Article Text

Abstract
Objectives To examine the role of hospitals and office-based physicians in empirical networks that deliver care to the same population with regard to the timely provision of appropriate care after hospital discharge.
Design Secondary data analysis of a nationwide cohort using cross-classified multilevel models.
Setting Transition from hospital to ambulatory care.
Participants All patients discharged for acute myocardial infarction (AMI) from Germany’s largest statutory health insurance fund group in 2011.
Main outcome measure Patients’ odds of receiving a statin prescription within 30 days after hospital discharge.
Results We found significant variation in 30-day statin prescribing between hospitals (median OR (MOR) 1.40; 95% credible interval (CrI) 1.36 to 1.45), hospital-physician pairs caring for the same patients (MOR 1.32; 95% CrI 1.26 to 1.38) and to a lesser extent between physicians (MOR 1.14; 95% CrI 1.11 to 1.19). About 67% of the variance between hospital-physician pairs and about 45% of the variance between hospitals was explained by hospital characteristics including a rural location, teaching status and the number of beds, the number of patients shared between a hospital and an office-based physician as well as 16 patient characteristics, including multimorbidity and dementia. We found no impact of physician characteristics.
Conclusions Timely prescription of appropriate secondary prevention pharmacotherapy after AMI is subject to considerable practice variation which is not consistent with clinical guidelines. Hospitals contribute more to the observed variation than physicians, and most of the variation lies at the patient level. To ensure care continuity for patients, it is important to strengthen hospital capacity for discharge management and coordination between hospitals and office-based physicians.
- quality of health care
- health services research
- intersectoral collaboration
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We used a nationwide data set with comprehensive patient-level information on prescriptions, hospital and ambulatory care from the largest group of statutory health insurers in Germany to examine the role of hospital, physician and patient characteristics in timely prescription of appropriate secondary prevention pharmacotherapy.
The large number of 1118 hospitals and 32 207 physicians allowed us to disentangle the variation attributable to the levels of hospitals, hospital-physician pairs and physicians and to generate reliable estimates of between-provider variation based on cross-classified multilevel models.
Since our data allowed us to represent about 32% of all hospital discharges for acute myocardial infarction (AMI) in Germany, the true number of patients treated may be larger and the coefficients on AMI volume at the hospital and physician levels must, therefore, be interpreted cautiously.
As we had no information about patients readmitted for rehabilitation services (including patients participating in cardiac rehabilitation programme) and related pharmacotherapy, these patients had to be excluded from our analysis. It is possible that statin prescription rates may differ for these patients.
Introduction
Policy interest in measuring performance in healthcare is growing, driven by demands for accountability and by strong evidence of variation in utilisation, quality and outcomes among regions1 2 and healthcare providers.3–5 However, measuring the performance of specific providers, such as individual hospitals, is difficult when aspects of their performance depend on the actions of other providers, such as office-based physicians. Since the number of patients requiring care from multiple providers or sectors is substantial and on the rise,6 it is essential to account for the relative impact of each of these when measuring quality of care.
While small-area analyses allow the quality of care to be measured at the population level, they cannot be used to identify or evaluate groups of providers who deliver care. In the present study, we therefore combined two methodological approaches—empirical patient-sharing networks and cross-classified multilevel modelling—to address this challenge from complementary angles. In USA and Canada, several studies have identified networks of hospitals and physicians that, by virtue of sharing patients, can be considered jointly accountable for the care they deliver to them.7–9 These networks were subsequently used as novel units of analysis to measure provider performance.7 Moreover, the concept of sharing patients suggests potential determinants of effective collaboration: studies in USA have found, for instance, that the number of patients shared between hospitals and outpatient physicians was, as a measure of the strength of collaboration, associated with a decreased risk of complications following prostatectomy10 and increased survival in oncological patients.11 Cross-classified multilevel modelling, in turn, provides an analytical approach to decomposing the contribution of different kinds of clusters that are not nested hierarchically to individual-level outcomes.12 Studies using this approach have, for example, examined the contextual effects of schools and neighbourhoods on smoking behaviour in USA,13 as well as the variation in medication adherence following acute myocardial infarction (AMI) that was attributable to hospitals and, respectively, local health districts in Italy.14
In our study, we draw on both of these methodological approaches to examine empirical networks of hospitals and office-based physicians in Germany with regard to their impact on the timely onset of appropriate secondary prevention following discharge for AMI. We focused on transitions from hospital to outpatient care because of evidence suggesting that gaining insights into collaboration between hospital and ambulatory care providers may be important for improving the continuity of care for patients.6 Since current clinical guidelines recommend early onset of statin therapy for secondary prevention of AMI and do not list any contraindications for this approach,15 16 we examined the prescription of statins within 30 days after discharge as an indicator of cross-sectoral quality of care. We postulated that both the hospital of discharge and the office-based physician receiving the patient could influence the timely provision of this treatment and tested a set of hypothesised determinants (see table 1).
Conceptual framework to explain variations in quality of care
Methods
Health system context
In Germany, about 72 million people, or 90% of the population, were insured by one of 110 statutory health insurers as of January 2018. Almost all of the remaining population was covered by fully substitutive private health insurance.17 Healthcare is mostly free at the point of use, and the package of benefits available to the population is comprehensive. Since enactment of the 2012 Healthcare Structure Act, hospitals have been responsible for discharge management to ensure continuity of care. Prescriptions are generally issued by office-based physicians, including primary care physicians (PCPs) and specialists, among whom patients have free choice and direct access; PCPs do not function as gatekeepers to specialist care as they do, for example, in the UK.17 Since October 2017, hospitals have been able to prescribe medication for up to 7 days; previously, hospital staff could dispense limited doses to cover, for example, a patient’s medication needs for a weekend. Prescription drugs are subject to a moderate co-payment per pack, with annual caps for low-income groups and patients with chronic conditions.18 Selected pharmaceuticals, including some first-line statins, are exempt from co-payments.19 Affordability concerns are therefore unlikely to affect in any substantial way a patient’s propensity to consult an office-based physician to obtain a prescription.
Data
We used a nationwide data set from the largest group of statutory health insurers, the Allgemeine Ortskrankenkassen (AOK), which cover over 24 million people across Germany. We created a comprehensive, linked data set with administrative and medical data from hospital and office-based diagnoses and procedures. The initial sample included all AOK patients discharged with a primary diagnosis of AMI (ICD-10-GM (International Classification of Diseases 10th Revision, German Modification) code I21) from a hospital in 2011 (n=69 005, which represents about 32% of all hospital cases for I21 in 201120). We excluded patients who had been hospitalised for AMI in the 365 days before their first admission for AMI in 2011 (n=4544), which we defined as the index admission. To examine a patient’s history and outcomes, we limited the analysis to patients who continued to be insured by the AOK for at least 360 days or died in the 360 days after the index admission, and who had been insured by the AOK in the year before the index admission (excluding another n=181 patients). We excluded patients who died on their way to hospital or in hospital (n=7978), patients who were readmitted for (any kind of) rehabilitation services (n=3429) since we lacked information about pharmacotherapy for these patients, and patients younger than 18 years (n=13). We collected information on comorbidities from hospital and office-based claims data for the 365 days before the index admission. We defined multimorbidity as the presence of three or more conditions from a list of 46 chronic conditions, following an approach developed for German statutory health insurance (SHI) data by van den Bussche et al.21 We identified statin prescriptions using Anatomical Therapeutic Chemical codes (C10AA or C10BA or C10BX). The study exclusively used anonymised secondary data collected for billing purposes in the social health insurance system, and was hence deemed exempt from ethics review and informed consent in line with German guidelines for good practice in secondary data analyses.22
Identification of hospital-physician networks
Because we hypothesised that the inter-relationships between office-based physicians and hospitals might explain a significant share of variation in appropriate secondary prevention after discharge (see table 1), we identified empirical networks of hospitals and office-based physicians caring for the same patients. Earlier studies of hospital-physician networks7 9 first assigned patients to their usual office-based provider (UP) and then linked this UP to the hospital in which the majority of the UP’s patients received care. To better represent clinical reality in Germany, where a hospital may discharge patients to multiple office-based physicians, and any given office-based physician may receive patients from multiple hospitals, we adapted this method as follows: we assigned each patient to the hospital from which he or she had been discharged to office-based care. Since hospitals in Germany are responsible for ensuring effective discharge management, we regarded the hospital of discharge, in the context of our study, as the hub of each network. In addition, we assigned each patient to a UP, whom we defined as the office-based provider who had delivered the majority of a patient’s office-based care, as measured in terms of the number of visits billed for the patient in the year before the index admission. We assumed that the UP would continue to provide care for the patient after hospital discharge. When identifying each patient’s UP, we only considered visits to specialties involved in office-based cardiac management (PCPs, internists and cardiologists). If a patient had the same number of visits to a PCP as they did to a specialist, we defined the PCP as the patient’s UP. If a patient had the same number of visits to two specialists, we defined the UP as the specialist who had billed SHI for the highest output volume. We dropped patients in cases where the physician’s identifier was missing (n=391). Lastly, we assigned UPs to all of the hospitals from which their patients had been discharged. Our final study population included 52 489 patients discharged from 1118 hospitals and treated by 32 207 UPs.
Analytical approach
To disentangle the variation attributable to the hospital level and to the physician level, we employed cross-classified multilevel models in addition to standard hierarchical models.13 23 We estimated binomial response models with a logit-link function using Markov Chain Monte Carlo (MCMC) methods and the Metropolis-Hastings algorithm.23 A Bayesian approach with non-informative priors was employed because maximum-likelihood procedures can generate biassed estimates of random effects in binary models.24 MCMC is preferable when estimating more than one set of random effects, when random effects may be correlated and when clusters comprise few individuals.13 This last point was relevant in our case because office-based physicians in our sample treated an average of only 1.98 (AOK) patients per year (see table 1). Importantly, while small cluster sizes do not enable precise conclusions to be drawn about the performance of individual physicians,25 the focus and strength of our study are the large number of clusters we were able to identify across Germany (1118 hospitals and 32 207 UPs). This allowed us to generate reliable estimates of between-provider variation.12
The 2.5th and 97.5th quantiles of the resulting posterior distributions provided 95% Bayesian credible intervals (CrIs). We estimated models in MLwiN using the runmlwin command in Stata SE V.14.13 Because we had data from only one group of statutory health insurers, we excluded hospitals with fewer than five AOK patients from our analyses. We evaluated model fit using the Bayesian Deviance Information Criterion (DIC), a likelihood-based measure of model complexity and badness of fit for comparing non-nested models. A lower DIC value indicates better model fit.26
We calculated the median OR (MOR) as a measure of heterogeneity, as well as variance partition coefficients (VPCs) to measure the proportion of total variance at a given level.27 In conditional models, VPCs decompose the residual variation (that remains unexplained by the predictor variables) and attribute the relative proportions to the different levels considered. We conceptualised patients’ observed statin use (prescription/no prescription) in terms of a continuous latent variable as their propensity to receive a prescription.27 28 In the cross-classified model with hospital-physician random interaction effects, we thus calculated the hospital VPC as the ratio of relevant variances V with the following formula: VPC hospital = Vhospital / (Vhospital +Vphysician + Vhospital-physician-interaction +  / 3).12 28 We used analogous formulas for physician VPC and physician-hospital VPC.
/ 3).12 28 We used analogous formulas for physician VPC and physician-hospital VPC.
If one were to repeatedly sample at random two patients with the same covariates from different clusters (eg, hospitals), then the MOR is the median OR between the patient with the higher odds of the outcome and the patient with the lower odds of the outcome.27 Thus, the MOR quantifies the extent to which a patient’s odds of receiving a prescription is determined by having been discharged from a particular hospital.27 MOR values greater than 1.00 indicate between-cluster variation in the odds of receiving a prescription. If the MOR equals 1.00, however, there is no difference between clusters.27 An advantage of the MOR is that it translates the cluster-level variance to an OR scale. This enables one to compare the magnitude of the contextual effect, as expressed by the MOR, with the magnitude of measures of association between measured patient-level (and hospital-level) covariates and the outcome.27 For the physician level, the MOR can be estimated and interpreted analogously.
Patient and public involvement
No patients were directly involved in setting the questions, selecting the outcome measure, and designing and implementing the study. No patients were involved in the interpretation or writing up of study results.
Results
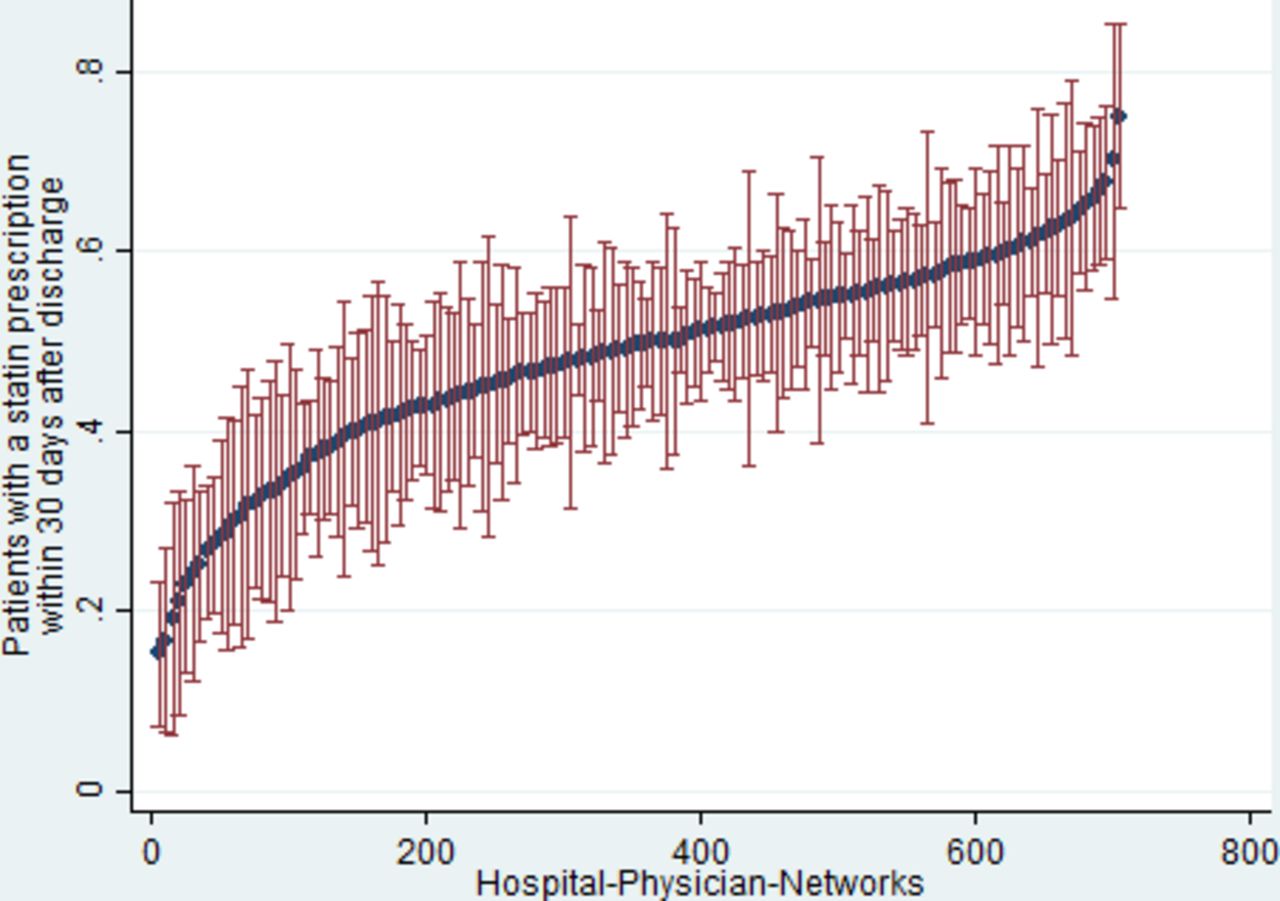
Network characteristics are shown in table 2; for population characteristics, see online supplementary S1. The proportion of patients who received a statin prescription in the 30 days after discharge varied significantly between hospital-physician networks (see figure 1), with an IQR of 52.5% (95% CI 48.2 to 56.9) to 71.3% (95% CI 63.9 to 78.8).
Supplemental material
{kind=link}
Network-level variation in 30-day prescription rates of statins. Includes only those hospitals with 20 or more patients from the analysis sample (n=48 998 patients)
Network characteristics and measures
Results of the cross-classified multilevel models for the random-intercept model without predictors (M1) and for the model that included patient characteristics (M2) are reported in online supplementary S2. All models included random interaction effects between hospitals and physicians. These improved model fit relative to the models without interaction effects, is evidenced by decreases in the Bayesian DIC statistics (see online supplementary S3 for all model comparisons). Thus, the effects that hospitals had on a patient’s odds of receiving a statin prescription in the 30 days after discharge varied according to which UP their patients visited and vice versa.
Supplemental material
Supplemental material
From the unadjusted model (M1), one can derive two main findings. First, hospitals, physicians and hospital-physician pairs are relevant for understanding variations in our quality indicator. This is shown by the MORs with CrIs that do not include the value of 1.00 (see M1, online supplementary S2), suggesting there was significant variation between hospitals (MOR=1.40; 95% CrI 1.36 to 1.45), between specific hospital-physician pairs caring for the same patients (MOR 1.32; 95% CrI 1.26 to 1.38) and, to a smaller extent, between physicians (MOR 1.14; 95% CrI 1.11 to 1.19). When comparing two identical patients from randomly selected hospitals, the MOR of 1.40 indicates that, in the median case, the individual odds of receiving a statin prescription would increase by a factor of 1.40 if the patient were to be discharged by the hospital with the higher odds of 30-day statin prescription. The MORs for hospital-physician pairs and for physicians can be interpreted analogously.
Second, the VPCs imply that hospitals contribute more to the observed variation than physicians, and most of the variation lies at the patient level. The VPC of 0.0360 for hospitals implies that 3.60% of the individual variation in the propensity to receive a statin prescription in the 30 days after discharge was due to systematic differences between hospitals. In addition, the specific hospital-physician pairs caring for the same patients accounted for 2.45% of the variation, while physicians accounted for 0.57%. Thus, in total, 6.62% of the observed variation was attributable to providers. The remaining 93.39% of the variation was due to patients.
Exploring potential determinants of these practice variations (M3, table 3), we found that hospital size (OR=1.24 for more than 300 beds compared with fewer than 100 beds) was positively associated and rural hospital location (OR=0.90) was negatively associated with the odds that a patient was prescribed a statin in the 30 days after discharge. Small, yet significant positive effects were evident for the number of patients shared between hospital-physician pairs (1.04), teaching hospitals (OR=1.06) and hospital (AOK) AMI case volume (OR=1.0007). For the physician characteristics, we found no evidence of association. The strongest associations were related to some patient characteristics. These included considerable positive associations for AMI severity (OR=1.68) and multimorbidity with three to five conditions (OR=1.45) and comparatively large negative associations for multimorbidity with six or more conditions (OR=0.68) and dementia (OR=0.63).
Results of cross-classified multilevel models: 30-day statin prescription at patient level
The proportional change in cluster variance statistics quantify the variance explained at the respective levels by these covariates. Using model M1 as the reference, the inclusion of 16 patient characteristics (M2, online supplementary S2) explained 41% of the variation between hospitals and 35% of the variation between hospital-physician pairs. Adding provider characteristics (M3, table 3) increased the explained variance at the level of hospital-physician pairs to 67%. The explained between-hospital variance increased slightly to 45%. Overall, the model with patient characteristics (M2) explained 22% and the model with patient and provider characteristics (M3) explained 27% of the variation in a patient’s propensity to receive a statin prescription within 30 days after discharge. It should be noted that in the models with covariates (M2 and M3), the VPCs have a conditional interpretation, as they decompose the residual (unexplained) variation. For model M3 this implies, for instance, that 0.49% of the unexplained variation that remains after adjusting for the covariates is due to the interaction between hospital-physician pairs.
Discussion
The aim of this study was to examine the role of hospitals and office-based physicians in timely provision of appropriate care after discharge from the hospital. To this end we analysed factors associated with variations in 30-day statin prescription for secondary prevention of AMI in Germany. Consistent with prior multilevel analyses of healthcare quality,25 we found that more than 90% of the variation could be attributed to the patient level. However, we found that each of the levels considered (hospitals, hospital-physician pairs and physicians) was relevant for understanding variations in statin prescription within the 30 days after discharge for AMI. Moreover, the MORs suggest that systematic differences between hospitals and between hospital-physician pairs were greater than between physicians. Since the variations in quality of care between hospital-physician networks in absolute terms are quite substantial, even when excluding hospitals with small case volumes (see figure 1), we believe these are important findings.
When exploring potential determinants of these variations (see table 1), the small but significant association with the number of patients shared between hospital-physician pairs is in concordance with earlier research from the social network literature that sees this as an indicator of stronger collaboration.11 29 We found that the hypothesised hospital-level predictors were significantly associated with timely prescription of statin treatment for secondary prevention of AMI. Previous research on AMI in Germany suggests that the number of beds and the teaching status of a hospital are measures of its overall resources;30 in the context of our study, the positive association found for these predictors may reflect greater capacity to implement effective care transition processes. Nevertheless, the associations found between hospital structures and quality of care are often less clear.31 Notably, adding provider characteristics (M3, table 3) increased the explained variance at the level of hospital-physician pairs from 35% in model M2 to 67%. This suggests that the association between hospital characteristics and the propensity of statin prescription depended on the specific hospital-physician pair, and potentially different mechanisms of coordination between different constellations of hospitals and office-based physicians. These findings merit further analysis. The negative association with a rural hospital location may, in turn, reflect quality deficiencies and limited access to office-based care in rural areas.32 For the physician characteristics included in our models, we found no evidence of association. However, there remained some significant residual heterogeneity between physicians in the full model (MOR = 1.15, see table 3). Potential underlying mechanisms of effective care transitions, such as having follow-up appointments scheduled before discharge,33 require further research.
Since current European cardiology guidelines do not list any contraindications to using statins for secondary prevention of AMI,15 16 patient characteristics should not be related to the odds of receiving a statin prescription in the 30 days after discharge. Our finding that 41% of the systematic differences between hospitals and 22% of the overall variation between patients could be explained by the patient characteristics considered therefore deserves attention. For some characteristics, such as having a diagnosis of dementia, this may due to concerns raised in the medical community about the appropriateness of statin therapy in certain patient groups (see table 1). Interestingly, moderate multimorbidity encompassing three to five chronic conditions was associated with larger odds of receiving a statin prescription, while the direction of association was significantly reversed for pronounced multimorbidity encompassing six or more chronic conditions. A possible explanation may be that, as the number of chronic conditions grows, concomitant increases in the risks of polypharmacy may lead physicians to delay or avoid adding another medication. Indeed, there have been calls internationally for clinical guidelines to include or adjust recommendations for patients with AMI with multimorbidity.34 Our findings suggest that it may be important to address these concerns in future guideline development efforts. Lastly, the significant associations with other patient characteristics, such as gender or the severity of AMI, merit further analysis about whether specific patient groups are systematically ‘lost in transition’35 following hospital discharge.
Our study has important limitations. As in any cross-sectional study design, the ability to draw causal inferences is limited. Also, since we had no information about patients readmitted for rehabilitation services (including patients participating in cardiac rehabilitation programmes) and related pharmacotherapy, these patients had to be excluded from our analysis. It is possible that statin prescription rates may differ for these patients. It should be re-emphasised that, since our data included only people insured by AOK, this allowed us to represent about 32% of all hospital discharges for AMI in Germany. From discussions we had with other large SHI funds, it appears that the low statin prescription rate following AMI we found is a known phenomenon in Germany. We therefore believe that our findings are plausible in this respect. However, it is important to point out that the total number of patients treated by a given hospital or physician may be larger and the coefficients on AMI volume at the hospital and physician levels must, therefore, be interpreted cautiously. Our study suggests that there is much scope for further in-depth analyses of underlying causes of (unwarranted) variations using a full data set. Finally, our focus on statin prescriptions was motivated by current clinical guidelines which recommend early onset of statin therapy for secondary prevention of AMI and do not list any contraindications for this approach (see the introduction section). With respect to other secondary prevention pharmacotherapy, data coverage would have been potentially incomplete (aspirin, for instance, is also available as an over-the-counter drug in Germany) or would have further decreased the size of our study population since other drugs such as ACE inhibitors and β-blockers are recommended only for certain subgroups.15 16 Therefore, we focused on statin prescriptions as one important indicator of timely provision of appropriate secondary prevention pharmacotherapy following AMI.
Conclusions
Timely prescription of appropriate secondary prevention pharmacotherapy after AMI is subject to considerable practice variation which is not consistent with clinical guidelines. While both hospitals and office-based physicians are relevant levels for understanding variations in performance, in our setting, hospitals contribute more to the observed variation than physicians, and most of the variation lies at the patient level. To ensure care continuity for patients, it is important to strengthen hospital capacity for discharge management and coordination between hospitals and office-based physicians. More generally, our study highlights the value of examining empirical networks of providers that deliver care to the same population with regard to their impact on the quality of care.
Acknowledgments
The authors thank the Scientific Institute of the AOK sickness funds (WIdO) for providing the data. The authors also thank two reviewers for their helpful comments on a previous version of this paper.
References
Footnotes
Contributors LSch, DK and LS made substantial contributions to the conception and study design. LSch and SF contributed to the acquisition of data. LSch, DK and SF contributed to the analysis of the data. LSch drafted the manuscript which all authors critically revised. All authors approved of the version to be published.
Funding This work was partially supported by the Central Research Institute of Ambulatory Health Care in Germany (Zi). The study sponsor had no role in designing the study; collecting, analysing or interpreting the data; writing the report; or in the decision to submit the paper for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All data relevant to the study are included in the article or uploaded as supplementary information.