Article Text

Abstract
Objectives To understand the barriers towards deceased organ donation among Indians living globally.
Design Integrative systematic review using narrative synthesis.
Data sources CINAHL, Medline full-text, PsycInfo, Scopus, Global Health, Web of Science, and PubMed Central, Indian Journal of Transplantation and Google Scholar.
Time period 1 January 1994 to 31 December 2021.
Participants Individuals of Indian origin living globally.
Results Eighty-nine studies were included with more than 29 000 participants and quality of the studies were assessed using Joanna Briggs Institute’s critical appraisal tool. Though majority of the participants had knowledge toward organ donation with a positive influence on willingness, the gap between knowledge and willingness was huge, with minimal registration influenced by the complex sociocultural constructs. Various sociocultural constructs such as family, fear and mistrust, religion, and bodily issues play a vital role. Differences were identified in willingness to donate and register between southern and other regions of India. Indian’s organ donation behaviour in other geographical locations differed based on the socioreligious background of the country they lived in such as in Malaysia, Canada and the UK. However, they were collective in decision-making and had complex sociocultural interference irrespective of the country the individual lived which differed only in their next generations.
Conclusion Though this study showed the complex relationship, and its influences on organ donation behaviour, lacunae were identified to further understand how such complex interactions determine or inform the behaviour. Also, methodological issues were identified, where this particular population outside India were collectively studied with their neighbouring population which are not homogenous. Studies in India majorly addressed a similar aim using similar methods which produced repetition of studies leading to lack of diversified, wider and in-depth research. Therefore, while this systematic review addressed the barriers toward organ donation among Indians living globally, it also informs various gaps in research and also methodological issues.
PROSPERO registration number CRD42019155274.
- health policy
- ethics (see medical ethics)
- transplant medicine
Data availability statement
No additional data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review on the barriers towards deceased organ donation among Indians living globally, registered with PROSPERO, and published.
Both quantitative and qualitative studies were included to address the aim of the review using integrative approach and narrative synthesis, an appropriate methodology.
Included studies exclusively represented the Indian population and studies that collectively studied Indians with heterogenous South Asian, or Asian population were excluded, thereby keeping the rigour of this study, and identifying methodological issues involved.
Findings are based on the quality of each studies appraised using appropriate tools, and the assessment is also made available to the view of the readers.
Studies were limited only to English language, and commentaries were excluded.
Introduction
Since the first deceased organ transplantation performed by Joseph Murray in 1960s, the science of transplantation has witnessed exponential growth.1 However, the gap between demand and supply of organs has represented a significant challenge,2 particularly among the Asian population who live both within and outside their continent.3–5 India located in the South of Asia is the second largest populated country in the world6 having largest migrating population in Asia,7 and also has the highest prevalence of diabetes and hypertension.8 Such non-communicable diseases among Indians9 10 leading them to end-stage organ failure11 12 increases their need for organs.
While the need for organ donors is high among the Indian population, the actual number of donors remain too low to satisfy the number of recipients on the waiting list,13 with the Indian national organ donation rate less than one per million population (pmp).14 Reluctance to donate organs among this ethnic population might not be isolated just within Indian border,15 with evidence suggesting that Indian population from the UK is also disproportionately impacted, where they continue to be over-represented in the recipient waiting list but under-represented in the donor list.16 This behaviour is again identified in Canada.17 Therefore, globally, Indian population has demonstrated lower organ donor registration and consent both within and outside the border.
There have been a larger number of studies conducted among the Indian population living globally to understand the factors that influence their organ donation behaviour. However, to date, there has been no systematic review conducted to synthesise the available evidence to understand the barriers toward organ donation among the individuals of Indian origin. Therefore, a systematic review was proposed with an aim to address this gap to gain a deeper insight into the barriers towards deceased organ donation behaviour among this particular population living globally.18
Method
Protocol and registration
This systematic review’s protocol has been registered in PROSPERO (CRD42019155274) and also published.18
Systematic search
Search strategy was developed collaboratively with the research team and a subject specialist librarian. Databases namely CINAHL, Medline Full-Text, APA PsycInfo and Global Health were accessed through EBSCO platform, Clarivate for Web of Science, Elsevier for Scopus and US National Library of Medicine—National Institute of Health for PubMed Central were utilised. Key terms related to organ donation were first identified from studies published along with search terms used in other systematic review on organ donation19 20 and were tested in different combinations. Later, for each database, the search terms were then customised seeking to capture the most appropriate studies to answer the aim of this review (online supplemental file 1).21 However, for other resources like Google scholar and the Indian Journal of Transplantation other strategies were employed. All the published papers from 1 January 1994 to 31 December 2021 were searched from the archives of the Indian Journal of Transplantation to identify relevant studies. With regard to Google scholar, we searched using two methods. The first method used the word ‘Organ Donation AND India’ in title; and the second method used the same keywords but searched anywhere in the article. However, due to very high number of search results in the second method, we limited the search until we found no further relevant studies (an approach used by other published systematic review).22
Supplemental material
The systematic review included studies with individuals of Indian origin living both within and outside India (ie, migrant/first/second generation), aged 18 years and above from varied settings.18 Cross-sectional and qualitative study design were included as they were mostly employed to understand the barriers toward deceased organ donation. For all the databases, search strategy was restricted between 1 January 1994 (ie, the year when the first law towards organ donation was enacted in India) and 31 December 2021 (ie, a recent day before the submission) and was restricted only to studies published in English. However, interventional studies, commentary or opinion papers, studies on blood, bone marrow, body, sperm, and egg donation were excluded alongside any studies which addressed only living donation.
Search outcome
Following a stage-by-stage exclusion from 8655 studies initially extracted from the main databases, 50 studies were included in final review along with 39 studies included from other sources (figure 1). The studies were initially exported to RefWorks (https://refworks.prorequest.com/). Microsoft excel was used to keep a record of studies excluded by duplicates, title, abstract and full text. All the 8655 studies along with studies from other sources were screened by two authors independently and the final 89 studies included were in-agreement with all the authors.
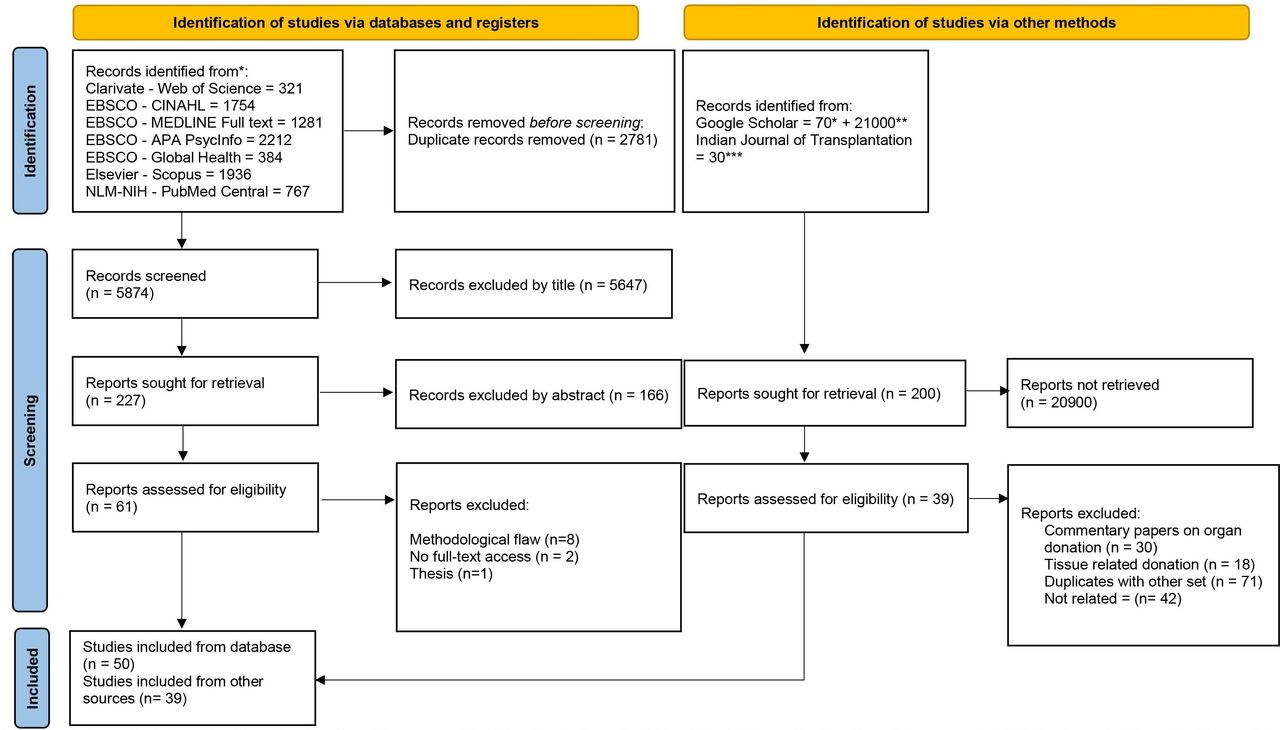
PRISMA flow chart. *Google Scholar method 1 explained in method section of the manuscript. **Google Scholar method 2 explained in the method section of the manuscript. ***Indian journal of Transplantation—all issues were manually searched from 1994. From: Page et al.126
However, during the process, studies conducted among Indians living outside India were identified to be collectively studied as South Asians or with other Asian population. For instance, a study conducted among Indo-Canadians in Canada included all neighbouring ethnic groups of India.23 Also, in other countries like the UK and Malaysia, Indian population was collectively studied along with other ethnic groups and the results were not distinctively shown24–26; therefore, eight studies had to be excluded due to these methodological limitations. The perspective of deceased organ donation varies even within India’s nearest neighbouring country.4 27 Therefore, this review included only the studies which exclusively reported the findings among Indian population.
Quality assessment
Appropriate critical appraisal tools from Joanna Briggs Institute were used to critique the rigour of each studies included,28 also used in other organ donation systematic review.19 29 Comprehensive reporting on the quality assessment for both cross-sectional and qualitative studies is reported in figures 2 and 3. Quality assessment was initially carried out by the primary researcher after which it was reviewed by the other two authors independently. Both the authors along with the primary researcher agreed on the quality assessment as mentioned in figures 2 and 3. The review included all studies; however, minimal emphasis was given for those studies that demonstrated only fewer items in the quality assessment checklist.

Quality appraisal checklist—quantitative studies.

{kind=link}
{kind=link}
{kind=link}
Quality appraisal checklist—qualitative studies.
Data synthesis
This systematic review followed an integrative review with narrative synthesis approach enabling to synthesise complex information towards the phenomena of interest30; a methodology also employed in another systematic review on organ donation that reviewed both quantitative and qualitative studies.20 Narrative synthesis primarily depends on words and texts to summarise the findings with four process elements such as (1) systematic search and quality appraisal, (2) grouping and clustering of the studies reviewed, (3) text summary development, and (4) assessment and interpretation.31
First, following the systematic search and quality appraisal, summary data were collected for each study, and they were recorded across a table which had information needed to cluster the studies to compare and study across (table 1). Second, with the cross-sectional studies, numerical results from each study were tabulated across a matrix and were compared across to study their relationship in terms of barriers. Later, full synthesis of the qualitative studies was undertaken by coding the findings sections using NVivo V.11. Codes were then organised into themes to address the barriers appropriately.
Evidence table
While comparing and studying across the studies included in the review to understand their relationship, various elements such as what the study is about, type of study, their approach, the findings, study settings and population studied were also considered. Noblit and Hare (1988) described this as ‘Reciprocal translation’, also used in other similar methodological approaches.32–36 Third, full syntheses of both cross-sectional and qualitative studies were studied across to understand the supporting and refuting evidence collectively. For each section of the findings, quantitative studies provided the initial context following which findings from qualitative studies were used to elaborate and explain. With limited qualitative study narratives to support or refute the cross-sectional study findings, they were incorporated into the integration of the findings wherever possible. Both convergent and divergent findings are explained in this review, whereby if divergent findings were identified explanatory factors such as type of study or setting, or population were provided to facilitate better understanding.20
Findings
Grouping and clustering
Among the 89 studies reviewed, majority (84%) were conducted among Indians living in India (n=75) while other fourteen studies were among people of Indian origin living in the UK (n=8), Malaysia (n=5), and Canada (n=1). Cross-sectional studies (n=79) included various settings such as general community, education institutions and hospital setting (table 1). Qualitative studies (n=10) used methods like in-depth interviews and focus group discussion (table 1). Among the 29 385 individuals involved in the retained studies, 27 503 individuals (94%) were from studies conducted in India. Among the studies conducted in the UK, there were 1235 individuals in total; however, one study had no evidence on the sample number of Indian participants involved,27 and the Malaysian studies had 647 individuals in total. The study participants from the Canadian study were not included since they were information taken from national registry which had around 228 879 Indian individuals.17
Findings
Integration and relationship
Based on the narrative synthesis, findings are described under the following six themes namely: (1) knowledge and awareness towards deceased organ donation, (2) willingness and actual behaviour towards deceased organ donation, (3) familial influence, (4) fear and mistrust, (5) religious influences, and (6) bodily issues.
Knowledge and awareness of deceased organ donation
Being the most common theme studied across, findings showed that knowledge had a positive correlation with willingness and practice.37–44 Both among Indians living in India and outside, younger adults, participants from higher socioeconomic status, and with higher education or healthcare education demonstrated higher knowledge towards deceased organ donation43–60 and individuals from southern region of India showed higher knowledge compared with other regions in India.61–66
While majority of the studies confirmed that almost all the participants had heard about organ donation and had higher awareness, knew what organs can be donated4 39 44 53–55 67–85 and that organs can be donated to anyone,46 61 80 the knowledge and understanding on brain death was less well understood.49 64 68 69 75 86–89 A qualitative study from an urban area in the southern region of India also found brain death as a new concept for many and hard to accept among the public.90 Also, many were not aware about the organ donor card,67 83 88 91–94 where and how to register and obtain an organ donor card40 50 53 55 56 70 71 94 95—an important component for organ donor registration. In addition, knowledge on the law that governs organ donation was also found to be low.40 71 92 96 97 Though a study among Indians living in UK showed that disinterest, emotional distaste, family opposition and religion to be the underlying cause for reluctance to register,58 among Indians living in India, the awareness on brain death, organ donor card, where and how to register were reported as important factors along with family and religion among individuals who were willing to register.40 49 50 53 55 64 67 69–72 86 91–96 98
Willingness and actual behaviour towards deceased organ donation
Greater knowledge showed positive influence on the attitude and willingness across all Indian regions.17 41 43 44 50 92 99–103 Similar to higher knowledge among individuals from southern region of India, willingness to register, to donate and to accept organs for transplant was also shown to be higher.38 45 46 49 66 68 92 99 101 However, though knowledge had a positive association towards attitude and willingness, the proportion of individuals willing to register, and actual registration was very low and similar across every study included. Correspondingly, even a study conducted among Indian students living in UK revealed that 55% of the individuals doubted if they would go ahead with registration.58 With such reluctance, Indians living in India, UK and Malaysia considered fear of misuse and family refusal as a major reason, alongside minor reasons like emotional barriers, bodily issues and religion.44 68 75 79 94 95 97 100 104–107 On contrary, the most common reasons to donate an organ was to save someone’s life, closely followed by prolong someone’s life, social commitment, altruistic deed and to keep at least the organs alive.72 75 91 99 104–111
Higher proportion of participants were willing to receive compared with donating38 45 46 58 68 99 101 112–114 among Indians living globally. Furthermore, studies revealed that among those who were willing to donate, majority were only willing to donate specific organs namely eye/cornea and kidneys,46 61 62 which may be related to the knowledge on what organs can be donated.67–72 76–78 86 Nonetheless, majority of the participants were willing to support and promote organ donation in their region and was similar across India.55 57 91 99 109 110
Younger adults, participants from higher socioeconomic status and participants with higher education or healthcare education demonstrated higher willingness towards deceased organ donation among Indians living globally.17 27 43 45 47 48 53 58–61 108 However, this was not consistent during the time of actual behaviour. Studies showed that there was almost equal distribution of participants from lower socioeconomic status and lower education, who gave consent and actually signed for deceased organ donation.47 90 96 However, this conclusion is based only from few studies which showed to be similar in north and south of India.47 90 96
Familial influence
In spite of willingness to register for organ donation, larger proportion of individuals have not initiated a conversation or discussed their willingness with their family members, an important behaviour for a successful donation52 65 68 71 82 93 100 115 116—however opted family as the major barriers towards organ donation,46 63 65 69 72 94 100 102 this was identified even among Indians living outside India.27 117 Qualitative studies conducted in India, the UK and Malaysia revealed the main reasons was their lack of confidence in initiating conversations around sudden deaths, and with these conversations perceived unwelcomed by their parents and elders.4 27 90 95
However, other few qualitative studies conducted among Indians who were born and grew in another country (ie, UK and Canada) revealed that they are less concerned of sharing their views compared with their older generations (ie, mostly migrant generation) and were more willing to discuss their wishes with their families,17 27 81 118 which could be related to acculturation. On the other side, qualitative studies conducted in southern India and the UK suggested that such conversation only occurred when individuals read or viewed such events.90 119 Also, during the time of consent request, unknown will of the deceased showed to be a significant challenge during the decision-making process,96 making such discussion very important during the crucial decision-making moments.
Willingness to support family members was shown to be higher among healthcare students compared with other students55 56 100 120 and lower among family members from rural areas.99 116 However, while higher proportion of individuals were willing to support family members for organ donation,38 44 61 71 88 92 101 118 only very few families actually supported this decision when families were approached for consent.90
Though studies included found no association based on marital status,38 45 101 one study found that unmarried individuals appeared to be more willing to donate compared with married couples.101 Also, participants who were aware of their spouse’s approval opinion, they were more willing to donate compared with those unaware of their spouse’s opinion.45 Among the type of family, individuals from ‘joint’ families had higher knowledge, while willingness to donate was found to be higher among nuclear families and also was identified to be highly influenced by the family.4 17 38 48 50 This was a similarity identified in India, Canada and the UK, showing it to be a collectivist decision-making, where involvement of the extended family is identified to be a part of decision-making among this population irrespective of the country they live.4 17 38 48 53 117 And involvement of extended family was identified to be a barrier among Indians in the UK, in this process.4
Fear and mistrust
Fear on misuse of organs by the healthcare team, and lack of trust was the other major barrier reported.55 63 64 68 69 71 72 78 83 89 94 97 104 105 Participants from several studies relate organ donation to organ trafficking and misuse which leads them to fear and mistrust.49 58 65 99 105 A qualitative study also revealed increased ambivalence that while on one side participants perceived organ donation as a noble act, on the other side they were also fearful of organ misuse due to the information that they hear through news and media on organ trafficking and exchange of money for organs.90
Also similar in the UK, among Indian participants, a mother was afraid to see an organ donor card in her child’s wallet as she was thinking if doctors will come to see it, then they may deviate the process towards donation and give less care towards saving her child.27 In parallel, general population from India also feared premature declaration of death for the need of organs.39 99 120 However, healthcare population groups were less likely to believe that there will be any premature declaration of death by the doctors.38 71 85 87
Religious influence
Overall, majority of the participants favoured organ donation.27 38 46 47 49 61 80 81 101 106 108 109 However, when further looked based on religion, different studies showed different religious groups to be more willing to donate compared with individuals from another religious group,45 48 61 73 121 showing no consistency on which particular religion is more supportive or rejective.45 48 52 61 121 In parallel, a qualitative study conducted among UK university students of Indian descendants showed lack of homogeneity even within one same religion. Some agreed that body needs to be intact for reincarnation, while other participants believed that body and soul are two different entities and that only the soul counts while body is left to decay in this earth.27 97 However, among studies undertaken outside India, Indian Muslim participants were identified to be less likely or supportive towards organ donation.4 44 95 106 117 Qualitative studies from outside India identified that lack of the standpoint of religion as one of the reasons leading to such reluctance and not the individual’s opinion.108 117
However, though there were differences of opinion across and within the religion, majority of the participants agreed that organ donation is not against religious views38 68 72 88 90 97 101 109 and also considered religion as the very least barrier towards organ donation.44 45 63 65 68 90 114 115 122 A qualitative study conducted among UK students with Indian origin showed that though individuals felt religion may influence their decision it was not the only factor that that will be considered in such decisions.27 Yet, favourable opinion of religion towards organ donation was found to be positively correlating with their willingness to donate.38 52
A qualitative study conducted in UK with Indian students revealed that younger generations were less bothered about religious views compared with older generations, which could have occurred due to acculturation.27 Also, participants preferred that religion should not be a criterion based on which allocation can be decided48 68 109 115 and that organ of a deceased person can be donated to a recipient from any religion.48 68 109 115
However, during the time of consent, a stakeholder from a qualitative study said that families who were not willing to donate use the concept of religion as a reason to decline donation, though none of the religion is against organ donation. In the same qualitative study, public participants from various religious group felt that their religion supports organ donation.90
Bodily issues
Majority of the individuals from the reviewed studies were not concerned about bodily issues though it has to undergo incisions while explanting.38–40 45 46 61 91 97 118 However, on the other side, majority also agreed that it is an individual’s complete right to have the organs within the body when dead.49 87 While majority of individuals were not concerned about incisions in the body, a qualitative study found that in the real time of consent, stakeholders found it easy to get approval for corneal donation and not solid organs as it may have many incisions over the body and disfigure it.72 In relation to funeral practices involving the deceased body, majority were aware that normal funeral practices can be conducted even after donating organs,38 49 61 87 91 115 contrast findings were also evident.49 55 87 However, majority opted body disfigurement, but less proportion, as one of the least reasons to be a barrier towards organ donation, both within and outside the borders of India.46 63 65 69 83 100 106 108
Discussion
To the best of our knowledge, this is the first systematic review that reviewed barriers towards organ donation among Indians living globally. Also, this is one of the few systematic reviews in organ donation that used integrative methodology. While majority in India have heard or are aware of organ donation, and had a positive correlation with willingness, their gap is wide. This indicates that there could be various factors other than knowledge which need to be studied in more detail. Organ donation being more embedded with health behaviour, there is a need to understand the relationship between behaviour and behavioural intention by adopting appropriate principles. This aids the specificity of policy and campaigns to address organ donor registration behaviour in this particular population.
Though gaps identified in majority of the quantitative studies merit qualitative studies, only very few qualitative studies were undertaken in India.87 90 97 For instance, though majority individuals were willing to be an organ donor, majority have not initiated any such conversation with their family members, yet considered family to be the major barrier.46 63 65 69 100 117 However, no further studies were exclusively undertaken to understand how a construct like family interferes in the decision-making toward registration and consent. Such studies will aid in developing and testing hypothesis or developing appropriate interventions to increase such conversation with family members. Such conversations play a very important role as the awareness on the willingness of the deceased plays a vital role in decision-making during consent.96 However, the influence of family can be different among Indians in India and outside India as the latter may have influences based on acculturation and enculturation27 58 while the prior maybe more concerned towards communication issues.52 65 68 90 93 100 115 116 While majority were willing to be an organ donor,27 43 45 47 48 53 58–61 they were unaware on how to register to be an organ donor.40 50 53 55 56 70 71 94 Therefore, further campaigns on registration procedure information will enable to improve organ donation in India.
This review showed that there are various complex interactions that happen in the society where an individual lives rather than just knowledge influencing organ donation decision. Fear and mistrust have shown to influence the uncertainty in decision-making for a very long time.27 40 48 55 63 64 68 69 71 72 78 97 However, studies failed to address how fear influences organ donation, what is the source of fear and how a construct like fear can be addressed. This fear could be due to the news or information that they hear on illegal organ donation and transplants practices around them or any other reasons,123 but not much have been studied why such fear exist among this population.
Also, while majority of the studies show influence of religion on organ donation, there is a greater need to understand how religion influences organ donation in India. Is it the misconception, or the lack of enabling religious community, or reluctance to take such conversation, or lack of information from the religious leaders or their physical practices that does not allow donation? Such in-depth studies need to be undertaken to gain a deeper understanding into the phenomena. Therefore, there is an urgent need, to study further how the interaction of the individuals with such a complex sociocultural and institutional structures influences the organ donation behaviour.
Various other factors such as age, sex, education and socioeconomic status showed greater influence on willingness to donate.27 45 47 48 53 58 61 However, studies showed that they did not hold true during the time of consent.47 96 This review therefore showed that there is some shift in behaviour during registration and the actual consent. This again probes to further the understanding on what happens during the time of consent, and why such a shift is seen in the intention to donate between these two time periods.
Overall, based on the studies undertaken among Indians living in India, the UK, Canada and Malaysia, similarities and differences were identified. The willingness and registration behaviour differed according to the geographical location where Indians lived in comparison to their native population. While Indians were considered to have higher attitude and willingness in Malaysia,84 114 Indians living in the UK and Canada were considered to have lower attitude and willingness.17 117 This could have been due to their respective sociocultural practices of Muslim major country (ie, Malaysia) and Christian major country (ie, Canada and the UK) with Hindu major population (ie, Indians). This argument is also supported by a study that compared organ donation willingness between Christian, Hindu and Muslim major native population.58 The similarity identified was that irrespective of their geographical location, this was a collectivist decision and not an individual’s decision4 85 117 with family, fear and mistrust, and bodily issues identified to be the major barrier.44 83 85 95 105 107 108
Methodologically, studies conducted among the Indian ethnic group outside India were collectively identified as South-Asians or Asians23–26 106 while they differ culturally, socially, politically, economically and even religiously.124 Two studies included from UK in this review have clearly shown such a difference with the neighbouring country (ie, India and Pakistan).27 58 Therefore, there is a need to address this population with such specificity in future research that can strengthen the practices even more efficiently. Also, with this population to be the largest migrating population in the world,7 it is important to understand their behaviour outside India. Studies show difference between various migration generations from the same ethnicity.27 58 This cannot happen without the influence of time elapsed since immigration, immigrant generation (ie, first, second or higher), acculturation, enculturation, perceived discrimination, attitudes/mistrust toward healthcare system, community barriers, sociocultural influence and many such complex determinants which adds further complexity to the issue of organ donation among such a population. Therefore, such specific research among this community is also needed to address the disproportionate representation between waiting list and donor list from this ethnic population outside the country of origin.
Though narrative synthesis is criticised for its lack of transparency, this study has tried to be as transparent as possible to strengthen its validity and credibility of the review and synthesis.30 125 The PRISMA flow chart, search strategy, data synthesis and analysis methods are clearly explained in this study to overcome those limitations.
Conclusion
This review showed that majority of the participants from India and of Indian origin hold positive attitude towards registration but show lower willingness and even lower practice of registration. Though this study showed the complex relationship and influences towards organ donation behaviour, lacunae were identified for further deeper understanding into such complex interactions determining the behaviour. There is also a lack of methodological rigour to study this population outside India, being collectively studied with their neighbouring population which are not homogenous. Also, within India, majority of the studies employed similar aims and methods leading to repetition of studies rather than diversified, wider and in-depth research.
Data availability statement
No additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
Institute for Health Research Ethics Committee from the University of Bedfordshire approved this study (IHREC931).
Acknowledgments
We would like to thank our librarian David Abdy from Institute for Health Research, University of Bedfordshire for his contribution with the development of the search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to conception of the study, design of work, data acquisition, data analysis, data interpretation, writing of the article, final approval, and accountability of the study. GR is the guarantor for this article.
Funding This review is led by the principal investigator Britzer Paul Vincent who is a PhD scholar at the Institute for Health Research, University of Bedfordshire funded by their Global Challenges Research Fund.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.