Article Text

Abstract
Objective To examine long-term effectiveness of rehabilitation services on physical function, pain severity and post-traumatic stress disorder (PTSD) in earthquake survivors over a 4-year period.
Design Prospective cohort study with early and late intervention and geographical control group.
Setting Three counties of Sichuan Province, China.
Participants 591 survivors of the 2008 Wenchuan earthquake were followed-up over a 4-year period ranging from 2008 to 2012.
Interventions In Mianzhu county, a comprehensive hospital-based and community-based rehabilitation programme was implemented in September 2008; in Anxian county, the same programme was implemented 1 year later; in Shifang county, the programme was not implemented and survivors from this county served as a control group.
Outcomes Physical function was measured using Modified Barthel Index (MBI), pain severity with Visual Analogue Scale and PTSD with the PTSD Checklist-Civilian Version. All outcomes were assessed at three time points (baseline from 2008 to 2009, 2010 and 2012) and analysed with mixed effects regression.
Results 400 patients completed all assessments. In all groups, physical function and pain severity improved over time. MBI improvement per month as compared with control was greater in the late rehabilitation (b=1.69, 95% CI 1.20 to 2.19) than the early rehabilitation group (b=0.96, 95% CI 0.68 to 1.24). This rehabilitation effect was however marginally decreasing over time. Superior improvement as compared with control with regard to pain was only found in the early rehabilitation group (b=−0.05, 95% CI −0.09 to −0.02). PTSD symptoms decreased over time, but the observed differences could not be specifically linked to the rehabilitation intervention.
Conclusion Physical rehabilitation of earthquake survivors appears to be effective in improving physical function and, if delivered early, pain. Effects on mental health are less clear and need further examination using more consistent and frequent assessments of relevant outcomes and determinants.
- rehabilitation medicine
- pain management
- mental health
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This prospective cohort study followed Wenchuan earthquake survivors over a 4-year period.
It evaluated the effectiveness of a comprehensive rehabilitation programme delivered along the continuum of care from the hospital to the community with a quasi-experimental design.
A control group of survivors from a setting where the programme was not implemented, survivors from an early implementation setting, and survivors from late a late implementation setting were compared with regard to functional and psychological outcomes.
Lack of baseline measurements for post-traumatic stress disorder precluded determination of initial rehabilitation effects.
Generalisability of our study to all Wenchuan earthquake victims with disabilities is limited as only patients with disabilities who presented at our partner hospitals could be included.
Introduction
Natural disasters can cause a significant numbers of sudden onset impairments such as complex fractures, amputations, spinal cord injuries (SCI), traumatic brain injuries (TBI) and peripheral nerve injuries that may result in disabilities including reduced functional independence, mental health problems and chronic pain.1–8 While it is generally agreed that natural disaster response should incorporate early rehabilitation programming for long-term health-related benefits, this has been traditionally neglected.9–11 On one hand, this neglect is due to the lack of or underdeveloped rehabilitation infrastructure in less-resourced settings where natural disasters usually have the greatest health impact.12 13 On the other hand, limited evidence with regard to the effectiveness of rehabilitation intervention programmes in disaster settings including a lack of evidence on longer-term functional outcomes may lead to reluctance of governmental and non-governmental relief organisations to fund and implement such programmes.14
The 2008 Sichuan earthquake resulted in 87 476 deaths and 350 000 injured persons of whom 10 000 sustained severe injuries including fractures, amputation, SCI and TBI.8 Under the direction of the Chinese Association of Rehabilitation Medicine, a comprehensive rehabilitation programme comprised of hospital-based and community-based services was implemented in two heavily affected, neighbouring counties in Sichuan province.8 Combining resources of non-governmental organisations (NGOs) (N), health departments (H) and rehabilitation volunteers (V), the so-called NHV programme included an evaluation strategy consisting of three prospective patient assessments. While effectiveness of rehabilitation services regarding improvement of physical function between 2008 and 2010 had been demonstrated previously, development of patient outcomes over a longer time frame remains to be investigated. Moreover, data on other outcomes including pain and mental health had not been analysed yet. While function and pain are primary targets of physical rehabilitation interventions in earthquake survivors, effects on mental health outcomes such as post-traumatic stress disorder (PTSD) symptoms are also conceivable, with possible pathways being through improved physical activity15 and social support16 among others. This study aims to close these gaps by evaluating the effectiveness of the NHV-rehabilitation services programme on outcomes of earthquake survivors with disabling injuries over a 4-year period ranging from 2008 to 2012. Follow-up data regarding physical function as well as additional outcomes including pain severity, and post-traumatic stress symptoms are analysed.
Methods
Design
This is a prospective cohort study with two intervention groups, a control group and three points of measurement over a 4-year period. Data are from a programme evaluation and secondarily analysed in this study.
Setting
Following the 2008 earthquake, a rehabilitation services programme was implemented in Mianzhu county (NHV-E) in September 2008 (4 months after the disaster) and in Anxian county 1 year later (NHV-L). The same rehabilitation programme was planned for implementation in Shifang county where participants were recruited and a baseline survey conducted with informed consent procedures as described in the previous section. However, due to resource constraints the county government eventually decided not to implement the programme. Participants from Shifang county who had initially been deemed eligible for rehabilitation, instead served as geographical control group.
All counties were heavily affected by the Wenchuan earthquake with 11 098 fatalities and CNY142.3 billion (CNY) total damage in Mianzhu, 1571 deaths and CNY88.9 billion total damage in Anxian and 5891 casualties and CNY12.2 billion total damage in Shifang. Distance from Wenchuan earthquake epicentre was 65 km, 95 km and 68 km for Mianzhu, Anxian and Shifang, respectively. The geographical location of the study counties is illustrated in figure 1. Baseline data were collected between September 2008 and March 2009 for NHV-E, in September 2009 for NHV-L, and in March 2009 for the control county. Initial follow-up assessments took place from August to November 2010 for NHV-E, from November 2010 to January 2011 for NHV-L, and from January to March 2011 for the control group. All groups were assessed a third time in July 2012. Baseline data were collected in the field. All other data were collected at central sites, that is, township hospitals.
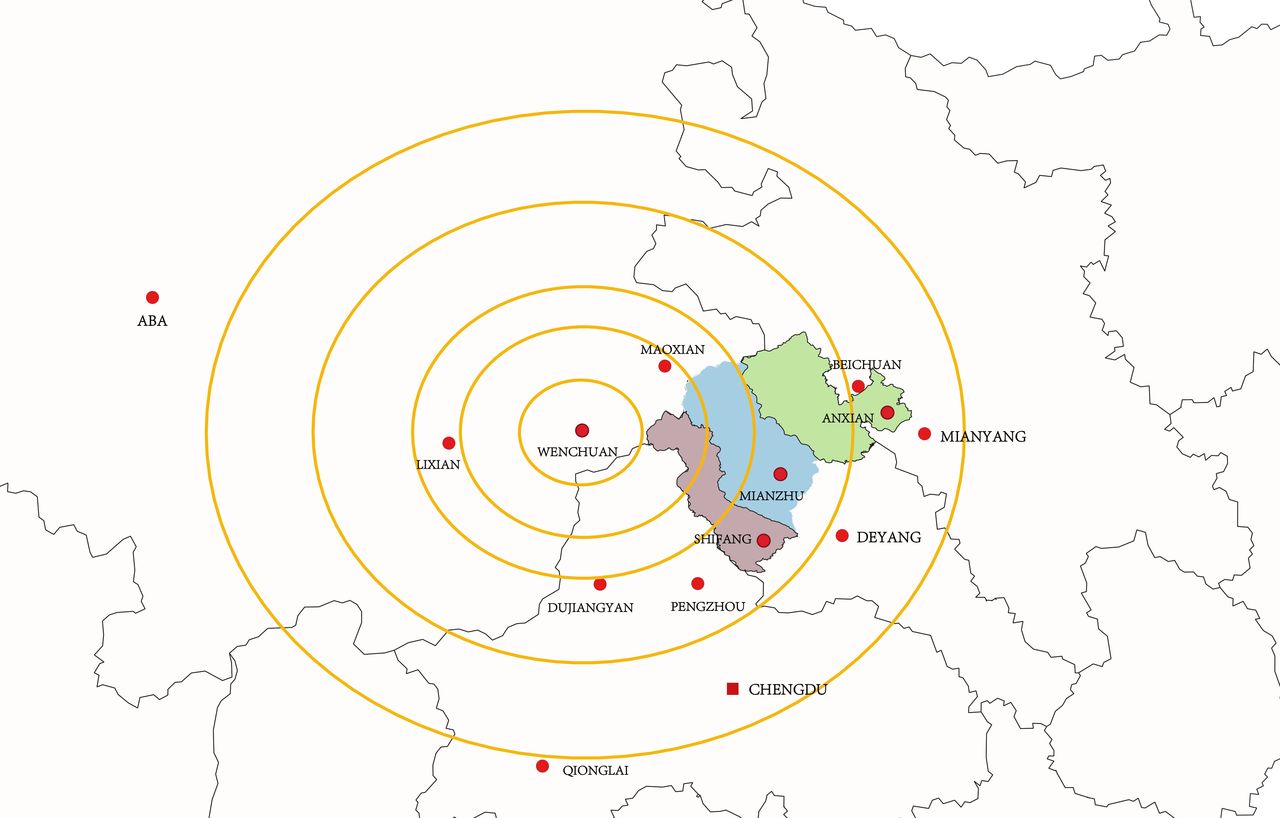
Geographical location of study counties (Mianzhu=NHV E, Anxian=NHV L, Shifang=control group) and distance from earthquake epicentre in Wenchuan.
Recruitment and sample size
Participants were recruited into the rehabilitation programmes (NHV-E and NHV-L) or intended programme (control) by county level health departments, hospitals and NGOs contributing to the programme. Rehabilitation services were offered free of charge. Since this was primarily an earthquake rehabilitation relief programme and not a research project, no formal sample size calculation was conducted.
Participants
According to the principles of intention to treat analysis, data from all participants initially recruited into the programme are included in this study in so far as they meet the following inclusion criteria: adult Wenchuan earthquake survivor with fracture, SCI, TBI, amputation, soft tissue or crush injury caused by the disaster and residing in one of the three counties mentioned above, provided written informed consent for participation in the programme evaluation, and not currently enrolled or had previously participated in another rehabilitation programme for treatment of Wenchuan earthquake-related injuries.
Interventions
The NHV multidisciplinary rehabilitation services programme included individualised hospital-based rehabilitation (at county-level hospitals) including rehabilitation medicine, physical and occupational therapy interventions and nursing care. Rehabilitation interventions included muscle strengthening and range of motion exercises, training in self care and mobility activities, education in bladder, bowel and skin care management, and provision of assistive devices if indicated. Duration of inpatient rehabilitation was 52.4 days on average in NHV-E (SD: 19.1, minimum: 9, maximum: 147 days) and 51.8 days in NHV-L (19.2, minimum: 13, maximum: 123 days). Average costs of inpatient rehabilitation were CNY6187 in NHV-E (SD: 2646.18, minimum: 1999, maximum: 28 093) and CNY 6225 in NHV-L (SD: 2162.15, minimum: 1308, maximum: 18 993). Once discharged to the community patients received limited follow-on medical rehabilitation services. Additional community-based rehabilitation services addressed personal empowerment, social support and employment via personal assistants, patient self-help peer groups and employment services, respectively, among other interventions. NHV focused initially on institutional rehabilitation and shifted to community-based rehabilitation when most earthquake victims were discharged into the community. The programme is described in more detail elsewhere.8
Measures and procedures
Primary rehabilitation outcomes included physical function and pain and were measured at all three assessment points. The secondary outcome PTSD was only assessed at the two follow-up occasions: in 2010 and 2012. Physical function was assessed using the Modified Barthel Index (MBI) (Chinese version), a measure of independence in activities of daily living and continence,17 while pain severity was measured with a Visual Analogue Numerical Rating Scale (VAS) ranging from 0 (no pain) to 10 (most severe pain the subject can imagine). Post-traumatic stress symptom severity was measured with the Chinese Version of the PTSD Checklist-Civilian Version (PCL-C).18
Sociodemographic information included age, gender, marital status, years of formal school education and injury type (summarised from hospital International Classification of Diseases - version 10 diagnostic codes). Few patients sustained crush, peripheral nerve or soft tissue injuries, these were therefore collapsed into one category ‘other injury’ for further analysis. All measures were incorporated in an assessment form administered by trained rehabilitation volunteers. Data were subsequently entered by two coders independently and differences reconciled.
Analysis
All analyses were performed with Stata V.14. The command gllamm was used for longitudinal Tobit models and mixed for linear mixed-effects regression.
Rehabilitation effectiveness on primary and secondary outcomes was analysed with longitudinal, mixed-effects regression models. In contrast to ordinary least squares regression, mixed-effects models account for clustering of participants in counties and correlation of repeated measurements within subjects. If rehabilitation services are effective heteroscedasticity, that is, different variances in subpopulations at different time points, is furthermore likely as interventions should reduce rehabilitation group variance over time. Accordingly, robust SEs based on the Huber-White sandwich estimator were calculated to allow appropriate estimation in case of heteroskedastic residuals.
Primary outcomes
The MBI and VAS pain scales19 have known ceiling and floor effects, that is a non-negligible proportion of participants assumes values at the scale maximum or minimum. For example, if a participant reaches the scale maximum of 100 for the MBI further improvement can no longer be measured. Longitudinal Tobit regression was used to model these outcomes to account for this issue. Maximal (or minimal) scale values are then said to be censored. In principle, a Tobit model estimates a latent variable that can assume values above the scale maximum (or below the scale minimum) by modelling censored data based on a binomial distribution with a scaled probit link and uncensored data based on a normal distribution and an identity link.8 Against this background, rehabilitation effectiveness was estimated by including binary variables for belonging to one of the rehabilitation groups (NHV-E, NHV-L) to represent baseline imbalance, time from earthquake to measurement in months to represent recovery due to other factors than rehabilitation (spontaneous recovery) and interaction terms for the rehabilitation effects over time (NHV-E*time; NHV-L*time). Due to baseline imbalance in demographic characteristics and injury types as well as differences in drop-out patterns (see the Results section, table 1), models were adjusted for gender (referent: female), age (mean centred), marital status (referent: not married), years of formal education (mean centred) and injury type (referent: fracture). Model fit was evaluated as follows: As data were clustered at two levels, that is, measurements nested in subjects which were nested in counties, the fit of models including random intercepts for subject and for subject and study county was tested. Furthermore, a model including a random slope for time to account for differences in individual responsiveness to time was considered as well. Finally, it is likely that rehabilitation as well as spontaneous recovery effects will decrease over time, that is, be larger at the beginning than at the end of the study period. Accordingly, we also tested a model which encompassed quadratic terms for time and rehabilitation effects in addition. Models were fitted subsequently and compared by likelihood ratio test; p values were corrected for the number of tests (Bonferroni adjustment). Based on the fixed parameters of the final models, trajectories for the different intervention groups were estimated adjusted for covariates and plotted.
Demographics and injury types across intervention groups and drop-outs (2010–2012)
Secondary outcome
PCL-C was analysed with a linear mixed-effects regression model adjusting for above mentioned demographics and injury type. Again random intercepts for subject and county as well as a random slope for time was considered. As data from only two assessment points were available, modelling of non-linear recovery and rehabilitation effects was not applicable in this case. Also, the interaction terms representing rehabilitation effects were simplified to dichotomous variables indicating belonging to one of the rehabilitation groups at follow-up (NHV-E*follow-up; NHV-L*follow-up). Since rehabilitation may only have an indirect effect on secondary outcomes through primary outcomes, a model including MBI and VAS as predictors was also tested. In the case of more than one random effect an exchangeable covariance matrix was employed.
Final models: In the case of MBI and VAS pain the best fitting model was a two-level random coefficient model featuring quadratic polynomials for time and rehabilitation effects and introducing a random intercept ζi for subject i and a random slope ξi accounting for individual variation in change over timepoints j. The residual error is noted by εij. The model formula reads:
VAS/MBIij*=b0+b1*malei +b2*agei +b3*marriedi +b4*educationi+b5*SCIi +b6*TBIi +b7*amputationi+b8*other injuryi +b9*timeij +b10*time2 ij + b11*NHV-Ei +b12*NHV-Li +b13*(NHV-E*timeij)+b14*(NHV-E*time2 ij)+b15*(NHV-L*timeij)+b16*(NHV-L*time2 ij) + ζi + ξi*time + εij with



The best fitting model for PCL-C was a two-level random intercept model employing the primary rehabilitation outcomes BI and VAS pain as predictors. The model formula reads:
PCL-Cij*=b0+b1*malei +b2*agei +b3*marriedi +b4*educationi+b5*SCIi +b6*TBIi +b7*amputationi+b8*other injuryi +b9*timeij +b10*NHV-Ei +b11*NHV-Li +b12*(NHV-E*follow upij)+b13*(NHV-L*follow upij)+b14*BIij +b15*VASij + ζi + εij with

Sensitivity analysis
Missing outcome data were exclusively due to lost to follow-up. Since only about 68% of the patients had completed all three assessments, bias introduced through missing data could be an issue. Under the assumption that data were missing at random (MAR-scenario), that is, missing of observations is determined by the previously observed data and not by the outcome values that would have been measured if subjects had not dropped out, mixed effects models do not produce biased estimates in the case of missing observations.20
To test this assumption and correct for study attrition, we used the propensity score method21 to calculate longitudinal sampling weights and rerun all models with weighted data. Earthquake survivors from the control group, younger people, those with lower education, fractures, TBI and lower pain scores in 2008 were significantly less likely to participate in the first follow-up assessment. Survivors from the control group and those with lower MBI scores in 2008 were less likely to participate in the second follow-up assessment.
Patient and public involvement
Since this was a secondary analysis of data from an evaluation of a government programme, patients were not involved in design, recruitment or analysis. On publication, a lay version of the results will be compiled in Chinese and distributed to earthquake survivors through the respective county-level health departments.
Results
Five hundred and ninety-one persons with disabling injuries comprising fractures, SCI, TBI, amputations as well as crush, peripheral nerve and soft tissue injuries were initially enrolled. Four-hundred completed all three assessments (67.7%). Figure 2 shows the assignment of participants to intervention groups and their flow through the study. Total follow-up time in this study was 1111.82 days on average (SD 281.21), 1202.38 in NHV-E (SD 275.28), 912.43 in NHV-L (SD 228.38) and 1081.87 in the control group (SD 233.81).

Flow of participants through the study.
Table 1 presents sample demographics and injury characteristics across intervention groups and compares drop-outs with complete cases. Most patients were female and diagnosed with fractures. At baseline, groups differed significantly in terms of injury characteristics and all demographics apart from gender. In all groups, patients with lower levels of education were more often lost to follow-up. Younger patients more frequently dropped from the early rehabilitation group (NHV-E), while males were more often lost to follow-up in the late rehabilitation group (NHV-L). Patients with fractures were more likely to drop from NHV-L and control group, and participants with TBI from the early rehabilitation group (NHV-E).
Unadjusted baseline (2009) scores for MBI (means, 95% CIs: NHV-E: 78.91, 76.9 to 80.92, NHV-L: 81.27, 77.96 to 84.59; control: 82.25, 79.35 to 85.15) and VAS pain (NHV-E: 3.95, 3.71 to 4.19; NHV-L: 3.95, 3.60 to 4.31; control: 3.87, 3.54 to 4.19) did not differ significantly across intervention groups. Baseline PCL-C scores (2010) were significantly higher in the control group (39.34, 37.59 to 41.09) than in both rehabilitation groups (NHV-E: 34.16, 32.96 to 35.37, NHV-L: 33.49, 31.57 to 35.40; F=12.14, p<0.01). Unadjusted MBI scores differed significantly across intervention groups at the first (NHV-E: 91.07, 89.88 to 92.26; NHV-L: 92.17, 90.36 to 94.00; control: 87.58, 84.46 to 90.72; F=4.6, p=0.01) but not at the second follow-up measurement (NHV-E: 94.61, 94.42 to 95.79; NHV-L: 95.70, 94.35 to 97.06, control: 93.08, 89.97 to 96.18). Unadjusted group differences were also not significant for VAS pain at both follow-up measurements (2010/11: NHV-E: 3.71, 3.44 to 3.96; NHV-L: 4.07, 3.71 to 4.42; control: 3.92, 3.60 to 4.24; 2012: NHV-E: 2.40, 2.16 to 2.62; NHV-L: 2.68, 2.33 to 3.03; control: 2.72, 2.41 to 3.03). Unadjusted PCL-C scores (NHV-E: 26.05, 24.87 to 27.23; NHV-L: 25.91, 24.24 to 27.58, control: 29.49, 27.82 to 31.15; F=5.05, p<0.01) were significantly higher in the control group at follow-up in 2012.
Primary outcomes: physical function and pain
Table 2 shows the parameter estimates from the models for MBI and VAS pain. Physical function showed significant intervention effects for both rehabilitation groups, while a rehabilitation effect on pain only was statistically significant for NHV-E. Baseline scores for physical function were lower in both rehabilitation groups than in the control group. Physical function further decreased with age and years of formal education. Patients with amputations and other injuries scored significantly lower than those with fractures. Reported pain scores increased with years of formal education. Patients with SCI reported significantly more pain, while those with amputations experienced less pain compared with patients with fractures.
Parameter estimates from mixed effects Tobit regressions for MBI and pain severity (VAS)
Figures 3 and 4 show the marginal trajectories of the development of MBI and VAS pain over time in each intervention group estimated from the above model. As expected, physical function improved first fast and then slower in the rehabilitation groups, whereas the initial increase was steeper in the late rehabilitation group. Conversely, physical function improved first slowly and then faster in the control group, possibly representing an effect of spontaneous recovery.

Estimated trajectories of physical function (Modified Barthel Index) across observation period adjusted for demographics and injury type. * indicates latent variable.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
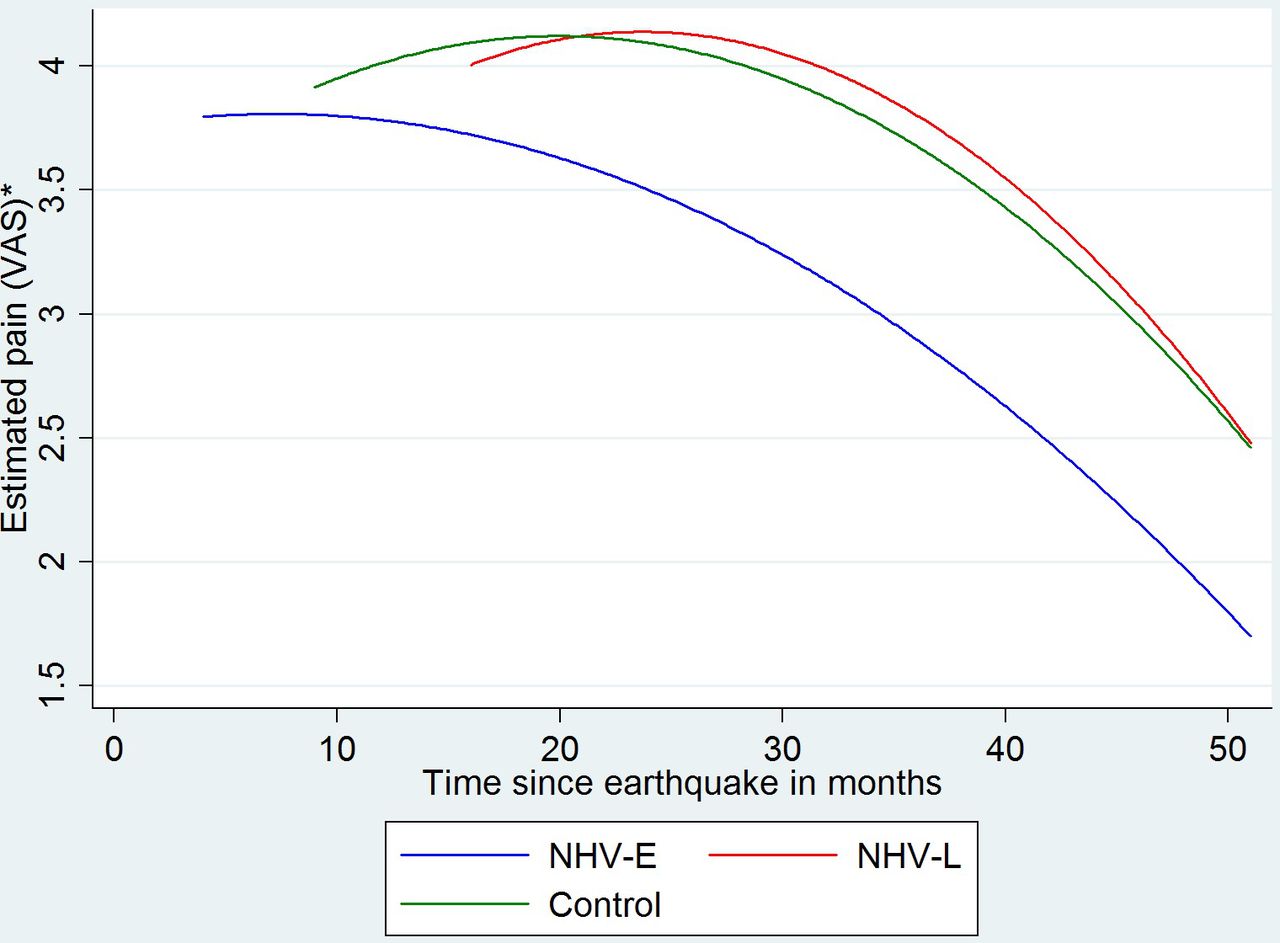
Estimated trajectories of pain severity (VAS) across observation period adjusted for demographics and injury type. VAS, Visual Analogue Scale.
A constant decrease of population-averaged pain severity is solely visible in the NHV-E group. In both other groups pain first increased and then decreased with a steeper decrease in the NHV-L group.
Secondary outcome: post-traumatic stress
Table 3 gives the parameter estimates from the model for PCL-C. Post-traumatic stress symptoms significantly decreased over time by half a point of the PCL-C score per months. While post-traumatic stress symptoms were lower in both rehabilitation groups in 2010, the decrease between 2010 and 2012 was largest in the control group. Patients with SCI showed higher levels of post-traumatic stress. The same applied to those with increased pain severity.
Parameter estimates from mixed effects regression for post-traumatic stress disorder symptom severity (PCL-C)
Sensitivity analysis
Results from the analysis with weighted data did not differ greatly from results with unweighted data with two exceptions. Amputation was no longer a significant predictor in the analysis of physical function that employed longitudinal sampling weights (p=0.072 vs 0.036) and NHV-L did not differ significantly from the control group at follow-up in weighted analysis of PCL-C (p=0.054 vs 0.018).
Discussion
We evaluated the long-term effectiveness of a comprehensive rehabilitation services programme for earthquake survivors with disabilities who were followed longitudinally over a 4-year period considering a range of outcomes. The study provided evidence for the long-term effectiveness of rehabilitation on physical function. The later implementation of the NHV programme was even more efficient in terms of a greater improvement over time. As some of the external rehabilitation volunteers who had been involved in the implementation of NHV-E were transferred to the late intervention setting and overall medical supervision and coordination of service delivery was the same, a learning effect is conceivable. Moreover, the training programmes for local health professionals had been updated based on previous experience. An alternative explanation is survival and selection bias. We cannot exclude that initial survivors with very severe injuries in the late setting had passed away after 1 year or were transferred to other care settings such as nursing homes or the academic level III hospital in Chengdu, the capital of Sichuan. Baseline scores of function and pain, however, did not differ significantly between early and late intervention setting. Moreover, while early rehabilitation was effective in pain reduction, a statistically significant effect of late rehabilitation was not found. Both rehabilitation groups also showed less post-traumatic stress symptoms, however, rehabilitation effects remain unclear due to the lack of a baseline assessment for this outcome.
Our results on physical functioning, that is, independence in activities of daily living, confirm findings from our previous study evaluating the effectiveness of the NHV programme in Wenchuan earthquake survivors over a 2-year period.8 Four years after the disaster, earthquake survivors who received institutional rehabilitation as well as community-based rehabilitation, continued to score higher than the control group, showing a sustained effect of the rehabilitation programme.
Early rehabilitation intervention with regard to pain management appears to be important since the late intervention group and the control group did not differ in this outcome. Linton et al 22 found, for instance, that early commencement of active treatment with physical therapy significantly decreased the likelihood of developing chronic pain. Early rehabilitation is also associated with reduced use of narcotics and invasive treatments for pain and reduced costs in patients with back pain and musculoskeletal conditions.23
The finding that PTSD symptom severity was significantly lower in the rehabilitation groups at both time points confirms results from a retrospective cohort study reported by Ni et al.24 The observed stronger reduction of the outcome over time in the control group could point to a similar effect of spontaneous recovery as observed for physical function. While it is likely that participation in one of the rehabilitation service programmes had a positive effect on PTSD-Symptoms, directly as well as indirectly through improved physical function and reduced pain, it cannot be excluded that the observed differences in PTSD symptom severity are due to baseline imbalance since baseline data are lacking.
This study has several limitations. First, the lack of baseline measurements of PTSD precludes the determination of initial rehabilitation effects (between 2008/2009 and 2010/2011) and non-linear time effects could not be studied for PCL-C since data from only two measurement points were available. Second, we provide a population-averaged estimation of rehabilitation effects. Effects may, however, differ across subgroups such as patients with different types of injuries. A study by Wen (2014), for instance, showed that no significant reduction of pain took place for patients with SCI over a 4-year period despite rehabilitative interventions. Third, details on types and locations of fractures, SCI, amputations, etc were not available to us from the data we were provided with for this secondary analysis. While one would expect different needs for rehabilitation services and outcomes depending on detailed type and location of injury, baseline scores in function and pain were similar across groups; imbalance between groups in this regard is thus unlikely to have influenced population-average outcomes. Fourth, although we performed sensitivity analysis, sample attrition remains a problem as we cannot exclude systematic patterns that are related to unobserved variables. Fifth, generalisability of our study to all earthquake victims with disabilities is limited by the fact that only patients with disabilities who presented at one of our partner hospitals could be included due to resource constraints and lack of pre-established protocols for drawing random samples from the whole affected population.
Future research should Include baseline measurements for all potentially relevant outcomes such as physical function, pain, mental health (post-traumatic stress, depression), participation and quality of life. Moreover, an assessment point at discharge from institutional rehabilitation is recommended to determine the effects of hospital versus community-based rehabilitation. The exposure to different rehabilitative therapies should be recorded to determine efficacy of measures used. Eventually, from an epidemiological standpoint, it is important to develop strategies for drawing random samples from the total affected population in order to determine point prevalence of disability and improve generalisability of findings regarding intervention effectiveness. Pre-established and ideally prefunded research protocols that can be activated when disaster strikes are thus desirable.25 26
In summary, physical rehabilitation of earthquake survivors appears to be effective in improving physical function and, if delivered early, pain. Effects on mental health remain unclear and need to be examined by future research. More consistent and more frequent assessments of relevant outcomes and determinants are recommended.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Provincial Ethics Committee at West China Hospital, Sichuan (K2018082). It was performed in accordance with the ethical principles of the Declaration of Helsinki and written informed consent was obtained from all participants. Informed consent procedures were repeated for each follow-up survey.
Acknowledgments
We would like to thank Dr Zhengen Zhao, Shaujun Zhang and all the rehabilitation volunteers for their great support during the data collection.
References
Footnotes
JR and XZ contributed equally.
Contributors JR wrote first draft, designed and performed the data analysis, and interpreted the data. XZ and JL designed the study, collected the data, interpreted the data and revised the draft for important intellectual content. MZ, SC and FK interpreted the data and revised the draft for important intellectual content. All authors read and approved the submitted version of the manuscript. JR responsible for the overall content as the guarantor.
Funding This project was funded by the Hong Kong Caring for Children Foundation (grant number not applicable) and Science and Technology Department of Shaanxi Province (grant number 2021SF-347, to JR, XZ).
Disclaimer The funders had no influence on design, data collection, data analysis, or data interpretation and conclusions of this study.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.