Article Text

Abstract
Objectives To determine disparities in rates, length of stay (LOS) and hospital costs of potentially preventable hospitalisations (PPH) for selected chronic conditions among Aboriginal and non-Aboriginal South Australians (SA), then examine associations with area-level socioeconomic disadvantage and remoteness.
Setting Period prevalence study using linked, administrative public hospital records.
Participants Participants included all SA residents in 2005–2006 to 2010–2011. Analysis focused on those individuals experiencing chronic PPH as defined by the Australian Institute of Health and Welfare.
Primary outcome measures Number and rates (unadjusted, then adjusted for sex and age) of chronic PPH, total LOS and direct hospital costs by Aboriginality.
Results Aboriginal SAs experienced higher risk of index chronic PPH compared with non-Aboriginals (11.5 and 6.2 per 1000 persons per year, respectively) and at younger ages (median age 48 vs 70 years). Once hospitalised, Aboriginal people experienced more chronic PPH events, longer total LOS with higher costs than non-Aboriginal people (2.6 vs 1.9 PPH per person; 11.7 vs 9.0 days LOS; at $A17 928 vs $A11 515, respectively). Compared with population average LOS, the standardised rate ratio of LOS among Aboriginal people increased by 0.03 (95% CI 0.00 to 0.07) as disadvantage rank increased and 1.04 (95% CI 0.63 to 1.44) as remoteness increased. Non-Aboriginal LOS also increased as disadvantage increased but at a lower rate (0.01 (95% CI 0.01 to 0.01)). Costs of Aboriginal chronic PPH increased by 0.02 (95% CI 0.00 to 0.06) for each increase in disadvantage and 1.18 (95% CI 0.80 to 1.55) for increased remoteness. Non-Aboriginal costs also increased as disadvantage increased but at lower rates (0.01 (95% CI 0.01 to 0.01)).
Conclusion Aboriginal people’s heightened risk of chronic PPH resulted in more time in hospital and greater cost. Systematic disparities in chronic PPH by Aboriginality, area disadvantage and remoteness highlight the need for improved uptake of effective primary care. Routine, regional reporting will help monitor progress in meeting these population needs.
- potentially preventable hospitalisation
- length of stay
- hospital costs
- primary care
- indigenous population
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- potentially preventable hospitalisation
- length of stay
- hospital costs
- primary care
- indigenous population
Strengths and limitations of this study
This is the first study to examine variations of total length of stay and direct hospital costs associated with chronic potentially preventable hospitalisations (PPH) among Aboriginal and non-Aboriginal Australians.
The study uses a complete collection of person-linked public hospital records over a 6-year period from 2005–2006 to 2010–2011.
The study provides a baseline for reporting of a health system performance measure focusing on individuals as well as populations experiencing chronic PPH.
Person-linked private hospital records and death records were not available to the study.
Hospital records for a group of the most vulnerable residents living in very remote areas and hospitalised in other jurisdictions were not included.
Background
Chronic health conditions are increasingly important contributors to poor population health throughout the world.1 The increased prevalence and duration of these conditions adds to the mounting pressure on health systems to respond to those needs. Hospital expenditures are a key component of these systems.2 Australia is an example of a developed and advantaged setting where annual hospital expenditure represents the largest recurrent and growing contribution3 4 to the average health expenditure of $6639 per person.5
In constrained budgetary environments, hospital performance measures are constantly scrutinised for efficiency gains. For example, inpatient length of stay (LOS) is closely associated with hospital cost6 and reimbursements,7 and Australia employs LOS in a suite of health system performance measures.3 8 From a hospital’s perspective, LOS indicates production of care adequate to meet clinical need while maximising bed availability and minimising treatment costs. From a patient perspective, hospital LOS means maximising quality outcomes from care while minimising risk of exposure to adverse events in hospital and time away from usual, societal roles.
Potentially preventable hospitalisations (PPHs) are another performance indicator making use of administrative data.9–11 Under different names such as potentially avoidable hospitalisations or ambulatory care sensitive conditions, and with some variations in conditions and coding,12–14 PPHs are widely adopted as an indicator of a community’s capacity to benefit from available and effective15–18 primary healthcare by: ‘preventing the onset of an illness or condition, controlling an acute episodic illness or condition, or managing a chronic disease or condition’ (p. 163).19 Primary healthcare is the second most expensive component of Australia’s health system at almost $55 billion annually.4 Recent expert commentary argued Australia’s primary health system provides around half the level of care recommended for chronic conditions that contributes to chronic PPH $2 billion annual cost to the health system.20 Therefore, PPHs provide an important junction between two critical system components in which policy makers and health planners can consider both the technical efficiency of one sector, its effect on another sector and opportunities to adjust allocations across sectors. Efficient use of healthcare resources can maximise health outcomes in the community served.21
Equitable distribution of health is another challenging21–24 but high priority21 for contemporary health systems. PPHs result from a complex interplay of person-related,25 26 health system, geographical27 and socioeconomic factors28–30 that highlight the need for directing resources towards appropriate and accessible health services.24 Localised understanding can help inform local responses to health need.21 31 While their underlying data do not refer to individuals, Australia’s Institute of Health and Welfare (AIHW) does work towards this by reporting aggregated PPH time series by age group, sex, state/territory jurisdictions, socioeconomic disadvantage, remoteness and Aboriginal and Torres Strait Islander status (herein respectively referred to as ‘Aboriginal’).32 Overall PPH rates are three times higher for the Aboriginal population compared with non-Aboriginal Australians,32 33 which supports their designation as a disadvantaged group in terms of their use of primary health care.34 This is consistent with indigenous population comparisons in the US,35 Canada36 and New Zealand.37 Chronic PPH conditions account for much of PPH for which there is a fivefold difference in the hospitalisation rates by Aboriginality.32 33 Australian reporting of chronic PPH conditions9 focuses on primary diagnoses of: angina, asthma, chronic obstructive pulmonary disease (COPD), congestive cardiac failure, diabetes complications, hypertension, iron deficiency anaemia, nutritional deficiencies and rheumatic heart disease (specific diagnosis and procedural criteria for chronic PPH are listed in online supplementary table A). While the indicator could be further developed by including other conditions such as chronic kidney disease,38 discrete chronic PPH conditions currently reported for angina, COPD,38 congestive cardiac failure39 40 and rheumatic heart disease41 are each associated with disparities between Aboriginal and non-Aboriginal populations. A particularly significant area is that of PPH from diabetes complications, the most frequently reported chronic PPH among Aboriginal Australians.32 42–45 Similar disparities in chronic PPH between Aboriginal and non-Aboriginal populations are reported across Australia’s states and territories of Victoria,45 the Northern Territory,44 Queensland,46 Western Australia,47 New South Wales48 and South Australia (SA).49 50
Despite considerable evidence of variations in PPH rates and LOS, relatively little is known about how the two measures covary.51 Given the extent of disparities in chronic PPH rates by Aboriginality, this appears an opportune place from which to improve understanding of who in the community is more likely to experience potentially unnecessary, prolonged and costly hospitalisation. The first of only two studies that considered chronic PPH and LOS together focused on diabetes hospitalisations among older, Hawaiian people categorised as either Asian, islander or white.52 The second Australian study considered results for individuals on the basis of Aboriginal identity.48 The results affirmed higher chronic PPH rates among Aboriginal people compared with non-Aboriginal contemporaries of the same age, sex and living in the same geographic area. Moreover, elevated rates were accompanied by LOS that was 4% higher on average.48 However, neither study explicitly describes the variation of chronic PPH and LOS rates within the populations studied, yet evidence in other areas point to considerable within-population heterogeneity in health outcomes. For example, analysis of premature mortality among Aboriginal South Australians showed an interaction between area level socioeconomic disadvantage and remoteness where the social gradient between disadvantage and premature mortality outcomes increased as remoteness increased.53
None of the recently reviewed literature on PPH and LOS analysed the costs associated with the hospital events. Such information is critical to inform complex commissioning decisions of the opportunity cost, at least from a health system perspective, of pursuing technical and allocative efficiencies while reducing the human and societal costs represented by a person’s time out of role.
If health systems are to attend to the needs of people and populations, it is important to focus on individuals and subpopulations in their localised setting. This focus will benefit from supplementing AIHW reporting, based on unlinked data, with administrative records linked to individuals and their use of services. The latter are becoming more routinely available in Australian states and territories. Using these in quantifying disproportionate hospitalisation, rehospitalisation and time spent in hospital while simultaneously describing the system resources involved can provide valuable information on which elements of the health system are working, for whom and in what context.2 54
This study considers the disparity between rates of PPH for chronic conditions for Aboriginal and non-Aboriginal South Australians. It examines the association between area level socioeconomic disadvantage, geographic remoteness and the frequency, length and cost of hospitalisation for chronic PPH within those populations. This paper addresses three questions: which individuals experienced chronic PPH?; how does the LOS and cost of hospitalisation for these conditions vary between Aboriginal and non-Aboriginal populations?; and what is the relationship between the ecological risk factors of area level socioeconomic position and remoteness with PPH for chronic diseases within these populations?
Methods
Ethics approval
Research ethics committee approvals are held from SA Health (467/08/2014) and the Aboriginal Health Council of South Australia (04-11-406).
Study design
A period prevalence study using linked, public hospital administrative records.
Data sources
Hospital separations
Details of the universally available healthcare for patients admitted to public hospitals are collated at time of their discharge, or separation, from hospital then added to the Integrated South Australian Activity Collection (ISAAC) maintained by SA Health, the state government’s lead health agency. The term ‘separations’ is used synonymously with ‘admissions’14 51 55 56 and ‘hospitalisations’12 18 25 30 40 45 48 52 reported in other research referenced by our study. Chronic PPH within ISAAC records for financial years 2005–2006 to 2010–2011 were categorised using AIHW criteria for ICD-10 primary diagnoses and relevant procedure codes.57 ISAAC includes mandatory fields of age, Aboriginal identification and Statistical Local Area (SLA) of usual residence. Residents of the Anangu Pitjantjatjara Yankunytjatjara Lands (APY Lands) access over 95% of their hospital services in the neighbouring jurisdiction (at Alice Springs Hospital in the Northern Territory).58 This activity is not recorded within ISAAC so any residual APY resident hospitalisations were removed from hospital and population denominator counts.
Hospital costs across the period were calculated in a uniform manner using Australia’s National Efficient Price for public hospital healthcare activity in 2015–20167 and expressed in Australian dollars. These prices are based on each separation’s Australian Refined Diagnostic Related Group (v7.0) with loadings for outlying LOS, Aboriginality (4%) and area remoteness (ranging from an additional 8% in outer regional to 22% for very remote areas).
Hospital separations for individuals
Analysis of separations for individual people was facilitated by probabilistically linked project keys from SA-NT DataLink, an organisation within Australia’s data linkage network. These keys enabled grouping of each person’s separations across hospitals and time. Each individual’s records were assigned the last recorded age and the SLA recorded in that person’s index, or first occurring, separation. Aboriginality was categorised on the basis of a person having identified as Aboriginal in any hospital separation during the observation period. Identification of Aboriginal status can be difficult and introduce misclassification bias.59 Accordingly, a more stringent definition for sensitivity analyses was based on a person identifying as Aboriginal on more than 75% of records.
Population and statistical geography
South Australia is in southern, central Australia. Comprising a land area of almost 1 million square kilometres and a resident population of 1.64 million60, 71% in the capital’s metropolitan area, SA has a low population density of 1.67 persons per square kilometre. The Aboriginal population comprised 2.3% of population with one half residing in the metropolitan area.60
The study’s population denominators were based on Australia’s Census years in 2006 and 201161. The relevant estimates of resident population by sex, age and Aboriginality include sex and age profiles by rurality and total population for SLAs, the smallest routinely available geographic areas for intrastate analysis.62 The mean annual total population for each SLA was 12 584 (SD=10 029) ranging from 0 to 36 407.63
The Australian Bureau of Statistics (ABS) index SLAs by socioeconomic characteristics64 and geographic remoteness. Census 2011 Index of Relative Socioeconomic Disadvantage (IRSD)57 64 65 ranks SLAs whereby 1 is least disadvantaged and 123 the most disadvantaged area. These are further aggregated to disadvantage quintiles of approximately equal population size.62 SLAs with nominal population and no relative IRSD rank would not contribute to the analysis and were omitted. The Accessibility/Remoteness Index of Australia (ARIA+) uses road distance to service centres62 to allocate a continuous measure ranging from 0 (high accessibility) to 15 (high remoteness). SLAs can be collapsed into categories of major city (ARIA+ ≤0.2), regional (ARIA+ >0.2 and ≤5.92) and remote areas (ARIA+ >5.92).
Data analysis
Crude, unadjusted rates of individuals experiencing chronic PPH with respect to Aboriginality, sex, age and area level IRSD quintiles and remoteness categories were summarised using cross-tabulations. Among these individual patients, the mean number of chronic PPH separations and the associated mean, total LOS and hospital costs was determined.
LOS and cost outcomes were then placed into a broader, population context. Indirect sex and age adjustment66 with 5-year age groupings to 75+67 controlled for confounding from sex and age variations between Aboriginal and non-Aboriginal people experiencing chronic PPH and the population more generally. Area outcomes therefore represent the ratio of observed versus expected outcome based on South Australian totals. For example, an outcome of 1.50 for total chronic PPH LOS among a population group indicates the ratio of observed versus expected LOS across that group was one and a half times, or 50% higher, than the South Australian average after adjusting for sex and age differences.
Outcomes of LOS and hospital cost ratios observed among the population of each SLA were positively skewed and subsequently normalised using square root transformations. The relationship between transformed outcomes and the potential covariates of SLA IRSD rank and remoteness were examined using least squares regressions68 with each SLA’s contribution weighted by population size. While the focus was on chronic PPH as a group, diabetes complications are known to be nationally over-represented among Aboriginal people69 as the largest single chronic PPH condition and up to 10 times the rate of the non-Aboriginal population. To examine any potential bias introduced by an association between diabetes complications, area disadvantage and remoteness, records were further stratified as either diabetes complications or all other chronic PPH with analyses repeated for each. The reported coefficients and 95% CIs represent the change in the standardised ratio for each one unit change in disadvantage rank and remoteness.
All analyses used Stata V.14.2.70
Results
Crude separations
Of 1 828 846 public hospital separations involving usual SA residents, 117 127 (6.4%) were categorised as chronic PPH. Aboriginal people experienced these at 2.2 (95% CI 2.1 to 2.4) times the rate of non-Aboriginals (n=4391 at 26.7 chronic PPH per 1000 persons per year compared with n=112 736 at 12.1 per 1000 persons per year).
Demographic and diagnostic profile (person-based analysis)
Chronic PPH involved 60 208 individuals, 1892, or 3.2%, of whom were Aboriginal. Table 1 quantifies aspects of their experience showing Aboriginal people were 1.8 (95% CI 1.6 to 2.1) times more likely to be hospitalised than non-Aboriginal people. There were several marked differences in conditions responsible for hospitalisation with diabetes complications being the primary diagnosis for more than one-third of Aboriginal patients with chronic PPH compared with around one in five non-Aboriginal patients. Chronic PPH events can involve more than one diagnosed chronic condition, and this was observed more frequently among Aboriginal patients. For instance, the 2311 diagnosed chronic conditions among 1892 Aboriginal patients hospitalised averages 1.22 per patient. The comparison for non-Aboriginal patients was 1.14 comprising 66 343 chronic condition diagnoses among 58 316 patients.
Demographic and diagnostic distribution of Aboriginal and non-Aboriginal patients experiencing a first chronic PPH in South Australian public hospitals, 2005–2006 to 2010–2011
Aboriginal patients experiencing chronic PPH were more likely to be female and of a much younger age compared with non-Aboriginal patients (median ages of 48 and 70 years, respectively). The proportion of individual Aboriginal patients from areas of most disadvantage (54.1% vs 26.7%) or regional and remote areas (64.2% vs 35.6%) was around double that of non-Aboriginal people.
The number of chronic PPH, associated LOS and estimated hospital costs averaged across individual patients are summarised in table 2. The dominant pattern is one of more frequent hospitalisation per Aboriginal person by sex, and across areas of residence and most age groupings. The average of 11.7 days LOS was 30% greater for Aboriginal patients with the differences peaking in the 55–74 age ranges. Hospital costs follow a similar pattern but with more pronounced differences by Aboriginality. For example, averaged hospital costs accumulated for Aboriginal patients were 56% higher than non-Aboriginal patients ($17 928 vs $11 515) with differences most prominent in the 55–74 age ranges. The absolute difference in excess of $11 500 represented an almost two-fold difference in relative terms.
Mean number of separations, total LOS and hospital cost associated with chronic PPH in South Australian public hospitals, 2005–2006 to 2010–2011
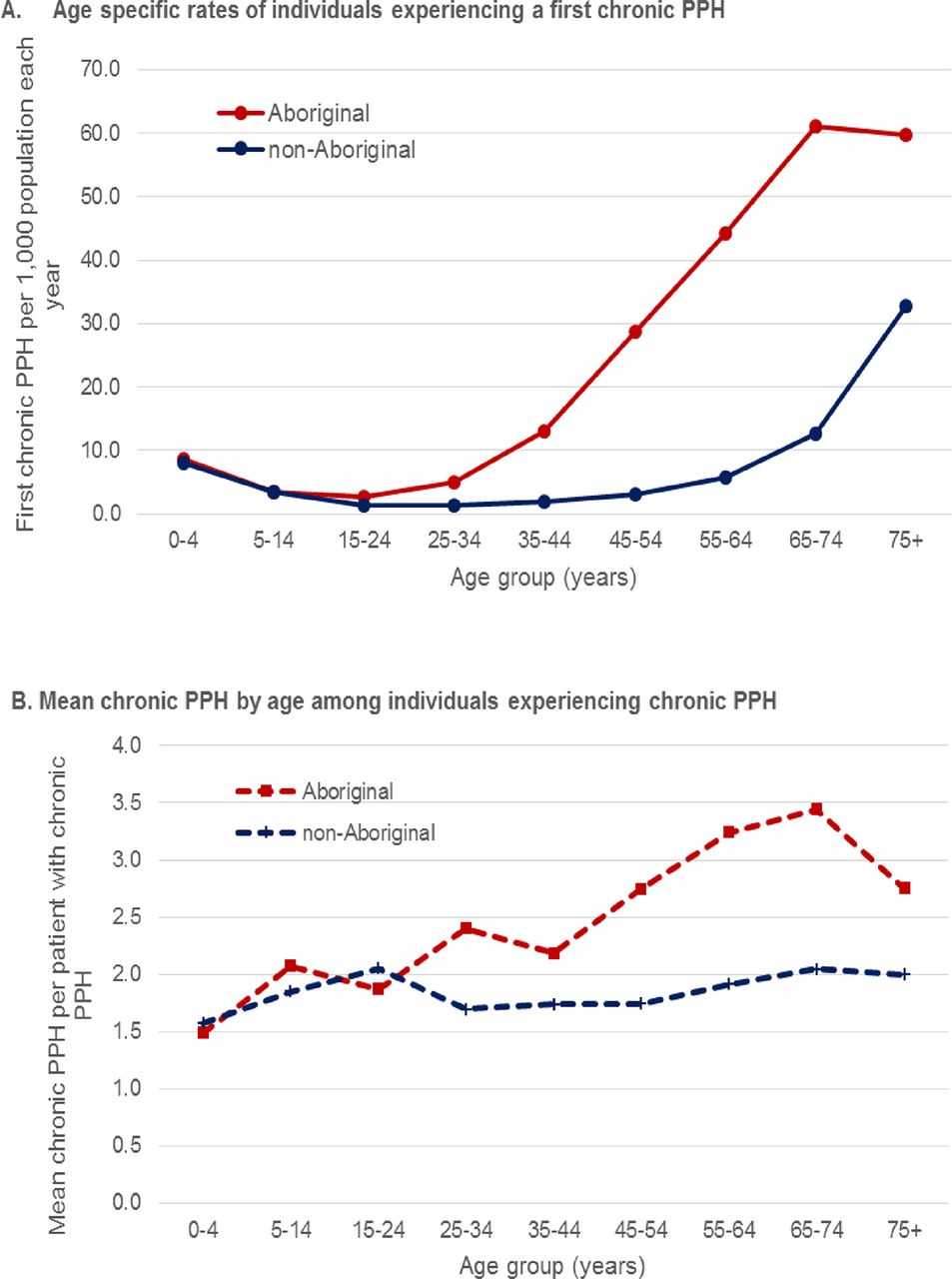
Figure 1A illustrates the stark disparity in the age at which Aboriginal and non-Aboriginal people experienced a first chronic PPH. Figure 1B then illustrates the mean number of separations those individual patients experienced. Aboriginal people aged 35–44 or more not only experienced markedly higher rates of chronic PPH but having had a first event, they were increasingly likely to experience at least one more event.

Rate of individuals with first chronic PPH and subsequent mean of chronic PPH by age and Aboriginality, South Australian public hospitals 2005–2006 to 2010–2011. PPH, potentially preventable hospitalisations.
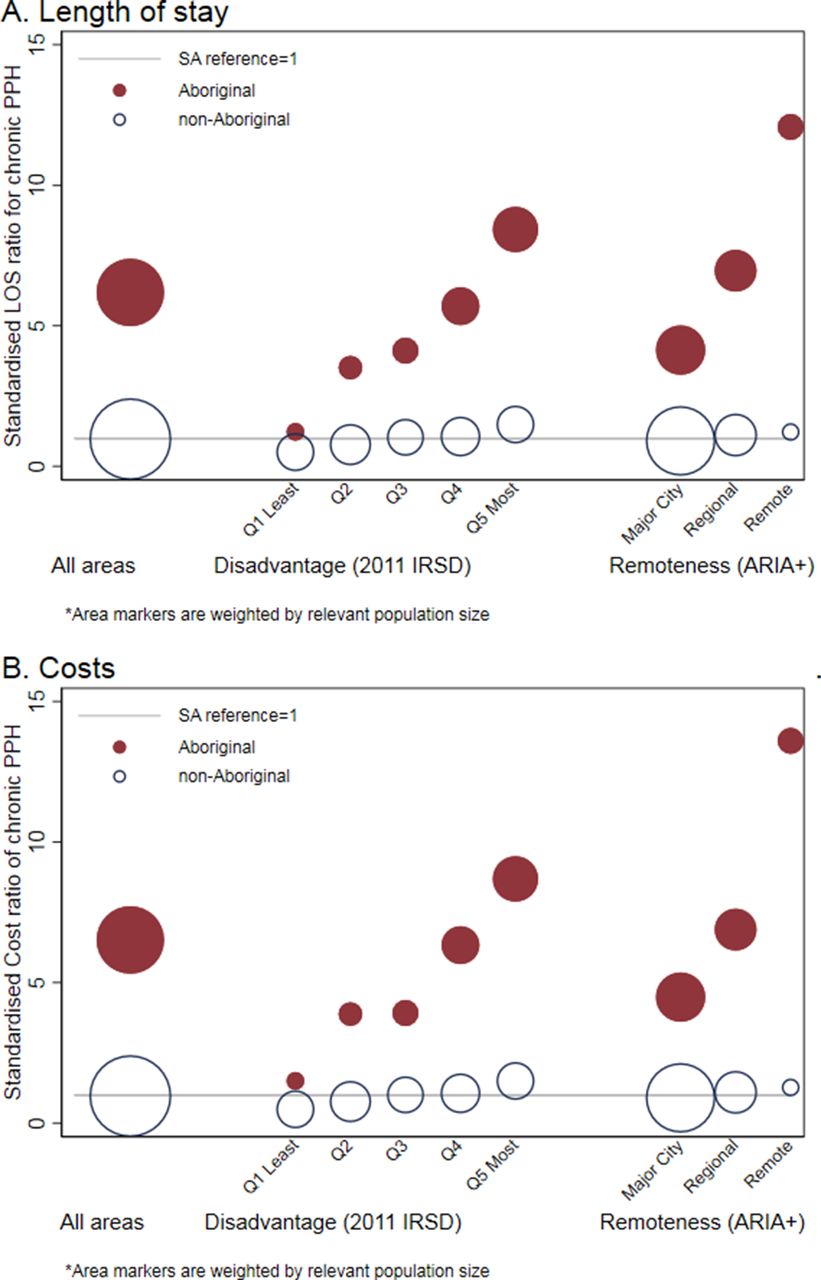
Sex and age standardised LOS and costs
Figure 2 places results for individuals hospitalised into a population context by graphing sex and age standardised outcomes by Aboriginality (LOS in figure 2A and costs in figure 2B) for all areas, then disadvantage quintiles and remoteness categories. Each marker is weighted by area population as per online supplementary table B. Figure 2A illustrates the LOS rate associated with chronic PPH within the Aboriginal population was six times more than the state average after adjusting for sex and age. Chronic PPH LOS among Aboriginal and non-Aboriginal populations progressively increased across levels of area disadvantage but change was far more pronounced within the Aboriginal population and concentrated among the relatively larger disadvantaged populations in quintiles 4 and 5. Similarly, comparison of major city with remote locations involved nearly threefold higher results from 4.2 to 12.1 times the state average. Hospital costs incurred (figure 2B) show very similar patterns with slightly higher mean differences between Aboriginal and non-Aboriginal results. Linear regression models between the two sex and age standardised outcomes of LOS and cost ratios across three levels (all chronic PPH, diabetes complications and all other chronic PPH) and the covariates of area level disadvantage and remoteness are presented for Aboriginal and non-Aboriginal populations in table 3. After allowing for sex and age differences, Aboriginal people’s LOS and cost outcomes, for each level, varied significantly across area disadvantage and remoteness. For example, within the Aboriginal population, the standardised LOS rate ratio associated with all chronic PPH was 2.09 (95% CI 0.00 to 5.83) times the state average (of one). The disparate LOS rate increased by an average of 0.03 (95% CI 0.00 to 0.07) with each change in disadvantage rank and a further 1.04 (95% CI 0.63 to 1.44) as remoteness increased. These associations of disadvantage and remoteness with LOS were consistent within stratified subgroups of diabetes complications and all other chronic PPH. However, the magnitude of change in LOS ratios was higher for diabetes complications (2.59; 95% CI 0.00 to 10.82) than for all other chronic PPH (1.86; 95% CI 0.43 to 1.21) before adjusting for the influence of area disadvantage and remoteness. The change observed in LOS for diabetes complications was around twice that for all other chronic PPH for both disadvantage (0.05; 95% CI 0.00 to 0.15 vs 0.02; 95% CI 0.00 to 0.06) and remoteness (1.62; 95% CI 0.73 to 2.51 vs 0.82; 95% CI 0.43 to 1.21). Similar variations in standardised cost ratio outcomes across levels of outcome and by disadvantage and remoteness were observed for the Aboriginal population.
{kind=link}
{kind=link}
Ratio of sex and age adjusted public hospital LOS (panel A) and costs (panel B) for chronic PPH by Aboriginality, disadvantage and remoteness in SA, 2005–2006 to 2010–2011*. ARIA+, Accessibility/Remoteness Index of Australia; IRSD, Index of Relative Socioeconomic Disadvantage; LOS, length of stay; PPH, potentially preventable hospitalisations; SA, South Australia.
Relationship of SLA attributes with standardised ratios* of LOS and cost by Aboriginality, South Australian public hospitals 2005–2006 to 2010–2011
Results for the non-Aboriginal population also show consistent associations between area disadvantage and each outcome and level whereby the standardised ratio increased as disadvantage increased. However, area remoteness was not associated with increased LOS or cost. Moreover, the base from which change occurred was substantially lower. For instance, the standardised LOS ratio for chronic PPH among the non-Aboriginal population before adjusting for disadvantage rank was less than half (95% CI 38% to 54%) of the state average.
The potential for interaction between area disadvantage and remoteness was examined without result. Sensitivity analyses using a more stringent definition of Aboriginality were also conducted but did not change our overall conclusions.71
Discussion
This study provides evidence of stark disparities in the rates with which Aboriginal and non-Aboriginal individuals experienced PPH for chronic conditions. Aboriginal people had almost twice the risk of experiencing a chronic PPH overall compared with their non-Aboriginal contemporaries. Other disparities noted include higher chronic PPH rates among Aboriginal females and younger adults with rates steeply increasing from least to most disadvantaged quintiles and/or remote areas of South Australia. Conversely, non-Aboriginal patients were more likely to be concentrated among older adults. A social gradient across disadvantage levels was also apparent; however, the steepness of the gradient from most to least disadvantaged areas was markedly lower for non-Aboriginal people. These findings are consistent with the wider literature focused on ethnic differences in PPH35–37 and underpin the disproportionate population rates of chronic PPH among Aboriginal South Australians.9 57 69
This analysis at the individual level furthers our understanding by demonstrating how, having experienced one chronic PPH event, Aboriginal patients were also more likely to endure further chronic PPH. This was associated with an increased accrual of time spent in hospital that was almost one-third higher for Aboriginal patients. Moreover, the associated hospital costs were more than 50% higher than for non-Aboriginal patients on average and more variable within the group of Aboriginal patients.
Sex and age adjusted rates of time spent in hospital for chronic PPH and expressed as rates per capita reflect the number of individuals and the length of time hospitalised. These standardised population outcomes showed LOS for chronic PPH among Aboriginal South Australians was six times higher than the state average. The best outcomes within the Aboriginal community were observed among the relatively few living in areas of least disadvantage, although these were still markedly higher than the state average. Diabetes complications are heavily implicated in chronic PPH for Aboriginal people. Their presence, with or without other chronic conditions, exacerbate LOS rates and hospital costs among Aboriginal people but not so within the non-Aboriginal population. Even after partitioning out diabetes-related hospitalisations, substantial differences in LOS and cost remain among other chronic PPH experienced by Aboriginal people.
The results further highlight systematic inequities between populations while also highlighting substantial within-population variation whereby a relatively small number of people experienced considerable time in hospital and away from their usual societal roles because of chronic health conditions. This is consistent with recent US literature demonstrating the role of chronic PPH, and particularly diabetes, as sustaining and even increasing disparities between African Americans and whites.56 Similarly, it affirms other Australian research highlighting widespread Aboriginal/non-Aboriginal differences and differences within the Aboriginal population in chronic PPH generally and the pervasive, adverse results of diabetes complications across geographic areas.48 Moreover, the results identified that increased chronic PPH were accompanied by systematically increased accrual of LOS and greater hospital costs.
The extent to which these differences are amenable to change needs further discussion. By definition, chronic PPH represent opportunities for change through exposure to primary healthcare, notwithstanding a range of individual, societal, clinical and system level factors are related to their occurrence72 73 and may each be associated with realising this potential. This is supported by studies of risk factor exposure across levels of socioeconomic disadvantage and remoteness.33 Whether the chronic PPH events were preventable in their immediate context is less certain. The high prevalence of diabetes complications and higher levels of chronic multimorbidities among Aboriginal patients observed in this study suggests comparatively more advanced disease for which hospitalisations, more often, for longer periods and at greater cost is an appropriate and expected result. A heightened need for preventive and early intervention through primary and community care is evident.
Authoritative reviews of the international literature found chronic PPH,74 75 and unplanned hospitalisation more generally76 among selected patient groups, were reduced by interventions promoting self-management support, continuity of care with a general practitioner and integration of primary and secondary care. Other interventions, such as case management, appear to reduce LOS.74–76 However, each review was restricted by a relative lack of robust evaluation of interventions as they are introduced into health systems. Such evaluations are emerging and indicate promising primary healthcare interventions in chronic disease management and diabetes are available. Australia’s largest randomised intervention in diabetes delivered positive outcomes in HbA1c levels, blood pressure, waist circumference, depression, care-plan take-up and chronic PPH in the trial group receiving each of five available quality improvement and flexible funding components.43 Mainstream general practice services are less available for remote Aboriginal populations exhibiting greater need in terms of chronic PPH LOS and costs, yet evidence of effective intervention among Aboriginal populations is available.77 Randomised diabetes care led by community health workers in regional and remote areas showed promising HbA1c reductions among poorly controlled type 2 diabetes patients78 and modest net reductions in diabetes-related hospitalisation in the treatment group.79 Nevertheless, a critical need for substantively increasing the training and supply of Aboriginal healthcare workers remains.80 Generally negative evaluation of incremental cost-effectiveness assessments based on short-term, averaged and disease-specific results43 79 may impede this investment.
Our description of who is more likely to experience chronic PPH, for what conditions, with what frequency and at what direct cost to the health system suggest three areas for developing incremental cost to outcome analyses. The first is to consider flow-on benefits from disease-specific interventions to other comorbid chronic conditions, especially where disparities in condition prevalence exist. Second, evaluation based on longer term accumulated hospitalisation costs for individual trial participants is warranted. Where project term constraints apply, our results provide an initial empirical base. Finally, placing individual participant results into a population context provides an information base for allocating resources that address healthcare needs for primary and community care at lower cost to individuals and acute care services.24
Subsequent reporting of cumulative LOS and costs at a person level adds value to system performance monitoring by making the person and patient the centre of reporting and evaluation, as well as the centre of care. Providing empirical evidence of change occurring at individual and population levels will help align system activities and monitoring with the ultimate aim of providing appropriate and effective care of patients and people, equitably and efficiently.
Limitations
The study has several limitations. First, cumulative LOS as an outcome variable is influenced by the nature of admission with interhospital transfers having longer LOS than emergency admissions.6 Recurrent hospital events for chronic conditions among people in regional and remote settings may involve comparatively more interhospital transfers or planned admissions for treatment where primary health interventions are scarce. Nevertheless, the observations summarised in this study represent an aspect of peoples’ lived experience of contending with chronic disease. Continuing research will benefit from focusing on mode of admission to hospital and the local availability of primary care. Second, the propensity to identify as Aboriginal has increased across recent times, and any undercounting in earlier Aboriginal population denominators would affect population rates. However, this study’s population estimates are drawn from the internally consistent ABS series covering 1996–2011 as based on the 2011 Census and the first available set of ABS non-experimental population denominators. Accordingly, there are no known inflation of rates due to population undercounts. Nevertheless, estimates incorporating Census 2016 will provide a valuable reliability check when used with concurrent hospital data in future analyses. Third, while public hospital care is universally available in SA and estimating rates makes appropriate use of population denominators, the omission of private hospital separations undercounts some chronic PPH, particularly among relatively advantaged citizens. Further studies will benefit from including these private hospital separations and from exploring whether chronic PPH were associated with planned care or the result of emergency presentations. Finally, the omission of the APY Lands SLA means chronic PPH outcomes associated with a very remote area and SA’s most disadvantaged are not represented.81 Subsequent research in the area will benefit from including APY Land residents hospitalised in the Northern Territory50 to ensure results for the most remote and disadvantaged population groups are not underestimated.
Conclusion
The results show heightened risk of chronic PPH among Aboriginal individuals that compounds into more rehospitalisation and accumulated time in hospital at greater cost to the person, their community and the health system. At a population level, the systematic change in chronic PPH and LOS by Aboriginality and area suggests efforts to address these potentially avoidable hospitalisations will benefit from targeting specific population segments, particularly in areas of greater socioeconomic disadvantage and geographic remoteness. This analysis helps guide such actions by identifying subpopulations within the wider community who could most benefit from improved understanding of antecedent causes of hospitalisation. Routine reporting across population groups and regions will help monitor progress in meeting the underlying population health needs with earlier, and perhaps lower cost, interventions.
Acknowledgments
DB is supported in part by an Australian Government Research Training Program Scholarship. AB is supported by The Sylvia and Charles Viertel Senior Medical Research Fellowship. The authors would like to thank: SAHMRI and the Wardliparingga Aboriginal Health Research Unit for providing a Summer Scholarship for TC and SA Health for administrative unit records via Statistical Linkage Project 2010-0004. John Glover, Torrens University’s Public Health Information Development Unit (PHIDU) and the Australian Department of Health for Aboriginal and Torres Strait Islander small area population estimates for 2006.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
Footnotes
Contributors DB conceived the project, performed the analyses and drafted the manuscript; TC contributed to literature searching and manuscript preparation; JK, AB and JL made important contributions to operationalising this study, interpreting the statistical analysis and revised the manuscript. All authors read and approved the final version of the manuscript.
Competing interests None declared.
Ethics approval SA Health; Aboriginal Health Council of South Australia.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The study’s data comprised of deidentified unit record administrative records. These were used under privileged arrangements set out in a study-specific confidentiality deed. The data cannot be accessed by another party without relevant departmental and human research ethics approvals.