Article Text

Abstract
Objectives The current study examines the mediating roles of resilience and self-efficacy and the moderating role of gender in the association between neuroticism and psychological distress in Chinese freshman nursing students (FNSs).
Methods A total of 1220 FNSs were enrolled from the Be Resilient to Nursing Career (ChiCTR2000038693) Programme and the following instruments were administered to them: NEO Five-Factor Inventory, General Self-Efficacy Scale, Connor-Davidson Resilience Scale and Kessler Psychological Distress Scale. A moderated mediation analysis and a generalised additive model analysis were performed.
Results The direct and indirect effects of neuroticism on psychological distress were significantly mediated by self-efficacy (B = 0.200, 95% CI 0.001 to 0.039), resilience (B = 0.021, 95% CI 0.007 to 0.038) and the interaction between self-efficacy and resilience (B = 0.016, 95% CI 0.005 to 0.028). The interactions between neuroticism and gender (β = 0.102, 95% CI 0.001 to 0.203, p<0.05) and between resilience and gender were significant (β = 0.160, 95% CI 0.045 to 0.275, p<0.01). A non-linear and positive association was confirmed between neuroticism and psychological distress.
Conclusions Self-efficacy and resilience significantly mediate the relationship between neuroticism and psychological distress. Gender moderates the relationships between neuroticism and resilience and between resilience and psychological distress.
- EDUCATION & TRAINING (see Medical Education & Training)
- Depression & mood disorders
- MENTAL HEALTH
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Serial multiple mediation model was used to explore the mediating role of self-efficacy and resilience in the association between neuroticism and psychological distress.
Moderation model was used to explore the moderating role of gender.
Generalised additive model analysis was performed to estimate the non-linear relationship between neuroticism and psychological distress.
Causal inferences cannot be drawn owing to the study’s cross-sectional design.
Introduction
An estimated global shortage of 5.9 million nurses was reported by the WHO in 2018.1 Nursing students, as future nurses, are receiving increasing attention from multidisciplinary researchers. However, the prevalence of depression and moderate to severe anxiety among Asian nursing students is 43% and 56%, respectively.2 3 Additionally, freshman students are 1.7 times more likely to experience psychological distress compared with senior students.4 5 Thus, the risk factors for psychological distress in nursing students, especially in freshman nursing students (FNSs), should be identified to help improve their mental health. Neuroticism is a stable personality trait characterised by negative emotions, such as worry and guilt; individuals with neurotic traits are more prone to psychological distress.6–8 Additionally, self-efficacy, defined by Bandura’s self-efficacy theory as a sense of control over one’s environment and behaviour, has been confirmed as a protective predictor of psychological distress.9–12 Moreover, resilience, defined as the ability to bounce back from adversity, has also been identified as a protective predictor of psychological distress in general population.13 In our previous study, a positive association between self-efficacy and resilience was confirmed among FNSs.14 Based on Kumpfer’s Resilience Framework, neuroticism-based stress can be efficiently buffered by resilience, resulting in adequate adjustment.13 Gong et al found that neuroticism was positively associated with depression; additionally, depressive symptoms were lower in the higher resilience group than in the lower resilience group.15 Although neuroticism, self-efficacy and resilience have been identified as independent predictors of psychological distress in various populations, to the best of our knowledge, the associations of these four variables among FNSs have not been fully explored. Moreover, it may be worthwhile to examine whether gender plays a role in the associations among neuroticism, self-efficacy and resilience. Therefore, the current study explores the following:
(1) The associations among neuroticism, self-efficacy, resilience and psychological distress based on a serial multiple mediation model, (2) the potential non-linear association between neuroticism and psychological distress using generalised additive model analysis (GAMA) and (3) the moderating role of gender. We hypothesise that (figure 1):
Neuroticism is negatively associated with self-efficacy and resilience and positively associated with psychological distress.
Self-efficacy and resilience significantly mediate the association between neuroticism and psychological distress.
Gender moderates the associations among neuroticism, resilience and psychological distress.
Neuroticism is positively and non-linearly associated with psychological distress.
Methods
Participants and procedure
A total of 1220 FNSs were enrolled from the Be Resilient to Nursing Career (ChiCTR2000038693) Programme between September and November 2020. The inclusion criteria were as follows:
(1) being a newly enrolled FNS in 2020, (2) ability to communicate fluently in Mandarin and (3) agreement to participate in this study. The exclusion criterion was a present or past diagnosis of a mental disorder. All participants were approached by trained researchers and informed consent was obtained before the formal investigation. The study has been described in detail elsewhere.14 16
Instruments
Demographic characteristics
Based on previous research,17 18 we collected data on FNSs’ demographic characteristics (eg, age, gender, residence) and profession-related information (eg, role model, medical staff as relatives).
NEO-Five Factor Inventory
The NEO-Five Factor Inventory (NEO-FFI) is a 60-item self-report scale used to assess personality traits on five dimensions, including neuroticism, extraversion, openness, agreeableness and conscientiousness.19 The current study focused only on the neuroticism dimension (12 items); higher scores indicated higher levels of neuroticism. The NEO-FFI demonstrated good internal consistency among Chinese adolescents.15 The Cronbach’s alpha coefficient for FNSs was 0.821 in the present study.
General Self-Efficacy Scale
General Self-Efficacy Scale (GSES) was developed by Zhang and Schwarzer.20 The reliability of the Chinese version of GSES has been confirmed.21 The scale comprises 10 items with higher scores indicating higher levels of self-efficacy. The Cronbach’s alpha for GSES was 0.898 in the present study.
10-item Connor-Davidson Resilience Scale
While the 25-item Connor-Davidson Resilience Scale (CD-RISC) was developed by Connor in 2003, a 10-item version was later developed by Campbell-Sills and Stein.22,23 It is a unidimensional scale and uses a 4-point Likert scale; higher scores indicate higher levels of resilience. The reliability of the Chinese version of 10-item Connor-Davidson Resilience Scale (CD-RISC-10) has been established.24 This scale has been successfully administered in previous studies.14 16 The Cronbach’s alpha was 0.875 in the present study.
Kessler Psychological Distress Scale
The Kessler Psychological Distress Scale (K10 measures the frequency of symptoms related to non-specific psychological distress such as anxiety experienced in the past 4 weeks.25 26 It comprises 10 items, with the total score ranging from 10 to 50. In China, the K10 has been widely used to screen psychological distress among the general population.27 28 The Cronbach’s alpha was 0.885 in this study.
Data analysis
First, descriptive statistics were used to analyse the demographic characteristics and Pearson’s correlation analysis was performed to estimate the associations among neuroticism, self-efficacy, resilience and psychological distress. Second, serial mediation analysis was used to establish the mediating model. Since the data were self-reported, common method variance (CMV) was checked using Harman’s single factor test.29 Neuroticism and psychological distress were identified as the independent (X) and dependent (Y) variables, respectively. Self-efficacy (M1) and resilience (M2) were recognised as the mediators. The total, direct and indirect effects were estimated and 95% CI were calculated with 5000 bootstrapping resamples. Third, a moderation analysis was performed to examine the moderating role of gender on the associations among neuroticism, resilience and psychological distress. Fourth, GAMA was employed to estimate the non-linear association between neuroticism and psychological distress.30 Fifth, psychological distress was classified into binary data (high as 1 and low as 0 based on a cut-off of 24),31 while neuroticism was classified into quartiles titled as ‘low neuroticism’, ‘medium neuroticism’, ‘high neuroticism’ and ‘very high neuroticism’ to further examine the association between neuroticism and psychological distress. SPSS (V. 26.0) and Empower Stats (V. 2.2) were used for all statistical analyses.
Patient and public involvement
No patients were involved in this study.
Results
Sample characteristics
A total of 1220 FNSs were enrolled in the present study; 21 participants were excluded due to missing data, resulting in a final sample of 1199 (98.3%). The gender ratio of male to female participants was 1:4.06. Demographic and profession-related characteristics are described in figure 1B.

The conceptual model and univariate analysis. FNSs, freshman nursing students.
Associations among neuroticism, self-efficacy, resilience and psychological distress
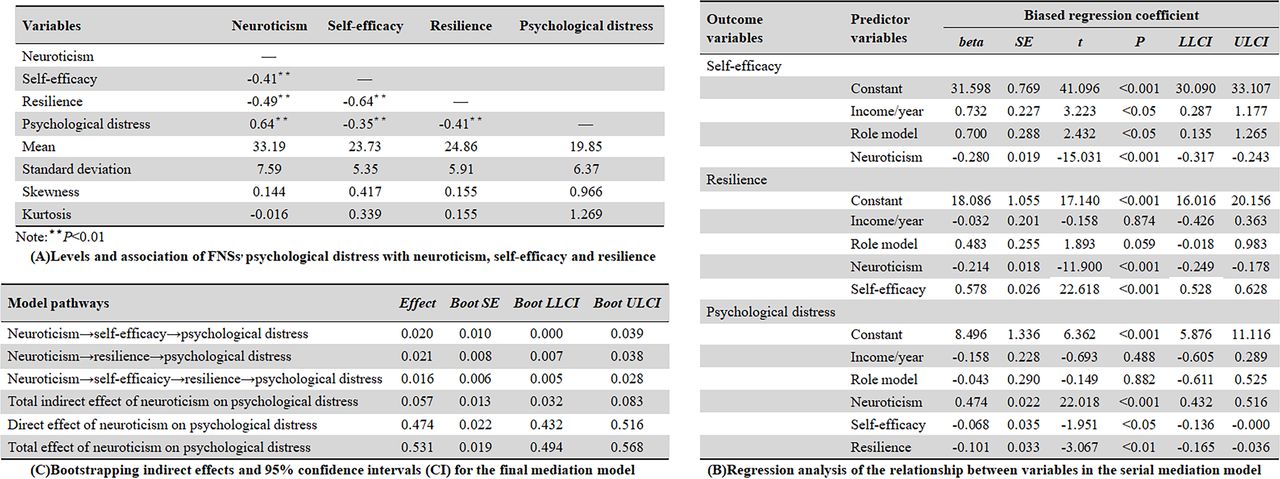
The common method bias test indicated a total of seven factors with eigenvalues greater than 1. The first factor accounted for 28.4% of the total variance and the common method bias was negligible. Psychological distress was significantly correlated with neuroticism, self-efficacy and resilience (r = 0.64, –0.35, −0.41, respectively; p<0.01).
Other results from Pearson’s correlation analysis are given in figure 2A.

The serial-multiple mediation model. FNSs, freshman nursing students.
Figure 2B shows that neuroticism was negatively associated with self-efficacy (β = −0.280, p<0.001) and resilience (β = −0.214, p<0.001). Both self-efficacy and resilience had a significant impact on psychological distress (self-efficacy, β = −0.068, p<0.05; resilience, β = −0.101, p<0.01). Figure 2C shows that the indirect effect of neuroticism through self-efficacy and resilience on psychological distress was significant (B = 0.016, 95% CI 0.005 to 0.028).
The moderation model
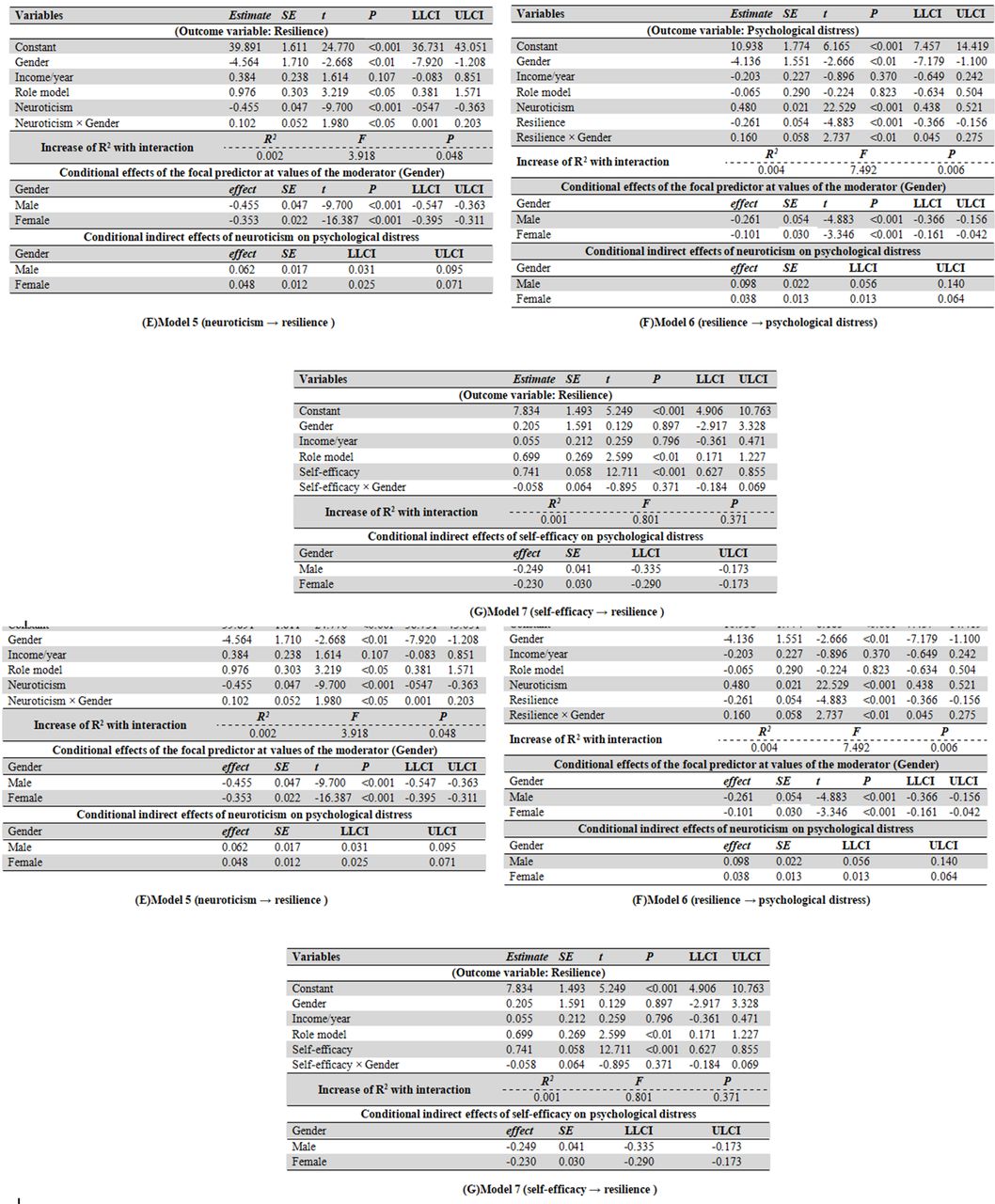
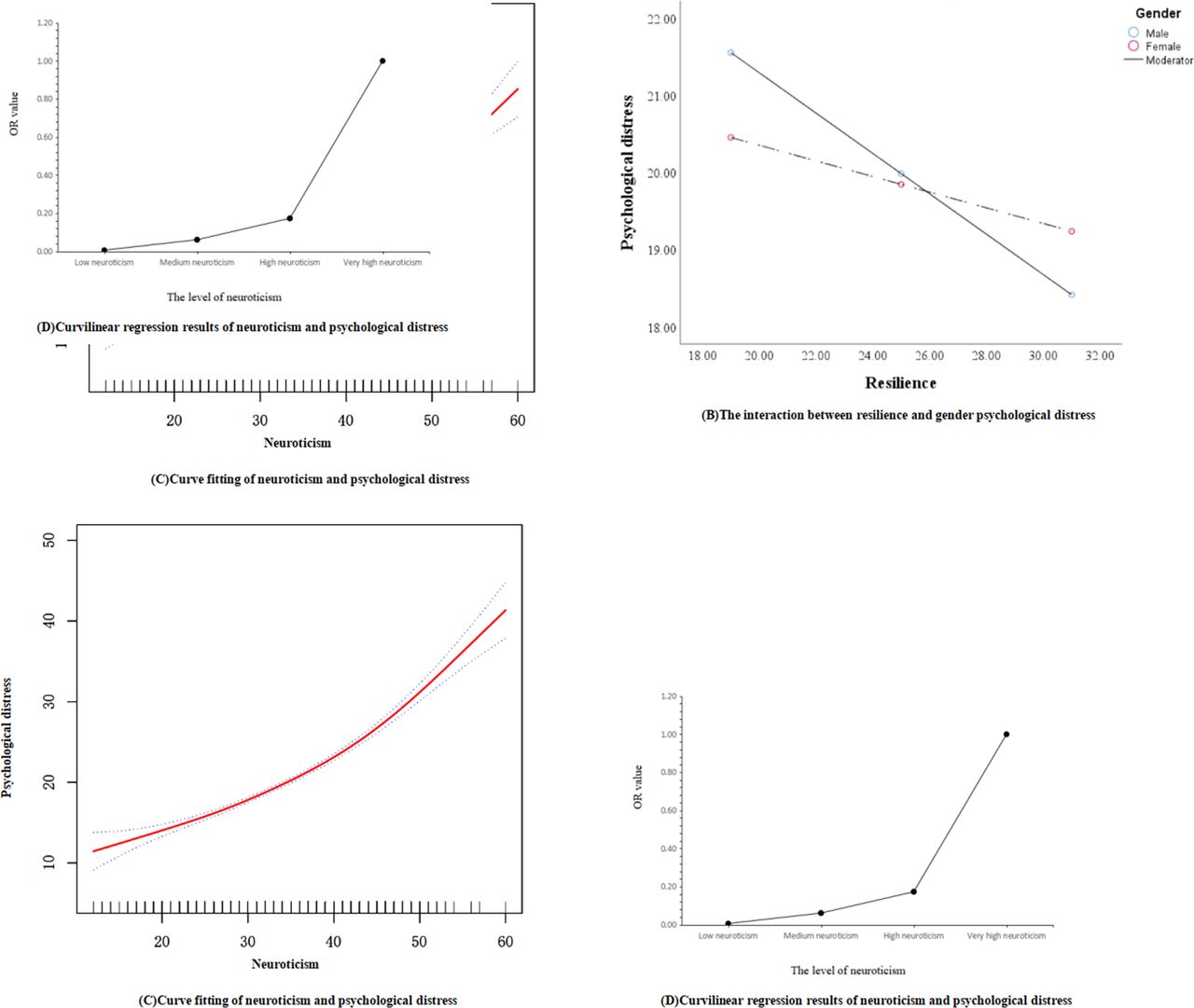
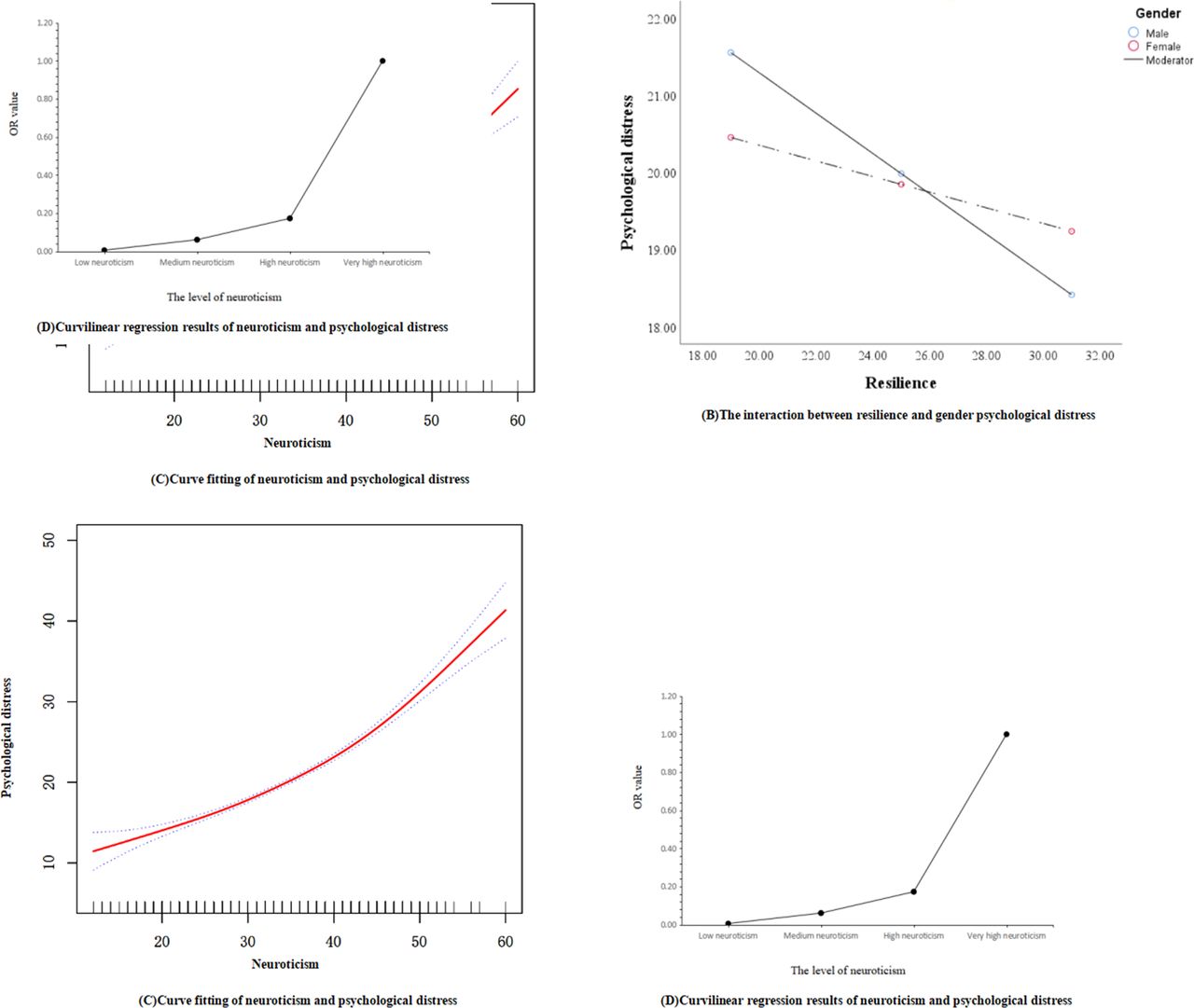
The results of the moderation analysis are depicted in figure 3. In Model 1 (neuroticism → psychological distress), the interaction of neuroticism and gender was not significant (B = −0.075, 95% CI −0.172 to 0.022, p=0.131), indicating that gender did not moderate the relationship between neuroticism and psychological distress. Similarly, in Models 2, 3, 4 and 7, the moderating effect of gender was not significant (B = 0.047, 95% CI –0.050 to 0.143, p=0.342; B = 0.123, 95% CI –0.013 to 0.0260, p=0.260; B = −0.067, 95% CI –0.163 to 0.030, p=0.177; B = −0.058, 95% CI –0.184 to 0.069, p=0.371, respectively). In Model 5 (neuroticism → resilience), the significant moderation effect of gender was recognised and visualised in the simple slopes test (βmale = −0.45, p<0.01; βfemale = −0.35, p<0.01, figure 4A). In Model 6 (resilience → psychological distress), as shown in figure 4B, gender could moderate the association between resilience and psychological distress (βmale = −0.26, p<0.01; βfemale = −0.10, p<0.01).
Analysis of moderating effects.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Simple slopes test and curveline regression.
Generalised additive model analysis
Figure 4C indicates a non-linear and positive relationship between neuroticism and psychological distress by GAMA. Figure 4D demonstrates that FNSs with low, medium and high neuroticism were 0.006, 0.061 and 0.173 times, respectively, as likely to have psychological distress as those with very high neuroticism.
Discussion
The associations among neuroticism, self-efficacy, resilience, psychological distress and gender have not been sufficiently explored in FNSs. First, the current study found that neuroticism is positively associated with psychological distress, which is consistent with previous findings.32 33 FNSs with high neuroticism scores were sensitive to external stressors and more prone to psychological distress. However, as neuroticism is a stable personality trait, efficient intervention has not been possible. Therefore, identifying FNSs with high neuroticism may be the first step to help improve their mental health. Second, the mediation model showed that self-efficacy and resilience significantly mediated the relationship between neuroticism and psychological distress, indicating the important pathway of neuroticism → self-efficacy → resilience → psychological distress, which was also partially confirmed in a previous study.14 According to this pathway, theoretically, increasing self-efficacy and resilience could help reduce the impact of neuroticism on psychological distress.34 Self-efficacy and resilience can be enhanced through specific programmes. For example, for resilience, Ye developed a programme called Be Resilient to Breast Cancer to promote breast cancer patients’ resilience resulting in increased quality of life.35–38 Such successful programmes could be adapted and used for FNSs. Based on these findings, more attention should be paid to FNSs with high levels of neuroticism and low levels of resilience and self-efficacy, which makes them prone to psychological distress.
Third, gender moderated the associations among neuroticism, resilience and psychological distress, which is consistent with existing literature.39–41 However, gender moderated only the associations between neuroticism and resilience and resilience and psychological distress. This indicates that the pathway of neuroticism → resilience → psychological distress was different for male FNSs compared with their female counterparts, which is consistent with previous research,42 43 and contributes to the gender difference in the model.
Fourth, a non-linear relationship between neuroticism and psychological distress was identified via GAMA, contributing valuable insights to the existing literature linking neuroticism with psychological distress.44
In summary, FNSs with high neuroticism and low self-efficacy or resilience are more likely to experience severe psychological distress, which should be addressed through early identification and intervention.
Limitations
Several limitations should be considered. First, the FNSs from the four universities included in this study may not be representative of the general FNS population; thus, these findings should be further validated with a larger sample comprising participants from diverse cultural backgrounds. Second, due to the cross-sectional nature of this study, causal relationships could not be established, and a longitudinal study should be conducted to replicate these findings. An ongoing 2 year follow-up assessment of this cohort (BRNC Programme) will provide additional insights in the future. Third, as medical students are quite different from other professionals, the instrument used to measure resilience in the current study may not have captured some characteristics of resilience. Therefore, new resilience instruments specific to medical students should be developed, which has been highlighted in other resilience-based studies.45–50 Fourth, several potential confounders, such as social support, hope and family function were not considered in the moderated mediation model due to heavy scale burden; this may have had an impact on the association estimation.
Conclusions
Self-efficacy and resilience mediate the relationship between neuroticism and psychological distress. Gender moderates the relationships between neuroticism and resilience and between resilience and psychological distress.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The present study is part of the Be Resilient to Nursing Career programPprogramme (BRNC, Registration number: (ChiCTR2000038693)) and was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine (No: ZYYEC-ERK【2020】132). The participants were reassured that their personal data would remain confidential and would be reported anonymously. All instruments used in the current study were used after obtaining the original authors’ permission.
Acknowledgments
The authors would like to thank the directors from the participating universities for supporting data collection and the newly graduated nurses who were involved in this research.
References
Footnotes
Contributors XM: conceptualisation, data curation, methodology, software, writing—original draft. HW: funding acquisition, investigation, software, methodology. XWa: methodology, software. XWu: investigation, resources, software, validation. JW: investigation, resources. ZY: funding acquisition, supervision, writing—review and editing.
Funding This research was funded by grants from National Natural Science Foundation of China (No. 71904033), Young Elite Scientists Sponsorship Program by CACM (2021-QNRC2-B08), Humanity and Social Science Youth Foundation of Ministry of Education of China (No. 19YJCZH227), Humanity and Social Science Foundation of Department of Education of Guangdong Province (No. 2020WTSCX009), Humanity and Social Science Foundation of Guangzhou (No. 2021GZGJ57), and Humanity and Social Science Foundation of Guangzhou University of Chinese Medicine (No. 2020SKXK01, 2021SKYB07).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.