Article Text

Abstract
Objective This study used 2010–2018 Health Insurance Review and Assessment Service National Patient Sample data to analyse the distribution and healthcare utilisation of patients with migraine in South Korea.
Design Retrospective, observational study using serial cross-sectional data.
Participants Patients with primary diagnosis of G43, a Korean Standard Classification of Diseases-10 code for migraine, were included in the analysis. The exclusion criteria were missing code information; code for dental, health centre or psychiatry; institution type specified as nursing hospital, psychiatric hospital, dental hospital, midwifery centre or health centre; blank entries for total cost or days of care. 453 246 records of patients and 117 157 patients corresponding to those records were identified.
Outcome measures Primary outcome measures were medical service utilisation status, treatment methods and drug use status associated with migraine.
Results Cases and patients of migraine increased from 48 846 and 19 468 (2010) to 52 729 and 20 802 (2018), respectively, increases of 7.95% and 6.85%, respectively, compared with 2010. Total cost of care increased from $921 857.88 (2010) to $1 711 219.60 (2018). The most common age range of patients was 45–54 years, with 2.69 times more female than male patients. In Western medicine hospitals, subcutaneous or intramuscular injection therapy was used frequently, while in Korean medicine hospitals, acupuncture therapy was used. Among Western medicine outpatients, more than 50% of the therapeutics prescribed for acute migraine were simple analgesics or non-steroidal anti-inflammatory drugs. The number of prescriptions for the prevention of episodic migraine increased from 13 600 cases (2010) to 20 546 cases (2018), representing the steepest increase in drug utilisation.
Conclusions Treatments frequently used in Western and Korean medicine hospitals and their frequency of use and costs were identified. The findings of this study can be used as a basis for relevant health policy decisions.
- migraine
- health informatics
- herbal medicine
Data availability statement
Data may be obtained from a third party and are not publicly available.
Data availability statement
The study used HIRA-NPS data (2010–2018), which are third-party data and not owned by the authors. The HIRA data are available upon direct request, via email or fax, and submission of the request form and declaration of data use, which are downloadable from the HIRA website (http://opendata.hira.or.kr) and upon payment of a data request fee (300 000 Korean won per dataset).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study analysed the status of healthcare utilisation among patients with migraine at the national level in South Korea for over 9 years (2010–2018).
This study compared treatments between Western medicine and Korean medicine institutions in consideration of the unique situation of the dual medical system in Korea.
The study followed patients’ treatment history for 1 year and without continuity between years; therefore, long-term follow-up was not possible.
Introduction
Migraine is characterised by persistent unilateral, pulsatile pain that intensifies with physical activities and is associated with nausea, vomiting, photophobia and phonophobia.1 2 Global prevalence of migraine is reported to be around 11%–11.6%,3 4 while in Asia, it is 10.1%. In Korea, the prevalence of strict migraine and probable migraine is 6% and 11.5%, respectively.5 Moreover, migraine is twice as prevalent among females (13.8%) than males (6.9%). Further, individuals with high educational levels and urban residents are more likely to have migraine.3 Migraine was the second most debilitating disease among all neurological disorders during 1990–2015 in the Global Burden of Diseases, Injuries and Risk Factors Study.6 In fact, the daily activities of 13.4% of patients with migraine in Korea were significantly affected by migraine in 2009.7
Migraine is classified as episodic or chronic based on the total number and frequency of attacks per month. Chronic migraine is diagnosed when headaches occur more than 15 days a month for over 3 months, and more than half of the headaches (at least 8 days) show signs of migraine.8 Migraine treatment can be divided into acute and prophylactic; patients with frequent severe pain require both types. Triptans, ergotamine derivatives, non-steroidal anti-inflammatory drugs (NSAIDs), opioids and some combination of these drugs are assessed as effective options for acute treatment.9 Preventive therapy includes beta-blockers, calcium channel blockers, antidepressants, antiepileptics, etc. Preventive therapy can reduce the frequency of pain attacks, duration of persistence and severity; it can also improve responses to acute treatment.10 11 Accordingly, recent studies have focused on prevention treatments.12
Medical dualisation in the Korean medical system allows patients to choose between Western medicine (WM) and traditional Korean medicine (KM). For migraine, oral drug therapy and injection therapy (ie, nerve block injections or onabotulinum, etc) are mostly used in WM, whereas acupuncture, moxibustion, cupping and herbal medicine are used in KM. Of these, acupuncture is the most researched and accepted complementary medical treatment. Acupuncture therapy can reduce the number of days with a headache of moderate or severe intensity;13 14 is effective in reducing migraine frequency and has fewer adverse effects than drug therapy.14 Systematic reviews have identified various herbal medicines as promising treatment options because of multiple physiological effects.15–17 Therefore, WM and KM treatments can complement each other to fulfil such a role.
Data from the 2018 National Health Insurance Statistical Yearbook indicate that migraine, as a single diagnosis (International Classification of Diseases code: G43), ranked 117th with 544 438 patients, had 1 200 205 days of hospital stay and witnessed a treatment cost of 75 579 253 won.18 Consequently, studies need to comprehensively and specifically investigate the types and costs of WM and KM treatments used in clinical practice. Moreover, studies should identify the status and characteristics of disease prevalence to address the need for mutually complementary WM/KM treatments, find effective treatments and reduce economic burden.
Therefore, we used South Korean Health Insurance Review and Assessment Service (HIRA) National Patient Sample (NPS) data to analyse distribution and healthcare utilisation status of patients with migraine to provide valuable information for establishing policies to reduce medical expenditures, identify universal treatments and develop disease prevention services.
Methods
Data source
HIRA-NPS data from 2010 to 2018 were used. Health insurance claims data are generated when a healthcare facility files an insurance reimbursement claim to HIRA after providing healthcare services to a patient. HIRA provides sample data in a 1-year unit using stratified random sampling for data accessibility and convenience of researchers. These are secondary data that were statistically sampled after removing personal and corporate information from the raw data consisting of medical services claimed for 1 year, based on the commencement date of medical care for that year. Data included treatment and prescription details of all patients who used healthcare services during that 1 year with a stratified systematic sampling of patients based on age (10-year range). Approximately 1.45 million patients were included by sampling 3% of all patients.19
Study design and population
Patients with records of at least one treatment at a WM or KM institution within the applicable period for primary diagnosis of G43, a Korean Standard Classification of Diseases (KCD)-10 code for migraine, were included.
The inclusion criteria consisted of patients of all ages who received treatment for primary diagnosis of KCD-10 code G43.0, G43.1, G43.2, G43.3, G43.8 or G43.9. Moreover, claims data included information regarding service details (treatment, procedures, tests, prescribed medication, etc), diagnosis, costs paid by the insurer, patient out-of-pocket costs, patient demographic characteristics and type of institution. The exclusion criteria consisted of cases with missing code information, such as only three digits entered for diagnostic code; form code for dental, health centre or psychiatry; the type of institution specified as nursing hospital, psychiatric hospital, dental hospital, midwifery centre or health centre; zero or blank entries for total cost or number of days of care.
Statistical analysis
Patients with migraine were classified by age (eight groups in 10-year increments between <15 and ≥75 years), gender, payer type (National Health Insurance (NHI), Medicaid and others), visit type (inpatient and outpatient care) and medical institution type (tertiary hospital/general hospital/hospital, clinic, KM hospital and KM clinic). Additionally, the frequency of each was analysed.
Following the HIRA guidelines from the Ministry of Health and Welfare, the total expenditure was divided into 12 items: examination, hospitalisation, medication, injection/procedure, anaesthesia, physical therapy, treatment and surgery, testing, radiological diagnosis, radiotherapy, special equipment and psychotherapy. For the number of claims, claims from each hospital visit were counted. For the number of patients, each visit to WM and KM was counted once each for WM and KM, while patients who used both were counted only once. Total expenditure was calculated as the sum of the cost paid by the NHI and the out-of-pocket cost paid by the patient. The frequency of claim and expenditure were analysed for each item.
The treatment received during outpatient visits to a WM or KM institution, its frequency, average cost per visit and average annual total cost were investigated. In addition, yearly changes were examined by graphs.
For drug codes assigned during treatment at a WM institution, the frequency of prescription of each type of drug (acute treatment for eliminating currently existing pain and preventive treatment for suppressing future episodic pain in patients with migraine), as per American Headache Society (AHS) guidelines, with average cost per treatment and average annual total cost per patient, was investigated. The yearly changes were examined by graphs. Additionally, frequently used anatomical therapeutic chemical (ATC) codes for alimentary tract and metabolism (ATC A01–A16) and nervous system (ATC N01–N07) products were analysed. However, no direct association with migraine was found.
All expenditures were converted by the currency exchange rate (Korean won to US$) for the applicable year and adjusted based on the health sector Consumer Price Index for 2018 (online supplemental file 1). All statistical analyses were performed using SAS V.9.4 (2002–2012 by SAS Institute).
Supplemental material
Patient and public involvement
None.
Results
Number of patients and cost of medical care for migraine
HIRA-NPS data from 2010 to 2018 identified 453 246 records of patients using WM or KM institutions, and 117 157 patients corresponding to those records were identified. The exclusion criteria consisted of cases with missing code information, such as only three digits entered for diagnostic code (n=4062); form code for dental, health centre or psychiatry (n=7147); the type of institution specified as nursing hospital, psychiatric hospital, dental hospital, midwifery centre or health centre (n=2564); and zero or blank entries for total cost or number of days of care (n=1105) (figure 1).
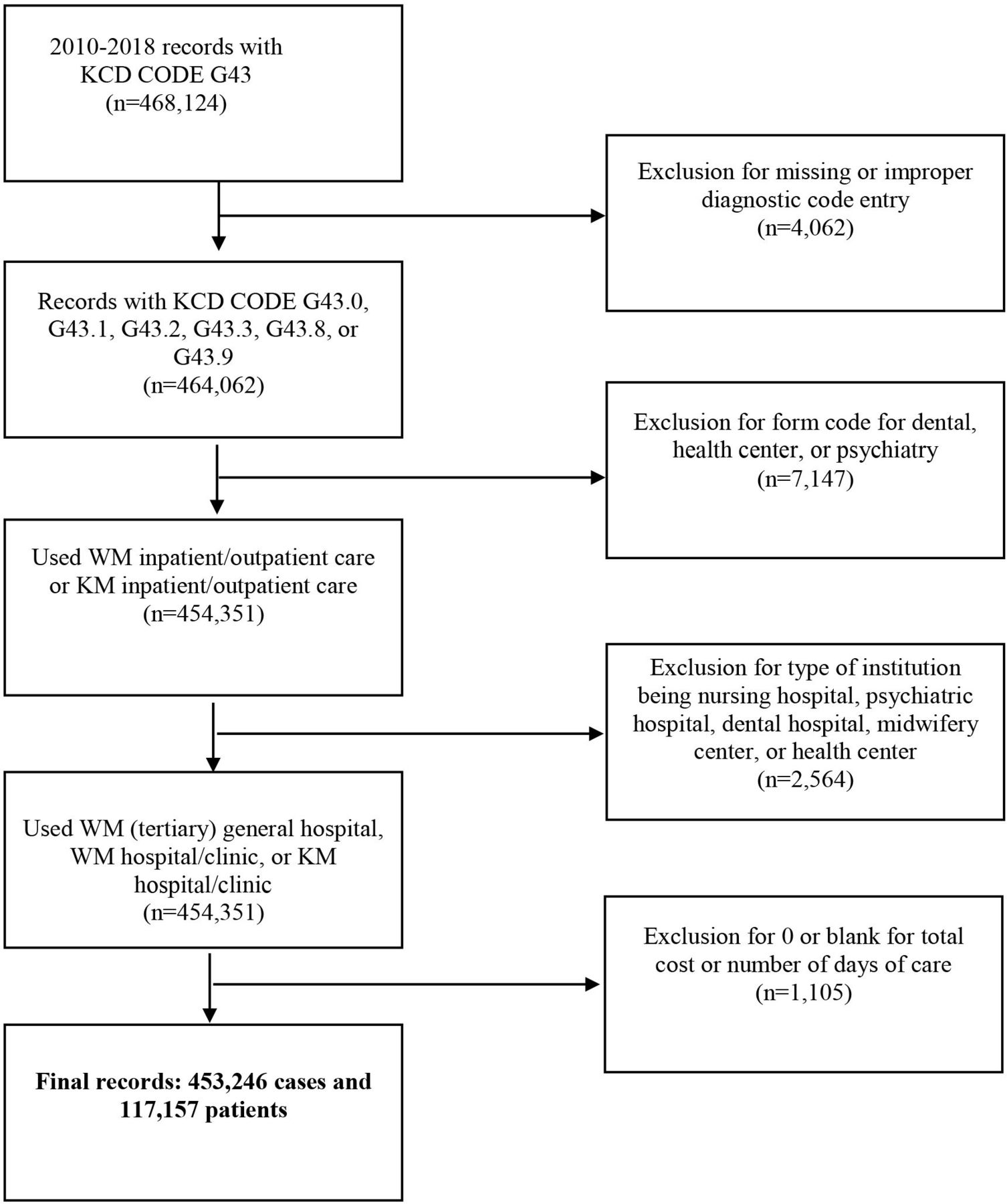
Flow chart of the study population selection. KM, Korean medicine; WM, Western medicine.
General medical service use for patients with migraine per claim
Statistics identify 48 846 migraine cases and 19 468 patients in 2010, which increased to 52 729 cases and 20 802 patients in 2018. There were no significant differences in the yearly change in patients with migraine for WM and KM institutions. However, the total treatment cost increased significantly from $921 857.88 in 2010 to $1 711 219.60 in 2018. Except for 2015, when it decreased slightly from the previous year by 4.16%, the total treatment cost increased steadily over the 9 years. Much of this increase was attributable to expenditure in WM institutions, while KM institutions’ expenditure remained constant (figure 2 and online supplemental file 2).

Growth of total and average expenditures of patients with migraine. KM, Korean medicine; USD, US dollar; WM, Western medicine.
In 2010, the average total expenditure per patient was $42.81 at WM institutions and $60.55 at KM institutions, approximately 1.41 times greater than WM institutions. However, in 2018, the value was $81.08 at WM institutions and $87.20 at KM institutions, 1.07 times higher than WM institutions. From 2013, this difference between WM and KM institutions continued to decrease. Except for 2015, the average expenditure per patient has been increasing steadily at WM and KM institutions (figure 2).
General medical service use for patients with migraine per patient
Among patients who visited a medical institution for migraine, there were 2.69 times more women (72.90%) than men (27.10%) (table 1). The payer type was 95.19% by NHI and 4.77% by Medicaid.
Characteristics of patients with migraine
Claims of healthcare utilisation according to the type of visit
Online supplemental file 3 shows the breakdown by claims of healthcare utilisation. Outpatient visits (99.10%) accounted for almost all visits to KM and WM institutions. For KM treatment, primary institutions accounted for 98.03%, indicating that most treatments were taking place in KM clinics. On the other hand, WM treatments occurred in clinics for 68.80% cases and tertiary hospital/general hospitals accounted for 31.17% cases, indicating high percentage of treatments at secondary/tertiary institutions.
Claims and medical expenditure per category
Among all treatments, the average expenditure appeared in the order of examination fee ($500 739.63), injection/procedure fee ($219 020.66), testing fee ($180 913.03) and special equipment ($132 005.79) (online supplemental file 4). Concerning the average 9-year growth rate, treatment and surgery fees increased the most (22.69%), followed by testing fee (16.22%) and hospitalisation fee (13.32%). Regarding radiological diagnosis and radiotherapy, the average number of cases over 9 years increased by 1.94%, whereas the average expenditure increased by 11.89%, showing the highest increase in expenditure per case (6.12%).
For WM-only treatment, the average expenditure appeared in the order of examination fee ($369 487.50), testing fee ($180 913.03) and special equipment ($132 005.79). Regarding the average 9-year growth rate, treatment and surgery fees were the highest (16.34%), followed by hospitalisation fee (16.34%) and testing fee (16.22%). Concerning the 9-year growth rate for expenditure per case, hospitalisation fee was highest (17.47%).
For KM-only treatment, injection/procedure fee showed the highest 9-year average total expenditure and the total number of cases ($188 946.14 and 58 585.33 cases, respectively). Concerning the 9-year growth rate for the total expenditure and total number of cases, medication fees were 10.80% and 17.53%, respectively, which were significantly higher than other items.
High frequency of care for migraine
Among WM treatments, subcutaneous/intramuscular injection showed the highest number of cases (n=57 942), followed by intravenous injection (n=16 307) (online supplemental file 5). Over 9 years, peripheral nerve block (PNB) was performed in 8033 cases with a cost of $23.87 per case, which was the highest. The total annual out-of-pocket cost per patient was $47.74, also the highest. Accordingly, each patient received approximately two sessions of PNB per year. The next highest average out-of-pocket cost per patient was personal psychotherapy at $37.35.
Among KM treatments, acupuncture had the highest number of cases (n=166 430) over 9 years and the total average out-of-pocket cost per patient per year was $27.86. The cost per case for acupuncture was $6.85, followed by bloodletting cupping ($5.83), direct moxibustion ($5.45), electroacupuncture stimulation ($3.73) and dry cupping ($3.43). The results showed that a single patient received all kinds of KM treatments approximately three to four times a year because it is an integrated treatment that includes all treatments in one session.
In the graph showing the 9-year trend in WM treatment, subcutaneous/intramuscular injection use consistently decreased, except in 2015 and 2018. However, intravenous injection and PNB consistently increased. Intravenous injection cases increased by 1.96 times from 1207 cases in 2010 to 2366 cases in 2018, while PNB cases increased by 1.71 times, from 722 cases in 2010 to 1241 cases in 2018 (figure 3). Among KM treatments, electroacupuncture stimulation and dry cupping consistently decreased (figure 4).

High frequency of care for migraine in Western medicine outpatients. DHT, deep heat therapy; ICT, interferential current therapy; IV, intravenous injection; LT, laser therapy; OI, other injection; PNB, peripheral nerve block; PT, psychotherapy; SC/IM, subcutaneous/intramuscular injection; SHT, superficial heat therapy; TENS, transcutaneous electrical nerve simulation; TPI, trigger point injection.

High frequency of care for migraine in Korean medicine outpatients. AP, acupuncture; BC, bloodletting cupping; DC, dry cupping; DM, direct moxibustion; EAST, electric acupuncture stimulation therapy; HP, hot pack; IM, indirect moxibustion; IR, infrared; PR, prescription.
Therapeutic drug use for migraine
Table 2 shows that among acute treatments for migraine, the number of cases using simple analgesics (acetaminophen, acetylsalicylic acid) or NSAIDs was highest (159 891 cases), with 54% of all acute treatments, followed by ergotamine (n=43 431) and triptan (n=39 289). The use of triptan was much lower than simple analgesics. However, the average expenditure per case and average expenditure per patient were $34.11 and $68.08, respectively, the most expensive among all migraine drugs.
Status of therapeutic drug use for migraine by purpose
For preventing episodic migraine, calcium channel blocker use was highest (62 439 cases), accounting for 42% of medications, followed by beta-blockers, antidepressants and antiepileptics. Antiepileptics showed an average expenditure per case and per patient of $11.81 and $30.78, respectively, being the most expensive among all medications.
Among drugs not classified as therapeutics but recommended for migraine by AHS, the number of cases with prescription drugs related to the alimentary tract and metabolism was highest (25% of all cases), followed by drugs for the nervous system. Of these, anxiolytics were prescribed in 86 496 cases, the third most often prescribed after simple analgesics and drugs for gastric acid-related disorders.
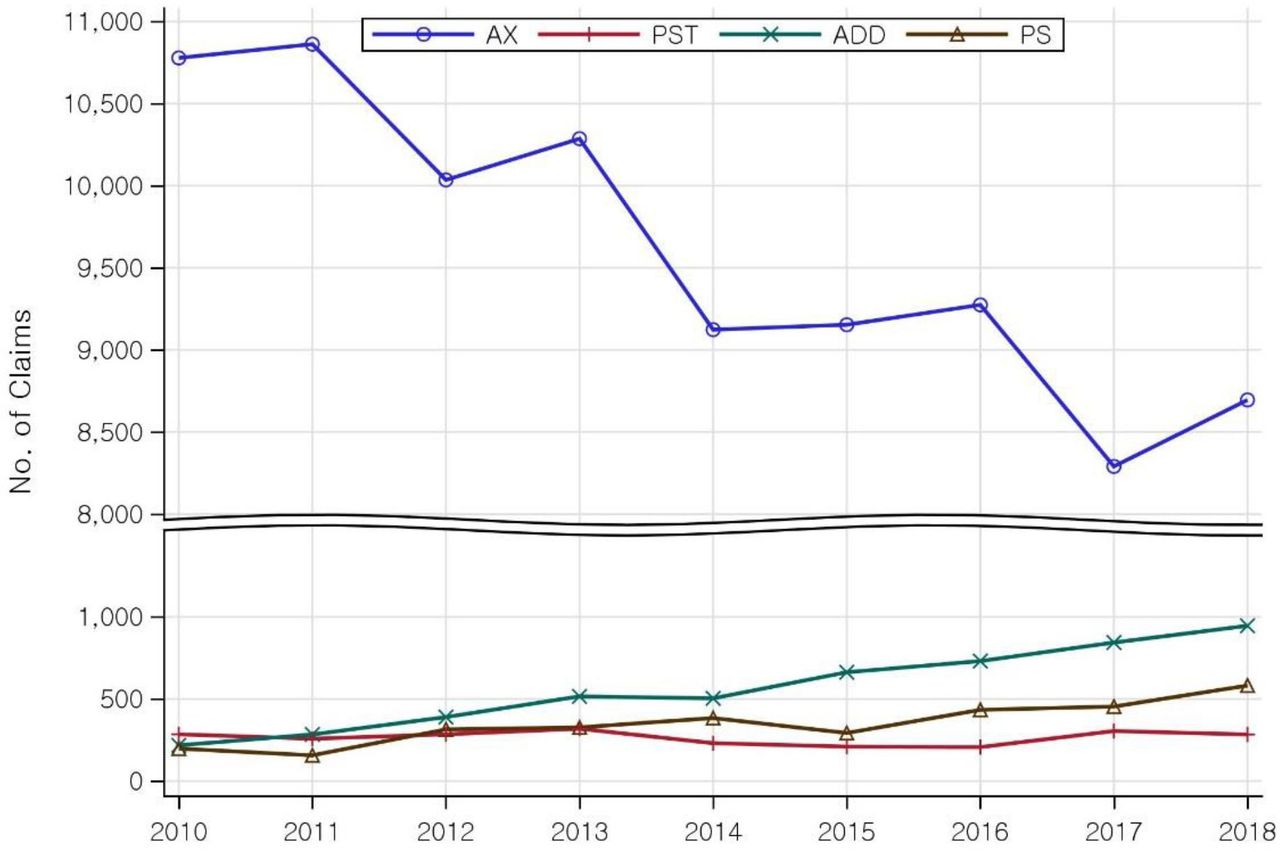
Prescriptions of both acute treatments and medication to prevent episodic migraine increased from 2010 (figure 5). Prescription for preventive medication increased sharply by approximately 1.51 times, from 13 600 cases in 2010 to 20 546 cases in 2018. Simple analgesics or NSAIDs and triptans showed an increasing trend, while other acute treatments for migraine showed no distinct trend (figure 6). Moreover, triptan use increased sharply from 2018 onwards (figure 6). Among medications to prevent episodic migraine, calcium channel blockers and antiepileptics showed an increasing trend. Of these, the use of antiepileptics showed a large margin of increase in recent years to almost 4000 cases (figure 7). Among drugs for the nervous system, prescription of anxiolytics showed a distinctly increasing trend (figure 8).

Nine-year trend of drugs used to treat migraine. AM, alimentary tract and metabolism; AT, acute treatment; NS, nervous system; OD, other drugs; PT, preventive treatment.

Nine-year trend of drugs used for acute treatment for migraine in detail. AEM, antiemetics; ER, ergots; NS, non-steroidal anti-inflammatory drugs; OP, opioids; TR, triptans.

Nine-year trend of drugs used to prevent migraine. AD, antidepressant; AEP, antiepileptics; BB, beta-blockers; CB, calcium channel blockers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nine-year trend of nervous system drugs used for migraine. ADD, anti-dementia drugs; ADHD, attention deficit hyperactivity disorder; AX, anxiolytics; PS, parasympathomimetics; PST, psychostimulant agents used for ADHD and nootropics.
Discussion
This study used HIRA-NPS data from 2010 to 2018 to analyse the distribution of patients with migraine based on patient characteristics, treatment methods, treatment costs, type of visit and annual distribution divided by WM and KM institutions. For treating migraine, WM institutions mostly use oral medication or injections, whereas KM institutions typically use acupuncture, moxibustion, cupping and herbal medicine.20 This was consistent with the findings in this study.
According to recent studies, global prevalence of migraine was 2.00 times higher among females (13.8%) than among males (6.9%),3 and women, especially those between 20 and 40 years old, showed a higher migraine prevalence (1.5-fold to 2.9-fold higher than men).21 Just as in our study, women visited a medical institution for migraine 2.69 times more than men. Prevalence by age group appeared in the order of 45–54 years (21.31%), 35–44 years (18.15%) and 55–64 years (15.92%), which was consistent with results from previous studies.22 However, prevalence by age group of patients who used only KM institutions showed a different order of 45–54 years (20.36%), 55–64 years (20.15%) and 65–74 years (19.15%). This could be attributed to KM service utilisation being relatively higher among middle-aged (40–59 years) and older adult (≥60 years) patients.23 Other studies on complementary medicine also reported that the demand for acupuncture was higher in older age groups.23 In this regard, analysis of the determinants of KM service use showed that individuals with poor subjective health status, restricted activities due to pain and chronic disease were more likely to use KM services,24 and it is believed that middle-aged and older adults tend to have more of these factors than other age groups.25
HIRA claims data from 2010 to 2018 and the frequency of outpatient and inpatient care of patients with migraine with diagnostic code of G43 were analysed. As migraine is a disease that does not restrict mobility and mostly appears as a chronic disease, outpatient care was predominantly higher.
The average expenditure per patient showed an increasing trend over the 9 years, with expenditure at KM institutions being 1.41 times higher than that at WM institutions in 2010 and 1.07 times higher in 2018; however, this difference is gradually narrowing. The most frequent treatment used at KM institutions was acupuncture, which has been reported as more effective in reducing the frequency of migraine and has fewer adverse effects than drug therapy.13 14 As KM treatments can serve as a cost-effective and complementary medical treatment option, systematic, in-depth studies and standardised treatment methods are needed for KM treatments.
The highest 9-year growth rate for total expenditure and the total number of cases with KM treatment was for medication fee, with an increase of 10.80% and 17.53%, respectively. According to HIRA drug benefit claims data, health insurance costs for herbal medicine increased by approximately 2.5 times from 14.2 billion won in 2010 to 35.8 billion won in 2018. Meanwhile, the percentage of herbal medicine cost among all treatment costs by KM institutions also increased from 0.84% in 2010 to 1.32% in 2018.23 Over the 9 years, there was an increasing trend in health insurance benefits for herbal medicine. Although the health insurance cost for herbal medicine for treating migraine continues to increase, it does not reach the average rate of increase for herbal medicine mentioned earlier.
For WM institutions, PNB had the sharpest increase in cases, which increased by 1.71 times over 9 years. PNB is a procedure used to administer local anaesthetic (lidocaine, bupivacaine or both) and a corticosteroid to the target site, based on the mechanism of reducing neuronal hypersensitivity at the secondary neuron level to reduce pain.26 27 Nerve blocks have been used for decades for treating various types of headaches, including migraine, and of these, greater occipital nerve (GON) block has been used most widely.28 However, the therapeutic effects of GON block for migraine are still controversial. One experiment demonstrated that GON block did not reduce the frequency and intensity of moderate-to-severe migraine in patients with episodic or chronic migraine, as compared with a placebo.29 However, other studies reported significant improvement in severity and duration of pain compared with a control intervention.30 31
Of the types of therapeutics, prophylactic drugs showed a larger margin of increase (1.51 times) in the number of prescriptions over the 9 years. Drug therapy for migraine can be divided largely into acute therapeutics and preventive medication. Preventive treatments are needed if migraine attacks are intolerably frequent, long-lasting, and severe or when they do not respond to acute treatment or are associated with hemiplegia or prolonged aura. Preventive treatments can reduce the frequency, duration, and severity of pain attacks and the disability due to pain by promoting better responses to acute treatment.32 In addition, the length of hospital stay and testing fees (for MRI and CT) could be reduced, thereby decreasing healthcare costs and resource usage due to migraine.33 The American Academy of Neurology recommends the following classes of medications for migraine prevention: antiepileptic drugs (divalproex sodium, valproate sodium, topiramate); beta-blockers (metoprolol, propranolol, timolol) and frovatriptan (for short-term preventive treatment of menstrual migraine). Moreover, the following drugs may be effective and should be considered for migraine prevention: antidepressants (amitriptyline, venlafaxine); beta-blockers (atenolol, nadolol) and angiotensin receptor blockers (candesartan).10 Recently, it has been reported that a protein called calcitonin gene-related peptide (CGRP), which is a neurotransmitter distributed in the peripheral and central nervous systems, plays a crucial role in causing migraine. Neuronal excitation induces secretion of CGRP and vasodilation, which then leads to migraine. By blocking these pain inducers, CGRP blockers can reduce the frequency and intensity of migraine. Therefore, CGRP blockers have been currently used as a preventive drug for migraine.34 35 According to an epidemiological study, a panel of experts recommended offering migraine preventive medication to 25.7% of patients with migraine and recommended considering migraine preventive medication for 13.1% of patients.36 Therefore, as the need for preventive medication and its use may continue to increase, future studies on their long-term use and appropriate preventive treatment strategies are necessary.
Strengths and limitations
This study had some limitations. First, diagnosis and treatment of migraine may not have been accurately reported. As the study used claims data prepared for reimbursement, it may be difficult to classify different migraine types accurately. Since HIRA-NPS only includes data submitted for receiving NHI benefits, there may be discrepancies between the diagnosis submitted by a medical service provider (physician) for health insurance reimbursement and the actual diagnosis. Medical staff may have overstated some non-existing symptoms for financial benefit or under-reported certain symptoms. Moreover, migraine is a neurological disorder with unclear pathogenesis, which may occur in combination with comorbidities, aura and prodromal symptoms.37 38 Therefore, some patients with migraine may have been excluded due to the assigning of a wrong code, while others may have been included due to misdiagnosis. In this study, we used data with G43 as the primary diagnosis code. However, cases where migraine was a subdiagnosis due to the severity of accompanying symptoms were not included. Therefore, future studies that use claims data should pay close attention to the accuracy of diagnostic codes.
Second, the study did not analyse drugs prescribed by KM institutions. HIRA-NPS claims data do not have drug pricing information for KM benefit medication reimbursed by NHI. The overall medication status of herbal medicine can only be estimated based on the total medication fee. However, the type, number of claims and amount paid for individual herbal medicine cannot be known. Moreover, even if drug pricing data were analysed, such effort may not accurately reflect the status of herbal medicine used in clinical practice. Currently, coverage for herbal medicine is very narrow, and prescriptions that could be used are fundamentally limited; further, KM treatments, mostly, are not covered. Herbal medicine currently covered by NHI includes 135 types: 68 single herb extracts and 67 mixed herb extracts. Of these, 68 single herb extracts represent only 17% of 408 herbal medicines and 13% of 518 herbal medicines in Korean Pharmacopoeia. In contrast, 56 standard prescriptions represent 15% of 381 basic prescriptions in herbal formula textbooks, meaning they represent only a small portion of herbal medicine and prescriptions appearing in the literature.39 Therefore, there is a significant limitation in analysing the type and cost of herbal medicine for migraine based on HIRA-NPS data.
Third, the data used in the study are serial cross-sectional data, which allow tracking of a patient’s treatment history for 1 year, without continuity between years. Therefore, long-term follow-up on patients is impossible. Thus, for long-term follow-up, a cohort study is recommended.
Despite these limitations, this study has the following strengths. First, this study was the first to analyse the status of healthcare utilisation among patients with migraine using HIRA-NPS data from 2010 to 2018. Moreover, no studies have compared the healthcare status of patients with migraine at the national level by year. Second, this study compared the treatment status between WM and KM institutions by considering Korea’s unique situation of a dualised healthcare system. Third, this study was also the first to divide drug therapy for migraine into acute and episodic preventive treatments to compare detailed prescription status based on the frequency of such drug therapy. While there have been studies comparing the status of individual drugs or their ingredients, no studies categorised these drugs to compare universal use status at the national level by year.
Conclusion
This study analysed HIRA-NPS claims data covering 9 years to investigate the healthcare utilisation status of patients with migraine in Korea. The study also compared and analysed visit status, type of treatment and cost of treatment separately for WM and KM institutions. To date, there have been no studies comparing healthcare utilisation for migraine at the national level; thus, the findings of this study could serve as a reference for the treatment and care for patients with migraine. The findings are also expected to be useful as a basis for national health policymaking decisions, including health insurance benefit determination and budgeting for relevant diseases.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Data availability statement
The study used HIRA-NPS data (2010–2018), which are third-party data and not owned by the authors. The HIRA data are available upon direct request, via email or fax, and submission of the request form and declaration of data use, which are downloadable from the HIRA website (http://opendata.hira.or.kr) and upon payment of a data request fee (300 000 Korean won per dataset).
Ethics statements
Patient consent for publication
Ethics approval
Informed consent was waived because the patients were unidentified. This study was approved by the authors’ Institutional Review Board (JASENG 2021-02-030).
Acknowledgments
We thank the Health Insurance Review and Assessment Service (HIRA) for providing data (HIRA-NPS-2010–2018) for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @.
Contributors SoL and JY drafted and wrote the manuscript. S-HL, YJL, SaL and I-HH supervised the entire process of research and writing. All authors made substantial contributions to conception, design and revision of the manuscript. All authors read and approved the final manuscript. SaL is responsible for the overall content of the paper as guarantor.
Funding This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (no. 2017R1A5A2015805).
Disclaimer The funder had no involvement in the study design; the collection, analysis and interpretation of the data; the writing of the report; or the decision to submit the paper for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.