Article Text

Abstract
Introduction The success of combination antiretroviral therapy has decreased the risk of perinatal HIV transmission and normalised pregnancy in women living with HIV (WLWH). Despite these advances, WLWH still face complex medical and psychosocial issues during pregnancy and postpartum, and there is a gap of knowledge on the experiences of becoming and being a mother living with HIV in today’s context. The overall aim of this study is to investigate psychosocial outcomes and experiences of WLWH in Scandinavia during pregnancy and early motherhood.
Methods and analysis This is a multicentre longitudinal convergent mixed methods study consisting of a quantitative survey study, a qualitative interview study and a mixed methods analysis. The survey study aims to examine psychosocial outcomes of WLWH across the pregnancy – postpartum trajectory. Participants are pregnant WLWH living in Scandinavia. Two control groups of HIV-negative pregnant women and non-pregnant WLWH are also included. Data is collected in the third trimester, 3 and 6 months postpartum using standardised questionnaires. Statistical analysis will assess changes over time and identify predictors of adverse outcomes. The interview study seeks to understand experiences of pregnancy and becoming a mother while living with HIV. Pregnant WLWH who are enrolled in the survey study will be asked to participate in individual interviews in the third trimester and 6 months postpartum. Data will be analysed using narrative analysis. The survey and interview results will be merged in a mixed methods analysis to assess confirmation, expansion or discordance between the data sets.
Ethics and dissemination Approval from the Danish Data Protection Agency (VD-2018–253), and the Finnish and Swedish Ethics Committees have been obtained (HUS/1330/2019 and Dnr: 2019–04451, respectively). Study results will be disseminated to patient organisations, through publications in peer-reviewed journals and at scientific conferences.
- HIV
- pregnancy
- motherhood
- depression
- stigma
- mixed methods
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Use of a convergent mixed methods longitudinal design will provide descriptive information of psychosocial outcomes in women living with HIV (WLWH) across the pregnancy – postpartum trajectory, in addition to an in-depth understanding of the experiences of these women.
This study will include pregnant WLWH in three Scandinavian countries (Denmark, Finland and Sweden), and follow them longitudinally.
Two control groups are included in the study to assess differences in psychosocial health among pregnant WLWH, pregnant women not living with HIV and non-pregnant WLWH.
It is a limitation that patients and public were not involved in the development of the research question or the design of the study.
The small sample size, due to low numbers of pregnant WLWH in Scandinavia, is also a study limitation.
Introduction
The success of combination antiretroviral therapy (cART) has resulted in a relative normalisation of pregnancy and a dramatic decrease in perinatal HIV transmission.1–3 Despite these advancements, women living with HIV (WLWH) still face complex medical and psychosocial issues during pregnancy, childbirth and postpartum.4 5 Although there has been increase in the annual number of HIV pregnancies in the last decade, both in Scandinavia and internationally,1 6 a gap exists in the research literature on the experiences of becoming and being a mother while living with HIV in today’s current context.
Women living with HIV in Scandinavia
There are approximately 1400, 1000 and 2800 WLWH in Denmark, Finland and Sweden, respectively, of whom 80% are of childbearing age.7–9 The majority of WLWH in Scandinavia are immigrants, mainly from sub-Saharan Africa, and HIV has mainly been transmitted by sexual contact.8 10 The healthcare system in the Nordic countries is tax-based and ensures universal access to both medical healthcare and many social support services.11 Hence, cART is provided free of charge and people living with HIV in Scandinavia are generally well treated with life expectancies approaching those of the general population.8 9 12 National antenatal screening for all pregnant women has been implemented as an opt-out programme (eg, all women are screened unless they decline).13 The proportion of WLWH that are diagnosed during pregnancy range between 18% to 37%.8 10 Treatment with cART has been recommended to all pregnant WLWH in Scandinavia since the late 1990’s and most women have an undetectable viral load at the time of delivery, resulting in a decreased risk of perinatal transmission to <1%.1 8 10 14 Condomless sex without assistance from artificial reproductive technologies and vaginal delivery are recommended in well-treated WLWH.1–3 8 15 Newborn treatment with prophylactic antiretroviral medicine lasts for 4 weeks after birth.8 14 16 The annual number of children born to WLWH in both Denmark and Finland has increased from 10 in the year 2000 to 45 in 2014, with no evidence of perinatal transmission of HIV if the mother has been well-treated with cART.1 8 10 In Sweden, approximately 60 to 80 children are born to WLWH each year.17
HIV and pregnancy
Several studies have shown that WLWH have fertility desires similar to the desires of the general population.18 19 Despite the normalisation of pregnancy in WLWH, becoming and being a mother with HIV is associated with unique pregnancy and postpartum considerations.5 In addition to the usual stresses of new motherhood, WLWH must also cope with stressors that include their own health, the unknown infectious states of their infants and attending to their infants’ unique needs such as the administration of prophylactic medications.5 In Scandinavia, national guidelines recommend not breastfeeding to WLWH as a small risk of perinatal transmission of HIV through the consumption of breastmilk remains, even in the context of cART.8 14 16 Several studies have highlighted the complexity and uniqueness of this issue for WLWH.20 21 Breastfeeding generally is considered natural and important for the mother-child relationship. Not being able to breastfeed may go against what is considered ‘good mothering’”.22 Moreover, breastfeeding may be the cultural norm for some immigrant women and formula feeding may be interpreted as a sign of HIV.23
Psychosocial and emotional well-being is essential to women during pregnancy to facilitate attachment to the newborn and to develop the capacity to parent effectively.24 Stigma continues to be a significant concern for WLWH.25 26 Interactions with healthcare professionals can either contribute to the women’s feelings of normality or enhance their experience of being different. Stigmatised care throughout the pregnancy–postpartum trajectory (eg, the period from pregnancy to after birth) has been reported in the literature.4 26 27 HIV-related stigma experienced during pregnancy may be associated with increased risk of depression, stress and social isolation.26 A high prevalence of depression in pregnant and postpartum WLWH is reported in several studies.28–30 Depression represents one of the most frequent distress conditions in the context of the transition to motherhood, and may be associated to a range of adverse behavioural and emotional outcomes for the child.31 The perception of being under surveillance due to increased medical monitoring during pregnancy may also affect the psychological well-being of these women.32
Thus, WLWH continue to contend with complex medical and psychosocial issues during pregnancy and early motherhood.5 33 Previous research in WLWH has concentrated on the physical health of the mother, prevention of perinatal transmission and the health of the unborn baby.34 35 While these foci are important, there remains a gap in knowledge about the impact of HIV on the psychosocial health and experiences of pregnant and postpartum WLWH. This study seeks to improve understanding of the maternal health challenges facing WLWH, such as stigma, perinatal depression and emotional well-being, so that goal-oriented interventions can be developed to improve the pregnancy and birth experience among WLWH.
Objectives
The overall aim of this study is to investigate psychosocial outcomes and experiences of WLWH in Scandinavia during pregnancy and early motherhood.
The specific objectives are:
Quantitative phase:
To examine psychosocial outcomes of women living with HIV across the pregnancy–postpartum trajectory.
To identify factors associated with adverse outcomes.
To assess differences in psychosocial outcomes between pregnant women living with HIV, non-pregnant women living with HIV and pregnant women not living with HIV.
Qualitative phase:
To elucidate the range of experiences of pregnancy and early motherhood while living with HIV among women in Scandinavia.
Integrated mixed methods analysis:
To integrate the quantitative survey findings and qualitative interview findings with the intent of obtaining a more comprehensive understanding of the psychosocial experiences and needs of WLWH across the pregnancy–postpartum trajectory.
Hypothesis
The hypothesis for the quantitative phase is that Scandinavian WLWH experience a high burden of psychosocial health challenges during pregnancy and early motherhood compared with the control groups, such as an increased prevalence of depression, stigma and social isolation, and this may be associated with their social situation, maternal country of birth and perception of stigma.
Study design
This is a multicentre longitudinal mixed methods (MM) research study. MM research is defined as an approach to research in which both quantitative and qualitative data are collected, analysed and integrated, thereby drawing interpretations based on the combined strengths of both sets of data.36 Increasingly, MM methodologists emphasise the importance of integration, not just qualitative and quantitative studies being conducted concurrently.37 The rational for using MM in this project lies in the need to gather different kind of data to answer the research objectives. Collecting both quantitative and qualitative data will enhance understanding not only of the psychosocial health of WLWH during pregnancy and early motherhood, but also elucidate the nuances and details of the women’s experiences. Thus, using a MM approach will provide a more comprehensive understanding of the psychosocial and emotional care needs of WLWH in Scandinavia.
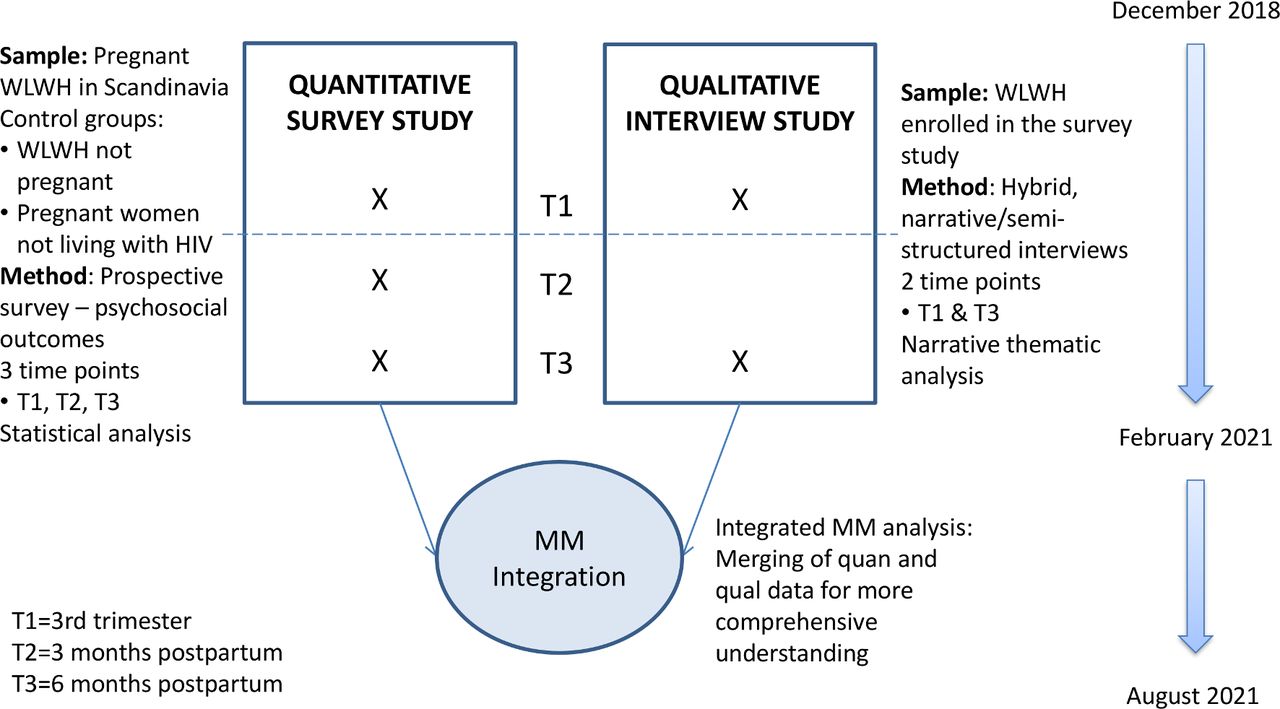
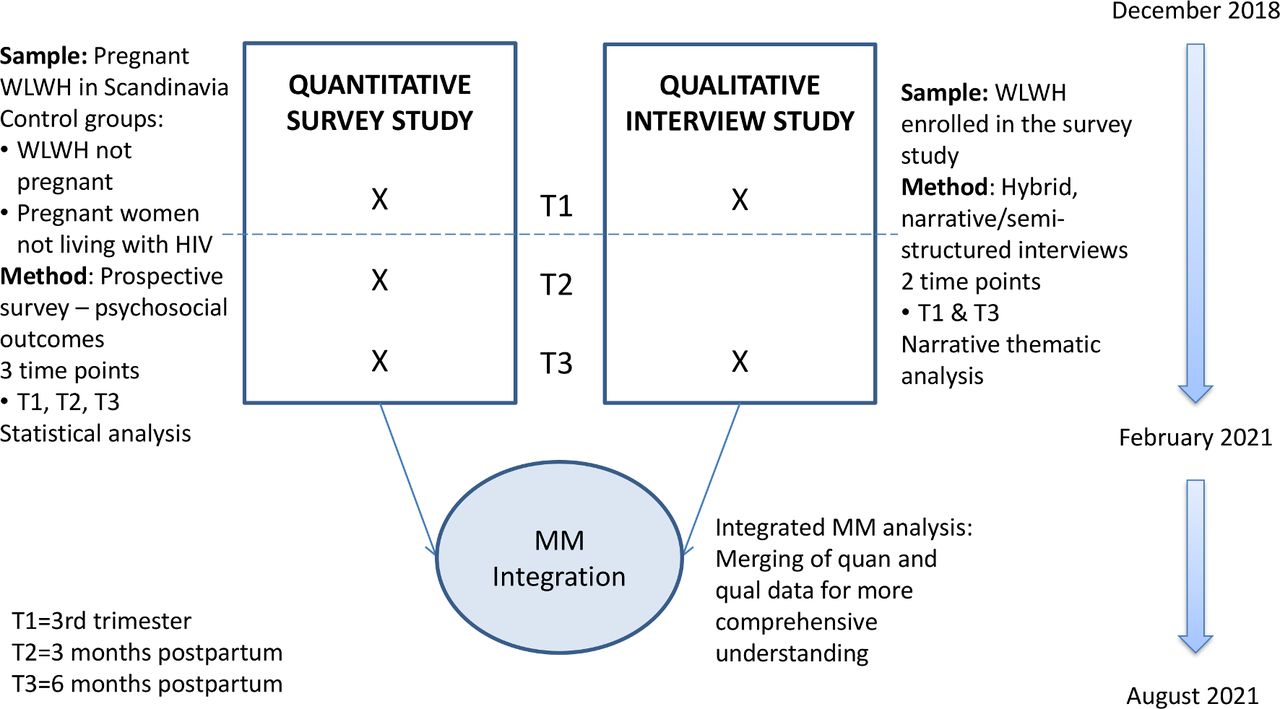
A convergent and longitudinal MM research design will be used. This is characterised by collecting and analysing quantitative and qualitative data separately but within the same study phase. The quantitative and qualitative results are then brought together through merging, with the aim of comparing the results.36 38 39 This project consists of two phases (see figure 1 and table 1). A quantitative phase with a prospective survey study using standardised self-report instruments and qualitative phase with a qualitative study using interviews. The use of a convergent MM design has a complementary aim as opposed to being part of a validation strategy.40 Thus, the results from the two phases will be merged in an integrated MM analysis to assess confirmation, expansion or discordance between the data sets.39
{kind=link}
Study diagram. MM, mixed methods; WLWH, women living with HIV.
Summary of research design, sample, data sources, time, analyses and expected outcomes
Theoretical framework
The philosophical and epistemological assumption that forms this research is pragmatism, a view that frames the integration of quantitative and qualitative methods within a single study from a question driven philosophy. Hence, this study is driven by research questions rather than an a priori stance regarding superiority of research methods.36 41
Methods
Quantitative phase
Population
In Denmark, treatment and care of pregnant WLWH are centralised at eight specialised centres during pregnancy and four specialised centres for delivery, and all pregnant WLWH living in Denmark will be asked to participate if they meet the inclusion criteria. In Finland, a majority of WLWH deliver at Helsinki University Hospital,8 while Sahlgrenska University Hospital treats about five to seven pregnant WLWH yearly. Eligible women are identified and recruited consecutively by the medical staff during routine clinical appointments at these centres. No honorarium is provided to participants. The inclusion criteria are: 18 years of age or older, pregnant, living with HIV, anticipated birth of a viable infant without life-threatening conditions or congenital anomalies, can speak and read Danish, Finnish, Swedish or English and willing to participate for the duration of the study. The estimated sample size is 80 WLWH. This is based on the number of children born to WLWH in the participating countries during the study period.
Control groups
Two control groups will be included in the quantitative survey study. Control group A consists of non-pregnant, women living with HIV, consecutively enrolled from the participating Departments of Infectious Diseases. The inclusion criteria are: between 18 and 45 years of age, living with HIV, not pregnant or planning to become pregnant, can speak and read Danish, Finnish, Swedish or English and willing to participate for the duration of the study
Control group B consists of pregnant women not living with HIV, consecutively enrolled at the Departments of Obstetrics at Copenhagen University Hospital, Hvidovre, Helsinki University Hospital or Sahlgrenska University Hospital. The inclusion criteria are: 18 years of age or older, pregnant, not living with HIV, anticipated birth of a viable infant without life-threatening conditions or congenital anomalies, no known chronic or psychiatric illness associated with increased surveillance or adverse pregnancy and birth outcome, can speak and read Danish, English, Swedish or Finnish and willing to participate for the duration of the study.
A ratio of 1 case:2 controls is chosen to increase precision. Thus, the estimated sample size is 160 participants in each control group.
Data collection
Data will be collected using standardised questionnaires at three time points; in the third trimester, 3 and 6 months postpartum (T1, T2 and T3, respectively). Control group A will follow the same time frame, that is, baseline, 3 to 4 months and 6 to 7 months. The questionnaire is available in English, Danish, Finnish and Swedish. Participants will answer the questionnaire themselves electronically in REDCap. Clinical data will be collected from the medical records and entered into the REDCap database.
Psychosocial outcomes
The HIV Stigma scale – short version will be used to measure overall perceived stigma, personalised stigma, disclosure concerns, negative self-image and concern of public attitudes.42 43 The scale consists of 12 items. Responses are on a 4-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’. A sum score is calculated, with a higher score indicating higher rates of perceived stigma.42 43 The HIV Stigma scale has been shown to be a reliable and valid measure of HIV-related stigma, also in WLWH populations.44 The scale has been translated and validated in a Swedish context.45 To utilise the sociocultural adaptations, the Swedish version will be translated into Danish and Finnish, and pilot tested prior to initiation of this proposed study. The HIV Stigma scale is not distributed to control group B.
The Edinburgh Postnatal Depression Scale (EPDS) will be used to assess symptoms of perinatal depression.46 The scale has 10-items with responses on a 4-point Likert scale ranging from 0 (absence of depressive moods) to 3 (worst mood). A total score ranging from 0 to 30 is calculated, and a cut-off point of ≤12 indicates an increased likelihood of clinical depression.46 The EPDS has been translated into Danish, Finnish and Swedish, has a well-documented validity and reliability and has been shown to be sensitive to changes over time.46 47 The scale does not mention the words pregnancy, child, birth or infant and has also been validated in a non-pregnant population.48 49
Perceived stress will be measured using the Perceived Stress Scale – 10 item (PSS-10), a self-administered scale that was developed to measure ‘the degree to which situations in one’s life are appraised as stressful’ during the past month.50 Responses are on a Likert-type 5-point format that ranges from 0 (never) to 4 (very often). The range for scores is 0 to 40 with higher scores reflecting greater perceptions of stress. The PSS-10 has been translated and validated in Danish Finnish and Swedish.51–53
Perceived social isolation will be assessed using the third version of the University of California, Los Angeles (UCLA) loneliness scale.54 The short version of the scale including three items will be used.55 Responses are on a 3-point Likert scale ranging from 1 (hardly ever) to 3 (often). Responses are summed into a total score, where higher scores indicate a greater degree of loneliness.54 55 The UCLA loneliness scale is the most widely used self-report scale measuring loneliness and has acceptable validity and reliability.54 56 The scale has been translated and validated in a Danish and Finnish context, respectively.57 58 The scale will be translated into Swedish using a translation – back-translation procedure.59
The Multidimensional scale of Perceived Social Support (MSPSS), a 12–item scale, is used to assess social support.60 61 The scale consists of three subscales; Family, Friends and Significant Others. Each item is answered from 1 (strongly disagree) to 5 (strongly agree). The total scores for each subscale range from 4 to 20, with higher scores suggesting a greater level of perceived social support. The MSPSS is a frequently used measure of social support in somatic illness, and good reliability and validity has been reported, also in a Danish context.62 63 The scale has also been translated and used in a Finnish and Swedish setting.64 65
The PACIFY questionnaire will be used to assess infant feeding perceptions and experiences among WLWH. The questionnaire was developed for a UK study investigating infant feeding among WLWH and contains 20 questions (personal communication w/Hermione Lyall). A modified version asking general questions about infant feeding will be used for control group B. The questionnaire will be translated into Danish, Finnish and Swedish, and is pilot tested prior to initiation of the study.
Clinical data
The following data will be collected from the patient records: maternal country of birth, maternal age at delivery, family situation, education, parity, mode of delivery, HIV medication, CD4 cell count, viral load, cART adherence, comorbidity, non-HIV medication, smoking, alcohol and drug use.
Statistical analysis
Descriptive statistics of demographic characteristics in the third trimester (T1) will be computed. The results of the different psychosocial outcomes (stigma, depression, stress, social isolation and social support) will be summarised at each time point (T1, T2, T3) to describe changes in mean scores of the different instruments over time and between groups. Only participants with data at all three time point will be included in this analysis. Bivariate correlations will be examined to determine relationships between the different study outcomes at all time points. Multiple regression analysis will be completed to explore the relationship between HIV-related stigma and multiple independent variables at all three time points and in the different exposure groups. A similar model will be used to explore the relationship between symptoms of depression and multiple independent variables. The co-variables included in the models will be chosen a priori based on the results from the bivariate analysis and clinical relevance. The site of enrolment will also be included in the model to account for variability between countries and sites. Analyses will be performed using Stata 13 software in collaboration with an experienced statistician. All reported p values are two-sided using a significance level of 0.05.
Qualitative phase
This descriptive qualitative phase consists of individual interviews connected (that is, involving the same participants) with the survey study through sampling. The interviews will be conducted in the third trimester of pregnancy and 6 months after birth.
Participants
All WLWH enrolled in survey study will be asked to participate in the qualitative phase and participants will be consecutively sampled until reaching data saturation (ie, the point when no substantially new information emerges from the interviews).36 66 Hence, WLWH will be recruited for both the survey and the interviews within the same time period. We anticipate that approximately 25 to 35 women will be sampled during pregnancy and at least 15 (accounting for attrition) in the second interview 6 months after birth.
Interviews
A study investigator will conduct individual interviews using a hybrid, narrative/semi-structured format.67 68 The opening question will be: ‘Can you tell us what your pregnancy/birth/mothering experiences have been like for you as a woman living with HIV?’ This will allow each woman to share her story. Probes will be used as clarifying and elaborating questions throughout the interviews, thus expanding the stories the women share within the larger narrative.67 Hence, initially participants will be asked to give a full narrative of their experiences. This is followed by a series of semi-structured questions and probes, to elaborate on themes not brought up by the woman herself (see online supplementary file 1). This ensures that the specified themes explored in the survey, for example, stigma, stress, depression, social isolation and social support, are also elaborated in the interviews. Thus, the same concepts are explored in both phases of the study, while still making room for new insights and perspectives. The interviews will be audio-recorded and will be conducted at the participant’s home or at the relevant hospital, whichever the woman prefers.
Supplemental material
Analysis
The audio-recorded interviews will be transcribed verbatim using a transcription protocol and analysed using narrative thematic analysis as described by Riessman.69 70 A thematic approach will be used where themes are identified as ‘told’ by the participant.70 Emphasis is on the content of the text, ‘what’ is said more than ‘how’ it is said.69 The analysis involves several steps: (1) The interviews are read several times to obtain a sense of the whole. (2) Emergent themes and patterns across the transcripts are identified, while paying close attention to the uniqueness of the whole story that was told. (3) The themes are compared for similarities and differences across participants and their narratives. Finally, the themes are brought together to create a coherent core story or a series of core stories.69 The first author (EM) will complete the initial analysis, which is then discussed with the research team to critically reflect on and review interpretations of the findings, and to make sure that the findings are based on the participating women’s narrative. NVivo 12 software, QSR International Pty Ltd, will be used in the analysis.
Mixed methods integration and analysis
Integration in MM research is defined as an intentional process by which the researcher brings qualitative and quantitative data together in one study.36 In this study, the quantitative survey data and qualitative interview data will be brought together for analysis through merging. The preliminary overarching themes across the quantitative and qualitative data are stigma, depression, stress, social isolation and social support. As an iterative approach is applied to the analysis, these themes may change based on the quantitative and qualitative results. Using joint display analysis, the survey and interview results will be merged by matching in a side-by-side comparison to assess confirmation, expansion or discordance between the data sets.36 39 Confirmation occurs if the findings from one type of data reinforce the results from the other. Expansion occurs when the findings from the two data sets diverge and expand the insights on WLWH by addressing different or complementary aspects of the prenatal and postnatal experience. Discordance occurs when survey and interview results are inconsistent, contradictory or disagree with each other.39 The results of the MM joint display analysis will be presented on a theme-by-theme basis and represented with joint displays.39 71 A joint display is a table where the quantitative and qualitative results are presented side-by-side. In addition, the joint display contains overall interpretations across the data, so called metainferences.39 71 Thus, joint display construction will be used in both the analysis and in the presentation of the results.
Research integrity to validity concerns
Creswell and Plano Clark38 highlight three key considerations to ensure validity in a convergent MM design. First, issues related to different sample sizes. In this study, the quantitative and qualitative data are collected for different purposes (quantitative generalisation vs qualitative in-depth description)38 resulting in different sample sizes in the quantitative and qualitative phases. The two study phases are connected through the sampling strategy, that is, women included in the survey will also be asked to participate in the interviews. Thus, recruiting the same women in both phases of the study will enhance our ability to integrate the quantitative and qualitative results in an MM analysis.38 The second consideration is related to the challenge of merging a numeric database and text data.38 Preliminary overarching themes have been identified a priori, that is, stigma, depression, stress, social isolation and social support. The quantitative and qualitative data thereby address the same concepts, while still making room for new results and insights. The final consideration is related to the need to explain divergent or discordant results.38 Discordant results are not considered a limitation in this study due to the complementary nature of this research.40 Should discordance occur, we will re-examine the data, collect additional data if necessary or use theory to explain the discordance.38
Patient and public involvement
Patients and public were not involved in the development of the research question or the design of the study. Participants will be asked to provide feedback on the dissemination and application of the results.
Discussion
This paper describes the design of a convergent, longitudinal MM study investigating psychosocial outcomes and experiences of WLWH in three Scandinavian countries during pregnancy and early motherhood. By publishing the protocol for this study, we make our methodological choices explicit and transparent. Although the study procedures have been detailed, we recognise the importance of retaining flexibility to examine unexpected topics/events that arise. A MM approach allows this, specifically with the flexible qualitative methods and through integration of quantitative and qualitative data.36
This study illustrates several state-of-the art features for a MM study. Through advanced planning, the qualitative and quantitative data collection will be matched to ensure that information from each type of data can be considered together. The study will employ joint display analysis as a process to compel careful consideration of the two types of findings together, and the drawing of interpretations across the two types of findings, that is, making metainferences. The study design includes a plan for the examination of discordance, should it arise, using recommended procedures. In addition, the study has been planned with consideration of the most up-to-date thinking about research integrity threats when conducting a MM study.
The findings to come from this study have several potential implications. First, by drawing on the strengths of both quantitative and qualitative approaches in a MM design, this study will provide descriptive information of psychosocial outcomes in WLWH across the pregnancy–postpartum trajectory, in addition to an understanding of the in-depth experiences of these women. Although, the lack of patient and community involvement during the development of the study could be a limitation. Second, understanding the experiences of WLWH in all its complexity is important because of the significance of maternal well-being on child outcomes and early intervention opportunities. Third, this study will include a nationwide sample of pregnant WLWH in Denmark and a sample of WLWH in both Finland and Sweden and follow them longitudinally. This will make it possible to capture changes in experiences over time and identify when in the pregnancy–postpartum trajectory interventions are most needed. Fourth, it is possible that some of the results will provide understanding of the positive interactions with healthcare professionals, thereby enhancing evidence-based practice. The results from this study can inform clinical practice in other Western countries that offer universal access to cART. Finally, this study can be utilised as a reference for the actual application of a convergent MM design in the field of maternal child health for WLWH.
Timeline
This is a 3-year study. Enrolment at the Danish sites was initiated in December 2018 and at the Finnish sites in July 2019. Enrolment in Sweden is expected to commence in October 2019. The enrolment of participants is estimated to take 18 months, with an additional 8 months of collecting follow-up data in the survey study. The anticipated completion date is 31 August 2021 (see figure 1).
Ethics and dissemination
Approval from the Danish National Ethics Committee is not required as no biomedical intervention is performed. All participating women will be asked to provide voluntary written informed consent at the time of enrolment and before any data collection. Data will be handled confidentially according the national regulations.
Study results will be disseminated through publications in peer-reviewed journals and at relevant scientific meetings and conferences. Results will also be disseminated at relevant clinical departments, patient organisations and to the participating women.
Conclusion
In the era of combination antiretroviral therapy, women living with HIV are still experiencing complex medical and psychosocial challenges during pregnancy and delivery. This multicentre longitudinal mixed methods study will provide a comprehensive knowledge of the psychosocial experiences and emotional care needs of women living with HIV in Scandinavia. Understanding and responding to the experiences of pregnant and postpartum women living with HIV is important, so that goal-oriented interventions supporting these women can be developed.
References
Footnotes
Correction notice This article has been corrected since it was published. Affiliation for Gitte Pedersen has been corrected.
Contributors EM is the PI and wrote the first draft of the study protocol. MDF is a senior mentor on the team and edited the study protocol with the PI. IA, ÅM, ISJ, MS, GP and TLK are members of the project group and have edited the study protocol with the PI. NW co-designed the study and edited the study protocol with the PI.
Funding This work is funded by The Novo Nordisk Foundation, Reference Number: NNF17OC0029508 and NNF18OC0052512.
Disclaimer The views expressed in the submitted article are the authors’ own and not an official position of the institutions or the funder.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study has been approved by the Danish Data Protection Agency (VD-2018-253) and the Finnish and Swedish Ethics Committees (HUS/1330/2019 and Dnr: 2019-04451, respectively).
Provenance and peer review Not commissioned; externally peer reviewed.