift of Life Network to support his role as a Regional Medical Lead. NO received funding from the Academic Medical Organization of Southwestern Ontario. MS receives a stipend from the Trillium Gift of Life Network to support his role as a Hospital Donation Physician. DG is funded through a Health-Professional Investigator Award from the Michael Smith Foundation for Health Research. JGB receives a stipend from the Trillium Gift of Life Network to support his role as a Regional Medical Lead.
Ethics approval The Queen’s University and Affiliated Hospitals Health Sciences Research Ethics Board will serve as the board of record for the streamlined research ethics review system (Clinical Trials Ontario) and all Ontario sites have gained approval; non-Ontario sites will need to obtain local ethics approval at their earliest convenience.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.