Article Text

Abstract
Objectives Homeless people lack a secure, stable place to live and experience higher rates of serious illness than the housed population. Studies, mainly from the USA, have reported increased use of unscheduled healthcare by homeless individuals.
We sought to compare the use of unscheduled emergency department (ED) and inpatient care between housed and homeless hospital patients in a high-income European setting in Dublin, Ireland.
Setting A large university teaching hospital serving the south inner city in Dublin, Ireland. Patient data are collected on an electronic patient record within the hospital.
Participants We carried out an observational cross-sectional study using data on all ED visits (n=47 174) and all unscheduled admissions under the general medical take (n=7031) in 2015.
Primary and secondary outcome measures The address field of the hospital’s electronic patient record was used to identify patients living in emergency accommodation or rough sleeping (hereafter referred to as homeless). Data on demographic details, length of stay and diagnoses were extracted.
Results In comparison with housed individuals in the hospital catchment area, homeless individuals had higher rates of ED attendance (0.16 attendances per person/annum vs 3.0 attendances per person/annum, respectively) and inpatient bed days (0.3 vs 4.4 bed days/person/annum). The rate of leaving ED before assessment was higher in homeless individuals (40% of ED attendances vs 15% of ED attendances in housed individuals). The mean age of homeless medical inpatients was 44.19 years (95% CI 42.98 to 45.40), whereas that of housed patients was 61.20 years (95% CI 60.72 to 61.68). Homeless patients were more likely to terminate an inpatient admission against medical advice (15% of admissions vs 2% of admissions in homeless individuals).
Conclusion Homeless patients represent a significant proportion of ED attendees and medical inpatients. In contrast to housed patients, the bulk of usage of unscheduled care by homeless people occurs in individuals aged 25–65 years.
- homeless
- hospitalised
- epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Use of large hospital-wide dataset including all emergency department presentations and medical admissions.
Presentations to other hospitals not captured.
Identification of homeless patients based on self-reported address at time of presentation to hospital as either no fixed abode or emergency accommodation, individuals giving an address of family or friends not identified as homeless.
Absence of data on the duration and nature of homelessness.
Introduction
Homeless people lack a secure, stable place to live. There are a variety of definitions of homelessness1: the European Typology of Homelessness and Housing Exclusion defines a person as roofless or homeless if they have a identification deficit in at least two of the following: no dwelling, no legal title to a place for exclusive possession, and no private and safe space for social relations.2 This definition of homelessness includes those who are sleeping rough (ie, those sleeping in the open air); those living in emergency accommodation such as a hostel, night shelter or B&B accommodation; those living with family and friends, or in a squat. Homelessness may be chronic (lasting >1 year), intermittent or short-term/crisis-related.3 In November 2015, the Dublin Regional Homeless Executive reported 3615 adults in emergency accommodation and a minimum of 91 individuals sleeping rough in Dublin.4
Homelessness is associated with ill-health. Many homeless people have multiple simultaneous chronic conditions, termed multimorbidity.5 The simultaneous trimorbidity of physical ill-health, mental ill-health and drug or alcohol misuse is highly prevalent in homeless people.6 Diseases related to alcohol and/or drug addiction including cirrhosis, infective endocarditis, abscesses, venous ulcers, infection with hepatitis C and HIV are more prevalent in homeless than housed people.7 In addition, studies from the USA and Canada have reported earlier onset in homeless people of frailty and other geriatric syndromes usually seen in older adults.8–10
Homeless people have been reported to use relatively little primary care,11 and often use the emergency department (ED) as their initial point of contact with healthcare. Internationally, homeless people have been reported to attend ED three to five times more frequently than housed individuals.12–15 Rates of inpatient admissions of homeless persons have also been found to be higher14 16 17 with longer length of stay (LOS) and increased readmission rates.17 18
We sought to compare the age profile and use of unscheduled ED and inpatient care between housed and homeless individuals in Dublin, Ireland.
Methods
Study setting
We carried out an observational cross-sectional study using data on all ED visits and all unscheduled admissions under the general medical take (internal medicine) in St James’s Hospital, Dublin, in 2015. St James’s Hospital is a large university teaching hospital serving adults resident in the south inner city in Dublin, Ireland. Patient data are collected on an electronic patient record (EPR) within the hospital and is also collected in the national hospital in-patient enquiry (HIPE) system, a computerised health information system designed to capture demographic, administrative and clinical data on all inpatient discharges from publicly funded acute hospitals in Ireland. Diagnoses recorded on the HIPE system are determined by trained coders on examination of patient records.
Data extraction
All ED attendances and unscheduled inpatient stays between the 1 January and 31December 2015 (inclusive) were extracted from hospital databases. Individuals were identified by a unique identifier (medical record number). LOS and outcomes of ED attendances and inpatient admissions were extracted from the hospital patient record.
Patients admitted under any medical specialty participating in the general medical take (internal medicine acute admissions) rota or under infectious diseases were defined as medical inpatients. This did not include patients admitted under geriatrics, neurology, nephrology, oncology, haematology, psychiatry or any surgical specialty. Geriatrics, neurology, nephrology, oncology and haematology were excluded because they do not participate in the unselected internal medical take. Age was defined as the age of the patient on the date of discharge from hospital. Patients without recorded address were excluded.
Operational definition of homelessness
Homeless individuals were defined as those with recorded addresses of no fixed abode (NFA) or any emergency accommodation (homeless hostels). Addresses were extracted from the patient record. Addresses are obtained from patients by trained receptionists on registration in the ED and are checked at each admission. The names and/or street addresses of homeless hostels were obtained from the Dublin Regional Homeless Authority Case Management website. The address field in the patient record was manually screened to identify addresses corresponding to homeless hostels. In addition, any addresses with more than two patients presenting from the same address within the calendar year were scrutinised to identify potential homeless hostels.
To assess the sensitivity of identifying homeless patients based on the address field in the EPR, patients who were referred to the Social Work Department for advice on homelessness were checked against those identified as homeless using the previous method.
Operational definition of housed and homeless population of catchment area
The catchment population of the hospital was obtained from previous publications.19 The homeless population of Dublin was taken from data collected by the Dublin Regional Homeless Executive,20 and the proportion of those falling within the catchment area of the hospital was estimated by consensus by the authors and by the head of research in the Dublin Regional Homeless Executive.
Data analysis
Data were analysed using SPSS. Mann-Whitney tests were used to compare differences in age and LOS between housed and homeless patients. Chi-squared was used to compare categorical data between housed and homeless patients. Spearman’s rank correlation coefficient was used to assess the association between age and LOS in housed and homeless patients.
Results
The catchment population of St James’s Hospital, Dublin is reported as 270 000. The homeless population sleeping rough or in emergency accommodation (hereafter referred to as homeless) of the catchment area was estimated as 1000 individuals, resulting in a prevalence of homelessness of 0.4% of the population of the catchment area.
Two-hundred and fifty address fields (including NFA and numerous homeless hostels as well as multiple spelling variants of the homeless hostels) were identified as homeless addresses and individuals giving these addresses as their current address were defined as homeless.
Hundred homeless patients were identified from referrals to hospital social workers for advice on homelessness. Seventy-two per cent of these had an address on their electronic patient record that had been identified as homeless.
Five ED attendances and 12 inpatient admissions had no address recorded.
ED attendances
The demographics of all ED attenders are described in table 1.
Demographics of ED attenders
Homeless individuals accounted for a disproportionally high number of ED attendances per proportion of the catchment population. Out of an estimated 1000 homeless adults in the catchment area, 909 (91%) homeless adults presented to the ED over this time period compared with 30 865 (11.4%) of 270 000 housed individuals in the catchment area. The rates of attendance per year were increased in homeless individuals and they accounted for increasing proportions of attenders with >4/year or >12/year attendances to the ED. Homeless ED attenders were predominantly males (table 2).
Demographics of housed and homeless ED attenders
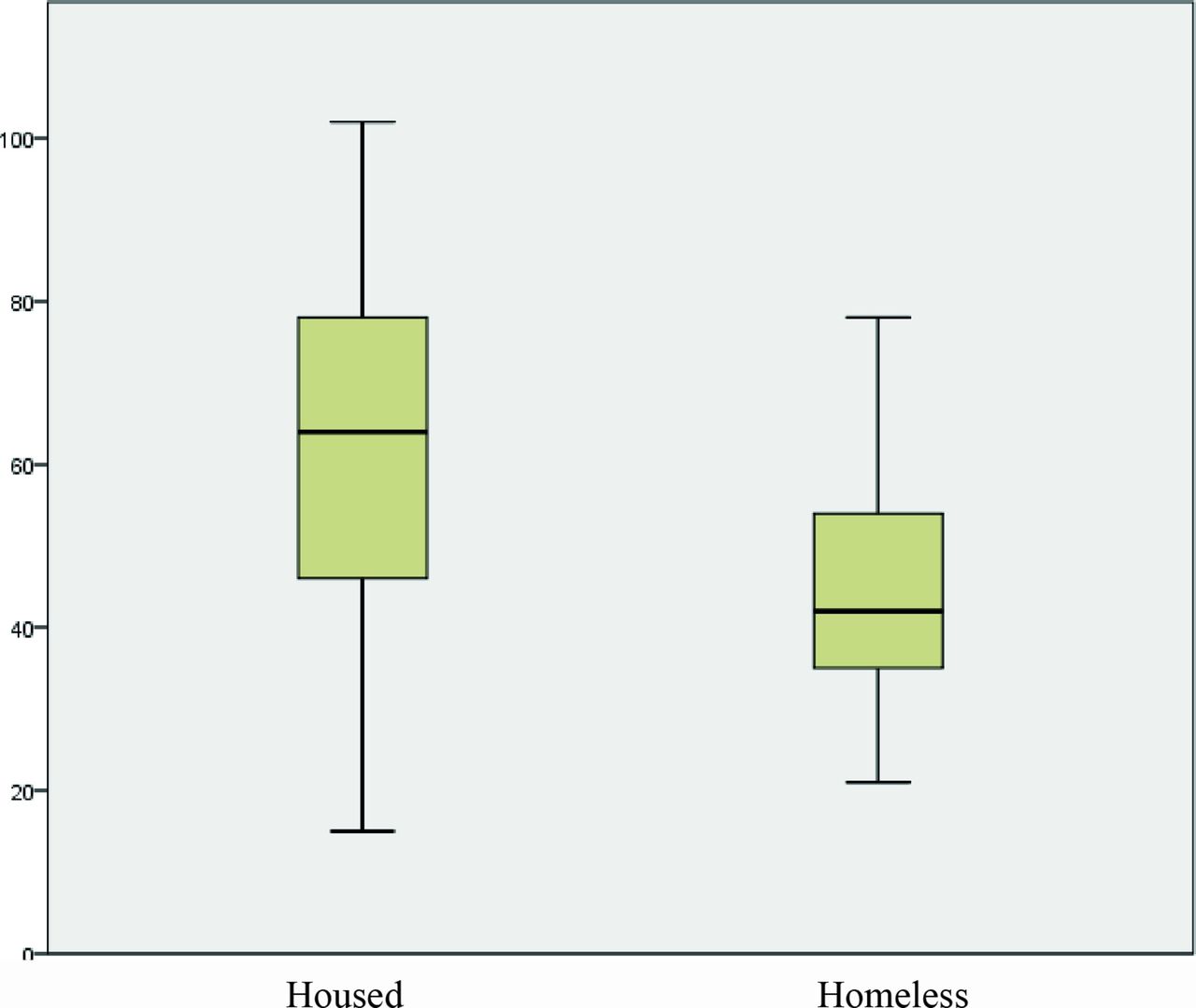
Homeless ED attenders are younger than their housed counterparts
The mean age of homeless ED attendees was 39 years (17–76) (95% CI 37.2 to 40.8), whereas that of housed ED attendees was 45 years (16-102) (95% CI 42.1 to 47.9) (figure 1). The difference in distribution of age was statistically significant (Mann-Whitney, P=0.000).

Age of housed and homeless ED attenders. ED, emergency department.
Homeless ED attenders were much more likely to leave the ED without being assessed or against medical advice (table 3). Rates of admission to the hospital in those who remained for assessment and management were similar between housed and homeless.
Outcomes of ED attendances
Patient presenting complaints were recorded at triage. These were then ranked in order of frequency in housed and homeless presenters (table 4). Presentations related to drug and alcohol use and mental health were more common in homeless ED attenders.
ED presenting complaints
Acute medical admissions
A total of 5104 individuals had unscheduled general medical admissions in 2015 (table 5). Seventy-five per cent of admissions were in individuals aged >45 years. Homeless individuals demonstrated a >10-fold increase in usage of unscheduled general medical inpatient bed days per capita of the catchment area compared with housed individuals (table 6). In contrast to housed medical inpatients, the majority of homeless medical inpatients were men.
Demographics of unscheduled medical admissions
Characteristics of housed and homeless unscheduled medical admissions
The mean age of homeless medical inpatients was 44.19 years (95% CI 42.98 to 45.40), whereas that of housed medical inpatients was 61.20 years (95% CI 60.72 to 61.68) (figure 2). The distribution of age was significantly different between the two groups (P=0.000, Mann-Whitney) (figure 3).
Age of unscheduled medical admissions.

{kind=link}
{kind=link}
{kind=link}
Bed days by age group.
Bed days in patients aged ≤64 years accounted for 33.8% (27 274/80 633) of bed days generated by all housed medical admissions, versus 88.3% (3689/4176) of bed days generated by all homeless medical admissions. This difference was statistically significant (P=0.000, Χ2). Bed days in patients aged ≤44 years accounted for 10.8% (8734/80 633) of bed days generated by all housed medical admissions, versus 49.1% (2050/4176) of bed days generated by all homeless medical admissions. This difference was statistically significant (P=0.000, Χ2) (figure 3).
Use of unscheduled healthcare is age-related in housed, but not homeless people
Increasing age was strongly correlated with LOS in housed medical inpatients (Spearman correlation 0.257 (0.233–0.292, P<0.005), whereas this was not the case in homeless medical inpatient (Spearman correlation −0.034 (−0.222 to 0.155, P=0.12)).
The 10 most frequent primary diagnoses for housed and homeless medical inpatients were determined (table 7). Acute respiratory diagnoses were frequent in both populations. Diagnoses associated with injecting drug use (abscesses and venous thromboembolic disease) and hepatitis C and/or alcohol use (hepatic failure and haematemesis) were more common in homeless inpatients. Cardiovascular disease (congestive heart failure and atrial fibrillation) were less common in homeless inpatients.
A higher proportion of homeless inpatients self-discharged against medical advice (table 8).
Primary diagnoses in unscheduled medical admissions
Outcome of admission
Discussion
Homelessness is a state of extreme socioeconomic deprivation, and is associated with increased morbidity and increased use of unscheduled hospital care (ED visits and admissions). We found that, in Dublin, homeless individuals have a 20-fold increased use of ED and over 10-fold increased use of unscheduled medical inpatient bed than housed individuals. These findings are similar, although the relative increase is higher in Ireland, to those reported from the USA, Canada and the UK.8 13 21–26
It is important to note a number of key demographic differences between homeless individuals in the USA and those in high-income European countries such as Ireland. Homeless populations in the USA include a high proportion of veterans and of ethnic minorities and those in Australia and Canada include a high proportion of individuals reporting themselves as Aboriginal/First Nation.5 Homeless people in Dublin are predominantly white Irish, with 4% reporting themselves as Irish Traveller.6 Very few Irish people are combat veterans. Eighty per cent of adults in emergency accommodation or rough sleeping in Dublin in January 2016 were ≤44 years old,4 20 this contrasts with the ageing homeless population reported in the USA.27 In Dublin, homelessness is strongly associated with drug use: up to 70% of homeless individuals report having used illegal drugs with over half reporting injecting drugs.6 Free primary and secondary healthcare is available to those in the lowest one-third income bracket in Ireland.
In our study, homeless patients were much more likely to leave the ED without being seen (41% vs 16% in housed patients). Patients who leave the ED without being seen have been reported to represent the failure of an emergency care delivery system to meet its goals.28 These rates are similar to those reported by Svoboda in Toronto29 and higher than those reported from London.30 Anecdotally, some of the homeless individuals who leave without being seen may have simply been seeking shelter for the night in the ED waiting room, with others requiring medical attention leaving due to withdrawal from alcohol and/or opiates and attention deficit hyperactivity disorder-related difficulties with waiting. Homeless medical inpatients were also much more likely to self-discharge against medical advice.
Homeless individuals accounted for a grossly disproportionate amount of inpatient bed days relative to their proportion of the catchment population. Cardiovascular presentations (congestive heart failure, atrial fibrillation and chest pain) were less common in homeless than in housed patients, whereas diseases related to alcohol and drug use (abscesses, hepatic failure and haematemesis) were more common in homeless patients. Seizures were also more common in homeless patients, which may result from the increased rate of traumatic brain injury and substance use in this population. Both groups presented frequently with syncope, pneumonia and exacerbation of chronic obstructive pulmonary disease/asthma. These presentations are common in elderly housed populations, but are seen in homeless patients at a significantly younger age.
We demonstrate a striking difference in the age profile of homeless patients compared with housed patients. The median age of homeless medical inpatients was 20 years younger than that of housed patients. Most bed days generated by homeless patients were in patients <65 year of age, which contrasted with the housed population. Of note, we excluded unscheduled and elective admissions to the Geriatric service, which consist solely of housed individuals >70 years of age. Work by Kushel et al8 on homeless veterans in the USA also reported a younger median age in homeless hospital patients with a 5–16 year difference in median age between homeless and housed veterans presenting with medical conditions. Earlier mortality in homeless people may account for their relative under-representation in older inpatients.
Limitations of this study include that presentations to other hospitals were not captured, and that diagnoses were captured by non-clinician coders. An additional limitation of the study was that identification of homeless patients was based on the address recorded on the patient electronic record, with an estimated under-reporting rate of 30% and an inability to identify those who gave the address of a family member or friend. Estimates of the proportion of the homeless population of Dublin within the catchment area of the hospital are crude, and there is a significant degree of mobility of homeless people within the city. However, the differences in usage of acute unscheduled care are so dramatic that even an underestimation of the homeless population by 100% in our study would result in a homeless population in the catchment area of only 2000 individuals, and the dramatic increase in use of unscheduled healthcare in homeless individuals compared with housed individuals would remain. Strengths of the study include the large number of patients included and the ability to focus analysis on medical inpatient admissions (thereby excluding psychiatric inpatient admissions).
Conclusion
Homelessness is associated with ill-health and dramatic decreases in life expectancy. In this study, we demonstrate that homelessness is also associated with a dramatic increase in the per capita use of costly unscheduled acute healthcare. A failure to address the structural causes of homelessness results in increased costs to society through increased use of healthcare, in addition to social care and opportunity costs. In contrast to housed patients, the bulk of usage of unscheduled care by homeless people occurs in individuals aged 25–65 years. Earlier mortality in homeless people may account for their relative under-representation in older inpatients. Primary and ambulatory care for homeless people, if aiming to prevent costly inpatient admissions, will need to cater a significantly younger population than services for housed individuals.
References
Footnotes
Contributors CNC: literature search, figures, study design, data collection, data analysis, data interpretation and writing of manuscript. SC and DC: data collection. JB, JK, CB, RAK and DB: editing of manuscript. FOR and AOC: literature search, data collection and editing of manuscript. RS: statistical advice.
Funding This work was supported by the Health Research Board and Health Services Executive under the grant NSAFP/2009/2.
Competing interests All authors have completed the Unified Competing Interest form and declare: support from the Health Research Board, Ireland (HRB) and the Health Services Executive, Ireland (HSE) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years, no other relationships or activities that could appear to have influenced the submitted work.
Ethics approval The study was approved by the Joint Research Ethics Committee of St James’s Hospital and the Adelaide and Meath Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.0k8c4