Article Text

Abstract
Objective Diabetes poses serious health threats and economic burdens to patients, especially in low-income and middle-income countries (LMICs). This systematic review searches for non-pharmacological interventions for the prevention of type-2 diabetes mellitus (T2DM) among patients who are non-diabetic and pre-diabetic from LMICs.
Settings LMICs.
Participants Adult population aged over 18 years without having diabetes.
Primary and secondary outcomes Primary outcome is to measure the change in the incidence of T2DM. The secondary outcome is to measure changes in glycated haemoglobin (HbA1c) level, weight/body mass index (BMI), fasting glucose level and 2-hour glucose from baseline of the included randomised controlled trials.
Methods This review has been conducted following the standard systematic review guidelines. A total of six electronic databases including MEDLINE, Embase, the Cochrane Library, Web of Science, ClinicalTrials.gov and International Clinical Trials Registry Platform were searched in February 2021 using a comprehensive search strategy.
Two sets of independent reviewers performed screening, risk of bias (ROB) assessment using the Cochrane ROB tool and data extraction. Narrative coalescence of selected articles was demonstrated using tables. No meta-analysis was performed due to the lack of homogenous intervention strategies and study settings.
Result A total of five studies were included for the review with a combined population of 1734 from three countries. Three of the studies showed a significant reduction in T2DM incidence after the intervention of physical training and dietary modifications. Four of the studies also demonstrated a significant reduction of different secondary outcomes like weight, BMI, fasting and 2-hour plasma glucose and HbA1c. All the studies demonstrated a low ROB in most of the bias assessment domains with some unclear results in allocation concealments.
Conclusions Emphasising non-pharmacological interventions for T2DM prevention can improve health outcomes and lessen the economic burdens, which will be of paramount importance in LMICs.
Systematic review registration number CRD42020191507
- general diabetes
- preventive medicine
- public health
- epidemiology
Data availability statement
Data are available upon reasonable request. The data sets generated and/or analysed during this review shall be available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The methodological rigour following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines is the major strength of this systematic review.
The prime strength of this systematic review is the inclusion of randomised controlled trials only, which helped to ensure the true effectiveness of the intervention programmes.
We included articles published in English only which might have missed some potential articles published in other languages.
Trials conducted only in India, Iran and China fulfilled the selection criteria and were included in the review. Therefore, the interpretation might not be socially and culturally applicable to other low-income and middle-income countries.
A meta-analysis could not be conducted due to the heterogeneity of the included articles.
Introduction
Diabetes mellitus is a group of metabolic disorders marked by excessive serum glucose levels caused by insufficient insulin secretion, insulin action or both. Type 2 diabetes mellitus (T2DM) is the most prevalent form of diabetes, which accounts for 90%–95% of all diabetes cases. It occurs when insulin secretion is insufficient to overcome an underlying abnormality of increased insulin resistance.1
Diabetes is linked to a number of adverse health outcomes. It increases the risk of cardiovascular disease and stroke significantly. In reality, most patients with diabetes die of cardiovascular complications. In 2017, diabetes has risen to the 10th spot on the Institute for Health Metrics and Evaluation global cause of death list,2 but it directly or indirectly contributes to the other top causes of death like coronary heart disease and stroke. Diabetic microvascular complications are the major cause of blindness, renal failure and non-traumatic amputations.
T2DM incidence has seen a rapid global increase during the past few decades. Diabetes prevalence in the world among adults over the age of 18 increased to 8.5% in 2014 from 4.7% in 1980.3 Diabetes affects more than 420 million individuals globally today. By 2030, this number is expected to reach 570 million, and by 2045, 700 million.4 The burden of diabetes in terms of prevalence, incidence, disability-adjusted life years and death is predicted to continue to rise from 2018 to 2025.5 The economic burden of diabetes is monumental but is usually largely overlooked. For instance, in 2019, direct and indirect medical and treatment expenses, as well as expenditures associated with diabetes-related disability and mortality exceeded US$760 billion which is around 10% of total health expenditure on adults.6 7 This trend of economic burden is predicted to continue its upward trend.8 Because diabetes has no cure, it is essential to focus on primary prevention via food and lifestyle changes.1
Uncontrolled T2DM can lead to blindness, renal failure, heart disease and other severe complications. There is a period before diabetes that is diagnosed in which blood glucose levels are elevated but not elevated enough to be labelled as diabetes. Pre-diabetes is the medical term for this condition.9 It is estimated that 1 in every 13 adults aged 20–79 years has impaired glucose tolerance which amounts to 463 million people.6 According to estimates, up to 70% of those with pre-diabetes progress to develop T2DM. Fortunately, advancing from pre-diabetes to diabetes is not a foregone conclusion.10 The preventability of diabetes has been demonstrated by several randomised trials (RCTs).
Early management in the pre-diabetes stage is beneficial to decrease diabetes development and related consequences since T2DM is a chronic illness with progressive impairment in glucose metabolism resulting in various systemic complications. Strong epidemiological evidence indicates that diabetes is associated with lifestyle. The non-randomised Malmö study indicated that a lifestyle programme for the prevention of T2DM in persons with impaired glucose tolerance is feasible.11 Previously, randomised intervention studies showed that changes in diet and physical activity can delay or even prevent the onset of T2DM in persons with impaired glucose tolerance.12–15 Studies in high-risk groups other than persons with impaired glucose tolerance have also been conducted. A Norwegian lifestyle intervention indicated a beneficial impact of diet and exercise on insulin sensitivity in people with several cardiovascular risk factors.16
A systematic literature review conducted in 2010 evaluated four cohort studies and found that the incidence of T2DM can be reduced by 28%–59% by lifestyle changes.17 A meta-analysis backs up this claim, estimating that to prevent or delay each case of diabetes, 6.4 (95% CI, 5.0 to 8.4) people would need to be treated through lifestyle intervention. Weight loss diets (low fat, high protein or the Mediterranean) appear to be helpful, but every one of them has drawbacks that necessitate careful food selection. Evidence also indicates that a weight reduction maintenance strategy demands frequent exercise.17
More than three-quarters of the people suffering from diabetes are from low-income and middle-income countries (LMICs), and diabetes prevalence is expected to rise fastest in these countries.18 Diabetes prevalence estimates in LMICs have largely relied on self-reporting, which might have vastly understated the true prevalence of T2DM in countries lacking robust screening protocols and access to care.19 However, In LMICs, there has been relatively little effort to adopt preventive programmes and delivery approaches for T2DM.20 Evidently, no such programmes from these regions were found in a relatively fresh systematic review of 38 real-world diabetes preventive trials.21 Given the significant differences in health systems, resources, culture and lifestyle risk factors among LMICs, this creates a significant evidence gap. To reiterate the fact, context-specific evidence is necessary and recommended, because the burden of diabetes will proportionately decrease with the narrowing of the evidence-to-action gap. It will also lead to lowering of death rates as well as lower healthcare expenditures.22–24 This systematic review seeks to evaluate the effectiveness of the non-pharmacological programmes for the prevention of T2DM conducted in LMICs to address that knowledge gap.
Methods
This systematic review was conducted using the Cochrane systematic review norms25 and PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) recommendations.25 26 The systematic review is registered in the International Prospective Register of Systematic Reviews. The protocol outlines the approach in depth, including the development of the search strategy, double-screening, double-data extraction, double-quality assessment of included articles and narrative synthesis.27 A detailed search strategy (online supplemental table 1) was constructed using the keywords including Exercise, ‘Physical activity’, ‘Nutritional therapy’’, ‘Meal plan’, ‘Weight loss’, ‘Lifestyle change’, ‘Lifestyle modification’, Diabetes, ‘Diabetes mellitus’, ‘Type 2 diabetes mellitus’’, T2DM, DM, LMICs, ‘Developing country’, ‘Peri-urban’’, urban, rural to search different electronic bibliographic database including MEDLINE through PubMed, Embase, the Cochrane Library (Cochrane Central Register of Controlled Trials-CENTRAL), Web of Science, ClinicalTrials.gov, International Clinical Trials Registry Platform, etc. The search period covered from the inception of the databases to February 2021. Non-pharmacological interventions on non-diabetic adult populations in LMICs were included in RCTs. Two reviewers independently screened the ‘title and abstract’ and ‘full text’ of the retrieved articles, and any disagreements were resolved by a third reviewer. To keep track of the screening process, reference management software ‘Rayyan’ was used. Each study was evaluated critically for the possibility of risk of bias (ROB). A narrative synthesis of study participant characteristics and intervention categories with specific primary and secondary outcomes was demonstrated. The risk ratio (RR) of diabetes mellitus (DM) status was recorded from baseline and end line information. Mean and SD of secondary outcomes (change in weight, body mass index (BMI) and fasting blood glucose level) were recorded from both the control and intervention groups.
Supplemental material
In terms of interventions, study duration and study settings, the included studies were too heterogeneous to be included in the meta-analysis. A narrative synthesis was performed as a substitute for a meta-analysis. We were not able to conduct a subgroup analysis or a sensitivity analysis for the same reason. In this systematic review, we did not observe the publication bias because we were not able to perform the meta-analysis. Funnel plots are generally used to estimate the risk of publication bias. It is also recommended in different studies to avoid a test of funnel plot asymmetry or the existence of publication bias if the number of selected studies is less than 10 in a meta-analysis.28
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
A thorough search of the literature in the selected databases using the search strategy resulted in the retrieval of 2737 articles. A total of 2592 articles were finally listed for the title and abstract screening after removing 145 duplicates. A total of 25 articles were selected following employing the inclusion and exclusion criteria for the full-text review.
We were unable to find the full text of only one article, even after communicating with the authors. The article was published in 1984, and we excluded it from our full-text review due to unavailability. The Da Qing impaired glucose tolerance (IGT) and diabetes study12 fulfilled all the inclusion criteria, but we decided to leave the article out of our review since it used the 1985 WHO criteria to define patients with IGT and diabetes. The criteria were updated in 1999. Currently, WHO,29 American Diabetes Association (ADA)30 and Diabetes UK31—all use the same diagnostic criteria, and all our included studies follow this guideline for the diagnosis of diabetes and IGT. As a result, the interpretations from the Da Qing study could be potentially misleading when compared with the other selected recent studies.32 Finally, after the full-text review, five articles were included for analysis. Figure 1 shows the PRISMA flow diagram of the inclusion process. Online supplemental table 2 is provided containing the list of 20 articles that did not fulfil inclusion criteria and were eventually excluded, along with the reasons for exclusion.
Supplemental material

Systematic review Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. *Causes of exclusion: not in low-income and middle-income countries = 15; not focusing on prevention of diabetes mellitus = 1; intervention provided on women with gestational diabetes mellitus = 1; not on adult = 1 pharmacological intervention = 1; used older (WHO) criteria to define patients with impaired glucose tolerance and diabetes = 1.
Five articles from three geographical regions with a combined sample of 1734 were included for final analysis. The basic characteristics of these selected articles are given in table 1. All the studies were recent publications, dating from 2015 to 2020. India and China both were the sites of two studies each. The rest was conducted in Iran. Two of the five studies were RCTs, two were parallel RCTs and the rest was cluster RCT. The period of the intervention varied from 6 months to 36 months. Participants’ age in the selected studies ranged from more than 20 years to 75 years. All of the studies had both male and female participants. The five studies used completely different intervention methods, such as peer-support lifestyle intervention,33 aerobic and resistant physical training,34 Fenugreek powder,35 high-monounsaturated fat diet36 and mobile-based intervention and behavioural theory.37 Online supplemental table 3 details the selection criteria and interventions used in each of the included articles. All the studies depicted the efficiency of the intervention in terms of the prevention of T2DM. Four of them used participants’ diabetes status as the primary outcome. One study used changes in dietary behaviours and physical activity as the main outcome. The primary outcome, diabetes status, was measured by oral glucose tolerance test (OGTT) following the ADA criteria in three studies.33–35 One study used fasting glucose level or 2-hour post-glucose challenge following the ADA criteria.36
Supplemental material
Attributes of studies included
Table 2 shows the summary findings of the primary outcome and tables 3 and 4 demonstrate the secondary outcomes of the included studies. Kavumpurathu and the team evaluated the impact of peer-support lifestyle intervention to reduce the incidence of T2DM. After 12 months of intervention, the incidence of T2DM was 14.9% and 17.1% in the intervention and the control group, respectively (relative risk: 0.88, 95% CI, 0.66 to 1.16, p=0.36) (table 2). The secondary outcomes also showed improvement in the intervention groups, but it was not found to be statistically significant. Xia Dai et al examined the effect of physical training on T2DM. The intervention group had three arms, resistance training (RT), aerobic training (AT) and a combination of both (RT+AT). After 24 months of intervention, all the intervention arms showed lower cumulative incidence than the control group (22%, 26%, 21% and 69% for the aerobic, resistance, combined and control groups, correspondingly). The age and sex-adjusted Hazard Ratios (HRs) were 0.26 (95% CI, 0.11 to 0.62) in the combined group, 0.35 (95% CI, 0.15 to 0.79) in the resistance group, and 0.28 (95% CI, 0.13 to 0.64) in the aerobic group. Among the secondary outcomes, the intervention arms showed a significant reduction in 2-hour plasma glucose level, glycated haemoglobin (HbA1c) level (table 3) and weight (table 4) than the control group. The trial conducted by Arpana Gaddam et al determined the effect of Fenugreek to avert the development of T2DM in people who are pre-diabetic. After following the intervention and the control group for 36 months, the incidence of T2DM was found to be 18.8% and 55.7%, respectively. Relative risk reduction was 0.6 (p<0.01). There was also a significant reduction in fasting and 2-hour plasma glucose levels.
Summary findings of primary/main outcome of the selected studies
Summary findings of secondary outcomes of the included studies (fasting glucose, 2 hours after plasma glucose, HbA1c)
Summary findings of secondary outcomes of the included studies (weight, BMI)
Shahbazi et al explored the outcomes of a fat diet without a weight-loss programme on preventing or delaying the onset of T2DM in subjects with either impaired fasting glucose or impaired glucose tolerance. The intervention group had two arms, a high-monounsaturated fat diet (HMD) and a normal fat diet (NFD). After 24 months of intervention, the incidence of T2DM was 9.4%, 13.2% and 18.4% in HMD, NFD and control groups, respectively.
Relative risk in HMD arm was 0.43 (95% CI, 0.1 to 0.9; p=0.03), and in the NFD arm was 0.60; (95% CI, 0.2 to 1.2; p=0.1). HMD and NFD arms were also shown to be effective in reducing the fasting and 2-hour plasma glucose level significantly. Zidu Xu et al tested a mobile-based intervention plus behavioural therapy to affect dietary behaviours and physical activity among the population at high risk of T2DM. The control group received the same intervention through printed material. After 6 months of intervention, the intervention group showed higher reduction of BMI (3 months—24.1 (23.5–25.2), 6 months—23.2 (22.7–24.3)) than the control group (3 months—24.1 (23.3–25.6), 6 months—24.2 (22.8–25.6)) when compared with 3-month intervention data.
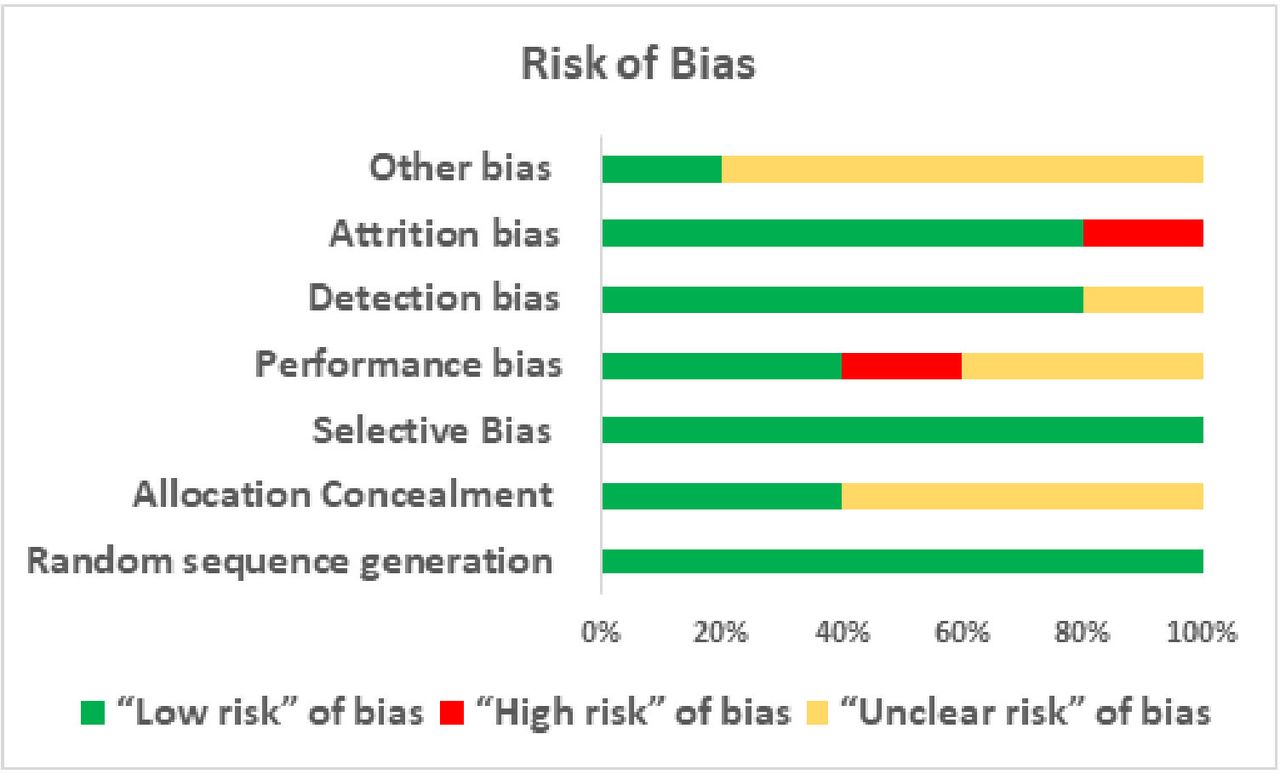
The quality of the included RCTs was assessed by applying the Cochrane ROB tool. Two authors assessed the studies independently and then cross-checked the result among themselves. They warranted the judgement of the senior author to resolve some disagreement and finally came up with a combined result with consensus. Figure 2 provides a graphical demonstration of the ROB in the studies.

{kind=link}
{kind=link}
Risk of bias assessment of included studies.
Random sequence generation of all included studies presents a low ROB. Four studies33–35 37 used a randomisation list generated by a computerised programme whereas one study36 used block randomisation to minimise the selection bias. Allocation of the included studies was concealed in two studies34 35 through assigning a unique code and in opaque and numbered envelopes. Thus, it presents a low ROB for 40% of the studies whereas 60% of studies33 36 37 represent an unclear ROB in this section. All the included studies reported their primary and secondary outcome according to their objective through which low ROB was reported against selective bias. One of the studies was triple blinded study33 whereas because of the characteristics of the study, respondents were not required to be blinded in another study.37 Two studies did not mention anything about performance bias.34 36 However, the study conducted by Gaddam et al35 portrayed a high ROB. Detection bias was assessed as low in four studies and unclear in one which was the opposite during assessing other biases (low in one study and unclear among four). Four studies (80%) mentioned the data related to attrition or loss to follow-up. Thus, they were assessed as a low ROB. However, one study (20%)34 was assessed as a high ROB as it conducted a per-protocol analysis having a high attrition rate. Figure 2 graphically demonstrates the ROB domains with corresponding assessment.
Discussions
The goal of this systematic review is to assess the effectiveness of non-pharmacological interventions in lowering the prevalence of T2DM in LMICs. For this purpose, we undertook a comprehensive search strategy to screen 2737 articles to finally select five RCTs with a total population size of 1734, spanning over the last 6 years, and conducted in three countries. The lack of older studies highlights the fact that non-pharmacological diabetes prevention strategies are a relatively new concept but are gaining attention lately. These trials assessed different intervention strategies like lifestyle intervention, physical training and dietary intervention on normal or patients with pre-diabetes. As there was no more than one study that used the same intervention strategy, no meta-analysis could be performed.
Our primary outcome was the incidence of T2DM, which was measured in the studies by assessing the OGTT or fasting glucose level and 2-hour glucose challenge according to the ADA30 or WHO29 criteria at baseline and end-line evaluation. Among the secondary outcomes, we measured weight, BMI, fasting and 2-hour glucose level and HbA1c level to assess the effectiveness of the intervention programmes.
Two studies used lifestyle intervention to reduce diabetes incidence. One used peer support, and the other study used a mobile-based application to deliver the intervention. Studies showed that lifestyle intervention lessons can lessen the probability of a person becoming diabetic.38 The peer-support study used sittings organised by professionals and then by non-professional peer leaders to deliver the lifestyle intervention knowledge among the participants. The control group received only informational booklets. The mobile-based intervention study used mobile-application-based push notifications to deliver messages on improving dietary behaviours, physical activity and so on. The first study found a decrease in diabetes incidence after the intervention period. But the result was not statistically significant. The second study used a different primary outcome, but among the secondary outcomes, it found a significant decrease in BMI between two points of the intervention.
The efficacy of dietary modification or intervention was measured in two studies. One used Fenugreek powder for its hypothesised effect on glucose homeostasis,39–43 and the other study used an HMD and NFD regimen to elucidate the effect of dietary modification. The ADA recommends that having the right amount of monounsaturated fat in the diet helps prevent T2DM.44 The first study administered 5 g debittered, defatted Fenugreek powder with 200 mL water before meal two times a day for 3 years and found a significant decrease in relative risk for T2DM in the intervention group. They also observed a significant reduction in fasting and 2-hour plasma sugar level in the intervention group. The second study contrasted an HMD and NFD group with the control group. The control group followed the US Department of Agriculture Food Pyramid Guide for diet. The use of a food-based US guideline in LMICs is surprising, but the study offered no explanation for this. After the intervention, the HMD section saw the most significant decrease in the incidence of diabetes compared with the NFD and non-intervention groups. The cumulative incidence also showed a marked reduction in the HMD arm.
Only one study evaluating the efficacy of supervised physical training to reduce the risk of T2DM was included in the review. This study had three intervention arms, RT, AT and both RT and AT. The control group was encouraged to follow normal daily activities. After 2 years of intervention, it demonstrated a higher cumulative incidence in the control group than in the intervention group with a significant HR. Among the arms, the combined physical training arm showed greater efficacy in diabetes risk reduction, followed by the AT arm. Both the studies using Fenugreek and exercise as interventions34 35 were conducted among pre-diabetic participants and reported cumulative incidence of diabetes after the intervention period. This resulted in a much higher proportion of controls ending up as diabetic (69% and 55.74%, respectively) which, however, was consistent with previous findings.45 A joint position statement from the American College of Sports Medicine and the ADA demonstrated the effectiveness of physical activity and physical training, especially the combination of both AT and RT.46
Although we left the Da Qing study out of the scope of this review, the findings from this large, randomised trial are worth mentioning nonetheless. This study recruited 577 IGT respondents, 530 of them completed the 6-year follow-up.12 The subjects were divided into one control and three active treatment groups (diet, exercise, diet +exercise). The cumulative incidence of diabetes was again higher in the control group (67.7%) compared with the intervention groups (43.8%, 41.1% and 46.0%, respectively, in the diet, exercise and diet-plus-exercise group), and showed 31%, 46% and 42% decreases in the risk of developing diabetes, respectively, in a proportional hazards analysis adjusted for changes in baseline BMI and fasting glucose. These findings demonstrate the similarities between the Da Qing study and our included studies despite using older criteria accentuating the use of non-pharmacological interventions to prevent progression to diabetes.
In terms of the effectiveness, it is difficult to compare the different intervention methods due to the lack of a uniform approach of the selected studies in measuring the impact. However, exercise and dietary interventions34–36 showed more significant results than lifestyle alone33 in preventing the onset of T2DM, reducing body weight and decreasing fasting glucose level. We did not find any trial comparing the effectiveness of lifestyle, exercise and dietary interventions conducted in LMICs. Three of the selected studies33 35 37 considered cultural aspects of the participants while designing the appropriate intervention. It was previously reported that culturally tailored and targeted interventions yield better results than a generalised approach to preventing diabetes.47 48 We also think that the distinctive difference in lifestyle, food habits and healthcare-seeking behaviour between people living in LMICs and high-income countries (HICs) warrant specifically-aimed interventions. This is the principal reason we explicitly chose LMICs as the place of studies to be included in this review.
We tried to broaden the reach of the review by conducting a comprehensive search in several databases but limited our searches to the English language only. There might be other studies in local languages other than English which we have missed in our search. This is one of the main limitations of our review. There were several studies conducted in other LMICs on non-pharmacological interventions for T2DM, but they were either conducted on patients with diabetes, or had different primary outcomes, or on younger respondents, and so on. At the time of our search, we only found studies from Iran, China and India that met all the inclusion criteria and were included in the systematic review. Besides, many urban settings in China are not economically different from metropolitan areas in most HICs. This fact underscores the need for further RCTs for the non-pharmacological interventions of T2DM to be conducted in LMICs. As the selected studies used different parameters and attributes to measure the primary outcome, and they have different intervention periods, it is difficult to have an exact comparison among the studies regarding the best strategy and duration of the interventions.
The principal strength of this systematic review is the inclusion of RCTs only, which helped to ensure the true effectiveness of the intervention programmes. We also followed the Cochrane guideline for systematic review stringently, which also ensured the high quality of the review. All the studies demonstrated low ROB in most of the bias assessments. There were some unclear results in allocation concealments and other biases. Four of the five studies used the same primary outcome, but all five studies used different intervention methods. The studies used a sufficient intervention period, but no crossover trials were found.
Future research should examine the efficacy of diverse non-pharmacological approaches for diabetes prevention programmes. These research must adapt culturally and geographically appropriate intervention measures for LMICs to maximise their effectiveness in both clinical and community settings. Policymakers and healthcare stakeholders from LMICs should formulate health policies to mobilise resources to emphasise the non-pharmacological interventions for T2DM. Resources for diabetes prevention programmes should be focused to enhance the ability to reach diverse adults and young adults at risk for type 2 diabetes.
Data availability statement
Data are available upon reasonable request. The data sets generated and/or analysed during this review shall be available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to acknowledge the contribution of the current donors providing unrestricted support to icddr,b that include: the Governments of Bangladesh, Canada, Sweden and the UK. We gratefully acknowledge these donors for their support and commitment to icddr,b's research efforts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KMSUR conceptualised the review. AS, RD, SE and MSI screened the articles, extracted data and assessed the risk of bias. KMSUR resolved the conflicts in screening, data extraction and assessment of risk of bias. AS, RD, SE, MSI and KMSUR drafted the manuscript. KMSUR reviewed, revised and finalised the manuscript. All the authors approved the final version of the manuscript. KMSUR is the guarantor of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.