Article Text

Abstract
Objectives In Western countries, lower socioeconomic status is associated with a higher risk of cardiovascular disease (CVD) and premature mortality. These associations may plausibly differ in Asian populations, but data are scarce and direct comparisons between the two regions are lacking. We, thus, aimed to compare such associations between Asian and Western populations in a large collaborative study, using the highest level of education attained as our measure of social status.
Setting Cohort studies in general populations conducted in Asia or Australasia.
Participants 303 036 people (71% from Asia) from 24 studies in the Asia Pacific Cohort Studies Collaboration. Studies had to have a prospective cohort study design, have accumulated at least 5000 person-years of follow-up, recorded date of birth (or age), sex and blood pressure at baseline and date of, or age at, death during follow-up.
Outcome measures We used Cox regression models to estimate relationships between educational attainment and CVD (fatal or non-fatal), as well as all-cause, cardiovascular and cancer mortality.
Results During more than two million person-years of follow-up, 11 065 deaths (3655 from CVD and 4313 from cancer) and 1809 CVD non-fatal events were recorded. Adjusting for classical CVD risk factors and alcohol drinking, hazard ratios (95% CIs) for primary relative to tertiary education in Asia (Australasia) were 1.81 (1.38, 2.36) (1.10 (0.99, 1.22)) for all-cause mortality, 2.47(1.47, 4.17) (1.24 (1.02, 1.51)) for CVD mortality, 1.66 (1.00, 2.78) (1.01 (0.87, 1.17)) for cancer mortality and 2.09 (1.34, 3.26) (1.23 (1.04, 1.46)) for all CVD.
Conclusions Lower educational attainment is associated with a higher risk of CVD or premature mortality in Asia, to a degree exceeding that in the Western populations of Australasia.
- CARDIOLOGY
- EPIDEMIOLOGY
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The large sample size and number of events, and the use of multiple imputation of missing values, controls for both random and systematic error, and thus enables accurate estimation of associations—although ideally there would be no missing values.
-
The extensive and broad experience, both individually and collectively, of the authors ensures a cogent and informed synthesis of the results of this research project.
-
The individual participant data were compiled from existing studies, without a common protocol.
-
Education is a common measure of social status, but may be best regarded as a relative, than as an absolute, classification when comparing cultures.
Introduction
A large number of studies have clearly demonstrated higher rates of major causes of death—including cardiovascular disease (CVD), selected cancers, respiratory illness and injuries—in people who are more socially deprived.1–5 It is now well recognised that these associations are graded across the full spectrum of socioeconomic status (SES).
Most of this evidence is derived from studies of Western societies. In Asia, where the burden of chronic disease is increasing rapidly,6–8 there are prima facie reasons to anticipate that SES may have different relationships with risk to those seen for Western societies—body frames and environmental exposures, both of which are related to SES, would be expected to differ. Nevertheless, our recent review of SES and the risk of premature mortality in Asia9 found an overall inverse association between SES and all-cause, CVD and cancer mortality, albeit with substantial between-study heterogeneity in the measures of SES used and effect sizes.
To our knowledge, a direct comparison of the effects of the same measure of SES between Oriental and Occidental populations has not previously been made. Data from the Asia Pacific Cohort Studies Collaboration (APCSC), a large scale individual data pooling project based in Asia and Australasia (Australia and New Zealand), affords us the opportunity to make such a comparison.
Methods
Study design
Details of the APCSC have been described elsewhere.10 In brief, a study was eligible for inclusion if it met the following criteria: (1) the population was drawn from the Asia Pacific region; (2) it had a prospective cohort study design; (3) it had accumulated at least 5000 person-years of follow-up; (4) date of birth (or age), sex and blood pressure were recorded at baseline; (5) date of, or age at death was recorded during follow-up.
The index of SES used in this study was educational attainment, which was recorded in 24 studies within APCSC. This was self-reported and categorised into three groups: no completed education or completed only primary school; completed secondary school; and completed tertiary (university or college). Within each study, height and weight were ascertained by direct measurement; body mass index (BMI) was computed as weight (kg)/height (m2). Blood pressure and total blood cholesterol were generally measured using standard protocols.10 Study participants provided information on cigarette smoking (current smoker/non-smoker) and alcohol drinking (yes/no). Cohorts were classified as Asian if the participants were recruited from mainland China, Hong Kong, Japan, Singapore, Taiwan or Thailand; and as Australasian if from Australia or New Zealand.
End points
All studies recorded deaths11 and eight studies additionally reported non-fatal stroke, and seven reported non-fatal coronary heart disease (CHD) outcomes. Cardiovascular events were defined as fatal or non-fatal CVD, CHD and stroke; non-fatal outcomes were not recorded for cancer.
Statistical analysis
We analysed the association between education and classical risk factors for chronic disease using χ2 tests for trend. The effects of SES on clinical outcomes were analysed using Cox regression models, stratified by sex and study, and the primary analyses were stratified by region (Asia/Australasia). Further, a priori, we planned to analyse the effects of SES adjusted for age and for a range of additional potential confounding factors: BMI, smoking and alcohol consumption, systolic blood pressure (SBP), blood cholesterol and diabetes. The effects of education were summarised by tests for trend across education groups by fitting education as an ordinal variable in the Cox models. Effect modification according to region was examined using Wald tests. In secondary analyses, the hazard ratios for primary or below v tertiary education for all-cause mortality and CVD were explored within age groups by region, sex by region and across country-specific subgroups.
Many of our participants had missing values (see online supplementary appendix table S1) for several of the studied confounders (except age and SBP), with some confounders being missing for all individuals within particular studies. A variety of approaches are commonly used to deal with missing data. The complete case analysis—omitting participants with any missing value—is the simplest way which may result in reduced power and has potential for bias in the resulting estimates. Multiple imputation is a principled alternative, that can often improve power and reduce bias. Since some of the variables being imputed are not normally distributed, we imputed using the MICE algorithm,12 with (for computational advantage) ‘study’ taken as a fixed effect. Our imputation model also included educational attainment (primary or none/secondary/tertiary), age, sex, BMI, smoking status, alcohol status, SBP, blood cholesterol, diabetes, event status (yes/no), and days to event or censoring. Imputations were obtained by running independent chains of 1000 iterations to generate five imputed data sets. Sensitivity analyses included using a random effect for study in the imputation model (ie, a random intercept accounting for heterogeneity in the underlying baseline hazards across studies), multiple imputation using data augmentation, varying the random seed in the imputation process and the number of imputed data sets derived (all of which gave similar estimates; results not shown) and a complete case analysis (shown in the online supplementary appendix).
A p value <0.05 was considered significant; a priori, no corrections were made for multiple comparisons. Analyses were performed using R V.2.15.3 (R Foundation for Statistical Computing, Vienna, Austria) and SAS V.9.3 (SAS Institute Inc, Cary, North Carolina, USA).
Results
The mean age of participants in the 24 cohorts combined was 47 years; 32% were female (table 1). Compared with participants from Asian cohorts, those from Australasia were generally older and more were female. As the level of educational attainment increased, the percentage of women decreased in both regions, but more especially in Asia (table 2). In Australasia, those in the higher education groups were younger and slightly leaner; these effects were incremental across the education groups. Australasian men and women who received tertiary education were more likely to be alcohol drinkers, but less likely to smoke or have diabetes, and had lower levels of blood pressure and cholesterol than others. In the Asian studies, the gradient between education and diabetes was weaker and the gradients for alcohol drinking and mean cholesterol were reversed.
Summary characteristics of participants in the 24 APCSC studies
Baseline age-adjusted and sex-adjusted mean value (or percentage, where stated) by level of education attained
Over a median of 7.3 years of follow-up, 11 065 deaths were recorded, of which 3655 were due to CVD and 4313 were cancer (table 3). Both adjusting for the effects of age and sex and additionally adjusting for several confounders, participants with the highest educational attainment had the lowest risk of all-cause mortality, and those with the lowest attainment had the highest risk. While this gradient was seen in Asian and Australasian studies, it was markedly steeper in Asia (p value for interaction <0.0001). After full adjustment, in Asia, those with primary education or below had a 56% higher risk of death during follow-up, compared with 14% in Australasia. CVD mortality was also inversely associated with education in Asian and Australasia populations; again, the association was strongest in Asia (p=0.0002). An inverse association with increasing level of educational attainment was also found for death from cancer in the Asian studies, although the weak gradient was not statistically significant in Australasia. Education was significantly and inversely associated with other causes of death (non-CVD or cancer) in both regions: more strongly so (p=0.04), in Asia. Adjusting for potential confounders only partially attenuated the association between education and all outcomes in both regions.
Hazard ratios (95% CI) for level of education attained in relation to major causes of death
Table 4 shows the inverse associations of education with all CVD, CHD and stroke events, including non-fatal outcomes in each case. Results for all CVD were similar to those for CVD mortality. For all CHD and all stroke, inverse gradients with educational attainment were apparent, consistent with all other outcomes but the hazard ratios for CHD were relatively weak and virtually identical in the two regions (p=0.80, after full adjustment). For stroke, the hazard ratios were more extreme in Asia (p=0.007); Asians with the lowest educational attainment had a 54% higher risk of stroke, compared with the highest attainment, after full adjustment; the corresponding estimate for Australasia was a non-significant 8%. In these Asian data the stroke to CHD event ratio was roughly 2:1, whereas in Australasia it was about 1:2. Consequently the hazard ratios for stroke and CVD are relatively similar in Asia whereas the hazard ratios for CHD and CVD are relatively similar in Australasia.
Hazard ratios (95% CI) for level of education attained in relation to cardiovascular disease
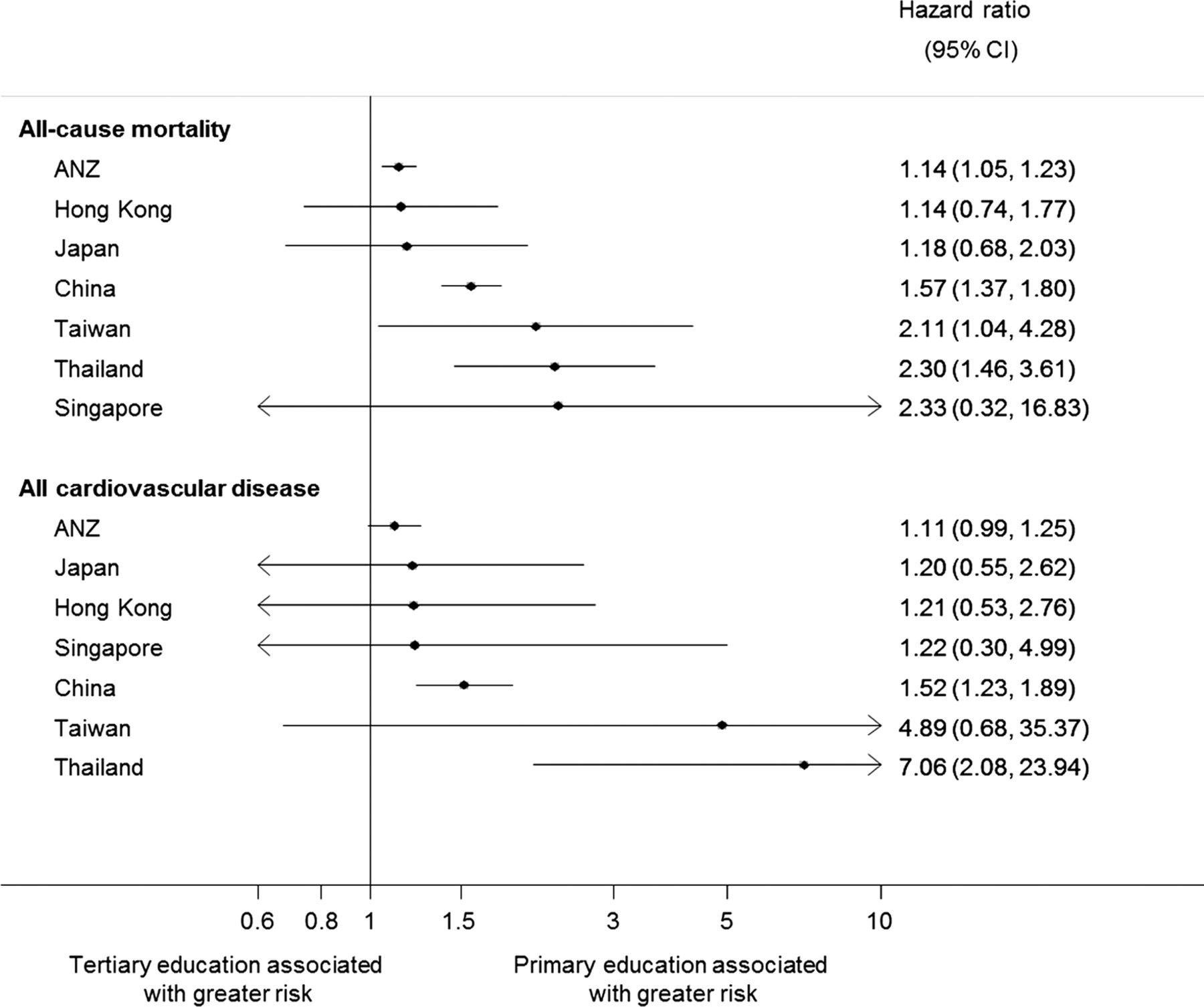
There was no evidence that the associations between education and either all-cause mortality or total CVD differed by age or sex in either region (figure 1). Country-specific analyses suggested that the differential between low and high educational attainment, in the risks of all-cause mortality and all CVD, was largest in China, Taiwan and Thailand (figure 2). Results for Singapore were unreliable due to small numbers, but for the other Asian countries results were similar to those from Australasia.

Hazard ratios (95% CIs) for primary or below versus tertiary education in relation to all-cause mortality and total cardiovascular disease, by age within region and sex within region. Hazard ratios are adjusted for age and sex (as appropriate) plus systolic blood pressure, total cholesterol, body mass index, smoking and alcohol drinking.
{kind=link}
{kind=link}
Hazard ratios (95% CIs) for primary or below versus tertiary education in relation to all-cause mortality and total cardiovascular disease, by country. Hazard ratios are for age, sex, systolic blood pressure, total cholesterol, body mass index, smoking and alcohol drinking. ANZ, Australia and New Zealand.
Results from the complete case analysis were broadly similar, especially in Australasia where there were relatively few missing values (see online supplementary appendix tables S2–S5). In Asia, the hazard ratios for primary or no education versus tertiary education were generally higher in the complete case analysis, but not so much as to alter the conclusions drawn (see online supplementary appendix tables S4 and S5).
Discussion
As far as we are aware, this is the first study to have examined the relationship between SES and mortality experience simultaneously in participants living in Asia and Western societies. We found that a relatively high educational attainment was associated with a lower risk of mortality and CVD in both populations. Overall, the gradients tended to be steeper in Asia than Australasia, with the greatest differential between low and high educational attainment being mostly seen in the least well-developed countries that were included in our study: China, Taiwan and Thailand.
Education as a measure of SES
The highest level of education attained has clear influence on occupational opportunities and earning potential. It is an attractive measure of SES for international comparisons because it is likely to be relatively well standardised between countries and is easily obtained from a standard questionnaire.13 Other advantages, compared with measures based on income or occupation, is that educational attainment is specific to an individual, relevant after retirement and not subject to possible reverse causality, whereby illness causes loss of income or employment, preceding death or clinical diagnosis of disease. On the other hand, educational attainment will rarely capture knowledge and experience gained through life, while economic returns, for the same level of education, may differ significantly across ethnic and sex groups. In our review of SES measures in Asia, educational attainment was a stronger predictor of in-study mortality than either income or occupation.9
Education and risk profiles in the Asia-Pacific region
Our results show that lower educational attainment was associated with less favourable risk profiles in Asia and Australasia. As in previous studies,2 ,14 ,15 we found inverse relationships between education and age, SBP, smoking and diabetes, with the exception that the proportion of alcohol drinkers in studies from Australasia was higher in the best educated group—consistent with previous studies in the West.16–18 Mean BMI has, as in this study, often been found to be positively related to social deprivation, although not inevitably.19 ,20 The association between serum cholesterol and level of education found in Asian and Australasian studies is consistent with previous literature which showed an inverse association between education and serum cholesterol in high-income countries but the reverse in low-income to middle-income countries.2 ,21 ,22 These differing patterns reflect rapid urbanisation of the latter, in which more educated people are more likely to move to urban areas and adopt less healthy lifestyles, such as sedentary behaviour and the consumption of proatherogenic diets.23
Education and non-communicable disease mortality in the Asia-Pacific region
Although major risk factors such as diabetes, high-blood pressure and smoking contributed to the mortality and morbidity in both regions, we generally found a steeper gradient of the effect of education on adverse outcomes in Asia compared with Australasia. This might be explained by differences in national social and economic policies. In a study of the relationship between education and mortality in nine industrialised countries, Kunst et al24 found that inequalities in mortality were twice as large in the USA, Italy and France as in the Netherlands, Denmark, Sweden and Norway and proposed that one potentially relevant factor was welfare and income policies. During the 1970s, income inequalities were relatively large in the USA, France and Italy and relatively small in the other countries. In our study, the majority of participants from Asia were living in China where the inequality gap was large in the 1990s.25 Thailand and Singapore were also in a period of rapid economic transformation during that period.
Healthcare policy and infrastructure may also play an important role. In Australia and New Zealand, like most other high-income countries, medical resources are relatively plentiful, more equitable and accessible than in China. While the healthcare reform in Australia has been well-organised since 1975, China introduced healthcare reform as late as 1997. This reform has exacerbated inequalities.26 ,27 Many public hospitals and healthcare centres in China had low government subsidies and had to rely on increasing charges from patients. Profitable hospitals were increasingly built by private entrepreneurs. As a consequence, the lack of government funding for accessible and affordable healthcare coverage became a primary cause of socioeconomic disparity in health as medical resources were concentrated in urban hospitals and the individual out-of-pocket expenses for health expenditures increased sharply.27
Differential effects of educational attainment on health outcomes could also be influenced by personal, household and neighbourhood factors.3 ,28 For example, variations in an individual's intelligence, religious belief and stress coping mechanism could intervene in the effect of education on health. A study from Scotland has shown that, after adjustment for IQ, the risk gradient across five socioeconomic indicators was markedly attenuated for both coronary heart disease and all-cause mortality.29 The family structure can be a major cause of health disparities in the elderly (different support from different family backgrounds, family size or education of the offspring). This is more likely to be an issue in Asia than Australasia; for instance, the percentage of the elderly living in nursing homes in China is less than half that in Australia.30 ,31 Environmental impoverishment, as depicted by area SES, has also been linked to health status and mortality.32 ,33
In general, those with better education are more likely to be aware of cancer symptoms, to have the opportunity for cancer screening, and to have more advanced and effective treatment. These factors probably explain the clear gradients with SES in our Asian studies. The lack of such effects in our Australasian studies is likely to be due to more homogeneous access to healthcare. There may also be differential effects by type of cancer. For example, level of education has been found to be inversely related to lung cancer, due to a lower prevalence of smoking among more highly educated people.34 ,35 In contrast, breast cancer risk is known to be greater for the more highly educated, presumably because of different reproductive patterns, such as delayed childbearing and fewer children.36 Colon and prostate cancer incidence have been inconsistently associated with level of education.37 In our study, cancer deaths were too few (especially in Asia) to reliably investigate each cancer individually, although age-adjusted hazard ratios for the most common cancers by region and sex are shown in online supplementary appendix table S6. Except for ovarian cancer in Asia, the crude death rate for the group with only primary education was always the highest.
Strengths and limitations
Our study has the strength of a large sample size, which has allowed us to produce reliable estimates, at subgroup levels, for several key outcomes. We have only considered educational attainment as a measure of SES, but we would expect broadly similar results should another measure have been used, based on our past experience with contrasting measures of SES in Asian and Western populations.9 ,38
One limitation with our Collaboration is that details on how events, especially non-fatal events, were captured are lacking. In this specific study, the biggest limitation is the great number of missing values for cholesterol, diabetes and BMI, especially in the Asian studies (see online supplementary appendix table S1). Our previous analyses39 suggested it was unlikely that multiple imputation would improve precision compared with a complete case analysis, because of the high degree of missingness, but we would expect it to lead to reduced bias. Consequently we have chosen to report values from multiple imputation as our primary results. Most missing values in the Asian data were from a Chinese occupational cohort, which contributed 77% of the data. By removing these subjects, the ‘healthy worker effect’ has been reduced. In Australasia, the complete case analysis resulted in the removal of participants from the two studies with the highest average age, reducing the mean age of the participants from 54 to 51 years. Conceivably, these systematic differences could have contributed to the general attenuation of hazard ratios with the complete case analysis, although our subgroup analyses did not suggest heterogeneity of the effects of education by age. Overall, the main conclusions from our study are the same whether or not we account for missingness. Another limitation was that the large Chinese occupational study dominates our Asian data, which limits our ability to make generalisations across Asia. Finally, those classified as primary or below in Asia were likely to have included more with no schooling at all than in Australasia, whereas those with the highest education in Australasia were likely to have more with postgraduate education. This could have exaggerated the difference in the observed gradients between the two regions.
Conclusions
Our study underscores the importance of disparities in educational attainment in cardiovascular disease, cancer and other causes of death in Asia and Australasia and, hence, the crucial role of education in disease prevention. The greater magnitude of the effect in Asia, and the huge number of people living there, suggests that national policies to strengthen education within the region would have an immense positive impact on human health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors Data analysis was performed by SAEP, FB and PV under the supervision of MW. HU, JW, GGG, SCH, XF, AD and THL supplied data. The manuscript was drafted by MW, GDB and PV and commented on by all the other authors.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval University of Sydney.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.