Article Text

Abstract
Objective To evaluate the association of 25-hydroxyvitamin D (25(OH)D) level on sepsis severity and risk of hospitalisation in emergency department (ED) septic patients when categorised as vitamin D insufficiency according to the level of 25(OH)D<30 ng/mL.
Design Cross-sectional observational study.
Setting A 900-bed academic tertiary hospital with an ED residency training programme in Bangkok, Thailand.
Participants An observational study of 101 ED septic patients aged ≥18 years was conducted between March 2015 and September 2015.
Outcome measures The level of 25(OH)D was analysed and correlated with sepsis severity assessed by Acute Physiology Age Chronic Health Evaluation-II (APACHE-II) and Mortality in ED Sepsis (MEDS) scores, and the risk of hospitalisation.
Results One hundred and one patients were enrolled, with an average age of 68±18 years, 56% female, APACHE-II score of 14±6, MEDS score of 8±5 and 25(OH)D level was 19±11 ng/mL. The prevalence of vitamin D insufficiency in our ED septic patients was 87% and the admission rate was 88%. A significant association between 25(OH)D level and sepsis severity scores was found, which was measured by APACHE-II and MEDS scores (−0.29; 95% CI −0.41 to −0.17, p<0.001 and −0.15; 95% CI −0.25 to −0.06, p=0.002, respectively). However, vitamin D insufficiency could not determine hospitalisation (OR=1.42; 95% CI 0.27 to 7.34; p=0.68 and OR=1.65; 95% CI 0.07 to 41.7; p=0.76 when adjusted by baseline covariates).
Conclusions The vitamin D insufficiency of septic patients in our ED was high and had a significant negative association with sepsis severity. However, vitamin D insufficiency status cannot predict the hospitalisation of septic patients who were admitted to the ED. Further research is needed to investigate the role of vitamin D supplementation in the ED in affecting sepsis severity.
Trial registration number TCTR20151127001.
- accident & emergency medicine
- intensive & critical care
- geriatric medicine
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Data sharing does not apply to this article as no datasets were generated or analysed during the current study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A high prevalence of vitamin D insufficiency in emergency department (ED) septic patients.
25-hydroxyvitamin D (25(OH)D) level was associated with the severity of ED septic patients.
25(OH)D level could not predict hospitalisation in ED septic patients.
May prompt adopting strategies to treat vitamin D insufficiency in ED septic patients.
Limited in sample size and only in a single centre.
Introduction
The two important forms of vitamin D (calciferol) in the human body are vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol), which are lipid-soluble vitamins widely recognised for their role in bone homeostasis.1 2 In addition to its role in bone homeostasis, vitamin D prevents some cardiovascular diseases, stimulates insulin secretion and significantly helps regulate the immune system and inflammatory process.3–7
Emerging evidence supports a significantly low level of vitamin D in septic patients than in those without sepsis in all age groups.8–10 It is known that patients with vitamin D deficiency are susceptible to infection or sepsis.11–14 Vitamin D exerts an immunomodulatory function for both innate and adaptive systems, documented via the presence of vitamin D receptors in most immune cells.5 Vitamin D has been shown to modulate monocyte activation, alleviate the inflammatory response induced by bacteria, viruses and fungi, possess bactericidal activity, promote phagocytosis and induce proliferation and differentiation of B and T lymphocytes.14 15 Moreover, the expression of cathelicidin, a potent antimicrobial peptide synthesised from neutrophils in the respiratory tract, bladder and gastrointestinal tract epithelium, is stimulated by vitamin D.3
The vitamin D insufficiency (≤30 ng/mL) or deficiency (≤20 ng/mL) status is associated with an increased risk of infection.16 17 Moreover, previous studies and meta-analyses demonstrated that patients with a low vitamin D level were more likely to be critically ill, had longer lengths of hospital stay and had higher mortality rates than those whose vitamin D was sufficient,4 7 17–22 and also increased mechanical ventilation duration in paediatric intensive care units (PICUs).9
There is a paucity of literature on the vitamin D status of emergency department (ED) septic patients. It is unclear whether these patients present with more severe illnesses. And whether a low vitamin D status is a risk factor for sepsis requiring hospitalisation.
Objectives
The main objective of the study was to assess the relationship between 25(OH)D levels on sepsis severity. The secondary objective was to demonstrate the risk of hospitalisation in ED septic patients who had a low level of vitamin D.
Methods
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Study design, setting and population
This was a cross-sectional study that included convenience sampling of patients who presented to the ED at a single academic tertiary hospital with an ED residency training programme in Bangkok, Thailand, between 1 March 2015 and 30 September 2015 during 08:00–24:00. Subject inclusion criteria were patients aged ≥18 years who visited ED with the clinical suspicion of sepsis and met the sepsis criteria at ED triage by the ED nurses.
Study protocol
ED triage nurses in our centre performed sepsis screening using the ‘Fast track SIRS’ criteria. The criteria included a patient with suspected infection who met at least two out of three criteria for determining systemic inflammatory response syndrome (SIRS); which were body temperatures less than 36°C or at more than 38°C, the respiratory rate more than 20 breaths/min or heart rate of more than 90 beats/min (bpm). Then ED nurses triage would tag the medical record card with ‘Fast track SIRS’ to activate all the ED team. Patients with pregnancy, history of pulmonary tuberculosis (TB), chronic kidney disease (CKD) stage 5, end-stage renal failure or chronic liver Child C, and if they or their healthcare proxy did not give consent for participation in this study were excluded.
Sample size
The sample size was determined to be at least 86 cases to obtain a significant p value of <0.05 and a power of 80% based on the study by Trongtrakul and Feemuchang10 which they found vitamin D insufficiency in 90% (87 of 96) of their septic patients in the preliminary results.
Definition of vitamin D insufficiency
We categorised the patients’ status of vitamin insufficiency into low when the level of their 25(OH)D was less than 30 ng/mL and sufficient for those who had a 25(OH)D level was ≥30 ng/mL according to the definition of the Endocrine Society.23
Serum 25(OH)D levels were analysed based on the electrochemiluminescence technique for the immunoassay method on the Cobas e 601 analyser (Roche Diagnostics, Indianapolis, Indiana, USA). The quality control of our laboratory module followed ‘the Randox International Quality Assessment Scheme programme’ and our unit was certified with ‘the ISO 15189: 2012 standard’. The variation coefficients of the assay were 6.5% at 19.4 ng/mL and 9.5% at 39.1 ng/mL.10 A qualification with 176-sampling compared with ‘the Bureau of Laboratory Quality Standards of the Ministry of Public Health of Thailand’ was reported with a sensitivity of 99.9% and a specificity of 99.9%.
Statistical analysis
Data were collected by a trained senior emergency medicine resident from the electronic medical records including age, sex, body mass index (BMI), vital signs, comorbidities, sepsis severity score assessed by Acute Physiology Age Chronic Health Evaluation-II (APACHE-II) score, and Mortality in Emergency Department (MEDS) score, hospital admission rate and the laboratory investigations. Venous blood sampling was drawn for 25(OH)D levels, complete blood count, blood urea nitrogen (BUN), creatinine, electrolytes, calcium, magnesium, phosphate and serum lactate level.
Categorical data were compared between vitamin D insufficient and sufficient patients reported by frequency (n) and percentage (%). Continuous data were reported by the mean and SD or median and IQR 1 and 3 (IQR 1, 3) as appropriate. The statistical relationship for categorical data was tested by the χ2 test or Fisher’s exact test, whereas the Student’s t-test was used for normally distributed continuous data, or the Mann-Whitney U test was used for non-parametric configuration. The association between vitamin D level and sepsis severity measured by APACHE-II and MEDS scores were analysed using univariable linear regression analysis.
Moreover, the risk for hospitalisation in vitamin D insufficient patients was analysed using multivariable logistic regression analysis adjusted by their baseline characteristics. Selection criteria for including variables as covariates were based on a p value less than 0.10 in univariable analysis. All data were analysed by using SPSS Statistics for Windows, V.22. (IBM Corp, New York, USA). A p value of <0.05 was considered the statistical significance.
Results
One hundred and five patients were eligible for the study. Four patients with a history of tuberculosis, chronic kidney disease (CKD) stage 5 and end-stage kidney disease (ESKD) were excluded, and there were no participants with missing data. Thus, a total of 101 patients were enrolled in the study. The overall baseline characteristics were a mean age of 68±18 years and 57% (n=57) were female. Sepsis severity from our ED patients assessed by APACHE-II score and MEDS score was 14±6 and 8±5, respectively. The demographic and characteristics were given in table 1, which no significant difference variables between the two groups of patients with insufficient vitamin D and sufficient vitamin D, except for the levels of 25(OH)D. Mean serum 25(OH)D levels in the total patients, vitamin D insufficient group and sufficient vitamin D group were 19±11 ng/mL, 15±8 ng/mL and 40±8 ng/mL, respectively.
Characteristics of septic patients according to vitamin D insufficient and vitamin D sufficient groups
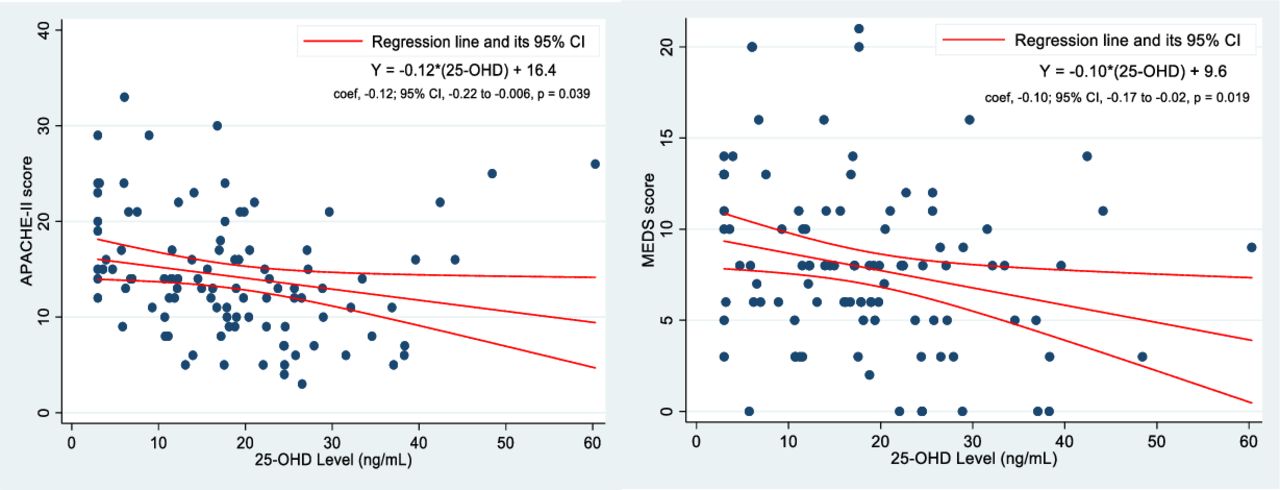
Regarding the outcome, the overall rate of hospitalisation was 88% (89/101). While, no significant differences regarding hospitalisation was found when comparing the status of vitamin D insufficient and sufficient, 89% versus 85%; p=0.65 (table 1). Additionally, we found that the level of 25(OH)D had a negative correlation to sepsis severity as assessed by APACHE-II and MEDS scores. Interestingly, a high level of 25(OH)D level greater than 40 ng/mL was found in five cases (online supplemental figure 1). The possibility of vitamin D supplementation shortly prior to the measurement may be the reason. Thus, we omitted these five cases. After reanalysing the regression line, we found the slopes at −0.29; 95% CI −0.41 to −0.17, p<0.001 and −0.15; 95% CI −0.25 to −0.06, p=0.002, respectively. Therefore, the level of 25(OH)D could be translated to predict sepsis severity with the equation of APACHE-II=−0.29×(25(OH)D+18.9 and MEDS=−0.15×(25(OH)D+10.5 (figure 1).
Supplemental material
{kind=link}
The correlation between 25-hydroxyvitamin D (25-(OH)D) level and (A) Acute Physiology Age Chronic Health Evaluation-II (APACHE-II) and (B) Mortality in ED Sepsis (MEDS) score.
Table 2 shows baseline characteristics of septic patients who were hospitalised versus those who were not hospitalised. Risks of hospitalisation in the univariable analysis were older age (p<0.001), lower SpO2 (p=0.01), high-grade severity score by APACHE-II and MEDS scores (both p<0.001), higher serum lactate (p=0.02) and lower serum chloride level (p=0.02). Besides, the univariable analyses demonstrated some trends toward significance from serum sodium (p=0.097) and serum albumin (p=0.06). All of these variables were included in multivariable logistic regression analysis as adjusted covariates.
The characteristics of septic patients according to hospitalisation status
We found no significant differences in the proportion of vitamin D insufficiency between the patients who hospitalisation compared with those who did not hospitalise, 88% versus 83%, respectively, p=0.65. Indeed, the level of 25(OH)D were also not different, with the value of 18±12 ng/mL versus 22±10 ng/mL, respectively, p=0.33. The result of our study revealed that the risk of hospitalisation could not be explained by vitamin D insufficiency. There was a positive effect size but without statistical significance, with OR=1.42; 95% CI 0.27 to 7.34; p=0.68 and OR=1.65; 95% CI 0.07 to 41.7; p=0.76 after adjusting for covariates (table 3). Moreover, the crude level of the 25(OH)D level also could not predict hospitalisation, OR=0.98; 95% CI 0.93 to 1.03; p=0.33. It still was not statistically significant after adjusting for baseline covariates, OR=0.99; 95% CI 0.86 to 1.15, p=0.94 (online supplemental table 1).
Supplemental material
Multivariable logistic regression analysis for vitamin D status associated with risks of hospitalisation of septic patients
Discussion
This study showed the prevalence of vitamin D insufficiency (25(OH)D<30 ng/mL) in our ED septic patients was high (87%) in Bangkok, Thailand, and the mean vitamin D level was equal to those in other South-Asian countries.24 Vitamin D insufficiency was also correlated with sepsis severity in the ED similar to studies in other clinical departments, similar to Ginde et al’s study.16
There is a correlation between vitamin D insufficiency and APACHE-II and MEDS scores by linear regression analyses (−0.29; 95% CI −0.41 to −0.17, p<0.001 and −0.15; 95% CI −0.25 to −0.06, p=0.002, respectively). However, vitamin D insufficiency does not independently correlate with the risk of hospitalisation, so vitamin D cannot be used to predict the need for admission. However, a higher APACHE-II score, lactate and chloride significantly increased the risk of hospitalisation. We suspect this is because high APACHE-II scores are a correlate of disease severity that is often used in the intensive care unit. Therefore, those with high scores on arrival to the ED are likely to be hospitalised.
Overall, vitamin D insufficiency is a prognosticator for sepsis severity but it cannot be used to identify which patients need hospitalisation. Measuring a vitamin D level in the ED is important if it will help decrease sepsis severity and improve outcomes.
The consequences of vitamin D insufficiency and deficiency are important, especially in sepsis17 25 because all prevention, evaluation and treatment of sepsis are crucial for reducing morbidity and mortality. Early identification and treatment of vitamin D insufficiency may improve antibacterial immunity and reduce sepsis severity.
Current evidence supported that a low level of 25(OH)D was independently associated with a higher risk of sepsis in critically ill patients.17 The particular risk was greater among septic patients with the most severe form of vitamin D deficiency, where 25(OH)D of less than 10 ng/mL.7 Interestingly, other subgroups of septic patients with vitamin D insufficiency (25(OH)D 20–30 ng/mL) or vitamin D deficiency (25(OH)D 10–20 ng/mL) could not indicate the risk of mortality at all.7
Unfortunately, the result of trials with the early high-dose vitamin D supplementation in intensive care unit (ICU) patients did still not show the benefit of the length of stay and hospital mortality over the placebo.26 27 The reasons for negative trials might be explained by a not yet-known appropriate dosage of vitamin D, the route of vitamin D administration, the proper time for vitamin D administration and the heterogeneity spectrum of patients with sepsis. Thus, direct future research with a larger sample size and more homogeneity of septic patients is needed.14 Additionally, besides only supplement vitamin D, a cocktail of medications that can modulate inflammation, such as, vitamin D in combination with a statin or metformin may need further investigation for treating sepsis.28
On the other hand, the Putzu et al study showed an association between vitamin D administration and significantly lower mortality rate in critically ill patients,29 and the Wang et al study showed the benefit of single-dose vitamin D to the incidence of septic shock in children with vitamin D deficiency in PICU.30 Additionally, a specific type of infection and the benefit of vitamin D supplementation was reported from one systemic review and meta-analysis in respiratory tract infection (46 randomised controlled trials).31 This study revealed the statistically significant benefit of reduced risk of acute respiratory tract infection (ARI) in children. Nonetheless, the Pham et al study in 2021,32 showed no clinical significance in the duration or severity of symptoms in older adults with ARI who were given vitamin D supplementation.
It has remained controversial whether supplementation of vitamin D in septic patients since ED would be beneficial. Nevertheless, we have demonstrated the correlation between vitamin D status and sepsis severity in ED. Afterward, we plan to study the dose, route and timing of vitamin D administration in ED sepsis patients and its impact on 30-day mortality since a prior US-based study demonstrated a significant difference in 30-day mortality in septic patients with insufficient vitamin D levels.4
The SIRS, quick Sequential Organ Failure Assessment (qSOFA) and National Early Warning Score (NEWS) are widely used to identify sepsis in ED as well as the conventional biomarker—serum lactate.33 34 Perhaps by studying the correlation between vitamin D and the qSOFA, the NEW score may improve prognostication in sepsis care.
There are several limitations to our study. We do not know the prevalence of vitamin D insufficiency in the overall ED population because this study only looked at the prevalence in patients identified as septic. This was also a single-centre study, a multi-centred study would provide a more comprehensive picture of sepsis and vitamin D insufficiency in Thailand. We also did not study 30-day mortality because our sample size was not sufficient enough to look at the association with 30-day mortality. Additionally, some inflammatory biomarkers, such as C reactive protein or interleukin 6, may be valuable to compare with the level of vitamin D. Unfortunately, at the time of our study performing, we did not routinely measure these laboratory investigations as is our current practice during the COVID-19 pandemic.35
Further areas of study could look at whether interventions such as the dosage and timing of vitamin D supplementation in septic patients presenting to the ED improve outcomes. Many studies have focused on the prevention or treatment of vitamin D deficiency after admission to the ICU for sepsis patients, and the results of these studies have been mixed.16 24–27 31 32 In addition, there are limited studies of vitamin D treatment in the ED.16
Conclusion
Vitamin D insufficiency is associated with severe sepsis as assessed by APACHE-II and MEDS scores. However, vitamin D levels in the ED cannot be used as a predictor of the need for hospitalisation. Further studies are needed to study if the early intervention of vitamin D insufficient patients can reduce sepsis severity and improve patient outcomes.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Data sharing does not apply to this article as no datasets were generated or analysed during the current study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Review Board (IRB) of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand: COA 69/2558. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @alissara115
Contributors AV, MR and KT performed the study and theme-generating data analysis; AV, MR and KT contributed to the project methodology and design; AV, PCI and KT drafted the manuscript; AV, MR, PCI and KT critical revision of the manuscript for important intellectual content and statistical expertise. All authors approved the final version of the manuscript to be published. KT is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.