Article Text

Abstract
Objective It is well known that climate variability and trends have an impact on human morbidity and mortality, especially during the winter. However, there are only a handful of studies that have undertaken quantitative investigations into this impact. We evaluate the association between the UK winter asthma mortality data to a well-established feature of the climate system, the Scandinavian (SCA) pattern.
Methods Time series analysis of monthly asthma mortality through the period of January 2001 to December 2015 was conducted, where the data were acquired from the UK’s Office for National Statistics. The correlations between indices of important modes of climate variability impacting the UK such as the North Atlantic Oscillation as well as the SCA and the asthma mortality time series were computed. A grid point correlation analysis was also conducted with the asthma data with sea level pressure, surface wind and temperature data acquired from the European Centre for Medium-Range Weather Forecasts.
Results We find that sea level pressure and temperature fluctuations associated with the SCA explain ~20% (>95% CL) of variance in the UK asthma mortality through a period of 2001–2015. Furthermore, the highest winter peak in asthma mortality occurred in the year 2015, during which there were strong northwesterly winds over the UK that were the result of a sea level pressure pattern similar to that associated with the SCA.
Conclusions Our study emphasises the importance of incorporating large-scale geospatial analyses into future research of understanding diseases and its environmental impact on human health.
- asthma
- geographical mapping
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Asthma mortality incorporated all ages and nationwide data.
Advanced time series and geospatial analysis, using high-resolution climate data.
Only few studies incorporating large geospatial climate analysis have been conducted to understand asthma mortality.
This study only explains a fraction of variance in asthma mortality due to a well-known geospatial climate pattern; however, other factors such as individual lifestyles or socioeconomic status were not considered.
Introduction
Despite numerous years of research, chronic respiratory diseases still remain a vital concern to the public worldwide.1 This is especially true for asthma which is a significant cause of impaired quality of life, and is now one of the most common chronic diseases in the UK2–4 with ~5.4 million individuals receiving treatment for it.2 3 The seasonality of asthma is well documented in the UK, where episodes of asthma, admissions to hospital and mortality for older age groups have been noted to peak during mid-winter.5 6 Past studies have suggested cross-infections from increased indoor crowding,1 as well as patient’s socioeconomic status7 as being responsible for this winter peak.
Indeed, socioeconomic indicators of well-being (poverty, income inequality, deprivation and fuel poverty) were found across 14 European countries to be associated with excess winter mortality.7 Despite numerous studies conducted on the epidemiology of asthma, taking into account the seasonality, hospitalisations, emergency department visits and socioeconomic status, there exists limited studies on the influence of climate patterns on asthma mortality. Particularly, it is unclear if there are any large-scale geospatial modes of climate variability that may help provide information and ultimately predictability that may guide future health interventions and policies.
Geospatial climate patterns, or teleconnections are long range, spatially coherent and time varying regions of atmospheric variability that are important in understanding changes in the climate system.8 The pioneering work on these geospatial climate patterns began in the early 1900’s with the interest in forecasting the intensity of the Indian summer monsoon.9 Out of this work came the discovery of the El Niño Southern Oscillation, an important geospatial climate pattern which is characterised by zonal fluctuations in sea surface temperatures across the tropical Pacific Ocean that vary on interannual timescales.10 11 Arguably, the most dominant climate pattern over the North Atlantic region is the North Atlantic Oscillation (NAO).12 13 Although the NAO remains dominant throughout the year, it is most pronounced during the winter and accounts for ~33% of the total variance in sea level pressures over the North Atlantic region.12 13 Recent European research has shown that the NAO has human health impacts,14 urban air quality15 as well as hospital admissions.16
Another important geospatial climate pattern over the North Atlantic region is the Scandinavian (SCA) pattern, which has a primary sea level pressure centre of action over western Norway with an opposing centre of action over the Northeastern Atlantic near Greenland.13 17 18 The SCA has been shown to influence precipitation, temperatures and cyclone activity across Northern Europe during the winter.13 18 In particular, the positive phase of the SCA is associated with higher precipitation over the UK and colder surface air temperatures over the northeastern North Atlantic.18
Changes in sea level pressures and surface temperatures are widely known to impact the respiratory system as well as other health conditions, including cardiovascular diseases19 and neurological activity.20 21 However, climatological variables such as sea level pressure, surface wind and surface temperature experience variability on large geospatial scales. Thus, we hypothesise that these large-scale patterns or teleconnections17 may play a role in understanding variability of health outcomes. In this study, we show the importance of the SCA, a mode of climate variability, on the UK asthma mortality in the past decade. This research will allow a broader audience, from clinicians to climate scientists in understanding the asthma epidemics in the UK.
Methods
Asthma data
Monthly asthma mortality occurrences for all ages in the UK, specifically England and Wales, from January 2001 to December 2015 were obtained from the Office for National Statistics (ONS), reference number 005955. The underlying cause of death was defined using the International Classification of Diseases tenth revision codes J45-J46 ‘Asthma’. The winter season was defined to be the months of December through February. During the winter season, the UK has exhibited an average ~125 deaths due to asthma, whereas the summer season averaged to ~77 deaths from 2001 to 2015. Thus, the winter season exhibited nearly ~62% greater asthma deaths than the summer from 2001 to 2015, leading our study to focus on the winter season.
Patient and public involvement statement
For this study, patients and/or public were not involved.
NAO and SCA indices
For the years of 2001–2015, the mean winter (December–February) NAO and SCA indices were obtained from the National Oceanic and Atmospheric Administration. The winter NAO and SCA account for ~33% and~14% of the total variance in sea level pressures over the North Atlantic region since 2001.12
Geospatial climate data
Mean winter (December–February) geospatial sea level pressures, surface zonal and meridional winds as well as surface temperatures were obtained from the ERA-Interim (ERAI) re-analysis dataset.22 The ERAI is the latest global atmospheric re-analysis produced by the European Centre for Medium Range Weather Forecasts, with a resolution grid of 0.75° by 0.75°.22
Grid point correlations
The SCA is primarily an atmospheric pressure pattern. For completeness, we also considered the NAO as well. However, the winter NAO index resulted in no significant correlation to the winter asthma mortality time series (r=~0.1). The winter asthma mortality time series and the winter SCA index were correlated to geospatial fields of sea level pressures, surface zonal and meridional surface winds as well as surface temperatures. The geospatial grid point correlations were restricted to the longitude domain of 40°W-40°E and a latitude domain of 40°N-70°N and for the period 2001–2015. At each grid point, the correlation between the winter asthma mortality time series and the various winter mean meteorological time series was calculated resulting in spatial correlations maps that reflect the relationship between asthma mortality and climate variability. A similar process was also undertaken to identify the climate signal associated with the SCA.
Statistical analysis
The winter asthma mortality time series and the winter SCA index were first normalised by subtracting the mean in the raw signal and then dividing by the standard deviation. After normalising, the asthma mortality time series and SCA index were then detrended by subtracting the trend from the original signal. In computing a correlation and/or spectral analysis of time series, it is necessary to remove the trend from the data, a procedure known as detrending.23 In fact in some cases, without removing the trend from the data, the correlation between two time series may result in a larger magnitude, than if detrended.23 This would result in a measurement bias of the variance suggesting it to be higher than it may be expected, since the variance in the trend is also being accounted for. For this reason, we chose to detrend the asthma data. Furthermore, the asthma data and geophysical fields (ie, sea level pressures, surface winds and surface temperatures) were found to have a serial correlation from one year to the next, resulting in red noise spectra that are characterised by a reduction in the number of degrees of freedom.24 For this reason, the statistical significance (>95% CL) of correlations were determined from a Monte Carlo simulation, generating 10 000 synthetic time series with the same spectral characteristics as the original time series.25 Thus, the distribution of correlations from the set of synthetic time series were used to estimate the statistical significance of the actual result. All figures were produced using Matlab 2012b.
Results
The time series analysis of monthly asthma data in the UK from January 2001 to December 2015 (figure 1), illustrates clear seasonal peaks during the winter months (figure 1A). The median in asthma mortality is 89.5 deaths/month. In addition, the greatest number of deaths due to asthma in the UK occurs during the winter season (December–February) with a median of 125.7 deaths/month (figure 1B). The specific month with the largest number of deaths due to asthma was in January, with a median of 138.9 deaths, whereas September was found to have the lowest with a median of 70.1 deaths. The winter of 2015 had the highest number of deaths due to asthma with an average of 143.7 deaths/month, where the maximum occurred in January 2015 with 211 deaths.
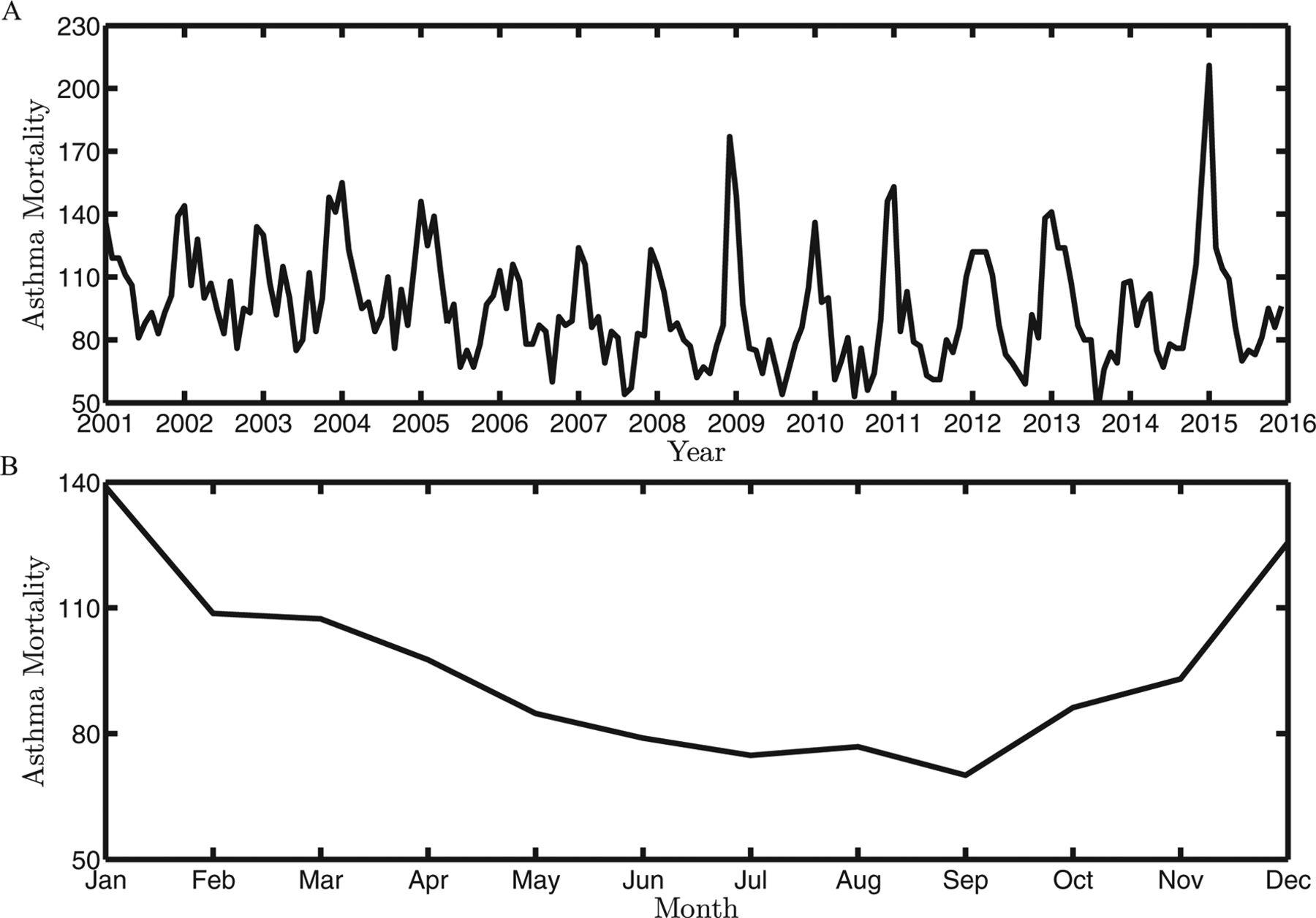
(A) The time series analysis of monthly asthma data. (B) Total monthly mean asthma mortality cases. These plots are shown from 2001 to 2015.
To investigate the existence of a coherent climate signal associated with asthma mortality, we first correlate the mean winter asthma mortality time series to geospatial sea level pressures along with surface winds (figure 2A) and surface temperatures (figure 2B). The correlation with sea level pressures reveal a clear dipole pattern with centres over the Eastern Atlantic (high) and Western Europe (low). This sea level pressure correlation pattern would result in clockwise (ie, anticyclonic) surface winds over the UK. The geospatial correlation with the surface winds is consistent with this and figure 2A shows that higher mortality are associated with statistically significant northwesterly winds across the UK. This flow would result in a cooler climate over the UK and is consistent with the correlation to surface temperatures (figure 2B). This East-West dipole pattern noted from figure 2A is seen with high asthma deaths, occurring during the winter; however, we would expect to see the opposite pattern with low asthma deaths.
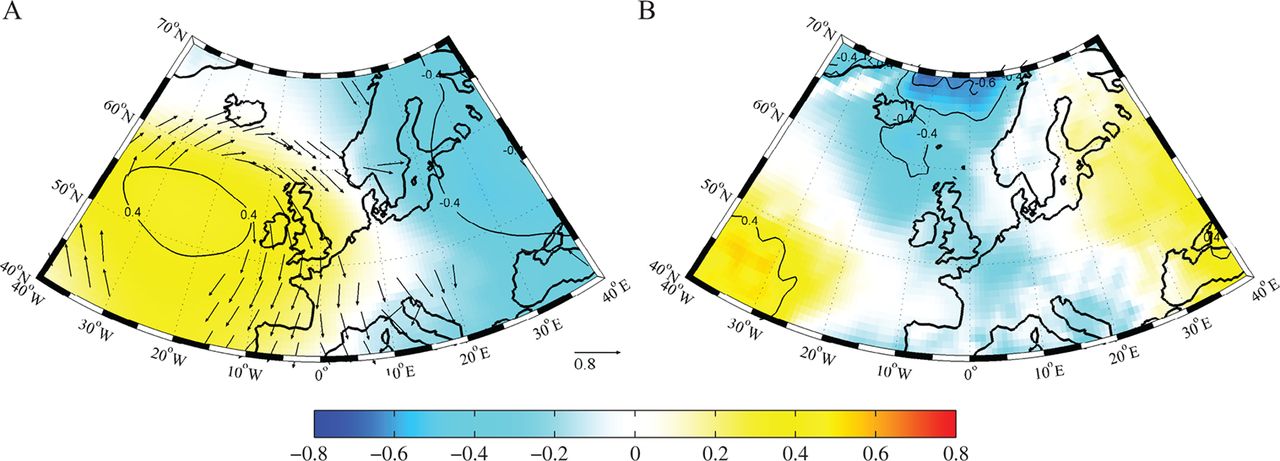
Geospatial correlation of winter asthma mortality time series to (A) sea level pressures and surface winds, along with (B) surface temperatures from 2001 to 2015. The statistically significant (>95% CL) correlations with surface winds have been shown, whereas contoured for the geophysical fields.
To confirm if the association between the mean winter asthma mortality time series to sea level pressures, resembled the SCA, we did a similar grid point correlation with the winter SCA index to sea level pressures and surface winds (figure 3A) as well as surface temperatures (figure 3B). Figure 3A shows a clear dipole pattern, which resembles the correlation pattern shown in figure 2A with centres over Western Europe (high) and Scandinavian regions (low). As seen from figure 3A, the positive phase of the SCA brings statistically significant northwesterly winds across the UK. By comparing figures 2A and 3A visually, the grid point correlations show a resemblance in dipole patterns of sea level pressures. However, this similarity does not extend to the correlation with the surface temperatures.

Geospatial correlation of winter Scandinavian index to (A) sea level pressures and surface winds, along with (B) surface temperatures from 2001 to 2015. The statistically significant (>95% CL) correlations with surface winds have been shown, whereas contoured for the geophysical fields.
The correlation coefficient between the winter asthma mortality time series and winter SCA index from 2001 to 2015 was found to be 0.43 (95% CL), as shown in figure 4. This suggests that the variability in the SCA has a ~20% influence on the UK asthma mortality during the winter season. For additional evidence of a geospatial climate pattern’s influence on the UK deaths due to asthma, we also looked at the atmospheric circulation during 2015, as this year had the highest number of winter asthma deaths over the period of interest. From figure 5A it is clear that sea level pressure anomalies were large (±12 hPa), with centres of action over the Norwegian Sea (low) and North Atlantic Ocean (high). This North-South dipole anomaly in 2015, brought northwesterly flow over the British Isles, causing a cooling over the UK and Eastern Atlantic (figure 5B).

Normalised winter asthma mortality time series and the winter Scandinavian index from 2001 to 2015.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Anomalies of geospatial winter sea level pressures (hPa) and surface winds (m/s), along with (B) surface temperatures (°C) for the year 2015. These 2015 anomalies were compared with the climatology during the period of 2001 to 2015.
Discussion
In the UK, asthma is a significant contributor to mortality, morbidity and healthcare utilisation, as well as financial costs to the public sector.5 26 In a time-span of one year (2011–2012), asthma resulted in ~6.3 million primary care consultations, ~93 000 patient hospitalisation episodes, where the average total costs were estimated to be ~£1.1 billion in the UK.26 Additionally, seasonality plays a vital role in asthma general practice episodes, hospital admissions and mortality.5 Our analysis is consistent with previous work that indicated a ‘U’-shaped pattern of the UK asthma mortality seen across the chronological 12 months in a given year, with highest asthma mortality observed in mid-winter.5
It is known that colder temperatures during the winter are associated with increased admission rates for respiratory causes across Europe.1 Breathing cold air through either the nose or the mouth causes airways to constrict resulting in inflammatory changes and airway hyper-responsiveness.27 A study in Finland has noted that colder climate-related respiratory symptoms are relatively uncommon (2.0%–7.0%) in healthy young adults, they are substantially increased (19.2%–51.4%) among those individuals with asthma, regardless of with or without allergic rhinitis.27
Our results indicate that there is a statistically significant correlation between the UK winter asthma mortality time series and a sea level pressure gradient across the British Isles. In such a situation, winters with an increase in asthma mortality would tend to be associated with northwesterly wind flow that would result in colder and presumably damper conditions over the UK. In addition, the sea level pressure correlation patterns bear some resemblance to the SCA. Indeed, an index of the SCA explains ~20% of the UK asthma mortality during the winter season.
Hence, winter asthma mortality time series and the winter SCA index were found to have a positive association (figure 4). For example, during the winters seasons of the years 2002, 2004 and 2015, the SCA index was above normal and these winters did indeed have above average asthma mortality in the UK. During the period of interest, the highest mortality due to asthma occurred in the winter of 2015. For this winter year, the anomalies in sea level pressure, surface wind and temperature (figure 5) were consistent with the geospatial correlations (figure 2 and 3). In particular, there was a North-South pressure dipole across the UK that was associated with northwesterly wind flow. This North-South dipole resembles the geospatial SCA. Furthermore, these strong winds over East Atlantic resulted in cooler temperatures during the winter of 2015, which is consistent with recent literature finding that the North Atlantic and Western Europe experienced extremely cold sea surface temperatures during the winter season of 2015.28
Conclusions
In this study, we find that asthma mortality in the UK is associated with a coherent geospatial structure in the surface climate of the North Atlantic and Western European regions. This pattern transfers northwesterly wind flow across the UK from the North Atlantic, resulting in colder regional temperatures. Previous work has noted a correlation between winter admission rates for respiratory illness and temperatures in Europe.1 This pattern bears some resemblance to an important winter geospatial climate pattern, the SCA. Approximately 20% of the variance in the UK winter asthma mortality from 2001 to 2015 can be explained through the SCA climate pattern. Hence this work suggests that geospatial climate patterns can have an influence to human health and consequently, additional future research should be conducted to further understand such a connection. We believe that this may result in improved forecasts of asthma mortality. Overall, we recommend that a geospatial approach to understanding chronic respiratory diseases be used in future studies of environmental impact on human health.
Acknowledgments
The authors would like to thank the editor and the anonymous reviewers for their constructive comments, which helped us to improve the manuscript.
References
Footnotes
Contributors HM conceived and designed the study as well as the figures. GWKM contributed to the data and statistical analysis. Both authors contributed equally to the writing and revising of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.