Article Text

Abstract
Objectives To understand whether and how effective integration of health and social care might occur in the context of major system disruption (the COVID-19 pandemic), with a focus on how the initiative may overcome past barriers to integration.
Design Rapid, descriptive case study approach with deviant case sampling to gather and analyse key informant interviews and relevant archival documents.
Setting The innovation (‘COVID-19 Protect’) took place in Norfolk and Waveney, UK, and aimed to foster integration across highly diverse organisations, capitalising on existing digital technology to proactively identify and support individuals most at risk of severe illness from COVID-19.
Participants Twenty-six key informants directly involved with project conceptualisation and early implementation. Participants included clinicians, executives, digital/information technology leads, and others. Final sample size was determined by theoretical saturation.
Results Four primary recurrent themes characterised the experiences of diverse team members in the project: (1) ways of working that supported rapid collaboration, (2) leveraging diversity and clinician input for systems change, (3) allowing for both central control and local adaptation and (4) balancing risk taking and accountability.
Conclusions This rapid case study underscores the role of leadership in large systems change efforts, particularly in times of major disruption. Project leadership overcame barriers to integration highlighted by prior studies, including engaging with aversion to clinical/safety risk, fostering distributed leadership and developing shared organisational practices for data sharing and service delivery. These insights offer considerations for future efforts to support strategic integration of health and social care.
- leadership
- integration
- health systems reform
- COVID-19
- digital health
Data availability statement
No data are available. Primary data collected for this study are not available to be publicly shared, as participants were assured confidentiality during the informed consent process. Given the small sample size and specifics of this case study, there is a risk of participant identification within the dataset.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study provides novel insights into whether and how effective integration of health and social care might occur during a period of major systems disruption, with a focus on how the initiative may overcome known barriers to integration.
This study extends prior empirical work by generating concrete, transferable insights into how leadership supported a major integration effort by fostering engagement across diverse organisations, mediating ambiguity in national guidance and creating space for local adaptation and balancing risk taking and accountability.
This is a single descriptive case study which may limit transferability, however we used extreme case sampling, which is ideal for identifying and characterising leading-edge practices or novel responses to extreme circumstances.
Like many rapidly evolving learning health systems models, further evaluation of impact on clinical outcomes is required.
Introduction
Health and social care integration is a national priority in the UK.1 2 However, initiatives to support integration (eg, sustainablity and transformation partnerships,3 integrated care pioneers4–6 and accountable care communities)7 have been highly variable, both in design and degrees of success.8 In 2021, a legislative proposal mandated integrated care systems (ICSs) to include National Health Service (NHS) organisations, local authorities, voluntary partners and charities.2 Evaluations of integrated care efforts have reported a wide range of barriers: misaligned governance, finance and commissioning arrangements across NHS and local care authority social services4 9; incompatible information technology systems and concerns about data sharing4 10 and challenges working across professional boundaries.11 12
Prior research has not fully examined the role of the broader political, social and historical context in which integration efforts are launched7; or relational aspects of partnership development.11 13 While leadership has been identified as essential to integrated care,12 14 the literature is primarily theoretical rather than empirical in nature,15 16 and no single model of leadership has emerged as relevant across diverse contexts. Experts call for more specific descriptions of how multilevel16 (or distributed) leadership17 manifests itself in integrated care partnerships.18 Others suggest further research is needed to understand leadership approaches that are successful in diverse policy and organisational environments,15 and the ways in which context might facilitate collaboration across organisational and professional boundaries remains a ‘black box’.19
The COVID-19 global pandemic disrupted multiple systems designed to protect public health and well-being in the UK.20 The extraordinary response to COVID-19 provided a unique opportunity to observe integration efforts during a period of major disruption, which potentially created an enabling environment for innovation.21 Therefore, we aimed to characterise a quickly emerging regional effort to operationalise the national vision for integrated support for highly vulnerable people. We carried out a rapid case study in order to understand whether and how effective integration of health and social care might occur in the context of major system disruption, with a focus on how the initiative may overcome past barriers to integration.
Study context
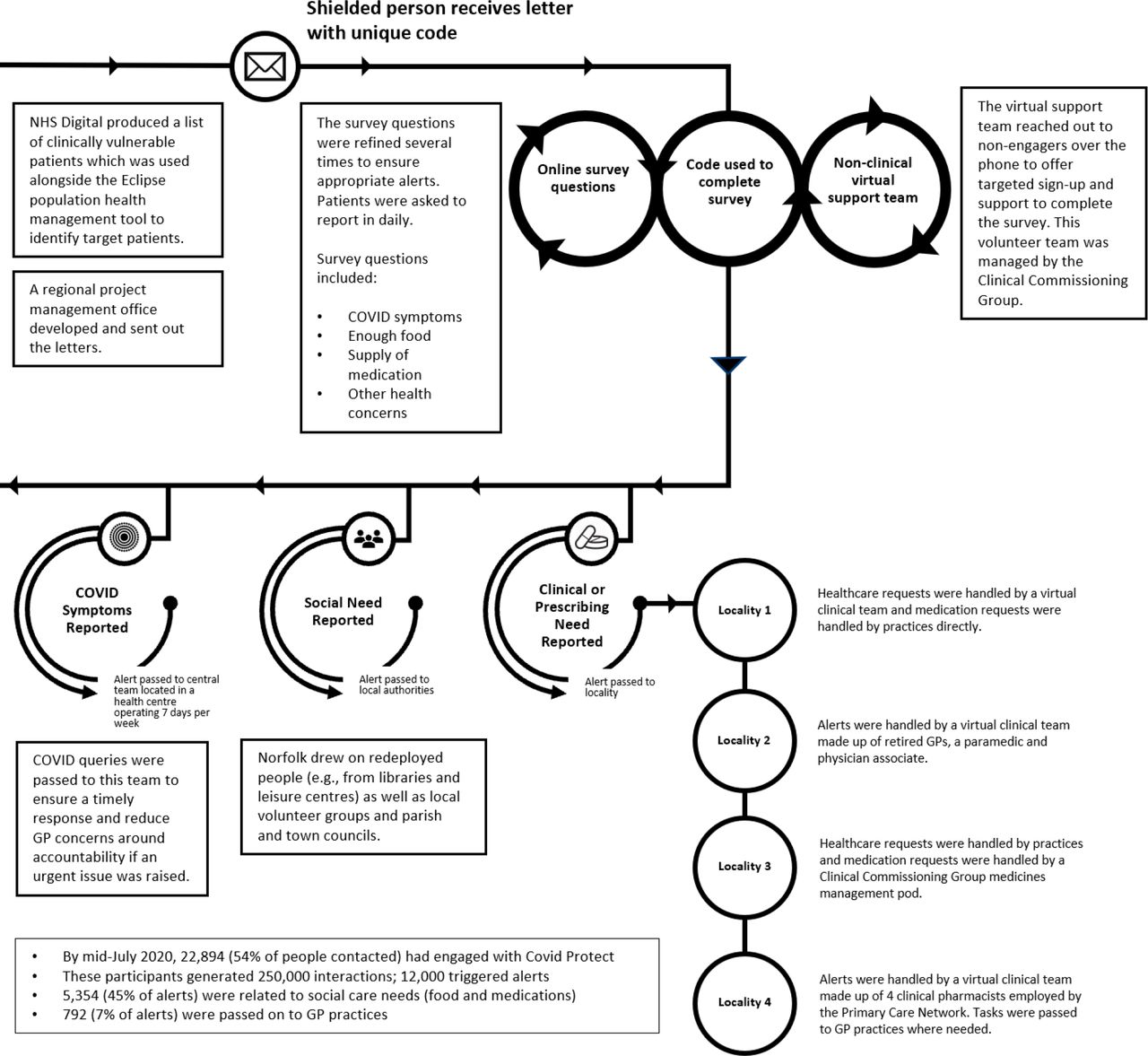
The COVID-19 global pandemic disrupted multiple systems designed to protect and promote public health and well-being in the UK.20 As COVID-19 hit the UK in February 2020, the response was urgent and far-reaching. The NHS generated a National Shielded Patient List of extremely clinically vulnerable people that local authorities were tasked with contacting to offer social care and support, working in coordination with other relevant organisations in the area.22 The level of patient-focused linkages across health and social care envisioned in the NHS response was particularly ambitious. Four control of patient information (COPI) notices were issued requiring NHS Digital, NHS England and Improvement, healthcare organisations, local authorities and general practitioners (GPs) to share patient information for disease control purposes.23 24 Recognising the need for the workforce to operate flexibly and move between organisations, NHS England and NHS Improvement produced multiprofessional workforce deployment guidance,25 and a COVID-19 Digital Staff Passport26 was developed. In local authorities, staff were also expected to be flexible so that organisations could make the best use of their resources and prioritise critical services. Finally, block payments for NHS providers reduced the need for local negotiation and data reporting for incentive payments. Building on the National Shielded Patient List, the innovation (‘COVID-19 Protect’) aimed to foster integration across highly diverse organisations (eg, Clinical Commissioning Group (CCG), GP practices, local authorities, volunteer service organisations), capitalising on existing digital technology to proactively identify and support individuals most at risk of severe illness from COVID-19 (figure 1).27 28
{kind=link}
The schematic diagram of COVID-19 Protect model. GP, general practitioner.
Methods
Study design
We used a rapid, descriptive case study approach29 with extreme case sampling30 to gather and analyse key informant interviews31 and relevant archival documents (eg, policies training curricula, operational communications). We identified the case through an executive management programme (led by LC and EL) designed to support digital transformation in the NHS and social care, in which participants described rapid adoption of novel approaches to delivering care in response to COVID-19. Deviant cases exhibit outcomes which are substantially different to other case study candidates. We considered the case as ‘extreme’ based on an early review from the CCG Research Team found that being engaged in the project appeared to be associated with more favourable COVID-19 outcomes, namely reduced mortality and hospital admissions. The work met the NHS Health Research Authority definition of service evaluation. The Consolidated criteria for Reporting Qualitative research checklist was used as a guide32; the completed checklist is included in online supplemental file 1.
Supplemental material
Data collection
We used a purposeful sampling approach,33 working with a liaison closely involved in COVID-19 Protect to identify key informants33 directly involved with project conceptualisation and early implementation, including a range of diverse roles, including clinicians, executives, digital/information technology leads and others. The final sample size was determined by theoretical saturation,34 which was achieved after completion of 26 interviews (total of 31 contacted, 4 non-responders, 1 refusal). Trained qualitative interviewers (LC, AA, EC, SC-C) conducted semi-structured interviews via video conferencing after obtaining informed consent that included our goals for conducting the study. Interviews were digitally recorded, professionally transcribed and reviewed to ensure accuracy. Interviews averaged 43 min in length (range 22–57 min). The semi-structured interview guide consisted of ‘grand tour’ questions35 to elicit study participants’ perspectives (online supplemental file 2). We used probes to generate ‘thick, rich descriptions’ of participants’ experiences, as well as to elicit both positive and negative views.36 37 We also gathered and systematically catalogued extensive archival documents provided by the project liaison and key informants. Documents included tools, protocols and templates (eg, standard operating procedures, clinical model overview, patient questionnaire, policies and regulations). All data were collected between October and December 2020.
Supplemental material
Data analysis
For the interview data, a four-person multidisciplinary team independently coded four transcripts, developing codes to classify data inductively and drafting an integrated code structure.38 Analysts then broke into teams of two, each team coding half of the remaining transcripts, resolving differences in coding by negotiated consensus. The final code structure (online supplemental table 1) was reapplied to all transcripts. We identified prominent and unifying themes across interviews using the constant comparative method of data analysis.39 40 In the final stages of analysis, we focused on the code categories that were most central to our primary research question, were supported by robust data, and offered novel information. We created multiple intersection reports to examine how codes related to one another, generating four overarching themes to capture the most prominent emergent insights from the dataset. We used established techniques (eg, highly experienced multidisciplinary researchers, methods to elicit both positive and negative views, professional transcription and verification, an analytic audit trail and participant confirmation) to ensure that data collection and analysis were systematic and verifiable.41 Analyses were conducted using ATLAS.ti V.8.
Supplemental material
For the archival data, a member of the study team systematically reviewed archival documents related to six domains: (1) clinical model and patient questionnaire; (2) project governance and GP practice engagement; (3) patient information; (4) data access and ethical considerations; (5) tools, protocols and templates and (6) the external environment, such as policies and regulations. Information from each group of documents was summarised to describe key points relevant to operationalising COVID-19 Protect, providing the research team detailed background and context to inform interpretation of the interview data.
Researcher reflexivity
Our research team was diverse with regard to disciplinary background, training and expertise. Three of us had roles in the digital leadership programme used for case identification that included a delegate who was our primary liaison to the COVID-19 Protect team. In order to mitigate potential for bias, we: (a) explicitly encouraged members to share discrepant views42; (b) actively engaged in reflexivity to explore our preconceptions throughout data collection, analysis and synthesis43 and (c) considered alternative conclusions from the data.44 Our motivations for conducting the research were described during the informed consent process.
We were guided by an ontology of critical realism (ie, we regard that there is a secular reality that may be largely captured through deep critical examination). Our epistemology is that it is possible to create knowledge through social constructionism (ie, using rigorous qualitative methods, we can elicit meaning from the lived experience of study participants and generate new insights from their shared experience). Our qualitative methodology is aligned with these assumptions. In terms of the brand of qualitative analysis, we used a reflexive thematic analysis approach.45 That is, we sought to understand the manifestation of leadership during crisis through finding patterns in the experiences of key informants. We triangulated these analyses with systematic review of project documents.
Patient and public involvement
No patients or members of the general public were directly involved in the design or implementation of this study. However, patient and community members’ experiences with the COVID-19 Protect project were gathered from interviews with a wide range of key informants. Findings were presented to the full COVID-19 Protect team and disseminated through a ‘Roadmap for Adoption’ document describing key processes, practices and tools related to the project.
Findings
Characteristics of study participants are reported in table 1. We identified four primary recurrent themes that characterised the experiences of diverse team members in the project: (1) ways of working that supported rapid collaboration; (2) leveraging diversity and clinician input for systems change; (3) allowing for both central control and local adaptation and (4) balancing risk taking and accountability. Each of these themes and associated subthemes are summarised in table 2 and described below, with illustrative quotations. Additional and expanded quotations are reported in online supplemental table 2.
Supplemental material
Study participant characteristics
Themes and subthemes
Ways of working that supported rapid collaboration
CCG leadership provided highly visible support throughout the project, fostering a common mission “there was a shared imperative and a very clear, shared objective as to what we were doing” (ID21), and reducing barriers to facilitate progress. At multiple junctures, members of the COVID-19 Protect team “heard directly from seniority that we could get on with things…(we) could raise issues immediately and they were unblocked” (ID14). The project team also identified concrete, meaningful ways to engage middle managers and frontline workers across the system. For example, those with patient-facing experience gave substantial input into refining the patient questionnaire, call handlers and supervisors were valued in operational problem solving, and locality teams made up of clinical and operational staff were tasked with developing standard operating procedures. In one locality, a change manager took the lead on alerts: “I was empowered to figure out how to manage alerts…and to make sure that people that lived within the boundaries of the area were fully supported” (ID3). Staff were energised by the rapid responsiveness to feedback. For instance, the software programming was viewed as ‘a heroic effort’ as suggestions were implemented within days:
people could see how fast their vision was being fulfilled…it gave people a belief that they could trek on and actually achieve what they set out to achieve (ID19).
Team members described a culture of appreciation, in which expressions of gratitude took many forms. Members were given role titles (eg, representatives from each locality became known as ‘clinical leads’), which made them ‘feel really proud’ and helped support role clarity. Project leadership routinely celebrated successes: “whenever there was a good feedback…he would always bring it up and celebrate” (ID24). As the project closed, the full team received small gifts and an email from senior leadership: “You should all be very proud of what you have done, and I shall continue to support you” (ID24).
Leveraging diversity and clinician input for systems change
The pandemic motivated an unusual degree of cooperation across sectors: “in the past, you would have transformation on one side…and the clinicians on the other side” (ID29) and “we just didn’t have any usual siloed thinking” (ID19). Alignment of roles was expedited: “normally to get things working across systems, it would take you months or years of negotiation and working out who was going to do what…that just melted away” (ID27).
Although the pandemic itself helped accelerate novel collaboration, project leadership ensured that this diversity was leveraged by attending to the composition of the project team: “It’s good to have…different people from each population there representing their area because they know certain foibles” (ID20) and encouraging expression of divergent views: “they were able to create that psychological safety that means that everyone can contribute no matter who they are and feel in that safe space to also appropriately challenge people” (ID22). Clinicians were deeply embedded in software design, and clinically driven decision-making was prioritised throughout the project where appropriate: “The project…brought clinicians in right at the beginning and every decision was clinically driven and clinically justified…clinical backing was absolutely key” (ID29).
GPs expressed concerns about data sharing and additional workload “There was a lot of assurance that needed to be provided that…we weren’t just opening up patient records to everybody” (ID32), and clinician-led, transparent dialogue was important to build trust:
We were on a call with everybody airing all their concerns, which meant there was lots of learning as we were going along, but in a positive way so that questions were being raised and helpfully answered by practices themselves… (ID17).
The investment in peer-to-peer clinician engagement appeared to begin to shift GP perspectives on both the project and broader population health approaches: “I think it started to open up awareness that there were some benefits to working in this way” (ID03). Nevertheless, some GP practices remained cautious.
A consequence of diverse organisations coming together in new ways meant there was some duplication, for instance, in closing feedback loops with local authorities: “We would definitely want to increase the level of coordination with local authorities…we did obviously link with them [but]…They were making phone calls to the same group of people” (ID01). Communications lagged at times, such as when some patients phoned in to their GP offices, some practices were unfamiliar with the programme, generating a degree of confusion or frustration. Nevertheless, building strong feedback loops between actors helped evidence the impact of stakeholder contributions, communicate programme achievements and minimise duplication.
Allowing for both central control and local adaptation
The central project team ensured a coordinated interface with national guidance and made rapid, iterative adaptations to the programme design and software. Given “a lack of clarity from [national] government…with almost daily changes of direction…adaptability was the only way” (ID31). At the same time, the central team recognised the importance of allowing each locality to develop their own approach based on existing clinical capacity and available resources: “[W]e said, ‘This is how the system works…you need to decide how best that will happen locally for you’” (ID16). In addition, the central team was mindful to respect the autonomous nature of GP practices: they are ‘masters of their own destiny’, and “they are their own businesses…we didn’t want to enforce a standard approach across all GP practices” (ID07):
We very much decided early that we didn’t want to rely on a kind of centralised process that we potentially didn’t feel would protect our vulnerable patients as well as we thought we could…Everyone was part of designing the system. (ID22)
However, developing models locally and at pace posed challenges which were freely discussed within the project and accepted as intrinsic to rapid, localised collaboration. Governance of a highly flexible model was “harder to manage…because there wasn’t a single approach…having a consistent clinical pathway would’ve made life easier” (ID07). Even when standard policies were in place, interpretation was variable across organisations: “there was no consistency as to which pharmacies would give out which drugs to which volunteers. There were standards, but the interpretation of those were sometimes different”(ID13).
Balancing risk taking and accountability
A sense of urgency compelled the team to move quickly and sometimes ahead of national guidance, putting aside risk mitigation practices that typically slow decisions: “Our patients are at risk. It’s for us to look after our own patients, not wait for others to tell us what to do…The train is about to leave the station. We need to get on the train, and we need to direct it” (ID14).
The removal of financial risks was regarded as key: ‘what really helped is the CCG and NHS were able to protect revenue streams…which allowed people to just focus on doing what was important’ (ID32). Organisational and departmental budgets were less of a sticking point: “we’ve all been much less precious about who’s paying for what…people have just got on and done it wth much less arguing over who’s paying for it” (ID13).
Normally we spend a long, long time going through formal business cases trying to justify how we’re going to spend something. In this case, we said…we know it needs the support, so we’re going to go at financial risk making sure that it’s appropriately staffed. We actually evaluated that element of it pretty quickly. (ID16)
Additional risks included clinical and privacy risks to patients, of particular concern to GP stakeholders, who reflected: “We’ll be the ones who are clinically negligent if your system doesn’t work” (ID17). Empowered clinical leads and operations teams brainstormed solutions, and largely (but not entirely) addressed such concerns by creating a COVID-19 surveillance team available online 7 days/week. The COPI notice permitted sharing patient information. Consequently, risk managers felt empowered to approve requests more quickly than usual:
You don’t get a pat on the back in the health service for being brave. Everybody wants everything signed off and to reduce the risk of anything to about zero. Because of the COPI notice…the senior information risk officers actually understood what was coming so they signed it off really quickly… (ID19).
While risk-taking was supported, accountability was also cultivated through flexible and pragmatic approaches. Reporting processes were put in place for ‘grip and control’, as well as informal feedback paths: “We were able to gently prompt. ‘You’re a little bit behind on some of your reviews’. Then suddenly, magically, they would start reviewing” (ID33). Those responsible for monitoring quality and performance were committed to building in accountability, although they were mindful not to overload staff with reporting requirements (‘we pared it right down’):
We also had to make sure that we weren’t taking any clinical risks…It was the balance of getting the governance in place in something that was so very, very fast-moving…Over a three week period, we tipped the see-saw to a point where, I felt, ‘Yes, we’ve got grip control…and the structures were in place’ (ID29).
Discussion
Integration of health and social care is a national priority in the UK, requiring major changes to current organisational, financial and social structures.1 2 The COVID-19 pandemic presented a rare opportunity to observe swift organisational change in the context of such a disruption. Using a rapid case study approach, we identified four themes that facilitated unique and substantial collaboration across sectors, with implications for future efforts to support strategic integration of health and social care. These themes were: (1) ways of working that supported rapid collaboration; (2) leveraging diversity and clinician input for systems change; (3) allowing for both central control and local adaptation and (4) balancing risk taking and accountability. The team’s ‘ways of working’ (also known as ‘culture’) were consistent with a ‘cooperative, integrative leadership culture’.46 Managing the inherent tensions in systems change efforts is a core leadership challenge.47 Leadership anticipated and engaged with tensions through explicit and deliberate ‘boundary spanners’ working across levels17 (eg, to achieve meaningful clinician buy-in) and developing ‘third-person strategies’ (structures, processes and systems which manifest as leadership).18
Prior literature shows that systems leadership is fundamental to building ICSs. However, this capacity is not well understood in a context that has been traditionally focused on leadership within single organisations.8 48 Our research complements and extends prior empirical work through generating concrete, transferable insights into how leadership supported a major integration effort by fostering engagement across diverse organisations (inspiring a shared mandate49 and promoting systems thinking),50 mediating ambiguity in national guidance and creating space for local adaptation51 (consistent with open systems theories of leadership)52 53 and balancing risk taking and accountability (consistent with the adaptive leadership principles).54 Specifically, this study shows how leadership overcame barriers to integration highlighted by prior studies,4 5 7 11 including engaging with aversion to clinical/safety risk, fostering distributed leadership and developing shared organisational practices for data sharing and service delivery. Identifying and addressing social care needs requires linkages across different levels of government as well as across government and non-government sectors.2 4 55 56 While best practices have yet to be established, our findings describe concrete examples of how systems leadership can catalyse and shape future integration efforts.
This case study also contributes to our understanding of learning health systems (LHS),57 providing an in-depth look at an actor-oriented network characterised by alignment around a common goal58; standards, processes and structures to enable multiactor collaboration and mechanisms for creating and sharing resources and know-how. Although clinicians tend to have a limited understanding of LHS frameworks, increasing resistance and limiting adoption,57 we describe concrete ways in which clinicians’ concerns were at least partly addressed through peer-to-peer advocacy and open forums for shared problem-solving. Our study extends recent taxonomies of LHS, which include clinical decision support models,59 by incorporating linkages to social care, and provides an empirical example of how value can be created by shifting from a value shop or chain towards a value network.60 Notably, LHS may also need to become forgetting health systems,61 and our case provides examples of how removal of longstanding policies intended to mitigate financial and privacy risks allowed for patient-focused and community-focused innovation.
Finally, our findings are consistent with and contribute to the literature demonstrating the role of leadership and ways of working (‘culture’)62 in health systems resilience (ie, a system’s ability to withstand shocks, adapt and transform).63 Prior studies have not fully examined the role of legitimacy of institutions. We saw clear strategies for fostering legitimacy, such as boundary spanners engaging with sceptical GPs.64 One model of health system resilience posits that leaders from across a system mobilise to create enabling environments for organisational adaptability and integrated transformation efforts when instability arises.65 We describe such a coordinated response, offering support for this model.
ICSs are intended to support the broader goals of improving population health and addressing health inequities. COVID-19 Protect laid the foundations for a population health management approach that can target hard-to-reach groups and those most in need of support. The project largely overcame common challenges such as data integration through deep engagement with stakeholders, particularly clinicians, to design user-friendly and relevant interfaces and to mitigate concerns about data privacy.66 Based on experiences with COVID-19 Protect, the team has since expanded the scope of the project into Protect NoW—a broader population health management approach targeting, for example, supports for patients with diabetes and cervical cancer screening outreach.
Our findings must be interpreted in light of several limitations. First, this is a single descriptive case study which may limit transferability, however we used extreme case sampling,30 which is ideal for identifying and characerising leading-edge practices or novel responses to extreme circumstances.29 67 Second, participants may have been influenced by social desirability response bias.68 We interviewed a wide range of key informants involved in designing and early implementation of the project, elicited details that would be difficult to misrepresent and instructed participants to share both positive and negative experiences.36 37 Notably, participants did express critical reflections and frustrations, and we sought critical and disconfirming evidence throughout our analysis process. We also conducted participant confirmation through oral presentations to the project team and review of findings by COVID-19 Protect project leadership.43 Third, like many rapidly evolving LHS models,59 further evaluation of impact on clinical outomes is required.28 Last, this study was conducted in the context of major disruption and the extent to which findings are transferrable to more routine integration efforts requires further evaluation. Nevertheless, our results are consistent with systems leadership theory and recent evidence from the UK that systems leadership capacity can be developed over a relatively short period of time.69
Of note, our intention was not to evtotal of 31 contacted, 4 non-responderaluate COVID-19 Protect, or to examine a programme that had been formally evaluated as successful. Instead, we sought to conduct a rapid case study to understand and describe in depth the practices and systems that need to be in place to allow cross-sectoral collaborations to flourish. Given the extraordinary interest in social and healthcare integration (and the recent national mandates), we expect that policymakers, executive and operational staff in health and social care and digital technology leads may find this deep description of the essential building blocks of cross-sectoral collaboration useful, as they have the potential to transcend the specifics of any one particular intervention or programme.
Data availability statement
No data are available. Primary data collected for this study are not available to be publicly shared, as participants were assured confidentiality during the informed consent process. Given the small sample size and specifics of this case study, there is a risk of participant identification within the dataset.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by Yale University Institutional Review Board (protocol 2000028439). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors substantially contributed to the manuscript. LC is the guarantor. LC: conceptual design, data collection and analysis, drafting of the manuscript, funding and supervision; AA: data collection and analysis, drafting of the manuscript; EC: data analysis, drafting of the manuscript; SC-C: data collection and analysis and drafting of the manuscript; BT: data analysis, drafting of the manuscript; EL: conceptual design, data analysis, drafting of the manuscript.
Funding The project was funded by the Norfolk and Waveney CCG and the Eastern Academic Health Science Network. BT was funded by the National Institute for Health Research (NIHR) West Midlands Applied Research Collaboration, https://warwick.ac.uk/fac/sci/med/about/centres/arc-wm/
Disclaimer The views expressed are by BT, and not necessarily those of the NIHR or the UK Department of Health and Social Care.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.