Article Text

Abstract
Objective To systematically search for research about the effectiveness of mandatory reporting of child maltreatment and to synthesise qualitative research that explores mandated reporters’ (MRs) experiences with reporting.
Design As no studies assessing the effectiveness of mandatory reporting were retrieved from our systematic search, we conducted a meta-synthesis of retrieved qualitative research. Searches in Medline (Ovid), Embase, PsycINFO, Cumulative Index to Nursing and Allied Health Literature, Sociological Abstracts, Education Resources Information Center, Criminal Justice Abstracts and Cochrane Library yielded over 6000 citations, which were deduplicated and then screened by two independent reviewers. English-language, primary qualitative studies that investigated MRs’ experiences with reporting of child maltreatment were included. Critical appraisal involved a modified checklist from the Critical Appraisal Skills Programme and qualitative meta-synthesis was used to combine results from the primary studies.
Setting All healthcare and social-service settings implicated by mandatory reporting laws were included. Included studies crossed nine high-income countries (USA, Australia, Sweden, Taiwan, Canada, Norway, Finland, Israel and Cyprus) and three middle-income countries (South Africa, Brazil and El Salvador). Participants: The studies represent the views of 1088 MRs.
Outcomes Factors that influence MRs’ decision to report and MRs’ views towards and experiences with mandatory reporting of child maltreatment.
Results Forty-four articles reporting 42 studies were included. Findings indicate that MRs struggle to identify and respond to less overt forms of child maltreatment. While some articles (14%) described positive experiences MRs had with the reporting process, negative experiences were reported in 73% of articles and included accounts of harm to therapeutic relationships and child death following removal from their family of origin.
Conclusions The findings of this meta-synthesis suggest that there are many potentially harmful experiences associated with mandatory reporting and that research on the effectiveness of this process is urgently needed.
- child protection
- medical law
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the most comprehensive review to date of mandatory reporting of child maltreatment, focusing on mandated reporters’ (MRs) experiences with reporting.
Although a systematic search was conducted, little information about mandatory reporting from low- and middle-income countries was retrieved.
Critical appraisal of included articles followed an established checklist and reporting of synthesis findings was done according to the Enhancing Transparency in Reporting the Synthesis of Qualitative research statement.
This meta-synthesis used an established method for synthesising study findings that enabled the creation of recommendations for MRs relating to the reporting process
Introduction
Global estimates of child maltreatment indicate that nearly a quarter of adults (22.6%) have suffered childhood physical abuse; over a third of adults (36.3%) have suffered childhood emotional abuse; 16.3% of adults have suffered childhood neglect and 18% of women and 7.6% of men, respectively, have suffered childhood sexual abuse.1–3 These estimates vary across countries. For example, according to 2015 US child protective services (CPS) reports, 63.4% of reported children experienced neglect.4 Given the high prevalence of child maltreatment and its potentially serious, long-term health and social consequences,5–8 many countries have taken steps to prevent child maltreatment and reduce its associated impairment, including through the introduction of mandatory reporting.
Mandatory reporting law, in the context of child maltreatment, “is a specific kind of legislative enactment which imposes a duty on a specified group or groups of persons outside the family to report suspected cases of designated types of child maltreatment to child welfare agencies”.9 The USA enacted the first mandatory reporting laws in 1963.10 11 These laws were more narrowly conceived, requiring certain mandated professions to report ‘severe’ or ‘significant’ physical abuse by parents or caregivers. Over time, legislation has expanded in the USA and has been replicated in other countries. Across jurisdictions, mandatory reporting can include other forms of maltreatment (notably physical, sexual and emotional abuse, neglect, children’s exposure to intimate partner violence (IPV) and prenatal exposure to drug abuse), reporting by more than mandated professionals (eg, by all citizens), reporting abuse perpetrated by non-caregivers and reporting beyond ‘severe’ or ‘significant’ abuse.12
Some information about the international context of mandatory reporting is available, but in general little information about this process is available from low- and middle-income countries (LMICs) (see online supplementary file 1). Furthermore, while we began this project with the intent of doing a systematic review of studies of effectiveness about mandatory reporting, we were unable to find any studies that could be used for this purpose (ie, no prospective controlled trials, cohort studies or case–control studies assessing the effectiveness of mandatory reporting in relation to child outcomes were retrieved from our systematic search). Instead, we found that while there are a handful of prospective studies assessing particular outcomes of mandatory reporting,13 14 most of the research discussing its impact relies on retrospective analysis of CPS reports15–18 or is related to mandated reporters’ (MRs), children’s and caregivers’ perceptions about reporting, as discussed in surveys,19–27 qualitative literature28–30 or case reports31–33 (qualitative literature is summarised in this meta-synthesis). Given the paucity of data on effectiveness of mandatory reporting, the purpose of this meta-synthesis is to summarise qualitative research about MRs’ experiences with reporting. A companion paper titled, A meta-synthesis of children’s and caregivers’ perceptions of mandatory reporting of child maltreatment (in preparation), will address caregivers’ and children’s experiences with mandatory reporting.
Supplementary file 1
Methods
Various methods for synthesising qualitative literature exist depending on the purpose of the review34 or the philosophical35 or epistemological36 stance of the researcher. As there is no standard way to summarise qualitative literature, for this meta-synthesis we follow the methods of Feder and colleagues,37 whose work builds on Noblit and Hare’s (43) approach to meta-ethnography. Meta-ethnography does not offer suggestions for sampling or appraising articles and at times can be criticised for lack of transparency.34 A benefit of Feder and colleagues’37 method is that they conducted a systematic search of qualitative studies with clear inclusion and exclusion criteria, thus enhancing the transparency of their study selection process. While the benefit of appraising qualitative research is still debated,38 Feder and colleagues’ approach to appraising qualitative literature prioritises studies that are ranked as of higher quality, which supports increasing recommendations to consider study quality, but also does not inappropriately exclude so-called lower quality studies that make ‘surface mistakes’ that would not otherwise invalidate their study findings.34 Finally, like Noblit and Hare’s (43) work, Feder et al’s37 approach to synthesising qualitative literature allows for the inductive creation of a set of higher order constructs (third-order constructs, discussed below) that reflect concepts identified in individual studies but also extends beyond them. While the quantification of qualitative work has been criticised, in this study, individual concepts are ‘counted’ to let the reader decide about the relative importance of the themes. We suggest that themes that appear at a lower frequency are not necessarily less important (eg, one account of harm to a child is significant and must be considered) but rather that this theme was less of a focus for MRs and study authors. For example, the theme of ‘cultural competence’ is not discussed by as many MRs as compared with all of the various factors that impact their decision to report, which is partially explained by the fact that 11 (25%) of included articles set out specifically to investigate factors that impact MRs’ decision to report. The results of this meta-synthesis are reported according to the PRISMA checklist and Enhancing Transparency in Reporting the Synthesis of Qualitative (ENTREQ) research statement35 (see online supplementary file 2).
Supplementary file 2
Search strategy
The systematic search was conducted by an information professional (JRM). Index terms and keywords related to mandatory reporting (eg, ‘mandatory reporting’, ‘mandated reporters’, ‘duty to report’, ‘failure to report’) and child abuse (broadly defined, including, but not limited to terms for child welfare, physical abuse, emotional abuse, neglect, sexual abuse/exploitation and children’s exposure to IPV) were used in the following databases from database inception to 3 November 2015: Medline (1947-), Embase (1947-), PsycINFO (1806-), Cumulative Index to Nursing and Allied Health Literature (1981-), Criminal Justice Abstracts (1968-), Education Resources Information Center (1966-), Sociological Abstracts (1952-) and Cochrane Libraries (see online supplementary file 3 for example search strategy). Forward and backward citation chaining was conducted to complement the search. All articles identified by our database searches were screened by two independent reviewers (JRM and AA) at the title and abstract level. At the level of title and abstract screening, an article suggested for inclusion by one screener was sufficient to put it forward to full-text review. Full-text articles were screened for relevance and put forward for consideration by one author (JRM); relevance for inclusion was confirmed by a second author (MK), with discrepancies being resolved by consensus.
Supplementary file 3
Study selection criteria
Our inclusion criteria were as follows: (1) primary studies that used a qualitative design; (2) published articles; (3) investigations of MRs’ experiences with mandatory reporting of child maltreatment, including physical abuse, sexual abuse, emotional abuse, neglect, exposure to IPV, prenatal exposure to maternal drug abuse or child sex trafficking; (4) presence of direct quotes from the participants to facilitate the formulation of the results and (5) English-language articles only. Excluded studies include (1) all non-qualitative designs, including surveys with open-response options; (2) studies that did not examine mandatory reporting in the context of child maltreatment (eg, mandatory reporting for elder abuse or IPV only) and (3) qualitative methods that did not lend themselves to direct quotes from participants (eg, forensic interviews).
Data analysis
Data analysis followed two parallel strands: (1) first and second-order constructs (table 1) were identified in each article and (2) each article was appraised with a modified critical appraisal tool for qualitative literature from the Critical Appraisal Skills Programme (CASP). For data extraction, each article was analysed for the perspectives of MRs (first-order constructs) and the conclusions offered by the author(s) of the article (second-order constructs). For first-order constructs, only direct quotes from participants (and any clarifying text provided by the study author) found in the Results sections of included articles were considered for analysis. For second-order constructs, only study author recommendations (often worded as ‘should’ or ‘ought’ statements and found in the Discussion of the article) were considered for analysis.
First, second and third-order constructs
Two reviewers (JRM and MK) independently placed the primary data from each study and its corresponding code into an Excel file, and these files were compared for consistency (JRM). After reviewing discrepancies across Excel files, one author (JRM) developed a master list of codes, and after discussion with a second author (MK) (where both authors reviewed all codes and corresponding data together), this list of codes was further modified. Any discrepancies identified by the two authors were resolved by a third researcher (HLM). After this point, one author (JRM) went back through and recoded all data in the excel file according to the master list of codes and a second author reviewed all recoding (MK). Readers are able to view this final Excel file, which includes all extracted data, codes (including master list of codes) and overall quality rating of included articles. Final conclusions (third-order constructs (table 1)) were all double checked (JRM) to ensure that they were supported by articles that ranked highly on the quality appraisal forms.
For critical appraisal, a modified appraisal tool from CASP was used to assess the quality of each article (see online supplementary file 4). Two independent authors (JRM and MK) appraised each article to assess if it addressed each CASP question (yes/no/unsure) and came to consensus about the final score for each article. Only the total CASP scores were considered, and studies were not excluded for poor study design, as (1) according to our inclusion criteria, we only included articles with full quotes from MRs, (2) we coded all MRs’ quotes as first-order constructs and (3) we felt that the exclusion of any articles could exclude a valuable quote/perspective from an MR and that this exclusion could impact the meta-synthesis findings.
Supplementary file 4
Data coding for this meta-synthesis was primarily inductive. Data analysis focused on identifying (1) first-order and second-order constructs that appeared across studies (repeating themes); (2) first-order or second-order constructs that were conflicting across studies or within studies and (3) unfounded second-order constructs or researchers’ conclusions or interpretations that were not supported by quotes from participants. First and second-order constructs that appeared across studies were re-examined to develop the third-order constructs or the conclusions of this meta-synthesis. Specifically, one author (JRM) identified third-order constructs that addressed strategies to improve MRs’ experiences with the reporting process—especially when these themes were supported by strategies offered by MRs in first-order constructs—and these themes were, per Feder et al,37 reworded as recommendations. For example, the recommendation that MRs should ‘Be aware of jurisdiction-specific legislation on reportable child maltreatment’ combines a second-order construct that suggests MRs need better training about jurisdiction-specific mandatory reporting legislation with the first-order construct in which MRs admitted that they lacked knowledge about mandatory reporting legislation. These third-order constructs were first discussed with the two authors (MK, HLM) involved in developing the first and second-order constructs to ensure they reflected their understanding of the data. Following this, a table that showed a ‘tally’ of which first and second-order constructs were combined to generate each third-order construct (and a brief rationale for combining them) was reviewed by all study authors and a discussion followed. Minor adjustments to the third-order constructs were made after this discussion. The biggest discrepancy across all authors of this meta-synthesis was whether or not we should offer recommendations specific to mandatory reporting at all, given that (1) we did not find any effectiveness data and (2) the qualitative studies suggest many negative experiences with reporting. However, the third-order constructs represent what is found in the included studies that we synthesised (ie, included studies did not recommend against mandatory reporting), and their presentation as recommendations is faithful to the approach used by Feder et al, which we set out to follow, and the experiences of MRs, as summarised in the included articles.
Results
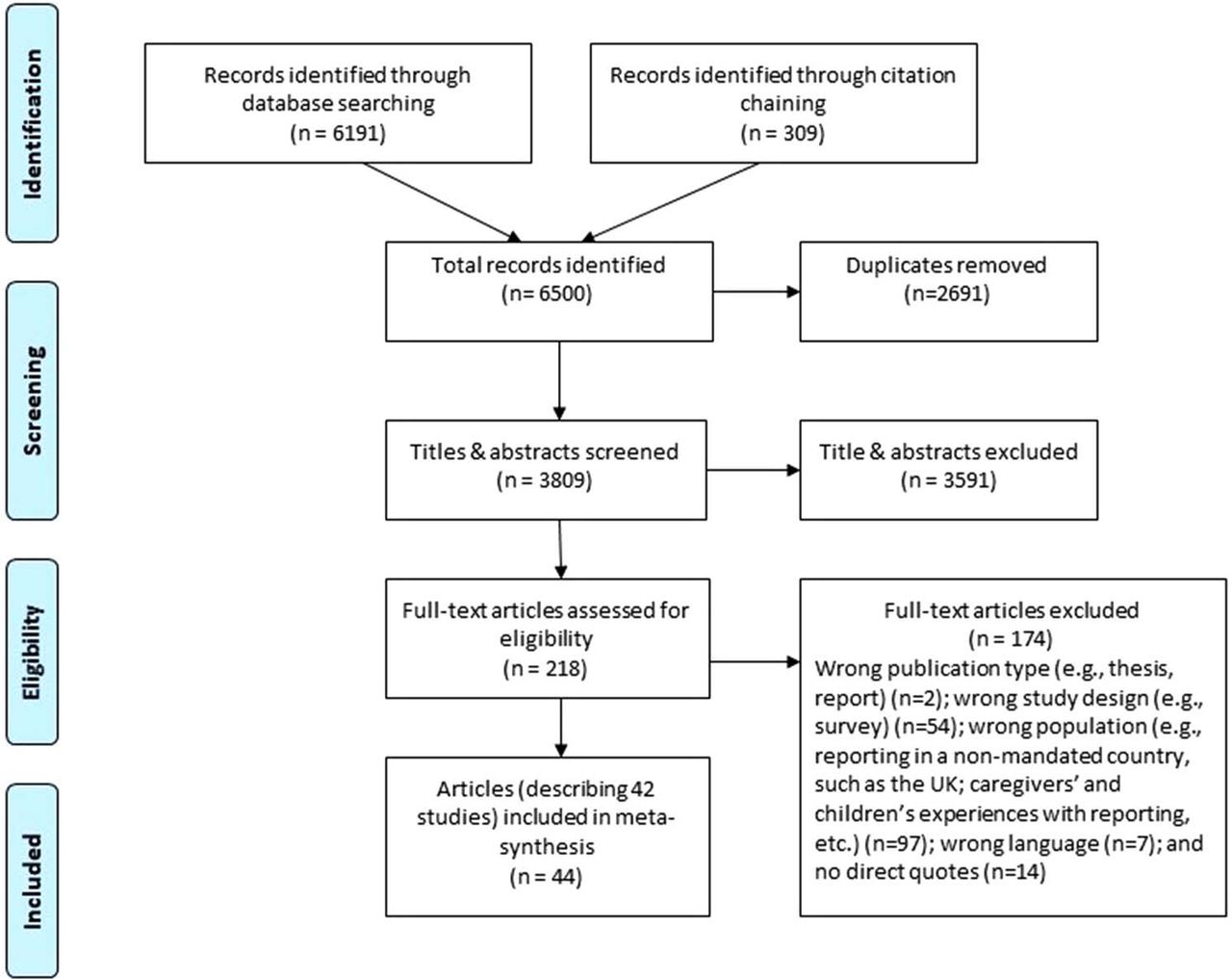
A total of 6500 records were identified and, after deduplication, 3809 titles and abstracts were screened using the screening criteria. After full-text screening of 218 articles, 44 articles (representing 42 studies) were included in this review (see figure 1). Details about participant and study characteristics are available in online supplementary file 5.
Supplementary file 5

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Study characteristics and methodological quality
The methodological quality of the studies varied and the total score percentages for each article (total possible score was 20 ‘yeses’) are reported in table 2. These studies represent the views of 1088 MRs, including 231 physicians, 224 nurses, 168 CPS professionals, 156 teachers, 114 psychologists and therapists, 85 social workers, 19 dentists, 16 domestic violence workers, 16 police officers. This underestimates the number of participants included because it was challenging to determine exact number of participants in some of the studies (including one study with 10 focus groups). MRs’ ages were reported in 25% of studies and ranged from 20 to 60 years of age; their years of experience were reported in just over 50% of the studies and ranged from 6 months to 41 years of experience. Only six articles39–44 discussed any training that MRs received about recognising and responding to child maltreatment; aside from one study42 that was examining the impact of child maltreatment training, it is hard to determine if or how training (or lack of training) influenced MRs’ responses. Over 80% of the articles had been published since the year 2000, with seven articles published between 1981 and 1999. The studies took place in nine high-income countries (USA (15), Australia (6), Sweden (5), Taiwan (5), Canada (2), Israel (2), Norway (1), Finland (1) and Cyprus (1)) and three middle-income countries (South Africa (3), Brazil (2) and El Salvador (1)). Other studies from LMICs were identified45–49 that did not meet all of the inclusion criteria; this limitation of our study is discussed further below.
Methodological quality of studies
MRs’ decisions to report and experiences with reporting (first-order constructs)
Seven first-order constructs (views of MRs) are detailed below; all except construct seven (experiences receiving a report) are supported by articles from the top quartile (see table 2 above). As is shown in table 3, most of the articles (91%) addressed factors that influenced MRs’ decision to report (construct 1). These findings suggest that MRs struggle to identify less overt forms of maltreatment, including ‘mild’ physical abuse, emotional abuse, children’s exposure to IPV and abuse experienced by children with disabilities. MRs also were reluctant to report their suspicions of abuse and preferred to report only when they found physical evidence of abuse, such as physical injuries, bruises, broken bones, caries (and corresponding lack of treatment) or ‘total’ changes in behaviour. Unfortunately, most MRs did not clarify their reporting decisions in relation to specific forms of maltreatment. For example, only five articles28 50–53 discussed decisions to report (including hesitance to report) in relation to sexual abuse, and four of these articles discussed maltreatment of children with disabilities (suggesting particular challenges they faced in reporting maltreatment of children with disabilities).
First-order constructs (views of MRs) and the number (n) and per cent (%) of articles that address each construct
Factors that influenced the decision to report were distinct from the reporters’ judgements and views about mandated reporting (construct 2) and their experiences with reporting (construct 3), as expressed through specific accounts of positive or negative experiences. While six articles (14%) reported positive experiences with the reporting process, 32 articles (73%) mentioned negative experiences with the reporting process, including 13 articles (30%) that offered concerning examples regarding negative child outcomes, such as: when the child was not removed from harm and the abuse continued or intensified; when the child was removed from harm, but the foster care environment was worse than the family-of-origin environment and child death following a report or after being removed from the family of origin.
First-order constructs also addressed MRs’ values and knowledge related to child maltreatment and reporting (construct 4), MRs’ strategies for responding to disclosures of child maltreatment or for reporting (construct 5) and whether or not MRs felt personally responsible for reporting or passed this responsibility to others, such as a supervisor (construct 6). A handful of articles included CPS professionals' experiences with receiving a report (construct 7).
Strategies for supporting MRs (second-order constructs)
All second-order constructs (views of study authors) listed in table 4 below were supported by first-order constructs within the same study; all were also supported by articles from the top quartile of study quality score (see table 2 above). These constructs represent study authors’ suggestions for how MRs could improve their decision-making during the reporting process, including strategies for mitigating negative experiences. The majority of articles (86%) commented on the need for MRs to be trained in how to best identify, respond and report suspected child maltreatment (construct 1). Two other influential themes related to the need for increased consultation between MRs and between MRs and CPS (construct 2) and the need for increased communication among MRs, among MRs, children and families and between MRs and CPS (construct 3). Study authors also emphasised that MRs need to be better supported in their reporting process (construct 4) and that they need clear protocols related to identifying and reporting child maltreatment (construct 5). Some study authors emphasised that child rights and well-being must be prioritised throughout the reporting process (construct 6). A few study authors suggested that MRs’ and CPS’ responses to child maltreatment need to be culturally competent (construct 7) and emphasised that MRs must report suspicions of abuse when this is their legal obligation (construct 8).
Second-order constructs (views of study authors) and the number (n) and per cent (%) of articles that address each construct
These second-order constructs show that MRs need better support at all social–ecological levels: (1) personally, in terms of better training, including skills to identify and respond to child maltreatment, as well as skills for stress and coping management; (2) interpersonally, in terms of better opportunities for dialogue among colleagues about child maltreatment generally, as well as specific cases; (3) organisationally, in terms of more support for the time it takes to report (and the potential ‘costs’ to other patients when taking this time), safeguards for MRs’ personal safety when reporting and access to staff experts in child maltreatment; (4) in the community, especially in terms of better feedback about reported cases from CPS and in general better dialogue between different agencies involved in the reporting process and (5) nationally, in terms of national protocols about identifying, responding to and reporting child maltreatment.
Apparent contradictions
All of the apparent contradictions found within the studies (or constructs that conflicted within or across studies) are examples of correlates of reporting that have been discussed previously in the literature (eg, MRs’ decisions to report should or should not be influenced by the context of the family, the level of evidence available, the context of the reporter or the perceived impact of reporting on the child or family; MRs should or should not report children’s exposure to IPV or corporal punishment; MRs should or should not intervene with the family instead of reporting; the MR who identifies maltreatment should report it or refer it to a senior personnel). The solutions to these contradictions are more straightforward to resolve legally but less so ethically. For example, in cases where MRs suspect that harm may come to a child from the reporting process (based on their experience or their expert judgement), they are still required to report legally (when the type and severity of child maltreatment falls within their jurisdiction’s legislation).
Recommendations for MRs (third-order constructs)
The first-order constructs draw attention to several negative experiences MRs had with the reporting process, as well as a number of factors that influenced their decision to report. The second-order constructs summarise some institutional and cross-disciplinary responses to these concerns (offered by study authors), such as the need for increased feedback from CPS about reported cases, the need for clear protocols for identifying child maltreatment and reporting it and the need for MRs to be better supported in their reporting process. Most of the second-order constructs, however, discuss how MRs’ negative experiences with the reporting process can be addressed through increased training and better communication or consultation among MRs, their colleagues and CPS. The third-order constructs found in table 5 represent study authors’ interpretation, across the studies, of MRs’ and study authors’ strategies for mitigating negative experiences with the reporting process, which includes the level of knowledge about child maltreatment that is required by all MRs. Restriction of the analysis to studies in the top quartile of quality ratings did not change these third-order constructs.
Third-order constructs in terms of recommendations to MRs
Discussion
While our search retrieved no evidence about the effectiveness of mandatory reporting, and qualitative research cannot be mistaken for evaluation of effectiveness, findings from this review raise important questions about the effects of mandatory reporting by drawing on studies reporting the experiences of MRs across nine high-income and three middle-income countries. While some MRs have had positive experiences with reporting, the negative experiences reported in the individual studies are very concerning, especially those related to child outcomes. Some of these include accounts of children being revictimised by the reporting process, children whose abuse intensified after a report was filed, foster care environments that were perceived to be worse than family-of-origin environments and reports of child death after CPS intervention. Whether or not these negative experiences are reflective of national or international experiences must be assessed. Studies addressing MRs’ attitudes towards reporting address perceptions of negative experiences but are not able to address child-specific outcomes.54–56 For example, Flaherty and colleagues’54 US national survey of paediatricians found that 56% of physicians experienced negative consequences from reporting, including 40% who lost patients after reporting and 2% who were sued for malpractice. Some of these concerns are likely to be especially salient for MRs in countries where child protection systems are not well developed or do not function properly. MRs may have real concerns that reporting cases of child maltreatment to poorly trained or poorly resourced service providers could lead to adverse outcomes for children (see, for example, the concerns raised by Devries and colleagues46 about the very poor response of local services to children in Uganda). Particularly in these contexts, further research on the harms and benefits of mandatory reporting is needed.
Given that negative experiences with reporting discussed in this meta-synthesis spanned decades and nine high-income and three middle-income countries, it is not surprising that some authors have suggested that the interface between MRs and CPS agencies ‘requires renewed attention, in terms of both research and programming’.57 We were unable to find any high-quality research studies suggesting that mandatory reporting and associated responses do more good than harm. The lack of evidence about the effectiveness of mandatory reporting has been noted by others, including the WHO.58 More research addressing child-specific outcomes is needed on 1) alternative approaches to mandatory reporting as well as 2) alternative responses to investigation following mandatory reporting (such as differential response; see online supplementary file 1).
Researchers citing the benefits of mandatory reporting note that mandatory reporting laws are an “essential means of asserting that a society is willing to be informed of child abuse and to take steps to respond to it”11 ; they also note that mandatory reporting laws have resulted in the identification of more cases of child maltreatment59–61 and an increase in reporting from reluctant reporter groups.62 63 It has been argued by some authors64 65 that identification is not a sufficient justification given the problems with the mandatory reporting process; as described in this meta-synthesis, negative experiences seem to involve the reporting process itself and the associated responses (or lack of response). A key issue is the number of children identified by MRs who receive either no services or of greater concern—inappropriate, ineffective or harmful responses. MRs’ discussions of ineffective responses seem to be related most closely to their reports of ‘mild’ physical violence, neglect, emotional abuse or children’s exposure to IPV, which may lend credence to the suggestion that mandatory reporting is most appropriate for cases of severe abuse and neglect.11 More research about the effectiveness of mandatory reporting across abuse types and severity, as well as associated responses and strategies for mitigating harm (including strategies for including children and family in the reporting process), is urgently needed.
Implications for clinicians and policy-makers
Much of the research included in this meta-synthesis did not question the need for mandatory reporting (as many of the studies aimed to address MRs’ decision-making process with regards to reporting); instead, it included studies that addressed MRs’ negative experiences and reluctance to report with suggestions about the need for increased support, training, consultation and communication. The third-order constructs (final conclusions) of this study therefore offer recommendations for how MRs can mitigate negative experiences with the reporting process.
Analysis of recommendations by study authors suggests that MRs need better support for the reporting process at many levels: personally, interpersonally, institutionally, in the community and nationally. Personal support for reporters can include training or support for secondary traumatic stress—which many healthcare professionals experience—through, for example, strategies for debriefing.66–68 Emerging work is examining the methods by which health and social service providers can be trained to recognise and respond to child maltreatment disclosures and suspicions of child maltreatment (for example, see 69–71). Given that the evaluation of these training programmes falls outside the scope of this review, and that mandatory reporting is but one of many components of appropriate recognition of and response to children exposed to maltreatment, further work and evaluation is needed to understand the extent to which existing training programmes are capable of improving MRs’ recognition and response to children exposed to maltreatment or if further specialised training is needed. Among studies of training programmes for mandatory reporting with controlled designs, Kenny72 argues that Alvarez and colleagues’73 training programme shows the most promise. The components of the training programme, discussed further by Donohue et al,69 include discussions about identifying child maltreatment, reporting requirements and procedures, strategies for involving caregivers in the reporting process and information about consultation with colleagues and CPS—all identified as important components of training in this review. Whether or not the training programmes can be successfully modified to address the training needs of different countries and multidisciplinary trainees has yet to be assessed.
Interpersonal support can include increased opportunity for communication and teamwork between interdisciplinary and multidisciplinary colleagues through, for example, interdisciplinary training42 or multidisciplinary conferences.74 Relatedly, community support can include increased communication and collaboration between reporting professionals; the need for increased feedback from CPS about reported cases is also important.54–56 75 76 Poor communication or collaboration between CPS and MRs has long been cited as an area for much needed improvement.74 77–80 How exactly to improve collaboration, however, is complex and under-researched. As Winkworth and White81 argued in relation to Australian initiatives to increase collaboration between child protection, family relationship and family support service systems, “So ubiquitous is reference to collaboration in policy documents that it is in danger of being ignored altogether by service deliverers who are not clear about its rationale, how it is built, or its real value”. Finally, national support necessitates national protocols about identifying, responding to and reporting abuse, as well as increased clarity around specific reporting requirements (including increased clarity around national or jurisdictional reporting legislation). Whether or not national protocols improve the reporting process for MRs or help to improve child outcomes would need to be tested.82–84
Strengths, limitations and future research
The strengths of our review include a systematic search to inform the meta-synthesis; the use of clear a priori study inclusion and exclusion criteria; use of an established study appraisal checklist and transparent and reproducible methods for analysis. This review focused on MRs’ direct experiences with, or views about, the mandatory reporting process and as such does not reflect complete findings about (1) appropriate MR responses to the disclosures or identification of child maltreatment; (2) CPS workers’ experiences substantiating reports; (3) children’s and caregivers’ experiences with mandatory reporting and (4) professionals’ experiences with reporting in a non-mandated context (such as the UK). Reviews on these topics would be complementary to the findings of this review. While only English-language studies were included and only a handful of included articles discussed reporting processes in LMICs, the limited availability of research from LMICs suggests an even greater need to invest in research in these settings. Research about voluntary or policy-based reporting processes, as well as responses to mandatory reporting, may provide more information about reporting process from LMICs.
Conclusion
Mandatory reporting of child maltreatment has been variously implemented across jurisdictions and high-quality research on the effectiveness of this process is severely lacking. While our search retrieved no evidence about the effectiveness of mandatory reporting, through this meta-synthesis of MRs’ experiences with reporting, we have summarised many accounts of harm associated with reporting. Along with focusing on approaches to improve mandatory reporting, the field needs to address whether or not mandatory reporting actually improves children’s health outcomes through research that is sensitive to both severe and less overt forms of maltreatment. Our findings in no way imply that the recognition and response to children exposed to maltreatment is not a significant public health concern that requires coordinated responses. Rather, it implies that we must work to ensure that all of our methods for recognising and responding to children exposed to maltreatment demonstrate that they benefit children’s safety and well-being and do no additional harm .
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
Footnotes
Contributors Conceptualisation: HLM, KD, MC, JRMT, JCDM; Analysed the data: JRMT, MK, AA, HLM; Writing–original draft preparation: JRMT; Writing–review and editing: JRMT, MK, KD, MC, JCDM, CNW, HLM; ICMJE criteria for authorship read: JRMT, MK, KD, MC, JCDM, CNW, AA, HLM; Agree with manuscript results and conclusions: JRMT, MK, KD, MC, JCDM, CNW, AA, HLM.
Funding HLM and CNW receive funding from the Canadian Institutes of Health Research (CIHR) Institute of Gender and Health (IGH) and Institute of Neurosciences, Mental Health and Addictions (INMHA) to the PreVAiL Research Network (a CIHR Center for Research Development in Gender, Mental Health and Violence across the Lifespan—www.PreVAiLResearch.ca). HLM holds the Chedoke Health Chair in Child Psychiatry at McMaster University in Hamilton, Ontario, Canada. JRMT is supported by a postdoctoral fellowship from Violence Evidence Guidance Action (VEGA). MK is supported by Ontario Ministry of Health and Long-Term Care Women’s Health Scholar Post-Doctoral Fellowship Award. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.6d159.