Article Text

Abstract
Objectives Healthcare workers are more likely to be infected by SARS-CoV-2. In order to assess the infectious risk associated with working in a hospital, we sought to estimate the proportion of healthcare professionals infected with SARS-CoV-2 by screening staff in a University Medical Center in France.
Setting A hospital-wide screening campaign (comprising a serological test and a questionnaire) ran from 18 May to 26 July 2020.
Primary and secondary outcome measures The seroprevalence rate was analysed in a multivariate analysis according to sociodemographic variables (age, sex and profession), exposure to SARS-CoV-2 and symptoms.
Results A total of 4840 professionals were included, corresponding to 74.5% of the centre’s staff. The seroprevalence rate (95% CI) was 9.7% (7.0% to 12.4%). Contact with a confirmed case of COVID-19 was significantly associated with seropositivity (OR (95% CI: 1.43, (1.15 to 1.78)). The seroprevalence rate was significantly higher among nursing assistants (17.6%) than among other healthcare professionals. The following symptoms were predictive of COVID-19: anosmia (OR (95% CI): 1.55, (1.49 to 1.62)), ageusia (1.21, (1.16 to 1.27)), fever (1.15, (1.12 to 1.18)), myalgia (1.03, (1.01 to 1.06)) and headache (1.03, (1.01 to 1.04)).
- public health
- virology
- occupational & industrial medicine
- infection control
- COVID-19
Data availability statement
Data are available upon reasonable request. Individual participant data will be available immediately following publication, in particular, all of the individual participant data collected during the trial, after de-identification. Data will be shared to investigators whose proposed use of the data has been approved by an independent review committee identified for this purpose. Proposals should be directed to gignon.maxime@chu-amiens.fr. To gain access, data requestors will need to sign a data access agreement. Data are available for 5 years at a third party website.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Study carried out on a large number of healthcare workers (HCWs) in a hospital.
Assessment of the contagion among HCWs during the first wave of COVID-19.
Bias related to the retrospective collection of data.
Introduction
Healthcare workers are more likely to be infected by SARS-CoV-2 because of their close, prolonged contact with infectious patients and coworkers. At Amiens University Medical Center (Amiens, France), a large number of patients with COVID-19 were admitted to the intensive care unit following the emergence of local disease clusters at the very beginning of the epidemic in France (figure 1).

Timeline of COVID-19 epidemic among patients admitted to Amiens University Medical Center, and organisational actions RT-PCR. *Decrease in surgical activity, closure of departments and requisiton of their staff. RT-PCR, reverse transcriptase PCR; SFM, surgical face mask.
The French national public health agency runs a nationwide PCR-based screening programme, in order to identify infected healthcare workers following notifications from hospitals. As of 30 June 2020, 31 171 staff members in French hospitals had been infected, and 84% of these were healthcare workers. The proportion of infected hospital staff varied from one region to another: it was 3.4% in the Hauts-de-France region, where the city of Amiens is located.1
In order to assess the infectious risk associated with working in a hospital, we sought to estimate the proportion of healthcare workers who had been infected with SARS-CoV-2 during the first stage of the epidemic. Hence, the primary objective of the present study was to assess the prevalence of anti-SARS-CoV-2 antibodies among our hospital’s staff. We also evaluate this seroprevalence as a function of age, sex, the presence of symptoms, the profession and the risk of contamination.
Materials and method
The screening campaign at Amiens University Medical Center ran from 18 May to 26 July 2020. It covered 6500 hospital employees and comprised a free-of-charge, non-obligatory serological test and a self-questionnaire. The latter was based on the WHO protocol for seroepidemiological investigation2 and updated with the knowledge at the time of the study. It collected data on demographics, the profession (see below), the presence of symptoms suggestive of COVID-19 at any time after 24 February 2020 (the date of the first recorded case of COVID-19 among the centre’s staff) and the risk of exposure (ie, contact with a confirmed case of COVID-19, patients, professionals or in a private setting and level of exposure related to the type of unit).
The professions were classified into five categories: physicians (including residents), nurses (including specialist nurses in surgery, anaesthesia and paediatrics), nursing assistants (including child care assistants), other healthcare professionals involved in patient care (such as physical therapists, radiology staff, psychologists, dietitians and stretcher bearers) and other hospital staff members not directly involved in care (administrative staff, maintenance staff, laboratory and pharmacy staff, etc).
At this time of the epidemics, patients with COVID-19 were hospitalised in dedicated units. So, the risk of occupational exposure to SARS-CoV-2 can be estimated by defining four levels of exposure : high risk of exposure workplaces (dedicated COVID-19 units), lower risk of exposure workplaces (other units), administrative workplaces with contact with patients, other workplaces without contact with patients.
Inclusion criteria
All hospital employees aged over the age of 18 years and with a serological test result and a completed questionnaire were included in the present study. All employees could be included in the study, whether they have been infected or not.
Serological test
Serological tests were performed with the WANTAI SARS-CoV-2 Ab test. At this time, this qualitative test showed the best sensitivity (94.5%) and a high specificity (100%) in comparison with the other available kits for the detection of total antibodies.3
Statistical analysis
We calculated the seroprevalence with its 95% CI. Intergroup differences were assessed with a χ2 test. The threshold for statistical significance was set to 5%. ORs (95% CI) were calculated in univariate analyses. Variables with a statistically significant difference were then included in two regression analyses. Age, sex and the risk of exposure (the profession and contact with a confirmed case of COVID-19) were analysed in the first model, and all the symptoms were included as covariates in the second model. On each questionnaire, any questions with missing data were excluded from the analysis. All statistical analyses were performed using R software (V.3.6.0), with ‘forestplot’ package and ‘glm’ function.4
Patient and public involvement
No patient involved.
Results
We included a total of 4840 people, corresponded to 74.5% of the hospital staff (figure 2).
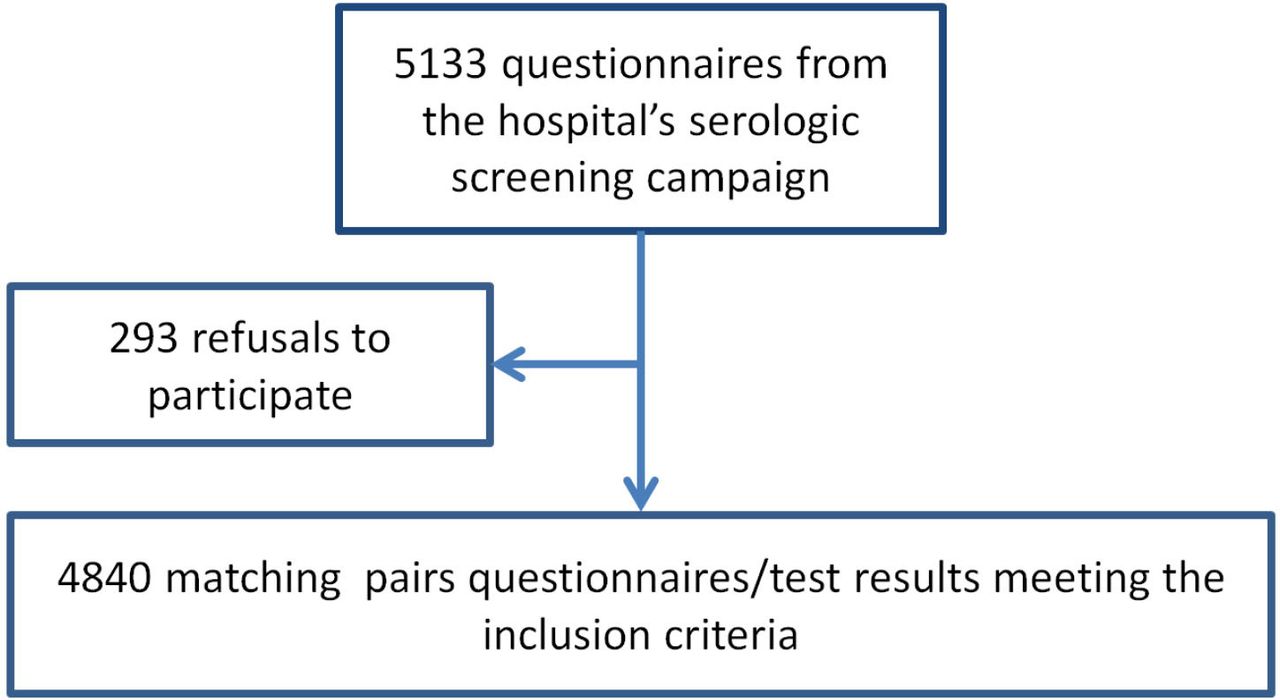
Study flow diagram.
The mean±SD age of the included staff was 40.5±11.4. Women (n=3778, 78.1%) outnumbered men. Total antibodies or IgGs against SARS-CoV-2 were detected in 471 participants, corresponding to a seroprevalence (95% CI) rate of 9.7% (7.0% to 12.4%).
In a multivariate analysis, the three variables significantly associated with seropositivity were female sex, contact with a confirmed case of COVID-19 and work as a nursing assistant (figure 3). The seroprevalence rate was significantly lower in the 30–39 age class than in the 18–29 age class.

{kind=link}
{kind=link}
{kind=link}
(A) Characteristics of the study population and exposure to SARS-CoV-2, and (B) symptoms that predicted seropositivity. SN, seronegative individuals; SP, seropositive individuals.
Data on symptoms were missing for 19 participants. At least one possible symptom of COVID-19 during the study period was reported by 3019 (62.6%) people: the prevalence of symptoms was significantly higher among seropositive people than among seronegative people (90.6% (n=426) and 59.6% (n=2593), respectively; p<0.01).
In a multivariate analysis, the symptoms that predicted seropositivity were fever, myalgia, headache, anosmia and ageusia. Conversely, the symptoms that predicted seronegativity were sore throat, wheeze, abdominal pain and rash. The other symptoms were not significantly associated with seropositivity or seronegativity.
Discussion
In a hospital-wide screening campaign, the seroprevalence (95% CI) rate for antibodies against SARS-CoV-2 among staff was 9.7% (7.0% to 12.4%).
Seroprevalence for antibodies against SARS-CoV-2 among healthcare professionals is known to depend on many variables, such as viral circulation in the region, the availability and use of personal protective equipment, and involvement in care for patients with COVID-19. Given that Amiens University Medical Center is located in one of the French regions most severely affected by COVID-19, we expected to find a higher seroprevalence rate among its staff.
A modelling study by the Pasteur Institute estimated that 5.3% (3.2% to 9.2%) of the population in the Hauts-de-France region had been infected with SARS-CoV-2 as of 11 May 2020.5 The French Public Health Agency has also estimated seroprevalence rates in the French population by age group, sex and county, using randomly selected serum samples.6 In week 15 (6–12 April 2020), the seroprevalence rate was 6.73% (5.36% to 8.11%). The number of infected people has increased since then but updated national data are not available. A number of international studies have investigated seroprevalence in the general population. However, it is difficult to compare seroprevalence rates when the level of viral contagion differs from one country to another.
The seroprevalence rate among healthcare workers has also been studied in various countries around the world. In studies of large numbers of healthcare workers in France’s neighbouring countries, carried out during the same period (April–July), the estimated seroprevalence rates ranged from 10.3% to 31.6%.7–10 In France, seroprevalence rate among healthcare workers in different hospitals has been estimated between 3.2% and 11.9%.11–14
In the present study, five symptoms were predictive of seropositivity: anosmia, ageusia, fever, myalgia and headache. In line with the literature data, anosmia was the best predictor of seropositivity.15–17 Results concerning the symptoms that predicted seropositivity should be considered only in the context of the infection with the Wuhan variant since symptoms suggestive of COVID-19 may have evolved with the emergence of other variants.
We found that the seropositivity rate was significantly higher among nursing assistants than among other professions. We do not have an explanation for this result, which has only been found in a few other studies.18 For example, Comar et al found a higher seroprevalence rate among physicians.19 Other studies did not observe an association between the profession and the prevalence of antibodies against SARS-CoV-2.20 21
Further studies are needed to explain our result, which may depend on many factors, ranging from the application of prevention measures to social conditions.
Eyre et al observed an association between seropositivity and working in COVID-19 units.22 However, other studies found that neither direct involvement in clinical care nor working in a COVID-19 unit increased the likelihood of being seropositive.16 17 20 21 Indeed, some researchers have even reported a below-average seroprevalence rate for individuals working in intensive care units.22 23 At this time of the epidemics in our hospital, patients with COVID-19 were hospitalised in specific units. Healthcare workers of these units were equipped with appropriate individual protective equipment and were trained by the infection prevention team. This may explain why professionals in these units do not have a significantly higher risk of contamination.
These various findings suggest that the availability and use of personal protective equipment (especially a face mask and alcohol-based hand sanitiser) effectively limit the risk of infection. In the months following this study, the information to all professionals on hygiene measures has been continued and adapted according to the recommendations.
In our hospital, other measures might have limited the circulation of SARS-CoV-2 (figure 1). Healthcare workers presenting symptoms suggestive of COVID-19 were offered a specific consultation and could provide a nasopharyngeal swab for reverse transcriptase PCR screening, within the limits of test availability. If SARS-CoV-2 was detected, workers remained on sick leave until 7 days after the symptoms had disappeared. The hospital’s usual activities were dramatically reduced: non-urgent consultations and surgical operations were cancelled. Employees could work from home if their presence at the hospital was not essential, and face-to-face meetings were replaced by video conferences.
The present study has some limitations. Our retrospective collection of data on symptoms induced bias. Indeed, participants were asked to report all the symptoms they had presented since 24 February 2020, some of which may have had a cause other than COVID-19. This bias might explain the low proportion of asymptomatic seropositive people (9.3%). On 23 July 2020, the French Public Health Agency estimated that 24.3% of PCR-positive individuals were asymptomatic.24 Our methodology prevented us from linking the self-reported symptoms to infection with SARS-CoV-2; this might have resulted in underestimation of the proportion of asymptomatic patients infected with SARS-CoV-2. Lastly, this study reported data collected after the first wave in France. At this time, data on cluster among the professionals were not available due to limited test accessibility. National contact tracing strategy dedicated to healthcare workers in French hospitals started in June 2020.
Data availability statement
Data are available upon reasonable request. Individual participant data will be available immediately following publication, in particular, all of the individual participant data collected during the trial, after de-identification. Data will be shared to investigators whose proposed use of the data has been approved by an independent review committee identified for this purpose. Proposals should be directed to gignon.maxime@chu-amiens.fr. To gain access, data requestors will need to sign a data access agreement. Data are available for 5 years at a third party website.
Ethics statements
Patient consent for publication
Ethics approval
This study complied with the European Union’s General Data Protection Regulation. Each participant received written information about the study’s objectives and procedures and gave their written consent to processing of their personal data. In line with the French legislation on non-interventional studies, the protocol was approved by Amiens University Hospital Committee (approval number ID: PI2020_843_0110), a hospital committee with competency for studies not requiring approval by an institutional review board.
Footnotes
Contributors MP-M designed the work, and was responsible for acquisition, analysis, and interpretation of data for the work. She drafted the work and approved the final version to be published. She agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. SC designed the work, and was responsible for acquisition, analysis, and interpretation of data for the work. She revised this paper critically for important intellectual content. She agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. CC was responsible for acquisition, analysis and interpretation of data for the work. She drafted the work and approved the final version to be published. She agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. EB was responsible for acquisition, analysis and interpretation of data for the work. He revised this paper critically for important intellectual content. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. J-LS designed the work and interpreted data for the work. He revised this paper critically for important intellectual content. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MD designed the work and made analysis. He drafted the work and approved the final version to be published. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. OG designed the work and interpreted data for the work. He revised this paper critically for important intellectual content. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MG designed the work, and was responsible for analysis and interpretation of data for the work. He drafted the work and approved the final version to be published. He agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. He accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The study was funded by the French Ministry of Health (award number: COVID-19-20-0135).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.