Article Text

Abstract
Objectives To assess the benefit of waist circumference (WC) measurements during routine conscription medical examination in two military conscription centres in Switzerland. We compared the prevalence of overweight and obesity assessed by body mass index (BMI) with the prevalence of elevated disease risks assessed by WC and waist-to-height ratio (WHtR). We investigated how these measures were associated with systolic blood pressure, physical fitness performance and socioeconomic determinants.
Design Cross-sectional survey.
Setting Two Swiss conscription centres in 2016.
Participants 1548 Swiss male conscripts, 18–22 years old.
Main outcome Prevalences of elevated WC, WHtR and BMI values according to WHO categories. Secondary outcomes include systolic blood pressure, physical fitness performance and endurance performance.
Results Using BMI cut-points, 25.0% of all conscripts were overweight or obese. When applying WC cut-points, 9.2% had an increased disease risk, while 14.8% of the conscripts were at risk using WHtR cut-points. In the BMI range of 25.0–27.4 kg/m2, 3.6% showed an increased disease risk when using WC and 24.6% when using WHtR cut-points. Of the conscripts with a BMI of 27.5–29.9 kg/m2, 72.4% had an increased disease risk using WHtR, and 42.5% when using WC cut-points. Determinants of elevated BMI, WC and WHtR were low occupational status, rural residential area, older age and location in central and Northwest Switzerland. Systolic blood pressure increased with increasing BMI, WC and WHtR. Physical fitness and endurance test performances decreased with increasing BMI, WC and WHtR.
Conclusion In addition to BMI, WC and WHtR add relevant information to the health assessment of young men. However, the prevalence of overweight/increased health risk differed when using BMI, WC or WHtR. Further studies should include measures of body composition to test whether these differences arise from muscular young men within the overweight BMI range, who had a normal WC.
- obesity
- body mass index
- waist circumference
- waist to height ratio
- blood pressure
- physical fitness test results
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- obesity
- body mass index
- waist circumference
- waist to height ratio
- blood pressure
- physical fitness test results
Strengths and limitations of this study
This is the first assessment of waist circumference (WC) measurements in Swiss-German male conscripts, including over 1500 individuals.
We compared WC and waist-to-height ratio with body mass index to assess the association with systolic blood pressure and physical fitness test performance.
We assessed several occupational and regional determinants of weight parameters in young Swiss men.
We cannot exclude WC measurement errors even though we instructed the measuring staff, created an instructive poster and visited measurement sites in the first weeks to ensure a correct measurement technique.
We had only a limited number of potential confounding variables to include in our analyses.
Introduction
Obesity and its detrimental health effects such as cardiovascular diseases (CVD) and type II diabetes are increasing worldwide1 and in Switzerland.2 Data from 2007 show that in Switzerland 27 000 cases of type II diabetes, 63 000 cases of hypertension and 37 000 cases of dyslipidaemia would have been avoided if overweight and obesity could have been kept at the levels reported in 1992.3 In 2006, direct and indirect costs caused by overweight and obesity reached 5.8 billion Swiss francs,4 and in 2012 these costs increased to 8.0 billion.5 Recent studies of schoolchildren6 7 and Swiss Armed Forces conscripts8 9 have shown that rates of overweight and obese children and young adult men have not increased during the past 5 years. Still, in 2015 every fourth conscript was categorised as overweight or obese in Switzerland, therefore potentially carrying an increased risk of disease.10
Epidemiological studies usually assess the prevalence of overweight and obesity by calculating the body mass index (BMI, body weight divided by the square of the body height). However, BMI is only a rough measure of overweight. It cannot distinguish between fat mass and muscle mass, and therefore does not allow drawing health-relevant conclusions about body composition.11 Waist circumference (WC) and waist-to-height ratio (WHtR) are increasingly used to make better inferences about health-related body shape and fat distributions, especially regarding abdominal fat. Although WC is an absolute measure, WHtR is corrected for body height.
BMI and WC differ regarding disease risk assessment within a population.12 Having more or less muscle mass is one of the possible explanations,13 because physical activity also correlates more strongly with WHtR than BMI.14 In fact, abdominal fat is more strongly associated with morbidity and mortality than BMI.15 16 However, to date it remains unclear which anthropometric measurements best indicate risks for diseases such as CVD or type II diabetes.17 18 Although some studies find a stronger association with CVD risk factors in WHtR than BMI, others find similar associations.19–24 Evidence from reviews show that the levels of association with morbidity and mortality outcomes even differ based on the disease of interest.25 26
Most existing studies of overweight and obesity in Switzerland rely on partially self-reported BMI, and the number of existing studies of WC per se and its difference from BMI among the Swiss population and particularly among young people is still small.27–33 This is striking since obese young people tend to carry their overweight into adulthood, which increases risk for morbidity and mortality in later life.34 35 Therefore, continuous and precise monitoring of overweight and obesity among young people as a basis for focused public health interventions could have an impact on the health status of the whole population over the coming decades.
In summer 2016, we investigated the feasibility and the benefit of WC measurements during the routine conscription medical examination in two Swiss Armed Forces conscription centres. Our specific research aims were to compare the prevalence of overweight and obesity based on BMI with the prevalence of elevated disease risks based on WC and WHtR to assess which of these measures better correlates with systolic blood pressure and physical fitness test performance in young men. We also investigated how these measures are associated with other variables such as age, and occupational and regional determinants.
Materials and methods
All Swiss men reaching the age of 19 in a given year are summoned for conscription in one of six Swiss Armed Forces conscription centres based on their official place of residence. Earlier or later conscription is possible, and total coverage of a given birth year is up to 95%.8 The conscription process in Switzerland lasts 2–3 days, depending on the centre. During the medical examination, standard protocols and measurement tools are used in all centres. In addition to health data, occupation and place of residence are recorded. Body height and weight are measured using a stadiometer and a regularly calibrated scale (both SECA), in underwear and without shoes. Among other tests, a physical fitness test consisting of several parts is carried out (more details follow). Blood pressure is measured with calibrated, automatic, upper-arm blood pressure monitors. If the blood pressure is above either the limit of 140/90, the measurement is repeated up to two times, and all results are recorded.
After the Swiss Armed Forces approved our study protocol, our study was conducted at the Swiss conscription centres of Mels (GR) and Windisch (AG) from July 2016 to August 2016. The WC measurements for our study were performed by trained army medical personnel, or by soldiers serving in the conscription process who are specifically trained to measure WC accurately. All army conscripts assessed in the two conscription centres during the study period were included in our study. We regularly observed the measuring procedure during the first weeks to ensure correct measurement technique. We instructed army personnel to use WHO standard protocol to allow an international comparison of our results with other studies.36 In WHO guidelines, WC is measured at the midpoint between the lower end of the rib cage and the upper end of the pelvis, assessed at the lateral side of the body. To ensure a uniform application of this protocol, we created an instructive poster that was displayed in the measuring rooms of both centres. We supplied the army with SECA 201 measuring tapes that allow an automatic and standardised tightening of the tape. The newly collected WC measurements were linked to the routinely collected health and occupational data by the army (Logistikbasis der Armee, LBA San), anonymised, and then sent to the investigator team at the Institute of Evolutionary Medicine at the University of Zurich for analysis.
We calculated BMI (kg/m2) from body height and weight and categorised BMI in accordance with WHO guidelines.1 Because we were particularly interested in the overweight BMI range from 25.0 to 29.9 kg/m2 (in which muscular young men might be misclassified by BMI), we subdivided the overweight WHO BMI category in two subgroups, overweight I (25.0–27.4 kg/m2) and overweight II (27.5–29.9 kg/m2) for our analyses. From WC and body height, we calculated WHtR (cm/cm) and categorised WC (cm) according to WHO guidelines and WHtR according to Ashwell et al 17 (table 1). The physical fitness test at conscription (Test Fitness Rekrutierung, TFR) assesses the physical performance of Swiss conscripts in five aspects of fitness: speed and strength of legs and arms, global trunk strength, coordination and endurance. Performance in each is evaluated with the help of a point scale (0–25 per aspect; in total, maximum 125). This test was previously validated.37 We analysed the TFR total and the endurance test separately. The army ranks the TFR by five performance categories ranging from insufficient to excellent (table 1). If more than one measurement of systolic blood pressure was taken from one conscript, the intraindividual mean was calculated and used in the analysis. Systolic blood pressure was categorised into normal (<140 mm Hg) and elevated (≥140 mm Hg) values.38
Upper part: categorisation of weight and disease risk parameters
Occupational status was based on the self-reported occupation of the conscripts. We used the SocioEconomic Index of Occupational Status to categorise each occupation.39 40 We also divided this index into tertiles. Students and conscripts without a profession or with an imprecise indication of profession (in terms of the official Swiss classification) were categorised in separate groups. We defined cases in which the entry for occupation was labelled ‘insufficient’ (n=23) or ‘without’ (n=102) as imprecise.8 The postal codes of the place of residence were categorised according to the Swiss Federal Office of Statistics to define the location of residence by major region (Grossregion) and urbanicity of the residence.10
Statistical analysis
We calculated descriptive statistics (means, SD, medians) for BMI, WC and WHtR, and compared the prevalence of elevated body weight/disease risk against each other in cross tabulations. We also calculated Pearson correlations between BMI and WC, and between BMI and WHtR. We calculated kappa coefficients41 to assess the agreement between classifications into normal weight, overweight/increased disease risk and obesity/strongly increased disease risk. The kappa coefficient was classified according to Altman’s reference: 0.41–0.60=moderate agreement, 0.61–0.80=good agreement, >0.80=excellent agreement. The associations among BMI, WC and WHtR, and determinants such as occupational status, urbanicity, major region and age were assessed by linear regression. The same method was used when analysing the association between the three anthropometric measures and systolic blood pressure and physical fitness test performance as outcomes. For this outcome analysis, we combined the underweight BMI category (BMI <18.5 kg/m2) and the normal BMI category (18.5–24.9 kg/m2) into one ‘normal’ BMI category of BMI <25.0 kg/m2 to have reference groups comparable to WC (<94 cm) and WHtR (<0.50). The linear regression that assessed blood pressure and physical fitness test results among overweight (BMI 25.0–29.9 kg/m2) young men above or below the respective WC and WHtR thresholds of 94.0 cm and 0.50 against normal BMI conscripts was additionally adjusted for age, occupational status and region of residence. We used the STATA (V.14.2) statistical package for all statistical analyses.
Patient and public involvement
According to Swiss federal law (Bundesgesetz über die militärischen Informationssysteme, BG 510.91, Art. 2, 9, 24–29), the Swiss Armed Forces are authorised to provide the anonymised data for academic research. The Swiss Armed Forces fully anonymised the records by removing all names, social security numbers, ID numbers and exact residential addresses. Because Swiss conscription is mandatory and the anthropometric measurements used in this study are non-clinical, governmental data, informed consent and ethical approval were not needed (Swiss data privacy act, SR 235.1; 19.6.1992 and Federal Act on Research involving Human Beings (Human Research Act, HRA) 810.30; 1.1.2014).8 42 43
Results
In total, 1548 young men were conscripted in the two centres between July 2016 and August 2016 (606 at Mels and 942 at Windisch). WC was available for 1536 conscripts (99.2%). The descriptive results of the anthropometric measurements and health parameters are reported in table 2 (upper table). The prevalence of overweight and obesity (BMI) and the prevalence of increased disease risk (WC and WHtR) differed (table 2, lower table). Using BMI cut-points, 25.0% (95% CI 22.8 to 27.1) of all conscripts were overweight or obese; using WC cut-points, 9.2% (95% CI 7.8% to 10.7%) had an increased disease risk; and using WHtR cut-points, 14.8% (95% CI 13.0% to 16.7%) had an increased disease risk. When comparing BMI and WC (figure 1 and table 3), a large percentage (16.1%, 95% CI 14.5% to 17.9%) of conscripts had a BMI above 25.0 kg/m2 but no increased disease risk (WC <94.0 cm), whereas only a few conscripts (0.3%, 95% CI 0.1% to 0.7%) had a BMI under 25.0 kg/m2 and an increased disease risk (WC ≥94.0 cm). When comparing BMI with WHtR, 11.3% (95% CI 9.6% to 12.8%) were overweight (BMI ≥25.0 kg/m2) with no disease risk (<0.50), whereas 1.0% (95% CI 0.5% to 1.6%) were normal weight with an increased disease risk. Pearson correlation coefficients were high between BMI and WC (r=0.908, p<0.001) and between BMI and WHtR (r=0.912, p<0.001).

Scatter plots of body mass index (BMI) versus waist circumference (WC) (above) and BMI versus waist-to-height ratio (WHtR) (below). The BMI WHO thresholds for normal weight, overweight and obesity are displayed as reference lines on the x-axes, the WC and WHtR threshold reference lines for increased disease risk and strongly increased disease risk are displayed on the y-axes. The solid black lines are the predicted linear regression lines. Orange and red data points indicate overweight and obese conscripts as measured by BMI, but with a WC/WHtR below the risk threshold.
Upper table: descriptive statistics for the anthropometric variables, systolic blood pressure and results of physical fitness test; lower table: absolute and relative frequencies for body mass index (BMI), waist circumference (WC) and waist-to-height ratio (WHtR) categories
Concordance of classification into weight/disease risk categories between body mass index (BMI) and waist circumference (WC) (upper table, n=1536, 100%), and BMI and waist-to-height ratio (WHtR) (bottom table, n=1536, 100%), respectively
If we compare anthropometric measures in conscripts with excessive weight (BMI ≥25.0 kg/m2, n=386), in the overweight I category (BMI 25.0–27.4 kg/m2, n=195), only 3.6% had a WC of more than 94 cm, and 24.6% had a WHtR over 0.5 (online supplementary figure S1). In the overweight II category (BMI 27.5–29.9 kg/m2, n=87), 72.4% of the conscripts had an increased disease risk (WHtR). In the obese BMI category (BMI ≥30.0 kg/m2, n=102), only a minority (8.8% for WC and 1.0% for WHtR) did not have an increased disease risk. The kappa coefficient for agreement between BMI and WC classifications was 0.40 overall (moderate agreement), but only 0.12 (poor) if restricted to conscripts with BMI ≥25.0 kg/m2 (n=384). Similarly, the kappa coefficient for agreement between classification according to BMI and to WHtR was 0.53 overall (moderate agreement), but only 0.08 (poor) if restricted to conscripts with BMI ≥25.0 kg/m2 (n=386).
Supplementary file 1
Linear regressions indicated only a weak association of occupational status with mean BMI (figure 2, left). In fact, only students showed a significant lower BMI than participants of medium occupational status. Conscripts living in urban areas showed a lower BMI than conscripts living in rural areas, and older conscripts showed a higher BMI than younger ones. The results are similar for WC and WHtR (figure 2, middle and right). Values of BMI, WC and WHtR were slightly higher in central Switzerland and the Northwest compared with other regions. However, most associations were not statistically significant or of moderate effect size. For detailed results, see online supplementary table S1.
Supplementary file 2

Coefficient plots showing the results of the linear regressions for the occupational and regional determinants of body mass index (BMI) (left), waist circumference (WC) (middle) and waist-to-height ratio (WHtR) (right).
Systolic blood pressure increased with increasing categories of BMI, WC and WHtR in linear regressions (figure 3, left), with significant differences between all weight/risk categories (p<0.001). Physical fitness test performance and endurance performance decreased with increasing categories of BMI, WC and WHtR (figure 3, middle and right). In general, coefficients in the BMI category overweight II (27.5–29.9 kg/m2) were closer to those in the increased risk categories of WC and WHtR, whereas the coefficients in the overweight I (25.0–27.4 kg/m2) category were closer to the normal reference group. In the categories of obesity (BMI ≥30.0 kg/m2) and of strongly increased disease risks in WC and WHtR, comparable coefficients emerged for all three weight parameters. For detailed results, see online supplementary table S2.

Coefficient plots showing the results of the linear regressions for blood pressure (left), physical fitness test (middle) and endurance test (right), according to body mass index (BMI) (above), waist circumference (WC) (middle) and waist-to-height ratio (WHtR) (below).
When the physical fitness test results were divided by categories of BMI (including overweight I and II), WC and WHtR (online supplementary figure S2), the previously described pattern was evident again, with 54.2% of all conscripts having good to excellent physical fitness results in the overweight I BMI category of 25.0–27.4 kg/m2, whereas 15.7% with a WC of 94.0–101.9 cm had good to excellent physical fitness results and 21.9% with a WHtR of 0.50–0.59 had good to excellent physical fitness results. A similar pattern is apparent for endurance test results, but not for systolic blood pressure.
Supplementary file 3
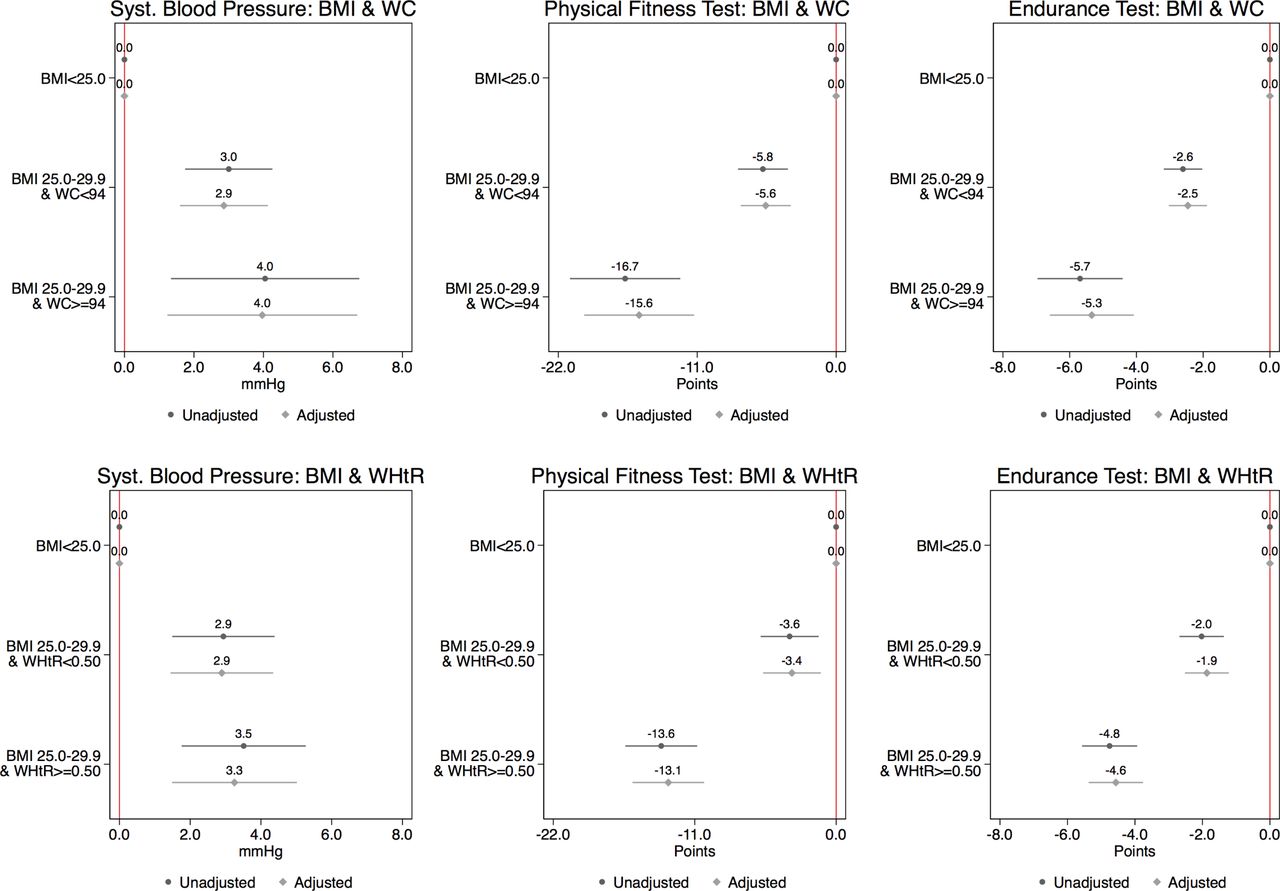
When we subcategorised the conscripts in the overweight BMI category 25.0–29.9 kg/m2 in overweight young men above or below the WC and WHtR thresholds of 94.0 cm and 0.50, and ran linear regressions assessing blood pressure and physical fitness test results among these two subcategories against normal BMI conscripts (BMI <25.0 kg/m2) (figure 4), we found that ‘overweight’ conscripts with normal WC or WHtR clearly performed better in the overall physical fitness test and the endurance test than overweight conscripts with WC or WHtR in the increased risk category. A similar but less pronounced pattern became evident for blood pressure. The coefficients did not change substantially when adjusting the regressions for age, occupational status and region of residence.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coefficient plots showing the results of linear regressions comparing blood pressure and physical fitness test results among overweight (BMI 25.0–29.9 kg/m2) young men above or below the WC and WHtR thresholds of 94.0 cm and 0.50 against normal BMI conscripts. In a second step, the regressions were additionally adjusted for age, occupational status and region of residence. BMI, body mass index; WC, waist circumference; WHtR, waist-to-height ratio.
Discussion
Although in epidemiological settings, BMI is the most common weight and health risk indicator,44 45 the assessments of WC and WHtR are recommended as additional measures to better capture the health risks of elevated visceral fat mass.17 18 In our analysis, we found two thresholds for increased health risk according to WC or WHtR. Because WC and height are correlated, WHtR may be a more effective measurement, and it seems that WHtR best correlates with visceral fat percentage and total fat mass.46 Taking WHtR as the measure, 11.3% (n=172) of all conscripts were classified as overweight by BMI without being at increased health risk, and 1.0% (n=15) were classified as normal weight by BMI despite being at increased health risk. Overweight (BMI 25.0–29.9 kg/m2) conscripts with a normal WC below 94 cm or a WHtR below 0.50 performed markedly better in the total physical fitness and endurance tests than overweight conscripts with elevated WC or WHtR values.
Only a few Swiss epidemiological data sets on WC measurements exist that can be compared with our study. Existing Swiss studies including WC data are based on schoolchildren,27 28 47 older people,29 the Swiss Salt Survey,30 33 the Swiss CoLaus study31 48 49 and the Swiss MenuCH nutrition survey.32 Because young men are rarely included in epidemiological health research studies, large reference samples of WC in young men do not exist for Switzerland. If we compare the prevalence of increased disease risk according to WC between men aged 15–29 years from the Swiss Salt Survey (n=165) and men aged 18–34 years from the MenuCH Survey with our subjects, the results are similar (7.3% vs 8.9% vs 4.7% in the 94.0–101.9 cm category, 6.1% vs 3.9% vs 4.5% in the ≥102.0 cm category). A recently published study of Swiss conscripts in the Italian part of Switzerland had a sample size similar to our study and showed similar results.34 The mean value for WC in that study was 82.0 cm, compared with 80.9 cm in our study. The proportion of Swiss Italian conscripts with WC ≥102.0 cm was 3.6%, compared with 4.5% in our study. Internationally, the study on Austrian 18-year-old conscripts that was performed between 2001 and 2005 is comparable to our study and showed similar results.50 The mean WC value in Austrian conscripts was 81.4 cm, compared with 80.9 cm in our study. These figures show that our sample is comparable to other samples of the same sex and similar ages.
One problem with BMI is that it cannot distinguish between muscle mass and fat mass. Our study revealed that this problem might be of special relevance in young men with BMI of 25.0–27.4 kg/m2. Our analysis indicated that both WC and WHtR classify conscripts as being at an increased disease risk only from BMI 27.5 kg/m2 onwards. The associations of variables such as physical fitness test performance and endurance test performance with BMI, WC or WHtR differed more in the category of overweight/increased disease risk than in the category of obesity/strongly increased risk. Furthermore, the analysis showed that health risks in overweight conscripts might be underestimated if assessed by BMI alone because of the inclusion of the healthy muscular men in this category. WC and WHtR seem to classify health risks better because healthy muscular men are not included in the slightly elevated risk category. In the British National Diet and Nutrition Survey, 67% of men were overweight and 24% were obese, whereas 53% had a WC ≥94, and 30% had a WC ≥102. According to the WHtR, 76% had a value ≥0.5% and 20% had a value ≥0.60.42 These figures are higher than our results because men of all age groups were included. However, the differences among obesity/increased risks according to BMI, WC and WHtR are not as strong as in our study, confirming that the problem of muscular men in the overweight category of BMI is probably an issue in young men only. We conclude that in the BMI range of 25.0–27.4 kg/m2, the truly overweight conscripts should be differentiated from the muscular conscripts to better assess whether and to what extent slight overweight increases health risks in both groups (taking into account additional information such as family history, smoking, nutrition, etc).
The strength of our study is that this is the first investigation of WC measurements in Swiss-German conscripts, totalling over 1500 individuals, which compared WC and WHtR with BMI to assess the association with systolic blood pressure and physical fitness test performance, as well as with occupational and regional determinants of weight parameters. One limitation was that we could not exclude interobserver errors in WC measurement even though we instructed the measuring staff, created an instructional poster and visited measurement sites in the initial weeks. In addition, because of a tight time schedule during the conscription process it was not possible to measure the WC of each conscript two times, by two persons. Generally, circumference measurements suffer from methodological challenges such as interobserver and intraobserver variability.51 52 It is therefore relevant to use standardised measurement protocols, well-trained measuring staff and validated measuring instruments.53 Another limitation was that we corrected for only a limited number of potentially confounding variables in our analyses. For instance, a number of conscripts were still undergoing professional training and it was not possible to classify these conscripts into occupational groups. We lacked further indicators such as income.
In addition to BMI, the measurement of WC and the calculation of WHtR adds relevant information to the health assessment in young men. Our results need to be confirmed at the national level. To verify our findings and find the best combination of weight and health indicators to predict health outcomes in epidemiological studies, we recommend measurements of body shape, body composition and metabolic parameters. A combination of BMI, WC and WHtR performs best in assessing disease risk.54 In addition, repeated measurements of the same persons over longer periods can reveal which indicators perform best at predicting disease risk in later life and disclose potentially changing risk profiles. Further studies should include women, and cohort studies should assess changes in body shape and composition over the life course from childhood to old age in the general population.
Acknowledgments
Franz Frey, Franco Muggli, Tiziano Angelelli, Radoslaw Panczak, Marcel Zwahlen, Murielle Bochud, David Fäh, Isabelle Herter-Aeberli, Pedro Marquez-Vidal, Arnaud Chiolero, Jean-Pierre Pfammatter, Petra Cadetg, Matthias Bopp, Nadine Stoffel-Kurt, Andrea Poffet, Kathrin Favero, Thomas Wyss and Hans-Peter Stamm for technical input and discussions; Christopher Ritter for English editing; Andreas Stettbacher (Chief Medical Surgeon of the Swiss Armed Forces) for providing the data; MicroGIS SA for support in data management; and, in particular, the medical-technical staff of the conscript centres of Mels and Windisch for WC measurements.
References
Footnotes
Contributors Conceived and designed the WC measurements: KS, NB, JF and NK. Coordinated collection of data and prepared data for analysis: AN, SSM and AT. Analysed the data: KS and NB. Wrote first draft: NB and KS. Commented on paper: all authors. Obtained funding: KS, FJR and NB. Obtained routine army data: KS, FJR and NB.
Funding This work was supported by the Swiss Federal Office of Public Health FPO (contract number 16.008898) and Mäxi Foundation (Zurich).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are generated and owned by the Swiss Armed Forces. The data and the permission to use them are available from the Swiss Armed Forces (Logistikbasis der Armee-LBA San) on submission and approval of a study protocol.