Article Text

Abstract
Objective Although public subsidies and physician recommendations for vaccination play key roles in increasing childhood vaccination coverage, the association between them remains uncertain. This study aimed to identify the association between awareness of public subsidies and recommendations for Haemophilus influenzae type b (Hib), Streptococcus pneumoniae (pneumococcal conjugate vaccine (PCV)) and human papillomavirus (HPV) vaccinations among primary care physicians in Japan.
Design This is a cross-sectional study.
Setting In 2012, a questionnaire was distributed among 3000 randomly selected physicians who were members of the Japan Primary Care Association.
Participants From the questionnaire, participants were limited to physicians who administered childhood vaccinations.
Primary and secondary outcome measures The primary measures were participants’ awareness of public subsidies and their recommendation levels for Hib, PCV and HPV vaccines. Multiple logistic regression analysis was performed to investigate the association between awareness and recommendation, with adjustment for possible confounders.
Results The response rate was 25.8% (743/2880). Of 743 physician respondents, 434 were included as analysis subjects. The proportions of those who recommended vaccinations were 57.1% for Hib, 54.1% for PCV and 58.1% for HPV. For each vaccine, multivariable analyses showed physicians who were aware of the subsidy were more likely to recommend vaccination than those who were not aware: the adjusted ORs were 4.21 (95% CI 2.47 to 7.15) for Hib, 4.96 (95% CI 2.89 to 8.53) for PCV and 4.17 (95% CI 2.00 to 8.70) for HPV.
Conclusions Primary care physicians’ awareness of public subsidies was found to be associated with their recommendations for the Hib, PCV and HPV vaccines. Provision of information about public subsidies to these physicians may increase their likelihood to recommend vaccination.
- primary care
- health policy
- preventive medicine
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to focus on the association between awareness of primary care physicians (PCPs) concerning vaccination subsidies and those PCPs’ recommendations for vaccinations for children.
To explore the characteristics of PCPs found associated with less vaccination recommendation, multivariable logistic regression analysis was performed with background factors such as the physician’s postgraduate year, proportion of paediatric patients and experience raising children as a parent.
Although participants were randomly selected, one limitation was non-responder bias, which was due to the PCPs’ voluntary participation in the survey.
Another limitation was that the generalisability of the results to PCPs outside of Japan was unclear.
Introduction
Vaccination has proven to be a successful and cost-effective health intervention in preventive care.1 Vaccination against Haemophilus influenzae type b (Hib) is a successful example. In the USA, the introduction of the Hib vaccine reduced the incidence of invasive Hib disease by 99%,2 while in Kenya a 93% decline was seen following vaccination.3 Therefore, many childhood vaccines (including Hib) are routinely provided, especially in higher income countries, where coverage is relatively high.4–8
In Japan, however, many important vaccines, including Hib, Streptococcus pneumoniae (seven-valent pneumococcal conjugate vaccine (PCV)) and human papillomavirus (HPV), were voluntary rather than routine, and voluntary vaccinations were not covered by the National Immunisation Programme, without subsidies by the Government of Japan.9 These vaccines were introduced in Japan in the following years: Hib in 2008, PCV in 2010 and bivalent HPV in 2009. There were no public subsidies for them at the time they were initially offered. Without public subsidies, patients must pay an out-of-pocket fee, and this cost burden may serve as a barrier to receiving vaccination.9 Routine vaccinations are defined by the Preventive Vaccination Law and scheduled in the National Immunisation Programme. These vaccinations are not mandatory, although the Government of Japan strongly recommends them. In principle, vaccinations are administered individually, mainly funded by the national and local governments, and free of charge to recipients in private or public facilities at the request of the local government.9 10 Coverage of traditional, routine vaccinations (eg, those for diphtheria, tetanus and measles) is high, and their associated diseases are well controlled.9 11 12 However, coverage of voluntary vaccinations is much lower, and some diseases those vaccinations target are endemic in the population.9 12 The Hib vaccine, for example, was first introduced to Japan in 2008 on a voluntary basis and had estimated coverage of 5%–10% in 2010.13 Therefore, the Government of Japan implemented subsidies for local governments for Hib, PCV and HPV vaccine fees from November 2010, all at the same time.14 The subsidies were intended for all children aged over 2 months and under 5 years for Hib and PCV, and all girls aged 12–16 years for HPV.15 Local governments determined the subsidy amounts. All local governments have now started providing public subsidies for these three vaccines.
It is generally accepted that recommendation of vaccination, to children and their parents by a physician, is important for increasing coverage.14 16–19 Primary care physicians (PCPs) provide care for all ages, from children to older people, and play a key role in childhood vaccination as vaccine providers as well as paediatricians. However, no previous studies have examined PCPs’ level of awareness of public subsidies for childhood vaccines in Japan, and the association between this awareness and recommendations for vaccination. Therefore, this study aimed to examine this association among PCPs in Japan for the Hib, PCV and HPV vaccinations.
Methods
Study design, setting and population
This study used a cross-sectional design with data drawn from a questionnaire conducted by the Japan Primary Care Association (JPCA), the largest academic association for PCPs in Japan. The majority of the JPCA physician members were internists working as PCPs at a clinic or hospital. The survey was conducted in September–November 2012. In total, 3000 physicians were randomly selected from among the 5977 JPCA physician members. Selection was made using a random number list. Subject participants were then selected from among these 3000 physicians in accordance with the inclusion and exclusion criteria. The inclusion criteria were physicians who were JPCA members and who administered childhood vaccination (defined as those who administered at least one of the Hib, PCV and HPV vaccines in daily medical practice). The exclusion criteria were physicians who were retired or living out of Japan or within 2 years of their postgraduate year, as the latter group are classified as ‘junior residents’ in Japan. Questionnaire items were based on previous studies.16 17 19–28 We used a self-administered, anonymous questionnaire design and collected data on the participating PCPs’ main practice category, practice setting (clinic, hospital or other), local government of the practice, population under jurisdiction of the local government, and experience as a kindergarten or other school physician. Questionnaires were sent to each participant by postal mail. Additional details are given below.
Patient and public involvement
Patients and other members of the public were not involved in this study.
Main exposure
The main exposure of this study was physicians’ awareness of the existence of local government public subsidies for the target vaccine (awareness of public subsidy). For each vaccine, respondents were asked ‘Does the local government of your place of practice subsidize the vaccination?’ The response options were ‘Yes’, ‘No’ and ‘I don’t know’. Answers of ‘Yes’ were defined as ‘awareness of public subsidy’. Answers of ‘No’ or ‘I don’t know’ were defined as ‘no awareness of public subsidy’.
Main outcome
The main outcome of this study was PCPs’ active recommendation of a target vaccine to children and the children’s parents in daily medical practice (‘recommendation’). For each vaccine, the respondents were asked ‘How do you recommend a target vaccine to vaccinees and their parents?’ The response options, on a Likert-type scale, were ‘Always recommend’, ‘Maybe recommend’, ‘No opinion’, ‘Not recommend actively’ and ‘Not recommend’. Answers of ‘Always recommend’ were defined as ‘recommendation’. ‘Maybe recommend’, ‘No opinion’, ‘Not recommend actively’ and ‘Not recommend’ were defined as ‘no recommendation’.
Possible confounders
Possible confounders were the physician’s sex, postgraduate year, a proportion of paediatric patients (paediatric patients in the total patient population) that was high (≥10%) or low (<10%), and experience raising children as a parent. We added in these data from the questionnaire and also used public information held by the local government to investigate the type of the subsidy (full subsidy or not) for the three vaccines for each participant.
Statistical analyses
Logistic regression analysis was performed for each target vaccine (Hib, PCV and HPV) to investigate the association between PCPs’ awareness of a public subsidy for the target vaccine and their recommendation of that vaccine. Then, multiple logistic regression analysis was performed to investigate the association between awareness and recommendation, adjusting for possible confounders (full subsidy or not, physician’s sex, postgraduate year, proportion of paediatric patients and experience raising children).
The analysis subjects were set after excluding participants with missing data for the main exposure, main outcome and possible confounders (mentioned above).
All statistical analyses used two-tailed tests of significance, with significance set at 0.05. Analyses were performed with Stata/SE V.13.1. Sensitivity analysis was performed for each vaccine using another method of recategorisation to reflect the dichotomisation of the dependent variable (recommendation), with the response option ‘Maybe recommend’ included in ‘recommendation’.
We obtained written informed consent from all participants before we conducted the survey.
Results
Study flow and demographics
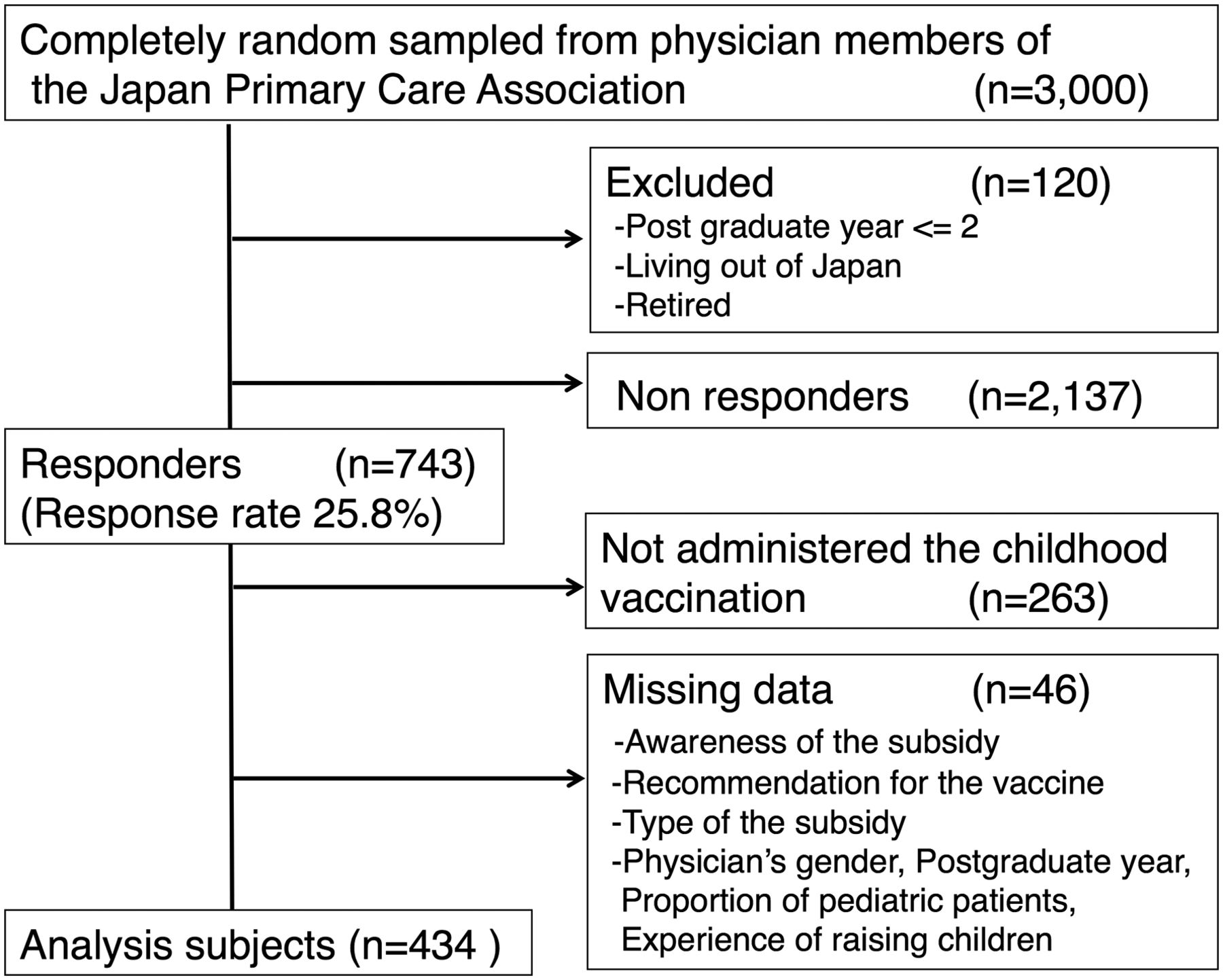
Of the 3000 randomly selected PCPs, 120 were excluded based on the inclusion and exclusion criteria, leaving a sample of 2880. We received responses from 743 PCPs, for a response rate of 25.8%. The respondents were from all 47 prefectures of Japan. Of these respondents, 480 (64.6%) administered childhood vaccinations. We analysed data for 434 (58.4%) after excluding 46 (6.2%) with missing data for covariates (figure 1). The majority of these PCPs were men, of postgraduate years 11–40, reported a clinical category of primary care, reported their practice setting as clinic and had experience raising children (table 1).
Participants’ characteristics
{kind=link}
Study flow.
Hib vaccine
The characteristics of PCPs were stratified by recommendation of the Hib vaccine and the association between awareness of an Hib vaccine public subsidy and vaccination recommendation (table 2). We found 327 (75.3%) PCPs reported awareness of a public subsidy and 248 (57.1%) recommended the vaccine. PCPs who reported awareness were significantly more likely to recommend the vaccine than those who were not aware (non-adjusted analysis: OR 6.18, 95% CI 3.77 to 10.12, p<0.001; multivariable analysis: adjusted OR (AOR) 4.21, 95% CI 2.47 to 7.15, p<0.001). A higher proportion of paediatric patients and of PCPs with experience raising children were positively associated with recommendation. However, a higher postgraduate year was inversely associated (table 3).
Primary care physicians’ awareness of public subsidies and recommendation levels for Hib vaccine, seven-valent PCV and HPV vaccine
Association between primary care physicians’ characteristics and recommendation of Hib vaccine
Pneumococcal conjugate vaccine
The characteristics of PCPs were stratified by recommendation of the PCV and association between awareness of a PCV public subsidy and vaccination recommendation (table 2). Overall, 315 (72.6%) PCPs reported awareness of a public subsidy and 235 (54.1%) recommended the vaccine. Physicians who reported awareness were significantly more likely to recommend vaccination than those who were not aware (non-adjusted analysis: OR 8.03, 95% CI 4.84 to 13.32, p<0.001; multivariable analysis: AOR 4.96, 95% CI 2.89 to 8.53, p<0.001). A higher proportion of paediatric patients and of PCPs with experience raising children were positively associated with vaccination recommendation, and higher postgraduate year was inversely associated (table 4).
Association between primary care physicians’ characteristics and recommendation of seven-valent PCV
HPV vaccine
The characteristics of PCPs stratified by recommendation of the HPV vaccine and the association between the awareness of an HPV vaccine public subsidy and vaccination recommendation are presented (table 2). We found that 389 (89.6%) PCPs reported awareness of the public subsidy and 252 (58.1%) recommended the vaccine. Physicians who reported awareness were significantly more likely to recommend vaccination than those who were not aware (non-adjusted analysis: OR 5.03, 95% CI 2.47 to 10.24, p<0.001; multivariable analysis: AOR 4.17, 95% CI 2.00 to 8.70, p<0.001). Experience raising children was positively associated with recommendation, and higher postgraduate year was inversely associated (table 5).
Association between primary care physicians’ characteristics and recommendation of HPV vaccine
Sensitivity analysis
The sensitivity analysis included recategorised outcomes for recommendation of vaccines. The results demonstrated that for each vaccine, PCPs who reported awareness of a subsidy were significantly more likely to recommend vaccination than those who were not aware: AOR 3.52 (95% CI 1.91 to 6.49, p<0.001) for the Hib vaccine, 4.42 (95% CI 2.45 to 7.98, p<0.001) for the PCV, and 5.08 (95% CI 2.29 to 11.25, p<0.001) for the HPV vaccine.
Discussion
This is the first investigation focused on the proportion of PCPs who have awareness of vaccination subsidies and their recommendations of Hib, PCV and HPV vaccines, and the association between awareness of such subsidies and recommendation of vaccination. We found a positive association between physicians’ awareness of the subsidy and their recommendation of vaccination.
These vaccines were recently introduced in Japan: Hib in 2008, PCV in 2010, bivalent HPV vaccine in 2009 and quadrivalent HPV vaccine in 2011. The subsidies for these three vaccines were implemented from November 2010. When subsidies were offered, information about them was conveyed to patients/families and providers through public outlets such as local government websites or public relations magazines. Additionally, public health nurses informed parents at the time the children received health check-ups. Local governments also sent notices about the subsidies to each medical facility and medical association. Gathering of data for this study was conducted in 2012, meaning the results reflect the actual clinical situation after the new introduction of vaccines among PCPs in Japan. The estimated coverage rates for these vaccines in 2012 were 70%–90% for Hib,29 30 80%–90% for PCV29 31 and 65%–75% for HPV.32 33 Our study showed that even among PCPs who administered childhood vaccinations, not all were aware that subsidies existed and not all actively recommended vaccination. Vaccination fees serve as a barrier to vaccination for patients,9 and PCPs need access to information about vaccine costs, especially with regard to public subsidies. Of the three vaccines studied, the HPV vaccine was most commonly recognised by the surveyed PCPs. This was also the most expensive of these vaccines, and healthcare professionals have cited financial concerns as a barrier to vaccination.34 It therefore appears PCPs need to be more aware of available subsidies for this vaccination.
However, the proportions of PCPs’ recommendations were similar for all three vaccines. These proportions were low when compared with those in other countries; for instance, 68% of family physicians in the USA adopted recommendations for PCV vaccination in 2001, 1 year after the Centers for Disease Control and Prevention recommended it.24 In 2008, 50% of the family physicians who administered the HPV vaccine in the USA strongly recommended the vaccine for girls aged 11–12 years and 85% for girls aged 13–15 years.25 However, studies conducted in 2011 reported that 40.0% of physicians (family physicians, paediatricians and obstetricians/gynaecologists) in the USA always recommended HPV vaccination, as did 45.6% of general practitioners in France.35 36 Although the proportion of PCP recommendations of vaccination may differ by country and time of year, recommendations from healthcare providers are important for patients, especially with regard to new vaccine.37
For all three vaccines studied, there was a statistically significant association between PCPs’ awareness of a public subsidy and their recommendation of vaccination. In comparing PCPs who had no awareness of subsidies with those who were aware, the AOR for recommendation was 4.21 for the Hib vaccine, 4.96 for the PCV and 4.17 for the HPV vaccine (tables 3–5). These results suggest awareness is an important factor behind vaccination recommendation. The robustness of our results was demonstrated in sensitivity analysis using another method of recategorisation. Recent studies have highlighted that the cost of vaccination is also a barrier for physicians to recommend vaccination.38 39 Multiple logistic regression analysis showed that, in addition to awareness, a higher proportion of paediatric patients were positively associated with recommendation of Hib and PCV vaccination, and experience raising children was positively associated with recommendation of all three vaccines (tables 3–5). These results suggest provision of information or experience with children on a regular basis may affect PCPs’ recommendations. We also found that a higher postgraduate year was inversely associated with recommendation (tables 3–5). The Hib, PCV and HPV vaccines were recently introduced in Japan, and PCPs with a lower postgraduate year may have greater interest in or knowledge about these vaccines because of their more recent education or training. This suggests providing information about public subsidies to older PCPs may be more effective than providing information to younger PCPs. A study conducted after the introduction of the Hib vaccine in the USA reported younger physicians were more accepting of the vaccine than older ones; this supports our results.40
Our study also suggested PCPs’ awareness of public subsidies, their having more paediatric patients and their having experience raising children were important factors in increasing their recommendations of childhood vaccination. For voluntary vaccinations without public subsidies, governmental introduction of a public subsidy may play an important role in increasing coverage.9 39 41 For vaccinations already subsidised, implementing a plan to inform PCPs about the subsidy and providing PCPs with updated education and information about the vaccine and subsidy system (considering physician characteristics, especially age and those with fewer paediatric patients) may increase the proportion of those who recommend vaccination.
This study did have some limitations. First, there was a potential non-responder bias due to the low response rate. The proportion of younger PCPs (postgraduate years 3–10) was higher among responders in this study than in the target population (table 1); therefore, PCPs who more actively promoted vaccination may have been more likely to respond. The actual levels of PCPs’ awareness and recommendations may be lower. Second, factors such as knowledge of vaccination, including vaccine safety and effectiveness, PCPs’ circumstances or abilities, and PCPs’ experience may have affected their recommendation behaviour.36 We did not investigate PCPs’ knowledge of vaccine safety and effectiveness; therefore, the association between their knowledge of vaccines and their vaccination recommendation behaviour should be investigated in a future study.39 To account for this limitation, we limited our analysis to PCPs who administered childhood vaccinations and we adjusted for the proportion of paediatric patients (factors related to PCPs’ medical care circumstances and abilities). As is a general limitation of observational studies, we did not evaluate the effect of unknown confounding factors. Finally, although the study participants were physician members of the JPCA, the largest society for PCPs in Japan, generalisability of the results to PCPs outside of Japan was unclear. Vaccination policy in Japan also changed after this study was conducted9 10; therefore, an interannual survey is needed to accurately comprehend the current situation of vaccination among PCPs.
Conclusions
In this study, we described the proportion of PCPs’ awareness of existence of public subsidies and their recommendations for the Hib, PCV and HPV vaccines, and revealed a significant association between awareness and recommendation. Even among PCPs who administered childhood vaccinations, there was variability in these two areas. Our results suggest that informing PCPs about public subsidies may increase their recommendations for these vaccines and improve vaccination coverage.
Acknowledgments
We thank the members of the Vaccine Project Team, Japan Primary Care Association (Tadao Okada, Akinari Moriya, Toshio Naito, Koji Ishibashi, Manabu Toyama, Kuniko Nakayama, Rei Suganaga, Takara Mori and Jiro Takeuchi) for implementing this survey; Izumi Maruyama, President of the Japan Primary Care Association, and the head office staff for their corporation in collecting and delivering the questionnaire; all physicians who took part in the survey; and the staff of the Community Medical Support Institute, Saga University (Tsuyoshi Kurata, Yoshio Hisata, Yukiko Yoshioka, Chiemi Hirotaki and Riyo Fukumori) for their contributions to this study. We also thank Adam Goulston, MS, ELS, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
References
Footnotes
Contributors All authors declare they have contributed to this article. YS conducted the questionnaire, designed and implemented the survey, and performed the analysis and interpretation of the data. YY performed the analysis and interpretation of the data and critical revisions. MH conducted the questionnaire, designed the study and performed critical revisions. NF conducted the questionnaire and performed the interpretation of the data and critical revisions. YG performed the interpretation of the data and critical revisions. TK arranged for the sampling and critical revisions. KT performed the interpretation of the data and critical revisions. TS conducted the questionnaire and performed the interpretation of the data and critical revisions. The JPCAVPT implemented the survey and performed critical revisions. SF performed the interpretation of the data and critical revisions. All authors read and approved this manuscript version for submission.
Funding This study was supported by a research grant for the Research on Emerging and Re-emerging Infectious Diseases, Health and Labour Science Research Grants from the Ministry of Health, Labour and Welfare of Japan (H23-SHINKO-IPPAN-017), and a Clinical Research Grant from St Luke’s Life Science Institute.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study protocol was approved by the Institutional Review Board of Saga University Hospital (2012-05-13) and the Kyoto University Graduate School and Faculty of Medicine Ethics Committee (E2528).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.