Article Text

Abstract
Objectives To determine the incidence of unintended pregnancy among female sex workers (FSWs) in low-income and middle-income countries (LMICs).
Design We searched MEDLINE, PsychInfo, Embase and Popline for papers published in English between January 2000 and January 2016, and Web of Science and Proquest for conference abstracts. Meta-analysis was performed on the primary outcomes using random effects models, with subgroup analysis used to explore heterogeneity.
Participants Eligible studies targeted FSWs aged 15–49 years living or working in an LMIC.
Outcome measures Studies were eligible if they provided data on one of two primary outcomes: incidence of unintended pregnancy and incidence of pregnancy where intention is undefined. Secondary outcomes were also extracted when they were reported in included studies: incidence of induced abortion; incidence of birth; and correlates/predictors of pregnancy or unintended pregnancy.
Results Twenty-five eligible studies were identified from 3866 articles. Methodological quality was low overall. Unintended pregnancy incidence showed high heterogeneity (I²>95%), ranging from 7.2 to 59.6 per 100 person-years across 10 studies. Study design and duration were found to account for heterogeneity. On subgroup analysis, the three cohort studies in which no intervention was introduced had a pooled incidence of 27.1 per 100 person-years (95% CI 24.4 to 29.8; I2=0%). Incidence of pregnancy (intention undefined) was also highly heterogeneous, ranging from 2.0 to 23.4 per 100 person-years (15 studies).
Conclusions Of the many studies examining FSWs’ sexual and reproductive health in LMICs, very few measured pregnancy and fewer assessed pregnancy intention. Incidence varied widely, likely due to differences in study design, duration and baseline population risk, but was high in most studies, representing a considerable concern for this key population. Evidence-based approaches that place greater importance on unintended pregnancy prevention need to be incorporated into existing sexual and reproductive health programmes for FSWs.
PROSPERO registration number CRD42016029185
- public health
- reproductive medicine
- preventive medicine
- epidemiology
- sexual medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to systematically review and analyse the incidence of pregnancy or unintended pregnancy among female sex workers (FSWs) in low-income and middle-income countries.
Broad inclusion criteria meant that the review allowed for the inclusion of a large proportion of the studies that have collected data on pregnancy or unintended pregnancy rates in this population.
However, limitations of broad inclusion criteria are that only one study had an a priori objective of measuring pregnancy incidence, and studies were highly varied in terms of their methodology, settings and study populations.
High heterogeneity prevented pooled analysis of all studies but allowed for subgroup analysis for cohort studies and for studies in which no intervention was introduced.
Pregnancy rates among FSWs could not be compared with the background general population rates because of the lack of availability of those data.
Introduction
Unintended pregnancy affects a large number of women in low-income and middle-income countries (LMICs) and can have significant impacts on maternal and child health.1–3 Unintended pregnancy is a high priority issue for many female sex workers (FSWs)4 5 who usually have dependents to support and for whom pregnancy may increase financial dependence on sex work and add to already high levels of stigmatisation.5 This has been confirmed by consultation with FSWs in Kenyai and workshops with FSWs to inform development of a pregnancy prevention intervention.6 Participants expressed considerable fear and anxiety about pregnancy, related personal and peer experiences of pregnancy scares and emphasised the importance of improving knowledge of family planning in their community (unpublished qualitative data, Mombasa, Kenya).
FSWs can face elevated risks of unintended pregnancy due to a high frequency of intercourse and a high number of sexual partners.7 8 Risks are exacerbated by concurrent paying and non-paying partnerships8 and by sexual and gender-based violence, gender inequalities and stigma towards sex work, which reduce women’s power to negotiate within sexual relationships.9–11 While gains have been made in terms of condom use with paying clients,12 rates of condom and other contraceptive use are consistently lower with emotional (non-paying) partners.5 13 14 In many countries, particularly in sub-Saharan Africa, few FSWs use long-acting reversible contraceptives (intrauterine devices and implants), and methods such as injections, condoms and pills may be used inconsistently or incorrectly, rendering them less effective.5 15 Limited knowledge and misunderstandings, particularly in relation to contraceptive side effects and impacts on fertility, are significant demand-side barriers to contraceptive uptake.4 5 16
Family planning services are often neglected as part of FSW-specific service provision, which have focused largely on preventing HIV and other sexually transmitted infections (STIs).12 17–19 Stigma of health workers towards sex workers can also limit access to contraception.20 21 FSWs have the same reproductive rights as all women, and their desires and needs in relation to pregnancy have often been neglected,22–24 similar to other marginalised populations, which have historically been subjected to reproductive coercion.25 26 It is important that those who do desire pregnancy are provided with non-judgemental care and that those who do not are given the opportunity and resources to prevent it. Moreover, many FSWs who become pregnant may be reluctant to enter maternal health services, given their previous experiences of discrimination and abuse from health workers.20 FSW programmes need to make concerted efforts to facilitate timely attendance of FSW at antenatal clinic and childbirth services. Importantly, FSWs often have remarkably high levels of HIV, and maternal health services are a key entry point for them to access antiretroviral treatment, which secures their health and reduces HIV in infants.
Despite a clear rationale for addressing unintended pregnancy in this population, it is important to acknowledge that intention is a problematic concept, which is more accurately represented as a spectrum than a dichotomy.3 27 Indeed, many women feel positive about pregnancy despite not intending to conceive, or may simultaneously desire both pregnancy and its avoidance, for different reasons. The degree to which women accept or welcome a pregnancy once it has occurred has been hypothesised to be a more important predictor of adverse outcomes than prepregnancy intentions.27 Fertility preferences are also likely to be less stable over time in LMICs undergoing fertility transition compared with high-income countries.3 FSWs’ intentions also differ between types of partner, requiring them to adapt contraceptive use accordingly.22 Furthermore, as a stigmatised group, FSWs may feel pressure not to disclose their intention. Despite these limitations, we have continued to use the term ‘unintended pregnancy’ in this paper for the sake of consistency with other literature and the lack of a feasible alternative.
The primary objective of this study was to determine the pooled incidence of unintended pregnancy among FSWs in LMICs. Given the expected low number of eligible studies, we also aimed to determine the incidence of pregnancy where intention is not known. Secondary aims were to examine the correlates and predictors of pregnancy and the incidence of induced abortion and childbirth in this population.
Methods
All stages of this systematic review and meta-analysis have been reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.28 The protocol for this review was registered with the international prospective register of systematic reviews (PROSPERO): number CRD42016029185.
Inclusion and exclusion criteria
Studies were included if they met key criteria in terms of population, outcomes and study design. FSWs had to account for at least two-thirds of the sample, unless data could be disaggregated by sex work status. We employed a broad definition of sex work, including women who self-identified as sex workers, those who engaged in transactional sex or part-time sex work and communities of women known to practice commercial or transactional sex. Study participants had to live or work in an LMIC29 and be of reproductive age (15–49 years). Studies targeting women with reduced fertility (eg, women in the first 6 months postpartum and those exclusively breast feeding or undergoing fertility treatment) were excluded.
Studies had to measure or report one of the following primary outcomes:
Cumulative incidence (proportion of women who became pregnant in a defined time period) or incidence rate (per person-time) of unintended pregnancy.
Cumulative incidence or incidence rate of pregnancy (where intention is not measured).
Unintended pregnancy was defined as any pregnancy considered by the woman to be not planned, intended or desired at the time of conception,30 as reported either prior to pregnancy or retrospectively. Such pregnancies may be described by the authors as unintended, unwanted, undesired, unplanned or mistimed.
Any study design that was able to measure one or more of the primary outcomes was considered, including both observational and intervention studies. Case studies, ecological studies, qualitative studies, editorials and commentaries were excluded. We planned to expand the inclusion criteria if insufficient studies measuring the primary outcomes were identified to include studies reporting prevalence of pregnancy in the previous 12 months. Cross-sectional studies were included in the initial screen for this purpose but were subsequently excluded as there were sufficient longitudinal studies measuring incidence. The addition of period prevalence in the last 12 months as an outcome would have required additional subanalyses; in addition, measurement of retrospective pregnancy intention in cross-sectional studies differs from prospective measurement as women may change their minds during the course of their pregnancy. Only studies published in English since 1 January 2000 were included.
Search strategy
A systematic electronic search of MEDLINE, Embase, PsychINFO and Popline was undertaken to identify relevant peer-reviewed articles. Search syntax included, as both subject headings and keywords: synonyms for ‘sex work’; list of LMICs from the World Bank29 and synonyms for ‘low- and middle-income’; and study design and descriptor terms, for example, ‘cohort studies’ or ‘controlled trials’ (full search strategy in online supplementary file).
Supplementary file 1
A search for unpublished grey literature was also undertaken, including conference proceedings and abstracts (via Web of Science and Proquest databases), research theses and the websites of relevant non-government organisations, including the Population Council, FHI 360 and Guttmacher Institute.
The last search was performed on 20 January 2016. Up to two attempts were made to contact authors when further information was required. Eligible studies recommended by contacted authors were also included.
Screening and data extraction
Screening of all abstracts, removal of duplicates and selection of full-text articles was conducted by one researcher, with a random selection of 10% screened in duplicate. Data from a random sample of 50% of included full-text manuscripts were extracted in duplicate. Discrepancies in eligibility and data extraction were resolved by discussion, with a third researcher arbitrating when necessary.
Summary estimates were sought rather than individual subject data. Data were extracted relating to: eligibility criteria; study aims, population and methods; setting and participant characteristics at baseline; primary and secondary outcome data for each time point reported; and quality assessment criteria. In addition to the primary outcomes, the following secondary outcomes were extracted: incidence of induced abortion (termination of pregnancy); incidence of birth; and correlates/predictors of pregnancy or unintended pregnancy. Authors were contacted to provide data relating to the primary outcome when it was not reported in the paper, for example, the total person-years of exposure.
Quality assessment
Methodological quality of the included studies was assessed using a modified version of the Joanna Briggs Institute Prevalence Critical Appraisal Tool31 (online supplementary file). This tool was designed to assess studies measuring prevalence or incidence and can be applied to multiple study designs. The tool was modified to address specific methodological concerns of our research question. Given measurement bias could result from infrequent or irregular pregnancy detection methods, items on these methods were specifically included. We also documented whether pregnancy incidence was an a priori study objective.
Quality assessment was undertaken in duplicate for 50% of studies, with discrepancies resolved by discussion. Studies were given a score out of 15 if they measured unintended pregnancy incidence, and a score out of 14 if they measured pregnancy incidence (the latter did not include an item on measurement of intention). Scores were then reported as percentages.
Analysis
We undertook a qualitative narrative synthesis of both primary and secondary outcomes and quantitative analysis of primary outcomes using Stata V.13.1.
Incidence rate (per 100 person-years) was taken as the unit of analysis. In studies reporting only cumulative incidence, we estimated person-time, censoring women at their first pregnancy and assuming that they became pregnant halfway through the study.
The Mantel-Haenszel I2 statistic was over 95% for both primary outcomes, so meta-analysis and meta-regression were not performed for all eligible studies, as had been planned. Instead, sources of heterogeneity were explored using subgroup analyses, and pooled incidence rates were calculated using DerSimonian & Laird random effects models for subgroups containing more than two studies and with I2 of less than 75%. The explored subgroups were clustered as covariates that may explain heterogeneity (geographic region and intervention vs non-intervention) and potential methodological explanations of heterogeneity: study design (cohort vs randomised controlled trial (RCT); study duration; and frequency of pregnancy measurement (measured regularly vs only when indicated). Interventions included any introduced by the study with the aim of improving sexual and reproductive health, including contraceptive provision and behavioural or biomedical interventions to prevent HIV/STIs.
We assessed study quality as a source of heterogeneity by examining scatter plots and Pearson correlation coefficients of quality score against incidence rate. We also qualitatively explored characteristics of different studies, including the following baseline population characteristics that may have impacted on pregnancy rates: age; contraceptive prevalence; consistent condom use; number of sex partners; coital frequency; STI prevalence; indicators of gender-based violence; and alcohol and other drug use.
Patient and public involvement
The research question and outcome measures were informed by previous qualitative work with FSWs conducted by the International Centre for Reproductive Health, Kenya. This confirmed that unintended pregnancy was an important issue for this population group. Patients and members of the public were not otherwise involved in the design or conduct of this study.
Results
The initial search yielded 6523 peer-reviewed and 118 grey literature articles and 11 identified by hand-searching (eg, due to recommendations from contacted authors). After removal of duplicates, this resulted in 3866 articles (figure 1). Based on title and abstracts, 750 manuscripts remained for full-text screening.
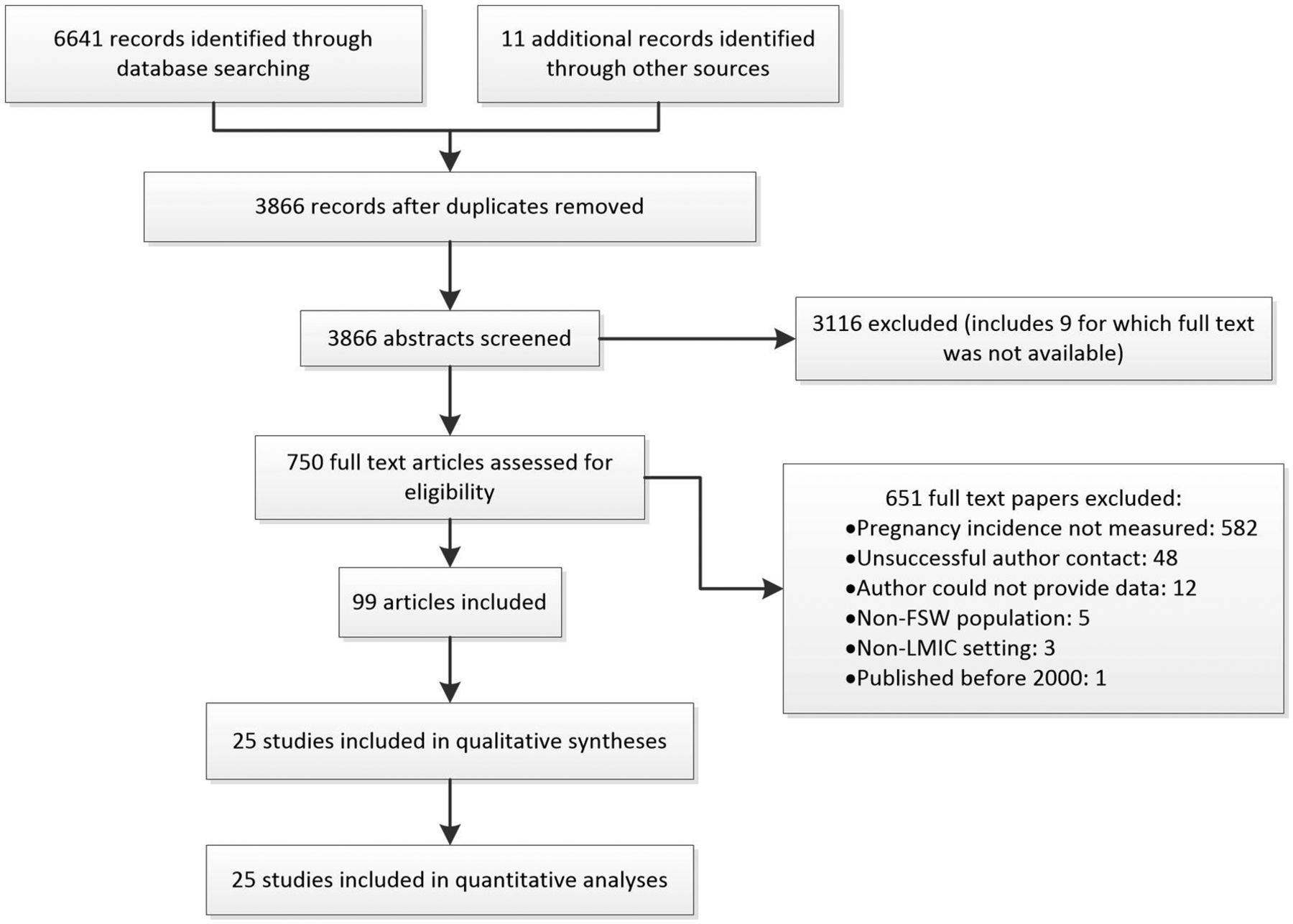
PRISMA flow diagram of search results and inclusion of studies after review.28 FSWs, female sex workers; LMICs, low-income and middle-income countries; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Pregnancy incidence was reported in 12 studies and was obtained for a further 13 studies after contacting authors. These 25 studies were reported in 99 papers. Ten studies measured unintended pregnancy (outcome 1), and 15 studies measured pregnancy without specifying intention (outcome 2); none measured both outcomes.
Fourteen cohort studies and 11 RCTs were included (table 1). Pregnancy incidence was not an a priori primary objective for any but was a secondary objective for a Rwandan HIV incidence study.32 The majority of studies aimed to test interventions to prevent HIV or STIs (n=11) or measure HIV incidence (n=8). Six undertook substudies in which they reported pregnancy incidence.33–38 Thirteen studies included any intervention: three involved provision of diaphragms or female condoms,39–41 and 10 studies were biomedical or behavioural interventions to prevent HIV/STIs (table 1). The latter included four studies that reported providing contraceptive counselling35 36 42 43 and one which offered free contraception when needed.44
Characteristics of included studies
Most RCTs in this review required women to remain non-pregnant for continuation.36 40 42 44–48 The majority of studies (n=19) took place in sub-Saharan Africa, most frequently in Kenya (n=8; table 1). There were also studies from the Americas (Mexico and the Caribbean) and East Asia (China, Thailand and Cambodia). All except three36 44 49 took place in urban settings. The study areas were frequently informal housing settlements, low-income areas or environments known for sex work and/or drug use.
Sex work was mainly defined as exchange of sex for money or goods (n=12) or money alone (n=4). In five studies, sex workers were self-identified, in two studies they were members of communities or working in areas known for commercial sex work36 46 and in two studies no definition was provided.48 50 Eighteen studies involved FSWs exclusively; the remainder targeted women with high-risk sexual practices or at high risk of HIV. These studies either reported pregnancy incidence in the sex work subgroup36 42 44 51 or FSWs constituted more than two-thirds of the sample.32 40 49 52 Fourteen studies were restricted to women without HIV at baseline, and one study to women living with HIV.37
Most studies (n=15) were conducted for 1–2 years, although they ranged from a 1 month pilot RCT40 to a 15-year open cohort study.37 The studies reporting pregnancy (intention undefined) tended to be of longer duration than those reporting unintended pregnancy (median duration 24 and 12 months, respectively; table 2).
Results of included studies reporting unintended pregnancy and pregnancy (intention undefined) in ascending order of incidence
Baseline population characteristics
Most study populations had a median of 5–8 years of education, and the majority of women were supporting at least one financial dependent (data not shown). Median duration in sex work was 3–5 years for most study populations, with one notable exception of 14 years in a study in Mexico.43 Concurrent non-paying sex partners were common, reported by 30%–100% of women in 12 studies.
Permanent and long-acting reversible contraceptive use was around 1% in most studies in Africa, with only one study in Kenya reporting significantly higher coverage (17.5%).50 By contrast, coverage of these methods was greater than 30% in China53 and Mexico.43 54 Consistent condom use was measured using diverse metrics but was generally low and very low with non-paying partners. Most studies reported frequent sex with multiple partners, and few reported a median of less than five partners per week.37 45 52 55 High rates of gender-based violence were noted in all studies in which this was measured, as well as physical or financial pressure not to use condoms.40 56
While the factors described generally contributed to high baseline pregnancy risk, several studies included FSW with notably lower risk profiles. For example, two studies were part of a large Kenyan open cohort, in which participants had few partners and sex acts per work, and older median age and lower STI prevalence than the other studies.37 45 In addition, a number of studies provided insufficient information to assess population risk for pregnancy.
HIV prevalence was reported in four studies and varied from 24 % in Kenya 50 to less than 3 % in Mexico 54 and Dominican Republic. 41 STIs other than HIV were prevalent, with one study reporting up to 36% of the study population having at least one STI on biological testing.35 57
Methodology and quality assessment
Quality scores, as percentages of the available total, are presented in table 2. The median quality score was 40% (IQR=36%–50%). Four studies scored 60% or greater; three of these measured unintended pregnancy32–34 and one measured pregnancy (undefined).53 Most studies scored poorly in the external validity and selection bias categories.
Measurement bias was an issue for some studies. Pregnancy was tested regularly in all but one44 of the unintended pregnancy studies; in contrast, five pregnancy (undefined) studies only measured it if suspected by the clinician or participant. Five of the pregnancy (undefined) studies measured pregnancy using self-report rather than a biological test.
Incidence of pregnancy
Incidence rate was reported by 14 studies and calculated for the remainder based on the available data, with the number of women who became pregnant as the numerator and person-years as the denominator. Women were censored at the time they became pregnant. The one exception was Deschamps et al,33 who counted multiple pregnancies and subtracted pregnancy time from total person-time.
Unintended pregnancy incidence rate (outcome 1) varied widely between studies, ranging from 7.2 to 59.6 pregnancies per 100 person-years (table 2; figure 2). The median rate of the 10 studies was 26.8, and seven reported a rate of greater than 20 per 100 person-years.

Incidence rates (per 100 person-years) for studies reporting unintended pregnancy.
Incidence rate of pregnancy (intention undefined – outcome 2) also varied widely, but rates were lower overall than unintended pregnancy, ranging from 2.0 to 23.4 per 100 person-years (table 2). The median rate of the 15 studies was 13.5, and only two reported a rate of greater than 20 per 100 person-years.
Meta-analyses
Random effects meta-analyses were performed for the two primary outcomes. Heterogeneity was high, with I2 statistic over 95% for both outcomes.
Incidence of unintended pregnancy
Explored covariates that may explain the high heterogeneity of unintended pregnancy incidence showed that geographical region did not explain this, whereas presence/absence of an intervention seemed important. The three cohort studies that did not involve an intervention had very low heterogeneity (I2=0%), and the pooled estimate for these studies was 27.1 unintended pregnancies per 100 person-years (95% CI 24.4 to 29.8; figure 3). These three studies scored at least 60% on quality assessment (table 2).

Forest plot showing subgroup analysis of unintended pregnancy incidence rates (per 100 person-years) by intervention versus no intervention.
Assessment of potential methodological explanations showed that study design (RCT vs cohort) and study duration seemed important sources of heterogeneity, while pregnancy measurement method did not explain the high heterogeneity. The cohort studies were more homogenous than the RCTs (I2=63.9% and 96.8% respectively), and had higher pooled incidence of unintended pregnancy (figure 4). The three studies of less than 1 year duration were more homogenous (I2=59.1%) and had higher incidence (44.5 per 100 person-years) than longer studies (figure 5).

Forest plot showing subgroup analysis of unintended pregnancy incidence rates (per 100 person-years) by RCT versus cohort study design. RCT, randomised controlled study.

Forest plot showing subgroup analysis of unintended pregnancy incidence rates (per 100 person-years) by study duration (cut-off 1 year).
Quality was not found to be a source of heterogeneity, as no relationship was demonstrated between study quality score and unintended pregnancy incidence rate (Pearson correlation coefficient 0.01; scatter plot not shown).
Incidence of pregnancy (intention undefined)
Subgroup analyses showed that study duration and geographic region were sources of heterogeneity for rates of pregnancy where intention was not known. Pregnancy measurement method and study design characteristics did not account for any heterogeneity for this outcome.
There were only two studies of less than 1-year duration53 56 (I2 0%). As with the unintended pregnancy outcome, these studies had a higher pooled incidence than studies of more than 1 year duration (14.9 vs 11.4 per 100 person-years).
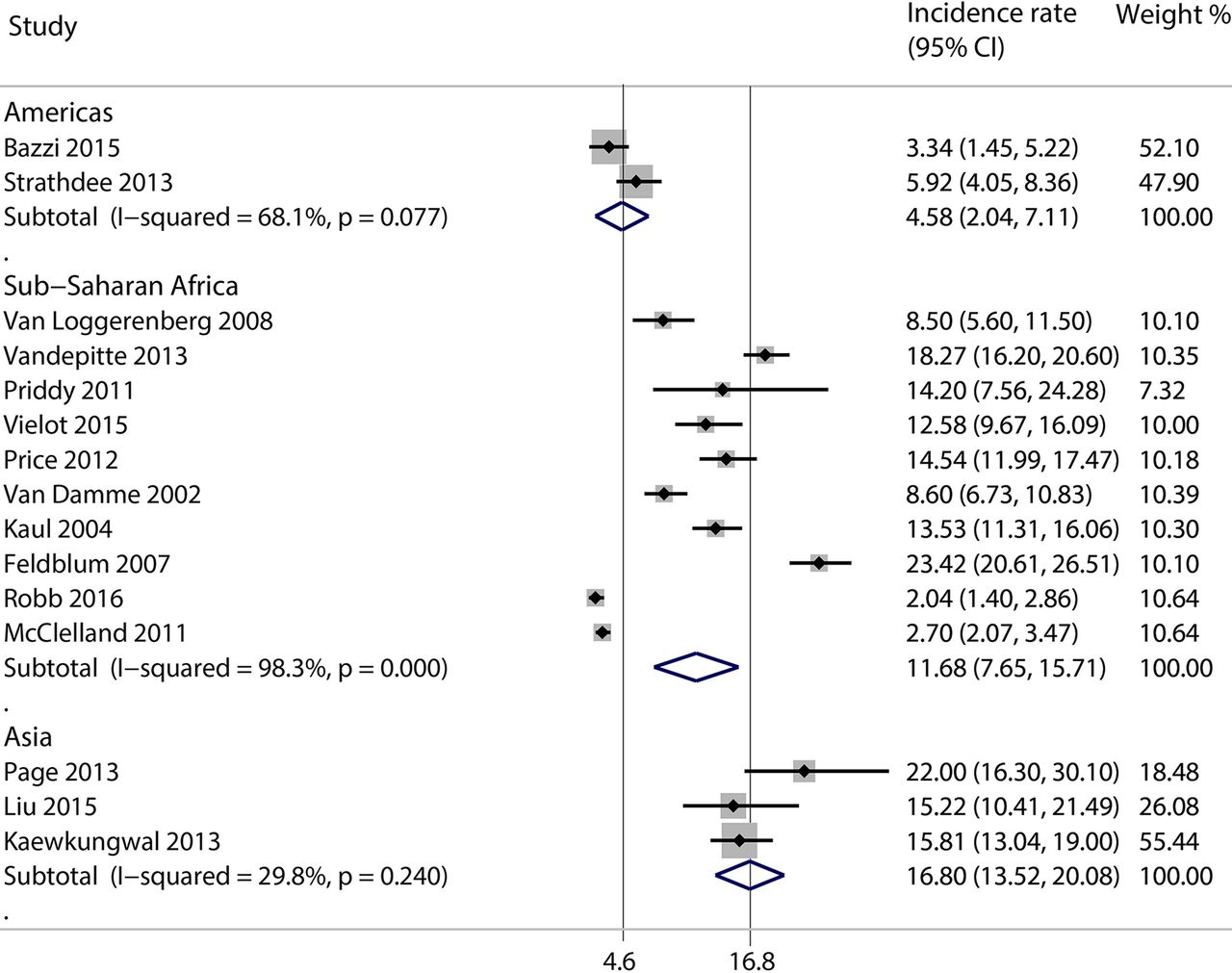
A subanalysis of geographic region showed that studies from Asia and the Americas (both in Mexico) were more homogenous (I2=29.8% and 68.1%, respectively) than those from sub-Saharan Africa (I2=98.3%). The pooled incidence of pregnancy was higher in Asia (16.8 per 100 person-years) and lower in Mexico (4.8 per 100 person-years; figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing subgroup analysis of pregnancy (intention undefined) incidence rates (per 100 person-years) by geographic region.
A scatter plot demonstrated a weak positive relationship between quality score and incidence rate (plot not shown; Pearson correlation coefficient 0.55).
Secondary outcomes
Three studies assessed pregnancy outcomes for FSWs (table 3). In two of the studies, outcomes were unknown for about 25% of pregnancies (in the Caribbean33 and Madagascar,35) resulting in underestimates of birth and abortion incidence. Abortion accounted for less than 20% of pregnancies with known outcomes. In contrast, in the third study, a multicountry study,48 62 abortions were recorded as adverse events (author correspondence), compared with only 10 reported as withdrawing from the study due to pregnancy, suggesting that over 85% of the total women who became pregnant reported an abortion.
Incidence of abortion and birth
Four studies developed multivariate regression models to determine the predictors of pregnancy35 37 or unintended pregnancy.5 33 Common findings were that younger age was associated with higher pregnancy incidence5 33 35 and that highly effective contraceptive use35 and consistent condom use35 37 were protective; however, one study in Kenya found that using condoms at the exclusion of other methods was a risk factor.5 Having a main or emotional partner increased the odds of unintended pregnancy5 33 but not of pregnancy (intention undefined).35 37 Deschamps et al noted some additional associations, including recreational drug use and male partners having other sex partners being protective against pregnancy. Only one study assessed reproductive history and income,5 and none considered HIV status as potential predictors or confounders.
Discussion
This review found that of the many studies examining FSWs’ sexual and reproductive health in LMICs, very few have measured pregnancy and even fewer have assessed pregnancy intention. While incidence varies widely between the included studies, it is sufficiently high in most low-income and middle-income contexts to constitute a significant health and social issue for FSWs.
Study design impacted on unintended pregnancy rates, with a lower rate seen in RCTs (20.8 per 100 person-years) than cohort studies (29.6 per 100 person-years). Most of the RCTs in this review required women to remain non-pregnant for continuation36 40 42 44–48 and although only six RCTs specifically mentioned providing contraceptive counselling or methods, others may have offered a larger package of services that was not reported.
To better understand the influence of services provided by studies, we compared studies that provided any intervention with those that did not and found that the three studies in the latter category had very low heterogeneity and high pooled unintended pregnancy incidence (27 per 100 person-years). As non-intervention cohort studies with quality scores of at least 60%, these were arguably the best designed to answer the review question.
The included studies may have underestimated population incidence of pregnancy, for several reasons. First, studies that only tested for pregnancy on suspicion could have missed early pregnancies or failed to ascertain the need to test. Second, pregnancies occurring between study visits and ending in spontaneous or induced abortion may have been missed. Third, social desirability bias is likely to influence self-reporting of pregnancy in studies using that measure. Fourth, participants may have joined some studies in order to access services, potentially receiving superior family planning services than would otherwise be accessible.58 Finally, there may be selective loss to follow-up among women who become pregnant, particularly in drug trials requiring women to remain non-pregnant for continuation.36 40 42 44–48 It is possible that these factors were more prominent in the studies measuring pregnancy without defining intention, contributing to the surprising finding that this outcome had generally lower incidence rates than unintended pregnancy.
Some ‘unintended’ pregnancies may in fact have been intended, because women may have been unsure about their intention or it changed over time.27 Only one study assessed intention repeatedly,34 and none used a validated instrument designed to measure this complex latent construct.59 Some participants may have wanted a pregnancy but felt pressure to say otherwise, depending on the social environment, external and internal stigma and the study design, for example, if they wanted to access HIV prevention and other services through the study but inclusion was restricted to those not wanting to get pregnant.
Conversely, it is likely that most women in the undefined intention category (outcome 2) who became pregnant may not have intended to do so. During recruitment for a pregnancy prevention intervention trial with FSWs in Kenya,6 less than 1% of those interested in taking part were planning to get pregnant in the next year (unpublished data). Similarly, in a cohort study included in this review, only 4% of participants expressed an intention to get pregnant at some point during the 12-month follow-up.5 34 A study in South Africa found a higher proportion (10%) wishing to conceive, but this is still a small minority of FSWs. While immediate pregnancy intentions may be low, however, future fertility preferences may be comparable with other women,60 and several authors have highlighted the need for appropriate services that promote safe conception and address FSWs’ need for different forms of protection with different partners.22–24 60
Quality scores were low, but it is important to note that we were assessing how well the studies answered our research question, rather than their own stated objectives. However, there was a notable absence of well-described sampling and recruitment techniques, suggesting that study populations may have been poorly representative of local FSW populations. This may have underestimated pregnancy incidence, as more marginalised members of the population, who are at greater sexual risk, are harder to reach and recruit by convenience or snowball methods. Indeed, the only study to use a random sampling approach found moderately high incidence of pregnancy (intention undefined; 15 per 100 person-years), despite 30% IUD coverage in this population.53 Furthermore, inclusion criteria limiting more than half of the studies to HIV negative women contributed to selection bias, particularly in sub-Saharan African studies, where HIV prevalence among FSWs is estimated at 37%.61 This may partly explain the observation that pregnancy incidence in sub-Saharan Africa was lower than Asia, despite the fact that total population fertility rates are lower in Asia. Higher quality scores seen in the Asian studies may also account for this discrepancy.
Quantitative analysis identified study duration as a clear contributor to heterogeneity in both outcomes. Incidence was lower in shorter studies and decreased over time within studies that reported incidence at multiple time points.32 35 This is due in part to the analytical approach, taken by all but one study,33 of censoring women’s person-time when they first become pregnant. As study subjects at highest risk fall pregnant early, they are censored early and cannot contribute additional pregnancies to the numerator. The remaining lower risk women are less likely to experience the outcome. The same phenomenon has been observed in closed cohorts with the outcome of HIV incidence.62 In addition, sexual risk behaviours often reduce over time in longitudinal studies, because of social desirability bias or health education from study participation,33 36 or attrition bias,63 which may have been a factor for 12 studies in this review with low or unreported retention rates among FSWs.
While measurement bias did not emerge as a significant source of heterogeneity, there was ambiguity in the reporting of pregnancy measurement, and it was often dependent on authors’ recollections. There was a weak positive association between study quality and incidence rates in the pregnancy (intention undefined) group. The lack of a clear relationship may be because quality issues can result in either an underestimate or overestimate of incidence.
Limitations
This review had a number of limitations. Foremost was the inclusion of studies in which (unintended) pregnancy incidence was not an a priori objective, which was the case for all but one. This likely resulted in methodological issues affecting participant selection and pregnancy measurement.
We also adopted a broad approach to other inclusion criteria. Several studies conducted in the late 1990s and early 2000s were included, which may be problematic as family planning coverage has grown and fertility rates declined since that time. The heavy reliance on authors to provide unreported data was a limitation and may have introduced bias, and older data often could not be accessed.
We used a broad definition of sex work, which may have increased the heterogeneity of the outcomes. However, this definition reflects the reality that there are many reasons for women to sell sex, which depend on local laws, culture and economies, and to arbitrarily limit to full-time sex workers, for example, may exclude studies of ‘hidden’ FSWs who are often especially vulnerable.64 65
Our analysis was limited by high heterogeneity, which prevented us from pooling overall rates or performing meta-regression to tease out the influence of different variables. Heterogeneity was not fully explained by explorative subanalyses and may in part be due to the low number of studies, low quality and incomplete data on risk factors. It should be noted that interpretation of these descriptive heterogeneity statistics require a certain level of caution, specifically where the number of cases is small. Variations in baseline population risk probably contributed significantly to heterogeneity, but these could not be quantified due to the incomplete and/or inconsistent measurement of risk factors between studies. Cultural, legal and economic contexts, such as cultural norms around motherhood and abortion law, also vary considerably between the different settings in which the studies took place, and influence fertility preferences, expression of pregnancy intention and access to prevention methods and abortion. These contextual factors could not be accounted for in our analysis.
Another limitation was that we were unable to directly compare rates of pregnancy between FSWs and other populations. Very high pregnancy incidence has been observed in HIV studies among women not categorised as sex workers66 67; however, these women were at high risk for HIV for other reasons (eg, multiple partners). Among the general population, unintended pregnancy incidence is estimated at 5.4 per 100 person-years in the developing world, and eight in Africa,68 substantially lower than the rates among FSWs presented here. Of the three studies in this review, which reported incidence for a broader study population as well as an FSW subgroup, two reported higher incidence36 42 and one reported approximately equal incidence44 in the FSW subgroup compared with the whole study population.
Conclusion
Ultimately, this review demonstrates a concerning lack of research on an issue which is a priority for many FSWs in low-resource settings. This is surprising as we found many studies on HIV incidence and prevention in this population, for which unintended pregnancy is both relevant to the primary outcome and may indicate overall sexual risk. There has been a modest increase in family planning availability for women in many countries since the early 2000s69 70; however, this has not been accompanied by research on whether these additional services have reached FSW populations or impacted on pregnancy rates. Access to family planning, particularly long-acting reversible contraceptives, may be improved by better targeting of FSWs through mobile outreach71 and integration with existing FSW-specific HIV prevention services, and by careful training of health workers and community workers in contraceptive counselling and follow-up.71 Also, it is important that concerted efforts are made to link FSWs who become pregnant with maternal health services, including services for antiretroviral treatment and preventing HIV transmission to infants.
This review found that studies measuring pregnancy incidence among FSWs were of low overall methodological quality and had highly varied results but that unintended pregnancy incidence was high overall and, based on available data, higher than the general population. There is an urgent need for quality research on unintended pregnancy incidence, the effectiveness of interventions to reduce it and the best models of reproductive health service provision for this large and stigmatised population.
Acknowledgments
We would like to acknowledge the many study authors who responded to our queries, in particular the following who provided additional data (in alphabetical order): Daniela Abramovitz, Kathy Baisley, Frieda Behets, Liviana Calzavara, Putu Duff, Paul Feldblum, James Iveniuk, Rupert Kaul, Diana Lara, Qun Li, Kate MacQueen, R. Scott McClelland, Mark Milazzo, Kimberly Page, Matt Price, Barbra Richardson, Merlin L. Robb, Steffanie Strathdee, Douglas Taylor, Abigail Norris Turner, Lut Van Damme, Francois Van Loggerenberg, Judith Vandepitte, Nadja Alexandra Vielot, Handan Wand, Deborah Watson-Jones and Helen Weiss. We would also like to thank senior librarian Lorena Romero at the Ian Potter library, who assisted with building the search strategy, and Professor Rory Wolfe, who provided additional statistical advice.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
Footnotes
↵i Our research group has worked closely with a local NGO (International Centre for Reproductive Health, Kenya) which has a long history of collaborating with and providing services for sex workers in Mombasa.
Contributors FHA, SL and MSCL conceived of and designed the study. All authors contributed to the protocol. FHA performed the search, screening, data extraction and analysis and drafted the manuscript. MC advised on search strategy. LW performed duplicate screening and extraction. PAA advised on analytical methods. All authors reviewed drafts and approved the final manuscript.
Funding This work was supported by the Australian National Health and Medical Research Council, which provided funding for the study (Project Grant GNT 1087006), a Career Development Fellowship for SL and a Postgraduate Scholarship for FHA.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available.