Article Text

Abstract
Introduction Peripheral arterial disease (PAD) is a marker of cardiovascular morbidity, causing disability, loss of mobility and poor quality of life, manifesting clinically in the form of intermittent claudication (IC). Physical exercise increases the distance walked and improves quality of life. The aim of our study will be increased walking distance prolonging the time of onset of pain in patients with symptomatic PAD (IC).
Methods and analysis This study will be performed in Mataró Hospital’s vascular surgery service and School of Health Sciences, TecnoCampus. This population comes from 15 primary healthcare centres ofNorth Barcelona, Spain (450 000 inhabitants).
This study will be a four-group parallel, longitudinal, randomised controlled trial, blind to analysis.
The main primary outcome of this study will be the improvement in pain-free walking distance. Others primary objectives are and improvement in functional status, quality of life and Ankle-Brachial Index (ABI). Secondary outcomes will be the analysis of cardiorespiratory fitness, evaluation of muscle fitness, determine the maintenance of primary objectives at 6 and 12 months.
We will be included 124 patients (31 per group). The changes of the outcome (Barthel, SF-12, VascQOL-6, ABI) of the three intervention groups vs the control group at 3, 6 and 12 months will be compared, both continuously (linear regression) and categorically (logistic regression). A person who has not performed at least 75% of the training will be considered to have not completed the intervention.
Ethics and dissemination The study will be conducted according to the Declaration of Helsinki . It was approved by the Ethics Committee of the Research Institute Primary Health IDIAP Jordi Gol (20/035 P),Barcelona 6 October 2020. Informed consent will be obtained from all patients before the start of the study. We will disseminate results through academic papers and conference presentations.
Trial registration number NCT04578990.
- Protocols & guidelines
- Vascular medicine
- Sports medicine
- Clinical trials
- Primary care
- Medical education & training
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Protocols & guidelines
- Vascular medicine
- Sports medicine
- Clinical trials
- Primary care
- Medical education & training
Strengths and limitations of this study
This is a longitudinal randomised controlled clinical trial to examine concurrent strength and endurance programmes in people with Intermitent Claudication.
Variable results will be measured in a quantified way by a multidisciplinar team.
The COVID-19 epidemiological environment can be a determining factor for carrying out groupal interventions.
We do not know the adherence to a long-term physical exercise programme carried out in primary care.
Introduction
The prevalence of peripheral arterial disease (PAD), increased gradually by age, increasing above the age of 60 years old. Between 2000 and 2020, the prevalence is expected to increase by 40% in China.1
In studies carried out in the general Spanish population, considered to be of low cardiovascular risk, the prevalence of PAD ranges from 3.7% to 8.5% depending on the different age groups studied.2–5
Between 40% and 75% of patients with PAD (diagnosed by Ankle-Brachial Index (ABI <0.9)) present symptoms (intermittent claudication (IC), respectively).6
Several studies have shown that PAD is a marker for cardiovascular morbidity and mortality in the form of myocardial infarction, stroke, vascular mortality and overall mortality compared with healthy people (ABI ≥0.9)7–9 causin, especially in people with IC, greater disability, greater loss of mobility and poorer quality of life compared with people free of this pathology.10 11 All of this was assessed using quality of life questionnaires and specific questionnaires for patients with PAD.12–14 In the same sense, a study carried out in Spain in 2013 concluded that these patients have a limited capacity for exercise as measured by the Walking Impairment Questionnaire15 and a significant reduction in quality of life assessed by the European Quality of Life Questionnaire (EQ-5D).15 Regardless of this limitation, PAD accelerates physical decline, even in patients with asymptomatic PAD, since often the absence of symptoms is due to the patient’s own restrictive physical activity thereby preventing their appearance.
Therapeutic strategies are aimed at two objectives: first to increase survival and second to improve symptoms and functional status through pharmacological and non-pharmacological treatment. There is a high number of patients with PAD who receive pharmacological treatment, but a small number achieve therapeutic objectives.16 17
Regarding non-pharmacological treatment, exercise can be an effective remedy to treat and prevent this disease, providing favourable systemic vascular effects that can reduce cardiovascular events, and has shown to improve blood perfusion, consequently improving the quality of life of patients. Specifically, in people with IC, supervised physical exercise programmes have shown an increase in the distance walked, a delay in the time of the onset of pain, and an improvement in quality of life compared with placebo.18–20
Walking training programmes have been shown to be effective in improving walking time.21 In turn, patients with PAD present impaired muscle fibres of the lower extremities,22 which causes muscle weakness23 24 and atrophy.25 26
In this regard, strength training of the muscle groups of the lower extremities would be justified in order to improve the ability to walk and quality of life in these patients.23
Strength training has shown to improve treadmill and flat ground walking ability in persons with PAD. Specifically, high-intensity strength training for the lower body is recommended as a training methodology to include in the treatment of PAD.23
On the other hand, concurrent strength and endurance training has been shown to improve physical capacity,27 28 and among patients with a higher risk of cardiovascular disease, it could provide more cardiovascular benefits, compared with aerobic or strength training on their own.29 However, this concurrent training methodology has been little explored and the comparison between concurrent strength and endurance training, exclusively strength training and the usual treadmill or walking training has not been performed in Spanish patients with PAD.28–30 This knowledge would help to determine which method could be more effective in inducing functional improvements in patients with PAD and, therefore, be applied based on the patient’s status.31 32
Although physical exercise programmes are of proven efficacy and relatively inexpensive, they are still little used in Spain for the management of patients with IC and the usual practice ends up being the recommendation in the form of standard advice for progressive ambulation that often is not carried out properly.
Furthermore, there are also no studies that assess the improvement based on the level of severity of the PAD measured according to the ABI value.
The aim of this paper is to assess the effectiveness of various supervised physical exercise programmes: concurrent strength and endurance training versus strength training versus walking training in patients with symptomatic PAD (IC) vs only advice to exercise in a Mediterranean population with low cardiovascular risk to determine the increase in the distance walked, the improvement in functional status and in the quality of life, as well as changes in the ABI 3, 6 and 12 months after the first visit.
Project objectives
The aim of the study is to asses whether an intervention based on supervised physical exercise (walking training, strength training and concurrent strength and endurance training, compared with standard advice) increases the pain free-walking distance, improves functional status, quality of life, ABI and cardiorespiratory and muscular fitness in people with IC.
Methods and analysis
Project period
Study is planned for the period between September 2021 and December 2022.
The planned end date is December 2023.
Setting
This study will be performed in Mataró Hospital’s vascular surgery service and School of Health Sciences, TecnoCampus-Pompeu Fabra University. This population comes from 15 primary healthcare centres of the Maresme area (North Barcelona, Spain).These centres cover a population of approximately 450 000 inhabitants.
Design
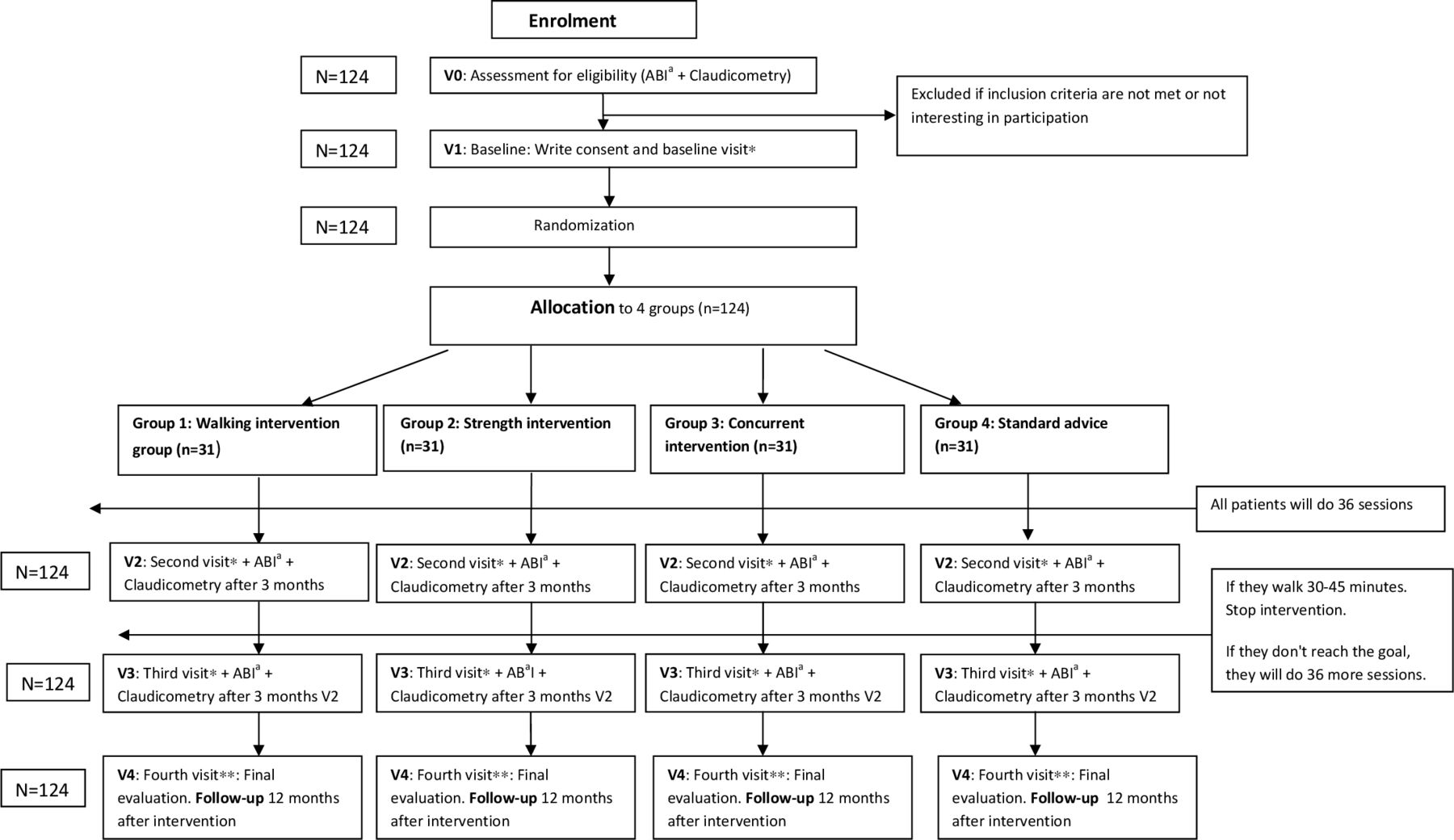
This is a four-group parallel, longitudinal, randomised controlled trial, blind to analysis, with a sample of participants studied between 3, 6 and 12 months after starting a physical exercise programme. Participants will be randomly assigned to four groups: (1) the walking intervention group will carry out a traditional supervised programme of progressive walking exercise; (2) the strength intervention group will carry out a strength training programme; (3) the concurrent training intervention group will carry out a combined progressive strength and endurance training; and (4) the control group will receive standard advice. The ARTPERfit design is shown in figure 1.

{kind=link}
ARTPERfit design. *Sociodemographic data, cardiovascular risk factors, previous vascular disease, drugs, treadmill walk distance, 6 min walk distance, Peripheral Arterial Disease Questionnaires, Quality of Life Questionnaires. **Cardiovascular risk factors, previous vascular disease, drugs, ABI, claudicometry, Treadmill walk distance, 6 min walk distance, Peripheral Arterial Disease Questionnaires, Quality of Life Questionnaires. aABI, Ankle-Brachial Index.
Recruitment
Participants will be recruited from the outpatient consultations of the Mataró Hospital’s vascular surgery service in a non-random, consecutive manner as they come to visit.
They will be checked to see if they meet the inclusion criteria; there are no exclusion criteria. If they do, they will be invited to participate and, if they accept, the inclusion visits, randomisation, intervention and follow-up will be carried out later (figure 1).
Eligibility criteria
Inclusion criteria are: (1) symptomatic patients with PAD visited in vascular surgery service of Mataró Hospital (ABI<0.9 and IC), (2) 40+ years of age, (3) read the patient information sheet, understand and sign informed consent (attached files as an online supplemental material).
Supplemental material
Supplemental material
Exclusion criteria are: (1) critical ischaemia and/or acute ischaemia of the lower limbs, (2) previous bilateral revascularisation of the lower limbs, (3) lower limb amputation, (4) cardiovascular, pulmonary, neurological and osteoarticular diseases that prevent the performance of the intervention, (5) appearance of IC beyond 30–45 min after the start of claudichometry and (6) refusal of the patient to participate in the study, inability to go to the centre due to lack of time or limiting disease.
Evaluation
Claudicometry and ABI at visits inicial and subseqüent avaluations will be performed by the vascular surgeon at Hospital de Mataró.
The initial and subsequent evaluations (3, 6 and 12 months) will be carried out by personnel specialised in physical exercise from the School of Health Sciences, TecnoCampus-Pompeu Fabra University.
Sociodemographic data, cardiovascular risk factors, previous vascular disease, drugs, PAD questionaires and quality of life questionaires performed at each visit by a trained nurse. It will also carry out the satisfaction questionnaire at 12 months in the intervention group.
Calculation of sample size
A sample of 124 patients, 31 per group, is needed to detect a 155 m improvement in pain-free walking distance after the intervention, assuming that the SD of the improvement is also 155 m (primary outcome 1). This is similar to an increase of 159 s walking without pain, for an average speed of 3.5 km/hour, as has been described previsouly.33 This calculation is comparable to any improvement as long as the SD is equal to or less than this improvement, and to comparisons between the control group and any of the other groups (correction for three comparisons using Bonferroni). This calculation is analogous for the rest of the result variables (Barthel, SF-12, VascQOL-6, ABI) as long as the difference observed between groups is equal to or greater than the common SD (primary outcome 2). The correlation between baseline and final measurement has been assumed to be 0.5. For comparisons between the treatment and control groups using the proportional version (proportion of patients improving in one group vs the other) the differences should be 50% improvement vs 15% or, equivalently, 35% vs 5%. In all calculations, a 20% rate of lost to follow-up, an alpha risk of 0.05, power of 80% and bilateral contrasts have been assumed.
Outcomes
The main objective of this project is to see the impact of an intervention based on supervised physical exercise on IC .
Main primary outcome
P1 Improvement in pain-free walking distance at 3 and 6 months.
Primary outcome
P2 Improvement in the general functional state (Barthel questionnaire) of people with IC at 3 and 6 months.
P3 Determine the improvement in the quality of life (SF-12 and VascQol-6) of people with IC at 3 and 6 months.
P4 Analyse the changes in the ABI at 12 months after the start of the study.
Secondary outcomes
S1 Analysis of cardiorespiratory fitness. Evaluation of functional capacity measured through VO2 peak in a gas analyser.
S2 Evaluation of muscle fitness by means of balance and strength tests of the lower extremities measured on a force platform.
S3 Determine the maintenance of objectives P1, P2 and P3 at 6 months after completing the intervention (12 months from the beginning of the study).
S4 Know the proportion of patients who continue to exercise 6 months after the end of the study (12 months from the start of the study).
Outcome mesures
Main primary outcome
P1 The outcome pain-free walking distance will be measured by the treadmille based walking and the 6-minuts walked test distance. The treadmill based walking is a pain free walking distance that was calculated as time walking on the treadmill until onset of IC.32 34
The goal would be an increase in walking distance of ≥155 m.
Primary outcome
P2 General functional state: using the Barthel questionnaire.
Maximum score: 100 points (90 if in a wheelchair).
Result: Degree of dependency <20 total; 20–35 severe; 40–55 moderate; ≥60 mild; 100 independent.
The goal would be an increase of 10 points.
P3 Perceived quality of life level through the specific questionnaires for PAD (VascuQOL-6) and quality of life questionnaires (SF-12).
The goal would be an increase of 10 points
P4 Changes in the ABI at 12 months.
The objective would be that at least 20% of the patients will go to a higher category:
Severe ischaemia (ABI ≤0.5) to moderate ischaemia (ABI 0.51–0.70) or moderate ischaemia (ABI 0.51–0.70) to mild ischaemia (ABI 0.71–0.89).
Secondary outcome
S1 Data corresponding to oxygen consumption (VO2), ventilation (VE), carbon dioxide production (VCO2), respiratory exchange rate (RER), partial pressure of oxygen at the end of expiration (PetO2) and the partial pressure of carbon dioxide at the end of expiration (PetCO2) will be recorded.
S2 Balance: The average of the two attempts will be assess.
Muscular: The mean values of vertical height and power recorded in the three jumps with a counter-movement will be measured.
Isometric test: The mean values of strength and explosive strength of both repetitions will be used.
S3 Determine the maintenance of objectives P1, S1 and S2 at 6 months after completing the intervention (12 months from the beginning of the study).
S4 Know the proportion of patients who continue to exercise 6 months after the end of the study (12 months from the start of the study).
At least 75% of sessions should be carried out in order to consider the intervention to have been performed.
Statistical analysis of outcomes
Descriptive statistics from each arm will be done, using frequencies and percents (categorical variables) and means and SD, or median and IQR if they not meet normality assumptions (continuous variables). All comparisons will be against the control arm, using χ2 tests (per cent), t-tests (means) and Mann-Whitney tests (medians) at baseline to check if the groups to compare are similar. The improvement on the different outcomes will be compared, independently, always comparing the control group with the other three arms and the baseline with the other visits (at 3, 6 and 12 months). The outcome difference will be analysed using binary variables (improvement on walking ≥155 m, improvement on Barthel ≥10 points, improvement on the VascQOL-6 scores ≥10 points, change to the upper category of ABI (yes/no)) using logistic regression, adjusting for potential confounders. In addition, the outcome difference will be analysed via lineal regression using the continuous difference (the former outcomes and fitness cardiorespiratory outcomes), adjusting for potential confounders, and transforming the variables, if needed, to follow the model assumptions. Proportion of patients still performing exercise 12 months after recruitment will be compared between arms using logistic regression, using still performing (yes/no) as dependent variable.
A participant who has not performed at least 75% of the training will be considered to have abandoned the intervention and will thus be excluded from the per-protocol analysis, but will still be included in the intention-to-treat analysis. % of training will be computed at 3 and 6 months. The outcome analysis will be performed both: per protocol (primary) and intention-to-treat (secondary). Patients who will leave training after 3 months because they are fit enough and had ≥75% of the training sessions done will be considered as adhered to the treatment at sixth month. This information will be included in the models as a dichotomus variable (‘months training’: 3 or 6).
We expect that the four arms to be comparable due to randomisation. However, propensity-score matching analysis will be added to the main analysis, to avoid unexpected differences.
As we expect to have all the information directly from the patient we do not expect to have much missing data.
Analysis will be partially blind. The analyst can guess what patients are from the control group (since they do not have the variable ‘months training’), but can not guess from what intervention arm are.
All analysis will be bilateral, with 5% significance and using Stata V.17 software.
Randomisation
Once patients agree to participate in the study (visit 1), the nurse who have performed the visit will ask to the statistician a group (control or one of the three intervention arms) where the patient shoud be asigned. The statistician will use an Excel sheet, with columns ‘group’, ‘age group (by 5 years)’, ‘gender’ and ‘severity of IC using the Rutherford questionnaire’35 (slight IC >300 m; moderate IC:100–300 m; severe IC <100 m) and with the rows randomly sorted, to select the first row still not asigned that matches with the selected participant.
Procedure
Variables
Distance walked without pain: distance walked in metres until onset of pain.
ABI: ratio of the higher of the two systolic pressures (tibial posterior and anterior artery) and arm systolic pressure using the systolic pressure of the highest arm.
Barthel questionnaire: consists of 10 items that measure a person’s daily functioning.
SF-12 questionnaire: is a self-reported outcome used as a quality of life measure.
VascQol-6 questionnaire: is a valid and responsive instrument for the assessment of health-related quality of life in PAD.
VO2peak: functional capacity measured in a gas analyser.
VE.
VCO2: VO2.
PetO2.
PetCO2.
Table 1 summarises the interventions that will be performed at each visit.
Interventions
Visit 0. Assessment for eligibility. ABI and claudichometry (performed by vascular surgery)
Visit 1. Baseline: Write consent and baseline visit (Collection of sociodemographic data, cardiovascular risk factors, previous vascular disease, drugs, treadmill walk distance*, 6 min walk distance**, life quality questionnaires*** and functional status questionnaires****). The 124 patients will be randomised into 4 groups of 31 people per group: 3 groups will be intervention groups (strength, endurance both) and a control group (standard advise on physical exercise).
Each of these groups will be subdivided into six people per group (except one group that will consist of seven people), in morning and afternoon shifts to improve accessibility (three times a week).
* Evaluating constant-load and graded-exercise treadmill test for IC.
To determine functional capacity, a graded-exercise treadmill test will be carry out to maximal toleration of claudication pain as previous studies described.36 37
After warm-up, patients will perform an incremental treadmill test starting at an initial speed of 2 mph and 0% grade with an increase every 3 min of 3.5% in grade until maximal claudication pain forced cessation of exercise. A perceived pain scale of 1–5 will be used every 30 s to determine the perception of the severity of the pain of claudication. 1=no pain, 2=onset of pain, 3=mild, 4=moderate, and 5=maximal pain. Furthemore, a constant-load treadmill test at light-moderate intensity will be performed to determine the slow component of oxygen uptake (VO2), mechanical and ventilatory efficiency. In both treadmill test, a gas analysis system (Ergostik, Geratherm Respiratory, Badd Kissingen, Germany) will be used and calibrated before each test using known O2 and CO2 concentrations and low, medium and high flow to calibrate VE. Gas exchange data will be taken breath-by-breath to obtain the variables VO2max, minute VE, ventilatory equivalent for oxygen (VE/VO), ventilatory equivalent for carbon dioxide (VE/VCO), RER, end-tidal partial pressure of oxygen and carbon dioxide (PetO2 and PetCO2, respectively). Blood pressure and heart rate (by 12-lead ECG) will be obtained during exercise.
** The 6 min Walk Test is a submaximal exercise test used to assess aerobic capacity and endurance. The distance covered over a time of 6 min is used as the outcome by which to compare changes in performance capacity.
*** VascuQOL-6 y SF-12.
****Barthel.
Group 1: walking intervention group
The intervention will consist of performing Treadmill training progression for 36–72 sessions. There will be three weekly sessions of 60 min duration per group session (5 groups of 6 people and 1 group of 7 people) in the morning and afternoon (at least 2 hours after eating), at the Tecnocampus centre supervised by a graduate of Science of Physical Activity and Sports.
Start of intervention
Session 1
Depending on the data obtained in visit 1 on the treadmill-based walking and the 6 min walking distance (carried out by a specially trained graduate of Physical Activity and Sports Sciences), the speed and degree of walking will be determined for each patient along with initial slope that is comfortable when walking until it induces symptoms of moderate IC (3–4) according to the Rutherford questionnaire33 in 5–10 min. Subsequently, there will be a period of rest (sitting or standing) for a few minutes until the pain in the lower limb disappears. This sequence will be repeated until the 60 min established in each session have been completed. The group supervisor will determine the progression of the intensity of the speed and the incline of the slope, increasing progressively and individually for each patient.
Session 2–36/72
The exercise programme pre-established in session 1 will continue until the 36 sessions are completed.
Visit 2: Three months after the start of the intervention, the same assessments will be repeated as in visit 1. In those participants who are able to walk 30–45 min, (still pausing, in the 60 min of the session), the intervention will end, although the control visits will be followed up. Otherwise, 72 sessions will be completed (6 months in total).
Visit 3: Three months after visit 2. All the parameters of visits 1 and 2 will be evaluated, and the intervention will be considered finished.
Visit 4: Twelve months after the start of the intervention, the same parameters as in previous visits will be evaluated again.
Group 2 strength intervention
The strength training programme will last 32 weeks. There will be three weekly sessions of 60 min, in groups (five groups of six people and one group of seven people) in the morning and afternoon (at least 2 hours after eating, where strength exercises will be carried out. The same guidelines as in the ‘walking intervention group’ will be followed, but in this case, applying strength exercises. If symptoms of moderate IC occur (3–4) based on the Rutherford questionnaire, a period of rest (sitting or standing) will be performed until the pain in the lower limb disappears. This sequence will be repeated until the strength training session is completed. The strength training will be carried out according to the guidelines established by our research group in a previous study.38 Briefly, strength training programme will be done with free weights, weight machines, plyometric exercises and unstable surfaces such as BOSU and TRX devices. Although the strength programme will focus primarily on lower extremity exercises, upper extremity strength exercises will be included to improve the quality of the strength training programme. In this sense, a circuit training methodology of 8 strength exercises will be implemented. The strength training programme will start with one set per exercise and will increase until reaching 3–4 sets per exercise at the end of the strength training programme. The number of repetitions per sets in each exercise will be between 5 and 15 depending on the intensity of the session. An initial rest of 30 s will be established between each exercise and 2 min between sets. The recovery time will gradually decrease (5 s between exercise and sets) depending on the evolution of each patient.
The first week of the strength training programme will focus on becoming familiar with the equipment and rating of perceived exertion39 familiarisation of how the patients should use the Borg Scale. For this purpose, patients will be asked for a perception of effort not exceeding 5 out of 10 (Borg scale, CR-10). The intensity and/or volume and/or density of the strength training will be gradually increased depending on the evolution of each patient until reaching a high intensity of 8 out of 10 (Borg scale, CR-10). High-intensity lower body strength training have been shown to be most beneficial in the treatment of PAD than light and moderate intensity (5–6 Borg scale, CR-10).21
Group 3 concurrent intervention
The concurrent programme will consist of alternating strength and endurance training in the same session for 36–72 weeks. There will be 3 weekly sessions of 60 min, in groups (five groups of six people and one group of seven people) in the morning and afternoon (at least 2 hours after eating, where strength exercises will be applied for 35 min and to complete the 60 min, the same guidelines as in the ‘walking intervention group’ will be followed, applying endurance training. If symptoms of moderate IC occur (3–4) based on the Rutherford questionnaire, a period of rest (sitting or standing) will be performed until the pain in the lower limb disappears. This sequence will be repeated until the 60 min established to end the concurrent training session has finished. The progression of the strength and endurance training will be carried out according to the guidelines previously established in groups 1 and 2.
Group 4 standard advice (control group)
They will receive standard advice from a healthcare provider, consisting of the recommendation to perform aerobic exercise with the lower extremities, warning that they should stop exercising at the moment that pain appears and resume it again when the pain disappears for a minimum of 30 min per session with a frequency of three times a week.
The methodology of visits 2, 3 and 4 will be the same in all groups.
In addition, the first three groups (intervention groups) will be given a satisfaction questionnaire.
No patient and public involvement.
Ethics and dissemination
The study will be conducted according to the guidelines of the Declaration of Helsinki . It was approved by the Ethics Committee of the Research Institute Primary Health IDIAP Jordi Gol (20/035-P), Barcelona 6 October 2020. Informed consent will be obtained from all patients antes del inicio del estudio. We will disseminate results through academic papers and conference presentations.
Data will only be accessible by investigators and statisticians committed to the project.
The results will be published in peer-reviewed journals and will be presented at national and international conferences and also disseminated among participants, patients’ communities and professionals of the Catalan Institute of Health through conferences.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: MTA, RF, GP and PT; Data curation: GP; Formal analysis: GP; Investigation: MTA, RF, MVG, EM, JLP, MG, NS and AHT; Methodology: GP, PT, GS; Supervision: MTA and RF; Validation: MTA, RF, GP, MVG, EM, MG, NS, AHT, PT and GS; Original draft: MTA, RF, GP and MVG; Writing-review and editing: MTA, RF, GP, MVG, EM, MG, NS, AHT and PT. All authors have read and agreed to the published version of the manuscript.
Funding This work was supported by a research grant from the Carlos III Institute of Health, Ministry of Economy and Competitiveness (Spain), awarded on the 2015 call under the Health Strategy Action 2017-2020, within the National Research Programme oriented to Societal Challenges, within the Technical, Scientific and Innovation Research National Plan 2017-2020, with reference PI20/00129, cofunded with the European Union ERDF funds.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.