Article Text

Abstract
Objectives This study aimed to examine the association of high-sensitivity C reactive protein (hsCRP) with mortality risk and the attenuated effect of non-communicable disease history (NCDhistory) on the association.
Design Prospective cohort study.
Setting Health Examinees cohort.
Participants A total of 41 070 men and 81 011 women aged ≥40 years were involved (follow-up: 6.8 years).
Outcome measures Data and cause of death occurring until 31 December 2015 were confirmed by death statistics from the National Statistical Office. We conducted advanced analysis after stratification by NCDhistory and sensitivity analysis after excluding death before 1 or 2 years from recruitment. Cox proportional hazard and restricted cubic spline models were used to assess the association.
Results The association between serum hsCRP and risk of all-cause mortality was observed with strong linearity in both genders and was not influenced by NCDhistory. The association of serum hsCRP with risk of cancer mortality was not observed in women with NCDhistory, but the association with risk of cardiovascular disease (CVD) mortality was predominantly observed in men with NCDhistory.
Conclusions This study suggests a dose–response association of hsCRP with mortality risk, including cancer and CVD mortality, in Koreans with low serum hsCRP, although the association with cancer and CVD mortality risk could be influenced by gender and NCDhistory.
- preventive medicine
- epidemiology
- cardiac epidemiology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a large population-based prospective study.
We examined the effect of very high-sensitivity C reactive protein (hsCRP) concentration on mortality risk.
The hsCRP level in the present study was measured within 18 hours at a single institution to minimise error/bias.
Due to random fluctuations in hsCRP, using a single measurement of hsCRP at baseline could reflect inaccurate status of blood hsCRP level in study participants and increase the instability of hsCRP.
This study lacked information on medication use at recruitment and during the follow-up period, as well as information on hormone replacement therapy among women.
Introduction
High-sensitivity C reactive protein (hsCRP) is an acute-phase response protein synthesised by the liver and is the most sensitive and dynamic marker of inflammation.1 Since hsCRP has been reported as a candidate marker of generalised atherosclerosis and cardiovascular disease (CVD),2 many studies3–7 have investigated the role of hsCRP level as a predictor of mortality risk. A recent meta-analysis8 reported the predictive role of serum hsCRP in all-cause and CVD mortality in the general population. Nevertheless, it is controversial whether the predictive role of hsCRP could be applied to the risk of mortality in Asians, whose hsCRP levels are lower than those of individuals in Western countries.
Serum hsCRP represents a low-grade inflammation state that is generally involved in the process of ageing.9 Several large cohorts, including the Study of Women’s Health Across the Nation,10 the Women’s Health Study11 and the Dallas Heart Study,12 reported significant differences in hsCRP level by race and gender. In two studies of multiethnic populations residing in the USA,10 13 the median hsCRP level in East Asians was less than half the concentration in Caucasians. Even among East Asian populations, the geometric mean of hsCRP levels varied depending on ethnic background.14 In addition, a meta-analysis11 reported the hsCRP levels among women of various ethnic groups living in the USA (from the Women’s Health Study) and the association between hsCRP and risk of mortality; the association was observed only in men, supported by the results from two cohort studies15 16 reported in Korea. On the other hand, increased hsCRP may be influenced by comorbidity itself because inflammation has emerged as an important factor in the progression of non-communicable diseases (NCDs), including CVD,17 cancer,18 chronic obstructive pulmonary disease (COPD),19 type 2 diabetes20 and fractures,21 which contribute to increased morbidity and mortality.
This study aimed to examine the association of serum hsCRP with risk of mortality in Koreans with low serum hsCRP and to evaluate the attenuated effect of non-communicable disease history (NCDhistory) on the association.
Methods
Study population
Details on the main objectives, rationale, study design and baseline characteristics of the Health Examinees (HEXA) study have been published elsewhere.22 Considering the homogeneity and comparability of participants, we created a qualified data set called HEXA-G (Health Examinees-Gem) from previously published HEXA studies.23 In the new HEXA-G data, a total of 141 968 participants remained after exclusion of withdrawers (n=12). In addition, 19 887 were excluded due to missing information (n=19 876) or small sample size (n=11) on any hsCRP components at the baseline survey. Ultimately, 122 081 subjects, including 41 070 men and 81 011 women, remained in the final analysis (figure 1). All study participants provided informed consent prior to entering the study.

Flow diagram of the analytical sample in the current study using the HEXA cohort. HEXA, Health Examinees; hsCRP, high-sensitivity C reactive protein.
Laboratory measurements
After at least 10 hours of overnight fasting, blood samples were obtained in the morning. Biospecimens included fasting blood samples that were collected in a serum separator tube and two EDTA tubes. All samples were then transported within 18 hours to the National Biobank of Korea and stored for future research purposes. hsCRP was measured using a turbidimetric immunoassay (ADVIA 1650 and ADVIA 1800; Siemens Healthineers).
Follow-up and ascertainment of mortality
All-cause mortality was confirmed by death statistics from the National Statistical Office, which provided the data and causes of all deaths occurring through 31 December 2015. We added the mortality data from Statistics Korea to our data set using each participant’s unique identifier. Information on death and causes of death was obtained from a record link with the national death certificate files in Korea. The main outcome of interest was all-cause mortality (defined as death from any cause), including cancers and CVD mortality. The cause of death was classified according to the International Classification of Diseases, 10th Revision. Deaths were coded as C00-C97 for cancer and I00-I99 for CVD.
Baseline variables
Trained interviewers collected information on demographic, socioeconomic and lifestyle factors. Anthropometric measurements were obtained using standardised methods. Body mass index (BMI) was calculated and all participants were defined into four classes based on the WHO classification of BMI for Asian adults:24 underweight (BMI <18.5 kg/m2), normal (18.5 ≤ BMI <23.0 kg/m2), overweight (23.0 ≤ BMI <25.0 kg/m2), obesity (25.0 ≤ BMI <29.9 kg/m2) and severe obesity (BMI ≥30.0 kg/m2). The current study defined metabolic syndrome using the National Cholesterol Education Program Adult Treatment Panel III,25 modified for Asian guidelines on waist circumference (≥90 cm and ≥80 cm for men and women, respectively). Non-smokers were defined as those who had smoked less than 400 cigarettes over the course of their lifetime. Participants who had smoked were categorised into two groups: non-current (never/former) and current smoker. Non-current drinkers were defined as those who had never consumed an alcoholic drink over the course of their lifetime or those who had not consumed alcohol at recruitment, while current drinkers were defined as those who persisted in consuming alcohol. Regular exercise was classified into two groups (yes/no) as follows: ‘Do you currently engage in regular exercise strenuous enough to cause you to break into a sweat at least once per week?’ Furthermore, considering the attenuated effect of NCDhistory on the association between serum hsCRP and risk of mortality, we performed advanced analysis after stratification by NCDhistory. We considered six main NCDs (hypertension, diabetes, hyperlipidaemia, cancer, cardiovascular and cerebrovascular diseases, and respiratory disease) to classify healthy subjects versus subjects with NCDhistory.
Statistical analysis
For the categorical analysis, we created nine categories based on the distribution of hsCRP levels in our population: ≤1.00 (reference group), 1.01–1.50, 1.51–2.00, 2.01–2.50, 2.51–3.00, 3.01–4.00, 4.01–6.00, 6.01–10.0 and >10.0 mg/L. For the advanced analysis after stratification by NCDhistory, the hsCRP levels were categorised into ≤1.00, 1.01–2.00, 2.01–3.00, 3.01–10.0 and >10.0 mg/L due to the reduced sample size in each subgroup. The concentrations of hsCRP were log-transformed for analyses due to the skewed distribution.
We calculated a follow-up time for each subject starting from the date of interview until the date of death or 31 December 2015, whichever came first. Using age as the time scale, subjects entered the risk set at the age at which they completed the baseline questionnaire and exited at their event/censoring age. The associations of hsCRP and all-cause mortality, as well as cancer and CVD mortality, were analysed by Cox proportional hazard models (adjusted HR (aHR)) and included adjustment for age, gender, demographic factors (education, marital status, job, BMI and NCDhistory) and lifestyle factors (smoking, alcohol consumption and exercise). We used Wald test to test for heterogeneity of risk between serum hsCRP level groups. The proportional hazards assumption was assessed on the basis of Schoenfeld residuals and was not violated for the variables of interest in the adjusted model for either cancer mortality or CVD mortality (p>0.05 for all categories). In addition, we conducted a sensitivity analysis to avoid latent period bias after excluding death before 1 year (aHR1year) or 2 years (aHR2years) since recruitment. Based on the Cox proportional hazard models, we made Kaplan-Meier curves and log-rank analysis after adjustment for age, gender, demographic factors (education, marital status, job, BMI and NCDhistory) and lifestyle factors (smoking, alcohol consumption and exercise). We employed restricted cubic splines (RCS) to evaluate the possibility of complex (ie, non-linear) hazard functions26 using continuous values of hsCRP (aHRcontinuous). We selected five hsCRP concentration values as knots based on hsCRP concentration percentiles, tested the linear and non-linear associations between knots using a cubic function, and presented the integrated graph smoothly. All statistical analyses were performed using SAS V.9.3 and RCS analysis was carried out using the SAS LGTPHCURV9 macro. Two-sided p values <0.05 were defined as indicating statistical significance.
Patient and public involvement
No patients and public were involved in the design, conduct, reporting and dissemination plans of the present study.
Results
The association of demographic and lifestyle factors with risk of all-cause mortality is presented in table 1. During the follow-up period (average 6.8 years), 1365 men and 864 women died. The median levels of hsCRP were 0.77 mg/L and 0.59 mg/L for men and women, respectively. The risk of all-cause mortality was inversely associated with female gender (aHR=0.38), high education (aHR=0.65), overweight (aHR=0.81) or obesity (aHR=0.83), current alcohol consumption (aHR=0.81) and regular exercise (aHR=0.83), but was positively associated with a single marital status (aHR=1.23), NCDhistory (aHR=1.57), underweight (aHR=2.05) and current smoking (aHR=1.97).
Baseline characteristics of participants by all-cause mortality
The risk of all-cause mortality increased in a dose-dependent pattern with serum hsCRP level (ptrend <0.001; online supplemental material 1), regardless of gender (ptrend <0.001 in both genders), even in the sensitivity analysis (ptrend <0.001 for aHR1year in both genders). The increased risk of female mortality with increased hsCRP level was observed in both premenopausal (ptrend=0.020) and postmenopausal (ptrend <0.001) women, although the statistical significance in premenopausal women disappeared after sensitivity analysis (ptrend=0.150 for aHR2years; online supplemental material 1). The integrated graph, based on the RCS analyses, indicated a strong and linear association of serum hsCRP level with all-cause mortality in both genders (aHRcontinuous=1.019 and 1.013 in men and women, respectively; figure 2A).
Supplemental material

Dose–response association between serum hsCRP level and risk of all-cause mortality in all (A), healthy subjects at recruitment (B) and subjects with non-communicable disease history at recruitment (C). aHR, adjusted hazard ratio (adjusted for age, gender, education, job, marital status, BMI, NCDhistory, smoking, alcohol consumption and exercise) BMI, body mass index; E, number of death; hsCRP, high-sensitivity C reactive protein; MR, mortality rate; PY, person-year.
The dose–response association between hsCRP level and risk of all-cause mortality was not influenced by NCDhistory (online supplemental material 2). After stratification by gender, however, the attenuated effect by NCDhistory on the association was observed only in women; the linearity of the relationship was observed in healthy women (ptrend=0.001 for aHR2years) but disappeared in women with NCDhistory, particularly after sensitivity analysis with exclusion of a 2-year follow-up time (ptrend=0.084 for aHR2years). Based on the RCS analyses, the pattern of increase in the association was different depending on NCDhistory (figure 2B,C). In healthy subjects, the risk of all-cause mortality increased with a gradual slope (strength) until 3.0 mg/L hsCRP, with a very steep slope until 4.5 mg/L and finally with a reduced and flattened slope after 4.5 mg/L (figure 2B). On the other hand, the slope of the association fluctuated as the hsCRP level increased in subjects with NCDhistory; the slope increased up to 3.0 mg/L hsCRP but decreased until 4.5 mg/L and rapidly increased after 4.5 mg/L (figure 2C).
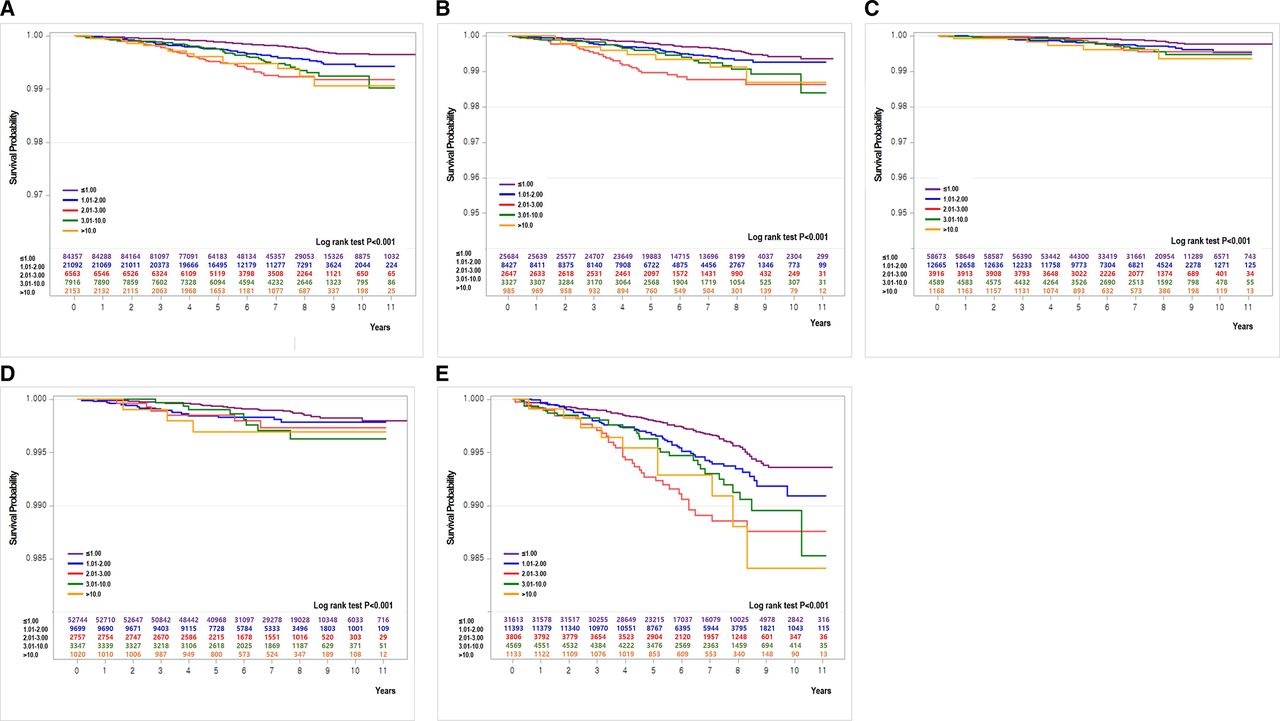
The association of serum hsCRP with risk of cancer mortality was not influenced by NCDhistory (ptrend <0.001 regardless of NCDhistory) (table 2 and figure 3A–E). After stratification by gender, the association was not observed in women with NCDhistory (ptrend=0.856); however, the association was not influenced by NCDhistory in men (ptrend <0.001 and ptrend=0.002 for aHR in both healthy and NCDhistory) (table 2). Although the risk of CVD mortality was linearly associated with increasing hsCRP levels, the association was dominant in men (ptrend=0.002) and in subjects with NCDhistory (ptrend=0.001; table 3) after stratification by gender and NCDhistory, respectively (figure 4A–E). After stratification by gender and NCDhistory, the association only appeared in individuals of both genders with NCDhistory (ptrend=0.015 and ptrend=0.035 in men and women with NCDhistory, respectively); no association between hsCRP level and CVD mortality risk was found in either healthy men or women.
Association between serum hsCRP level and cancer mortality by gender and NCDhistory at recruitment

Kaplan-Meier crude survival curves for cancer mortality according to serum hsCRP level in all (A), men (B), women (C), healthy subjects at recruitment (D) and subjects with non-communicable disease history at recruitment (E). hsCRP, high-sensitivity C reactive protein.
Association between serum hsCRP level and cardiovascular disease mortality by gender and NCDhistory at recruitment
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier crude survival curves for cardiovascular disease mortality according to serum hsCRP level in all (A), men (B), women (C), healthy subjects at recruitment (D) and subjects with non-communicable disease history at recruitment (E). hsCRP, high-sensitivity C reactive protein.
Discussion
This study suggests that the risk of all-cause mortality was associated with elevated hsCRP levels in a dose–response manner in both genders among Asians who have reported low hsCRP levels compared with other races and was not influenced by NCDhistory. The association was influenced by gender and NCDhistory, although a dose–response association of hsCRP with risk of cancer and CVD mortality was also observed in this population. The level of hsCRP was not associated with risk of cancer mortality among women with NCDhistory. The risk effect of high hsCRP level on CVD mortality was predominantly observed in men with NCDhistory.
Several large cohorts10–12 14 have suggested that serum hsCRP levels may differ according to ethnic background, with the highest concentrations seen in African Americans, followed by Hispanic, white, Chinese and Japanese individuals. Although the reason for this ethnic difference is not clearly resolved, genetic diversity,27 the relatively low BMI in Asian populations, and ethnic differences in diet and lifestyle28 have been suggested. Although the extent to which these findings adopt to Asian populations has been unclear, several recent studies11 16 conducted in Asia reported a positive association of hsCRP with mortality risk. In this population, the hsCRP level was associated with risk of all-cause mortality in a dose-dependent manner, even though the level of hsCRP was lower than in the Western population. A meta-analysis29 and large cohort studies3–6 supported the robustness of the association regardless of adjusted confounders, the cut-off point of CRP level and exclusion of deaths within the first 2 years of follow-up.
The reason for the discrepancy in hsCRP levels with respect to gender is not clearly resolved, although several studies suggested different lifestyle and metabolic risk factors between men and women30 and genetic diversity.27 A high level of serum hsCRP in our population was positively related to the increased risk of all-cause mortality in both genders, supported by several previous studies.8 16 31 Nevertheless, several studies reported no association of hsCRP level with all-cause mortality was observed in women.7 16 In particular, the association was shown in postmenopausal women only, which might suggest the protective effect of endogenous female hormones on the low level of hsCRP;32 the average hsCRP level was 0.48 mg/L and 0.68 mg/L for premenopausal and postmenopausal women in this study. The protective effect could be supported by the proposition that oestrogen or progesterone might to some extent repress the detrimental effects of chronic inflammation on tissue damage.33
Inflammation has emerged as an important factor in the processes of NCD, including CVD,17 cancer,18 type 2 diabetes,20 COPD19 34 and fracture.21 In addition, medications that had taken to treat any specific NCD, such as renin–angiotensin system inhibitors35 and statins and thiazolidinedione,36 could influence the level of hsCRP. The association between hsCRP and mortality risk was not attenuated by NCDhistory in either gender in this study, but the statistical significance of the association disappeared in women after sensitivity analysis (aHR2years). A dose–response relationship between hsCRP level and all-cause mortality risk was pronounced in both genders. On the other hand, the positive association of hsCRP with risk of all-cause mortality was significantly observed only in men with NCDhistory but not in women with NCDhistory. The attenuated effect of NCDhistory on the association between hsCRP and risk of cancer mortality was not observed in men, consistent with results from several studies which reported an association among healthy men3 or patients with cancer37 38 only. Most studies3 4 6 7 15 16 31 39 supported that CVD mortality increased with elevated hsCRP levels, predominantly in men.4 7 15 16 Although hsCRP levels are lower in our population than in other races, the level of hsCRP was positively associated with CVD mortality in men but not in women, similar to previous studies.7 15 16 31 39 After stratification by gender and NCDhistory, the association between hsCRP and risk of CVD mortality was dominant in subjects with NCDhistory in this study. Although many interventional studies have been conducted recently on anti-inflammatory drugs for prevention of CVD, the results are controversial. According to the results of our study, elevated inflammatory markers in people with chronic disease were associated with an increased risk of CVD mortality. This suggests that CVD mortality in people with chronic diseases might be reduced by use of anti-inflammatory medication.
This study has several strengths. As a large population-based prospective study, it was possible to (1) adjust for confounders; (2) perform a sensitivity analysis after excluding death before 1 or 2 years from recruitment; (3) assess an advanced analysis after stratification by gender and NCDhistory; (4) examine the association using various cut-off points of hsCRP considering low serum hsCRP levels in Asian populations; and (5) evaluate the complex (ie, non-linear) hazard functions using RCS on the association between continuous hsCRP levels and risk of mortality. In particular, most previous studies excluded subjects with more than 10 mg/L hsCRP due to their relatively low sample size or reflecting acute-phase reactions of severe inflammation, but we examined the effect of very high hsCRP concentration on the risk of mortality because it is possible that studies focusing on patient with hsCRP of 10 or higher could be conducted. In addition, the hsCRP level in this study was measured within 18 hours at a single institution to minimise measurement error/bias from institutional variations and to avoid bias from measurement or long-term storage before analysis.
Despite these strengths, the study also has several limitations. First, the use of a single measurement of hsCRP at baseline could reflect an inaccurate status of blood hsCRP levels in study participants and increase the instability of hsCRP due to random fluctuations over time. Nevertheless, a report40 on long-term hsCRP variability suggested that hsCRP variability within an individual is relatively small and that the variability could not account for the association. Second, our study lacked information on medication use at recruitment and during the follow-up period. Several medications related to NCDs, including statins, ACE inhibitors, fibrates, niacin, thiazolidinedione and oestrogen/progestogen hormone, could influence hsCRP level;37 however, we tried to overcome this limitation through advanced analysis after stratification by NCDhistory. Third, because there is no available information on hormone replacement therapy (HRT) among women and we could not examine the influence of HRT on the association of hsCRP with risk of hormone-related cancer or CVD mortality among women, we could not suggest the effect of female hormones on the association. In addition, further studies are needed on the effects of obesity, although the inverse relationship between all-cause mortality and obesity in our population was consistent with Zheng et al’s report in Asians.41 On the other hand, the inverse association of alcohol drinking with all-cause mortality could not be interpreted directly because we were not able to distinguish between mild drinkers and abusive alcohol drinkers and thus requires additional research in the future.
In conclusion, the association of hsCRP level is dose-responsively increased with the risk of all-cause mortality in men and women (particularly postmenopausal women). Otherwise, the association of hsCRP level with risk of cancer and CVD mortality could be attenuated by gender or NCDhistory.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Review Board of the Seoul National University Hospital, Seoul, Korea (IRB no: E-1503-103-657). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors S-AL, X-OS and DK designed and conducted the research. S-AL and SOK analysed the data and performed the statistical analyses. HP and J-KL managed the data mining and collection. S-AL wrote the manuscript and approved the final version of the submitted manuscript, also is responsible for the overall content as guarantor. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.